
Household Air Pollution and High Blood Pressure: A Secondary Analysis of the 2016 Albania Demographic Health and Survey Dataset


Abstract
:1. Introduction
2. Methods
2.1. Study Design and Sampling Technique
2.2. Outcome Variable
2.3. Exposure Variable
2.4. Control Variables
2.5. Statistical Analysis
3. Results
3.1. Sample Characteristics
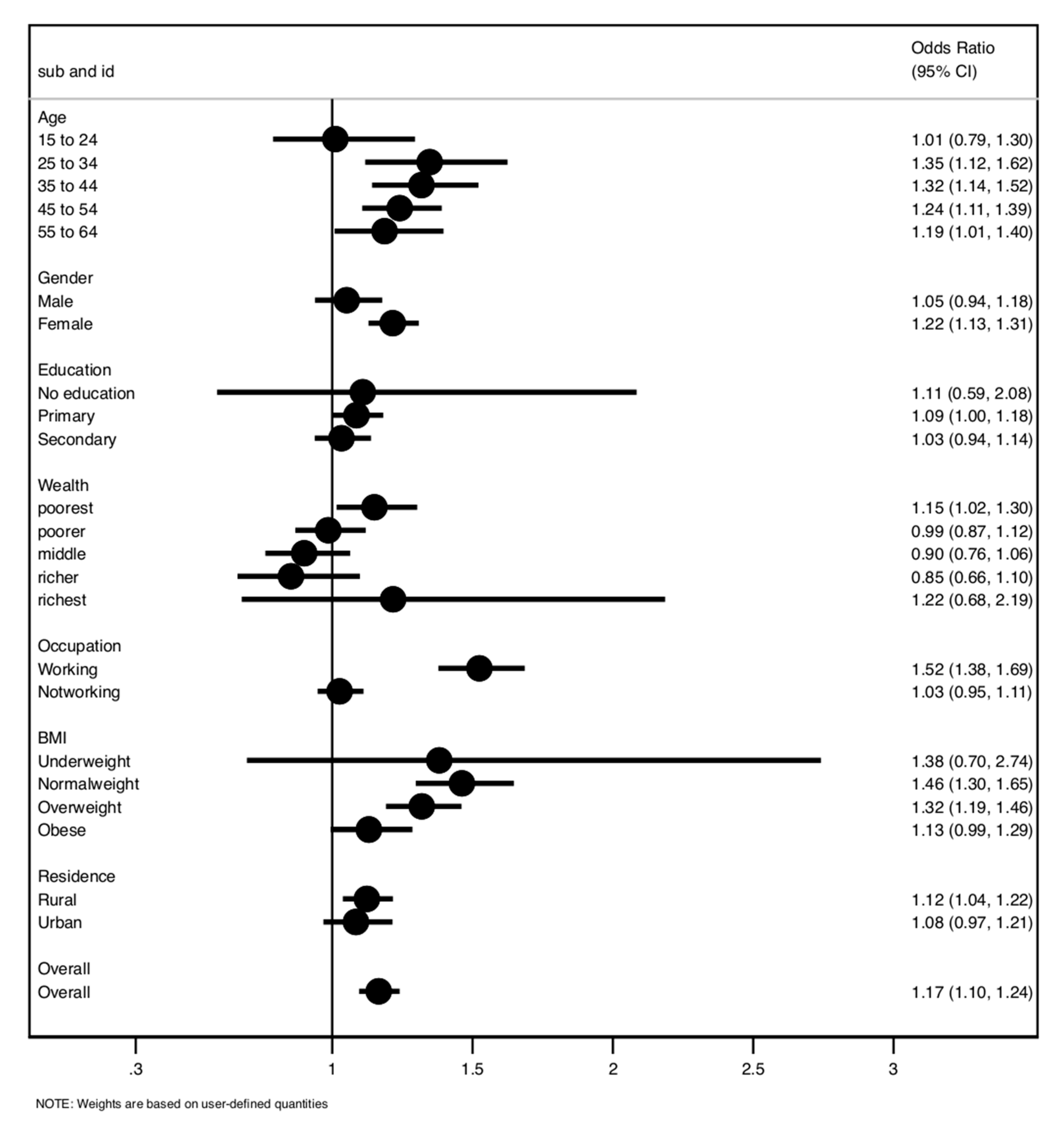
3.2. Association between HAP and Hypertension
4. Discussion
4.1. Strengths and Limitations
4.2. Policy Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Campbell, N.R.; Lackland, D.T.; Lisheng, L.; Niebylski, M.L.; Nilsson, P.M.; Zhang, X.H. Using the Global Burden of Disease study to assist development of nation-specific fact sheets to promote prevention and control of hypertension and reduction in dietary salt: A resource from the World Hypertension League. J. Clin. Hypertens. 2015, 17, 165–167. [Google Scholar] [CrossRef]
- Mozaffarian, D. Global Scourge of Cardiovascular Disease: Time for Health Care Systems Reform and Precision Population Health; American College of Cardiology Foundatiom: Washington, DC, USA, 2017. [Google Scholar]
- Kearney, P.M.; Whelton, M.; Reynolds, K.; Muntner, P.; Whelton, P.K.; He, J. Global burden of hypertension: Analysis of worldwide data. Lancet 2005, 365, 217–223. [Google Scholar] [CrossRef]
- Kumar, J. Epidemiology of hypertension. Clin. Queries Nephrol. 2013, 2, 56–61. [Google Scholar] [CrossRef]
- Zhou, B.; Bentham, J.; di Cesare, M.; Bixby, H.; Danaei, G.; Cowan, M.J.; Paciorek, C.J.; Singh, G.; Hajifathalian, K.; Bennett, J.E. Worldwide trends in blood pressure from 1975 to 2015: A pooled analysis of 1479 population-based measurement studies with 19.1 million participants. Lancet 2017, 389, 37–55. [Google Scholar] [CrossRef] [Green Version]
- Craig, L.S.; Gage, A.J.; Thomas, A.M. Prevalence and predictors of hypertension in Namibia: A national-level cross-sectional stu. PLoS ONE 2018, 13, e0204344. [Google Scholar] [CrossRef] [Green Version]
- WHO. A Global Brief on Hypertension: Silent Killer, Global Public Health Crisis; World Health Day; WHO: Geneva, Switzerland, 2013. [Google Scholar]
