
Traditional East Asian Herbal Medicine for Post-Stroke Insomnia: A Systematic Review and Meta-Analysis of Randomized Controlled Trials


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Registration
2.2. Inclusion and Exclusion Criteria
2.2.1. Types of Studies
2.2.2. Types of Participants
2.2.3. Types of Interventions
Experimental Intervention
Control Intervention
2.2.4. Types of Outcome Measures
2.3. Search Methods
2.4. Date Collection and Analysis
2.4.1. The Selection of Literature
2.4.2. Data Extraction
2.5. ROB Assessment
2.6. Data Analysis
2.6.1. Measures of Treatment Effect
2.6.2. Assessment of Heterogeneity
2.6.3. Data Synthesis
2.6.4. Subgroup Analysis
2.6.5. Sensitivity Analysis
2.6.6. Publication Bias
2.6.7. Summary of Evidence
3. Results
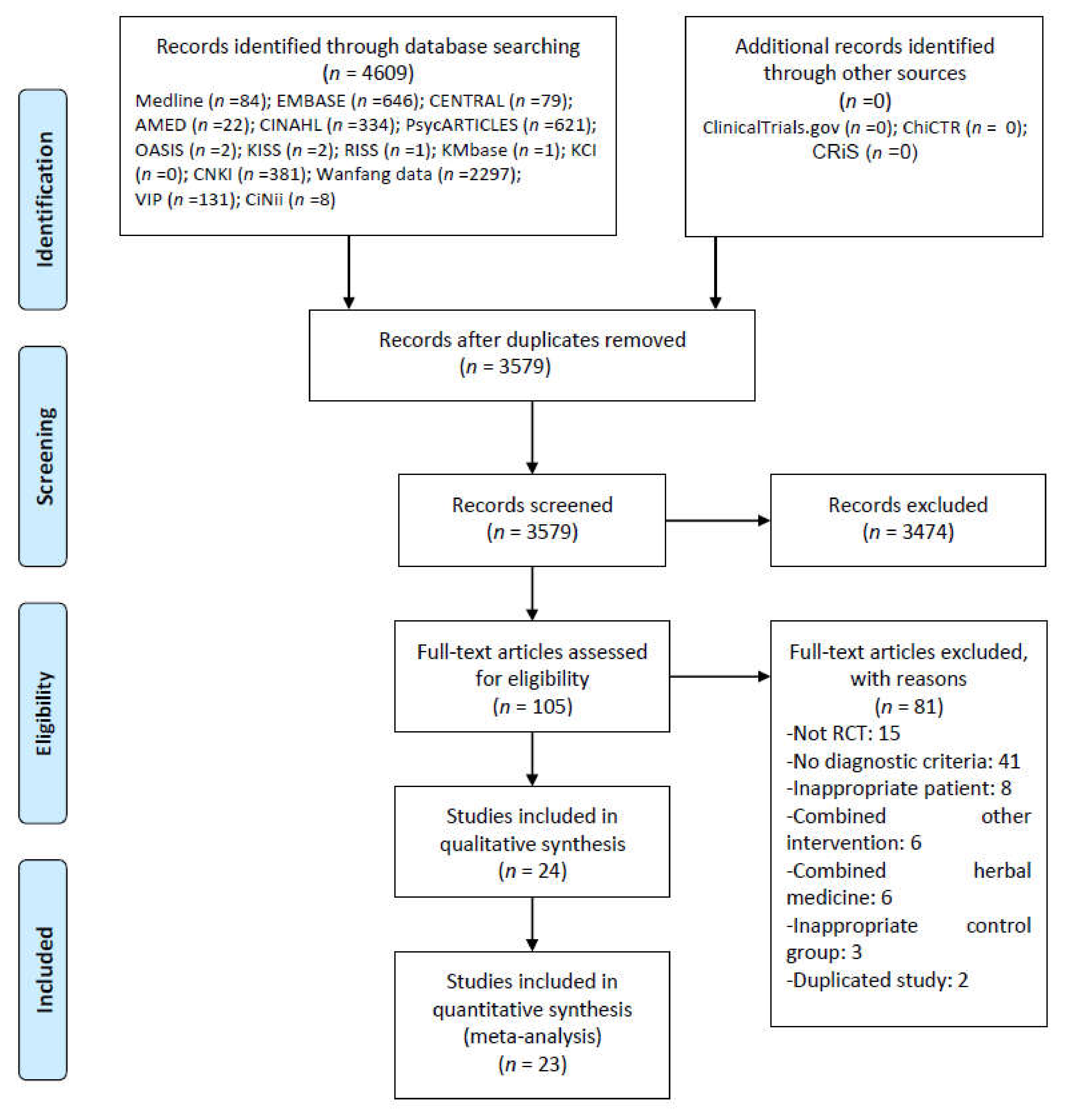
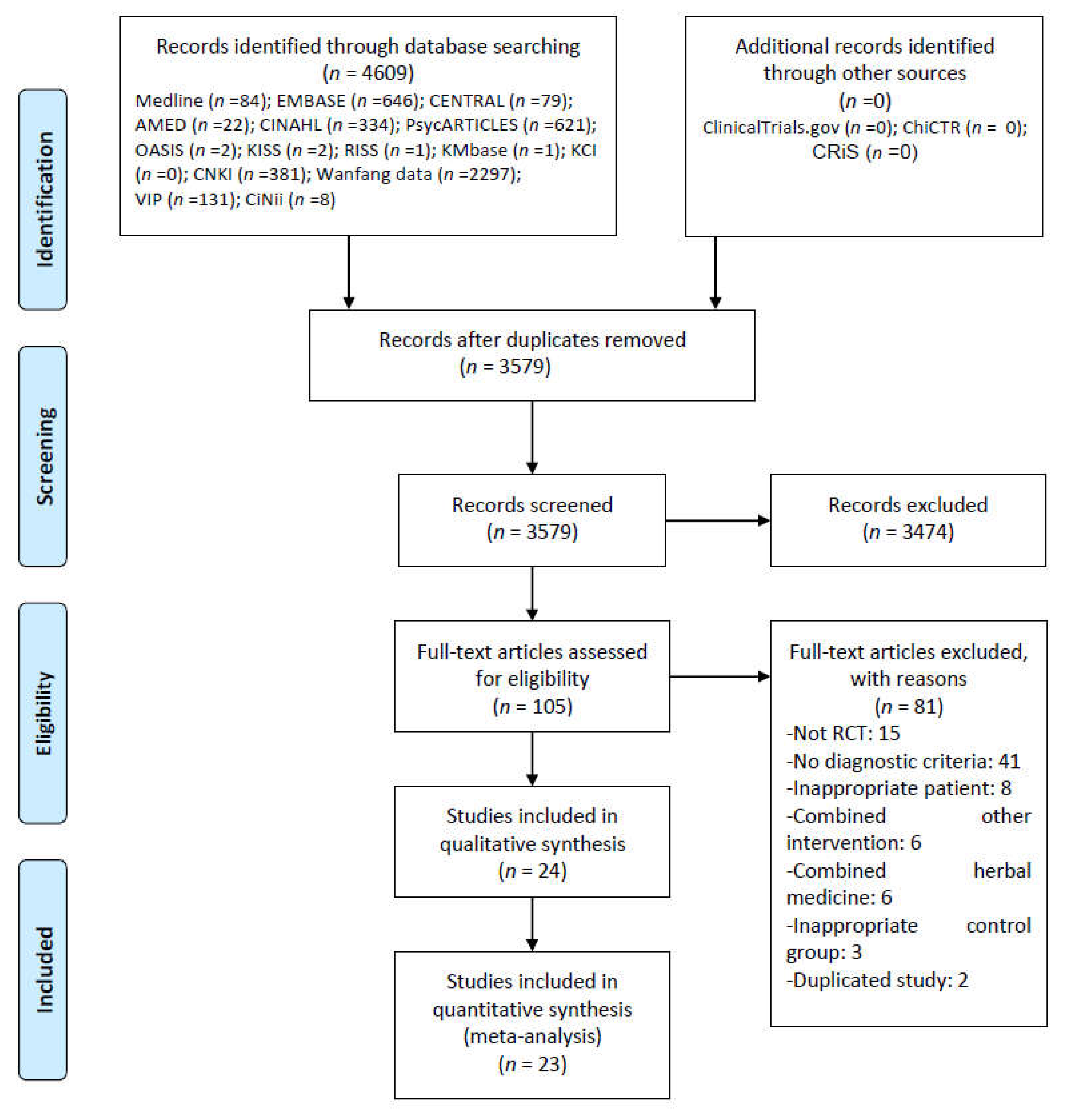
3.1. Study Selection
3.2. Study Characteristics
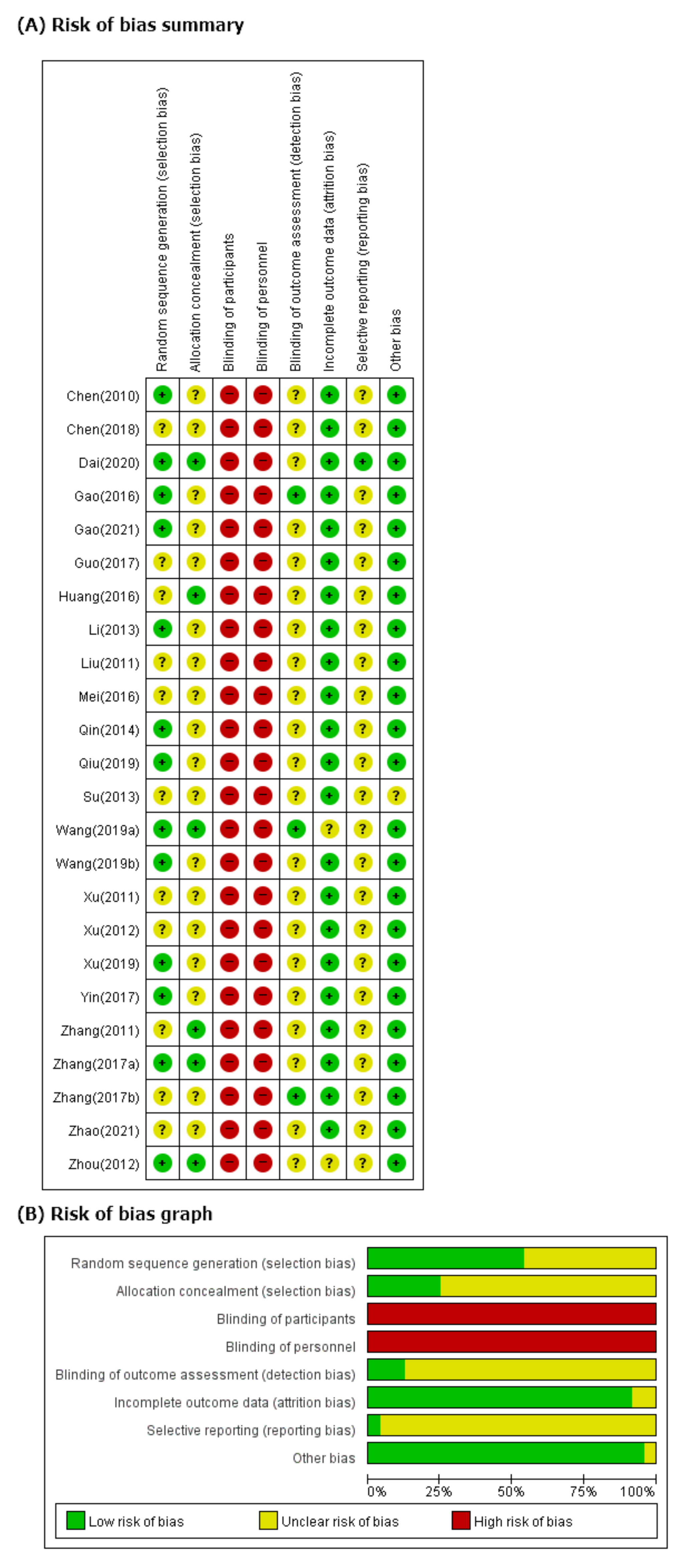