- Appelman, Y.; van Rijn, B.B.; Monique, E.; Boersma, E.; Peters, S.A. Sex differences in cardiovascular risk factors and disease prevention. Atherosclerosis 2015, 241, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Sarki, A.M.; Nduka, C.U.; Stranges, S.; Kandala, N.-B.; Uthman, O.A. Prevalence of hypertensionhypertension in low-and middle-income countries: A systematic review and meta-analysis. Medicine 2015, 94, e1959. [Google Scholar] [CrossRef] [PubMed]
- Pirkle, C.M.; Ylli, A.; Burazeri, G.; Sentell, T.L. Social and community factors associated with hypertension awareness and control among older adults in Tirana, Albania. Eur. J. Public Health 2018, 28, 1163–1168. [Google Scholar] [CrossRef] [PubMed]
- Apte, K.; Salvi, S. Household air pollution and its effects on health. F1000Research 2016, 5. [Google Scholar] [CrossRef]
- Mecaj, S.; llano, I. The Issue of Air Pollution in Albania. In The Ninth International Conference on Eurasian Scientific Development; Proceedings of the Conference; Association for Advanced Studies and Higher Education GmbH: Vienna, Austria, 2016; pp. 216–222. [Google Scholar]
- Juginović, A.; Vuković, M.; Aranza, I.; Biloš, V. Health impacts of air pollution exposure from 1990 to 2019 in 43 countries untries. Sci. Rep. 2021, 11, 22516. [Google Scholar] [CrossRef]
- WHO. Ambient (Outdoor) Air Pollution. 2018. Available online: https://www.who.int/newsroom/factsheets/detail/ambient-(outdoor)-air-quality-and-health (accessed on 5 December 2021).
- Rafaj, P.; Kiesewetter, G.; Gül, T.; Schöpp, W.; Cofala, J.; Klimont, Z.; Purohit, P.; Heyes, C.; Amann, M.; Kleefeld, J.-B.; et al. Outlook for clean air in the context of sustainable development goals. Glob. Environ. Chang. 2018, 53, 1–11. [Google Scholar] [CrossRef]
- WHO. Air Pollution. 2020. Available online: https://www.who.int/health-topics/air-pollution#tab=tab_1 (accessed on 4 December 2021).
- Lackland, D.T.; Weber, M.A. Global burden of cardiovascular disease and stroke: Hypertension at the core. Can. J. Cardiol. 2015, 31, 569–571. [Google Scholar] [CrossRef] [PubMed]
- WHO. The Top 10 Causes of Death. 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 6 December 2021).
- Gordon, S.B.; Bruce, N.G.; Grigg, J.; Hibberd, P.L.; Kurmi, O.P.; Lam, K.-B.H.; Mortimer, K.; Asante, K.P.; Balakrishnan, K.; Balmes, J. Respiratory risks from household air pollution in low- and middle-income countries. Lancet Respir. Med. 2014, 2, 823–860. [Google Scholar] [CrossRef] [Green Version]
- Ibrahim, M.M. Hypertension in developing countries: A major challenge for the “future”. Curr. Hypertens. Rep. 2018, 20, 38. [Google Scholar] [CrossRef] [PubMed]
- Giorgini, P.; di Giosia, P.; Grassi, D.; Rubenfire, M.; Brook, R.D.; Ferri, C. Air pollution exposure and blood pressure: An updated review of the literature. Curr. Pharm. Des. 2016, 22, 28–51. [Google Scholar] [CrossRef]
- Woolley, K.E.; Dickinson-Craig, E.; Bartington, S.E.; Oludotun, T.; Kirenga, B.; Mariga, S.T.; Kabera, T.; Coombe, A.; Pope, F.D.; Singh, A. Effectiveness of interventions to reduce household air pollution from solid biomass fuels and improve maternal and child health outcomes in low-and middle-income countries: A systematic review protocol. Syst. Rev. 2021, 10, 1–7. [Google Scholar] [CrossRef]
- Mohapatra, I.; Das, S.C.; Samantaray, S. Health impact on women using solid cooking fuels in rural area of Cuttack district Odisha. J. Fam. Med. Prim. Care 2018, 7, 11. [Google Scholar]
- Qiu, Y.; Yang, F.-A.; Lai, W. The impact of indoor air pollution on health outcomes and cognitive abilities: Empirical evidence from China. Popul. Environ. 2019, 40, 388–410. [Google Scholar] [CrossRef]
- Arku, R.E.; Ezzati, M.; Baumgartner, J.; Fink, G.; Zhou, B.; Hystad, P.; Brauer, M. Elevated blood pressure and household solid fuel use in premenopausal women: Analysis of 12 Demographic and Health Surveys (DHS) from 10countries’countries. Environ. Res. 2018, 160, 499–505. [Google Scholar] [CrossRef]
- Lee, K.K.; Bing, R.; Kiang, J.; Bashir, S.; Spath, N.; Stelzle, D.; Mortimer, K.; Bularga, A.; Doudesis, D.; Joshi, S. Adverse health effects associated with household air pollution: A systematic review, meta-analysis, and burden estimate on study. Lancet Glob. Health 2020, 8, e1427–e1434. [Google Scholar] [CrossRef]
- Deng, Y.; Gao, Q.; Yang, D.; Hua, H.; Wang, N.; Ou, F.; Liu, R.; Wu, B.; Liu, Y. Association between biomass fuel use and risk of hypertensionhypertension among Chinese older people: A cohort study. Environ. Int. 2020, 138, 105620. [Google Scholar] [CrossRef]
- Institute of Health Metrics and Evaluation. IHME-Compare G; University of Washington: Washington, DC, USA, 2016. [Google Scholar]
- IEAG Energy. CO2 Status Report 2017; International Energy Agency: Paris, France, 2018. [Google Scholar]
- Painschab, M.S.; Davila-Roman, V.G.; Gilman, R.H.; Vasquez-Villar, A.D.; Pollard, S.L.; Wise, R.A.; Miranda, J.J.; Checkley, W.; CRONICAS Cohort Study Group. Chronic exposure to biomass fuel is associated with increased carotid artery intima-media thickness and a higher prevalence of atherosclerotic plaque. Heart 2013, 99, 984–991. [Google Scholar] [CrossRef] [PubMed]
- Lim, Y.-H.; Kim, H.; Kim, J.H.; Bae, S.; Park, H.Y.; Hong, Y. Air pollution and symptoms of depression in elderly adults. Environ. Health Perspect. 2012, 120, 1023–1028. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samet, J.M.; Bahrami, H.; Berhane, K. Indoor air pollution and cardiovascular disease: New evidence from Iran. Circulation 2016, 133, 2342–2344. [Google Scholar] [CrossRef] [PubMed]
- Chobanian, A.V. Prehypertension revisit. Hypertension 2006, 48, 812–814. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, L.; Yang, A.; He, X.; Liu, J.; Ma, Y.; Niu, J.; Luo, B. Indoor air pollution from solid fuels and hypertension: A systematic review and metanalysis. Environ. Pollut. 2020, 259, 113914. [Google Scholar] [CrossRef]
- Lika, M.; Çoku, A.; Nelaj, E. Health impact assessment of air pollution in some regions in Albania. J. Life Sci. 2012, 6, 1028. [Google Scholar]
- Ofori, S.N.; Fobil, J.N.; Odia, O.J. Household biomass fuel use, blood pressure and carotid intima media thickness: A cross sectional study of rural dwelling women in Southern Nigeria. Environ. Pollut. 2018, 242, 390–397. [Google Scholar] [CrossRef]
- Fatmi, Z.; Ntani, G.; Coggon, D. Coronary heart disease, hypertension and use of biomass fuel among women: Comparative cross-sectional study. BMJ Open 2019, 9, e030881. [Google Scholar] [CrossRef] [Green Version]
- Balmes, J.R. Household air pollution from domestic combustion of solid fuels and health. J. Allergy Clin. Immunol. 2019, 143, 1979–1987. [Google Scholar] [CrossRef]
- Ferguson, L.; Taylor, J.; Davies, M.; Shrubsole, C.; Symonds, P.; Dimitroulopoulou, S. Exposure to indoor air pollution across socioeconomicsocio-economic groups in high-income countries: A scoping review of the literature and a modelling methodolody. Environ. Int. 2020, 143, 105748. [Google Scholar] [CrossRef] [PubMed]
- Abtahi, M.; Koolivand, A.; Dobaradaran, S.; Yaghmaeian, K.; Mohseni-Bandpei, A.; Khaloo, S.S.; Jorfi, S.; Saeedi, R. National and sub-national age-sex specific and cause-specific mortality and disability-adjusted life years (DALYs) attributable to household air pollution from solid cookfuel use (HAP) in Iran, 1990–2013. Environ. Res. 2017, 156, 87–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piedrahita, R.; Johnson, M.; Bilsback, K.R.; L’Orange, C.; Kodros, J.K.; Eilenberg, S.; Naluwagga, A.; Shan, M.; Sambandam, S.; Clark, M. Comparing regional stove-usage patterns and using those patterns to model indoor air quality impacts. Indoor Air 2020, 30, 521–533. [Google Scholar] [CrossRef] [PubMed]
- WHO. Burning Opportunity: Clean Household Energy for Health, Sustainable Development, and Wellbeing of Women and Children Well-Being; WHO: Geneva, Switzerland, 2016; Available online: www.who.int/airpollution/publications/burning_opportunities/en/ (accessed on 16 February 2022).
- Fullerton, D.G.; Bruce, N.; Gordon, S.B. Indoor air pollution from biomass fuel smoke is a major health concern in the developing world. Trans. R. Soc. Trop. Med. Hyg. 2008, 102, 843–851. [Google Scholar] [CrossRef] [Green Version]
- Smith, K.R.; Pillarisetti, A. Household Air Pollution from Solid Cook fuels and Its Effects on Health. In Injury Prevention and Environmental Health, 3rd ed.; Mock, C.N., Nugent, R., Kobusingye, O., Eds.; The International Bank for Reconstruction and Development/The World Bank: Washington, DC, USA, 2017; Chapter 7. Available online: https://www.ncbi.nlm.nih.gov/books/NBK525225/ (accessed on 16 February 2022). [CrossRef] [Green Version]
- WHO. Indoor Air Quality Guidelines: Household Fuel Combustion; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- McLean, E.V.; Bagchi-Sen, S.; Atkinson, J.D.; Ravenscroft, J.; Hewner, S.; Schindel, A. Country-level analysis of household fuel transitions. World Dev. 2019, 114, 267–280. [Google Scholar] [CrossRef]

{kind=link}
| Normotensive | Hypertensive | p-Value | |||
|---|---|---|---|---|---|
| Number | Percentage | Percentage | Percentage | ||
| % | % | ||||
| Sex | 0.000 | ||||
| Male | 5988 | 28.72 | 68.6 | 31.4 | |
| Female | 14,858 | 71.28 | 70.7 | 29.2 | |
| Education | 0.000 | ||||
| No education | 190 | 0.91 | 70.5 | 29.5 | |
| Primary | 9593 | 46.04 | 64.0 | 36.1 | |
| Secondary+ | 11,054 | 53.05 | 75.6 | 24.4 | |
| Wealth | 0.000 | ||||
| Poorest | 5828 | 27.96 | 66.7 | 33.2 | |
| Poorer | 5027 | 24.11 | 68.7 | 31.2 | |
| Middle | 4075 | 19.55 | 71.04 | 28.9 | |
| Richer | 3526 | 16.91 | 72.77 | 27.2 | |
| Richest | 2390 | 11.47 | 75.6 | 24.3 | |
| Not Working | 0.000 | ||||
| Working | 8515 | 40.8 | 27.9 | 12.93 | |
| Not working | 12,331 | 59.1 | 71.35 | 16.9 | |
| BMI | 0.000 | ||||
| Underweight | 503 | 7.4 | 91.55 | 7.35 | |
| Normal weight | 8252 | 40.3 | 84.01 | 15.98 | |
| Overweight | 7166 | 35.0 | 66.32 | 33.67 | |
| Obese | 4519 | 22.10 | 47.9 | 52.02 | |
| Place of Residence | 0.000 | ||||
| Rural | 11,303 | 54.2 | 68.34 | 31.65 | |
| Urban | 9543 | 45.7 | 72.2 | 27.77 | |
| Age of Households | 0.000 | ||||
| 15 to 24 | 4511 | 21.6 | 93.48 | 6.51 | |
| 25 to 34 | 4082 | 19.58 | 87.0 | 13.0 | |
| 35 to 44 | 4091 | 19.62 | 73.5 | 26.5 | |
| 45 to 54 | 5257 | 25.2 | 53.2 | 46.7 | |
| 55 to 64 | 2905 | 13.93 | 36.0 | 63.9 |
| Unadjusted | Adjusted Association | |
|---|---|---|
| OR (95% CI) | OR (95% CI) | |
| Household air pollution | ||
| Clean vs. unclean | 1.17 (1.10 to 1.24) | 1.09 (1.01 to 1.19) |
| Sex | ||
| Female vs. male | 0.90 (0.84 to 0.96) | 0.80 (0.74 to 0.86) |
| Education | ||
| No education | 1.29 (0.94 to 1.77) | 1.20 (0.84 to 1.71) |
| Primary | 1.75 (1.65 to 1.86) | 1.21 (1.12 to 1.30) |
| Secondary+ | 1 (reference) | 1 (reference) |
| Wealth | ||
| Poorest | 1.54 (1.39 to 1.72) | 1.51 (1.29 to 1.76) |
| Poorer | 1.41 (1.26 to 1.58) | 1.33 (1.16 to 1.53) |
| Middle | 1.27 (1.13 to 1.42) | 1.21 (1.06 to 1.39) |
| Richer | 1.16 (1.03 to 1.31) | 1.13 (0.99 to 1.31) |
| Richest | 1 (reference) | 1 (reference) |
| Not Working | ||
| Not working vs. working | 0.87 (0.82 to 0.92) | 1.02 (0.95 to 1.10) |
| BMI | ||
| Underweight | 0.42 (0.30 to 0.59) | 0.84 (0.59 to 1.21) |
| Normal weight | 1 (reference) | 1 (reference) |
| Overweight | 2.77 (2.47 to 2.88) | 1.50 (1.38 to 1.64) |
| Obese | 5.70 (5.24 to 6.19) | 2.67 (2.42 to 2.93) |
| Place of Residence | ||
| Rural vs. urban | 1.20 (1.13 to 1.28) | 1.07 (0.98 to 1.16) |
| Age of Households | ||
| 15 to 24 | 1 (reference) | 1 (reference) |
| 25 to 34 | 2.15 (1.86 to 2.50) | 1.78 (1.52 to 2.09) |
| 35 to 44 | 5.17 (4.5 to 5.93) | 3.72 (3.20 to 4.32) |
| 45 to 54 | 12.60 (11.07 to 14.36) | 8.40 (7.27 to 9.69) |
| 55 to 64 | 25.49 (22.15 to 29.33) | 16.86 (14.47 to 19.64) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abba, M.S.; Nduka, C.U.; Anjorin, S.; Uthman, O.A. Household Air Pollution and High Blood Pressure: A Secondary Analysis of the 2016 Albania Demographic Health and Survey Dataset. Int. J. Environ. Res. Public Health 2022, 19, 2611. https://doi.org/10.3390/ijerph19052611
Abba MS, Nduka CU, Anjorin S, Uthman OA. Household Air Pollution and High Blood Pressure: A Secondary Analysis of the 2016 Albania Demographic Health and Survey Dataset. International Journal of Environmental Research and Public Health. 2022; 19(5):2611. https://doi.org/10.3390/ijerph19052611
Chicago/Turabian StyleAbba, Mustapha S., Chidozie U. Nduka, Seun Anjorin, and Olalekan A. Uthman. 2022. "Household Air Pollution and High Blood Pressure: A Secondary Analysis of the 2016 Albania Demographic Health and Survey Dataset" International Journal of Environmental Research and Public Health 19, no. 5: 2611. https://doi.org/10.3390/ijerph19052611
APA StyleAbba, M. S., Nduka, C. U., Anjorin, S., & Uthman, O. A. (2022). Household Air Pollution and High Blood Pressure: A Secondary Analysis of the 2016 Albania Demographic Health and Survey Dataset. International Journal of Environmental Research and Public Health, 19(5), 2611. https://doi.org/10.3390/ijerph19052611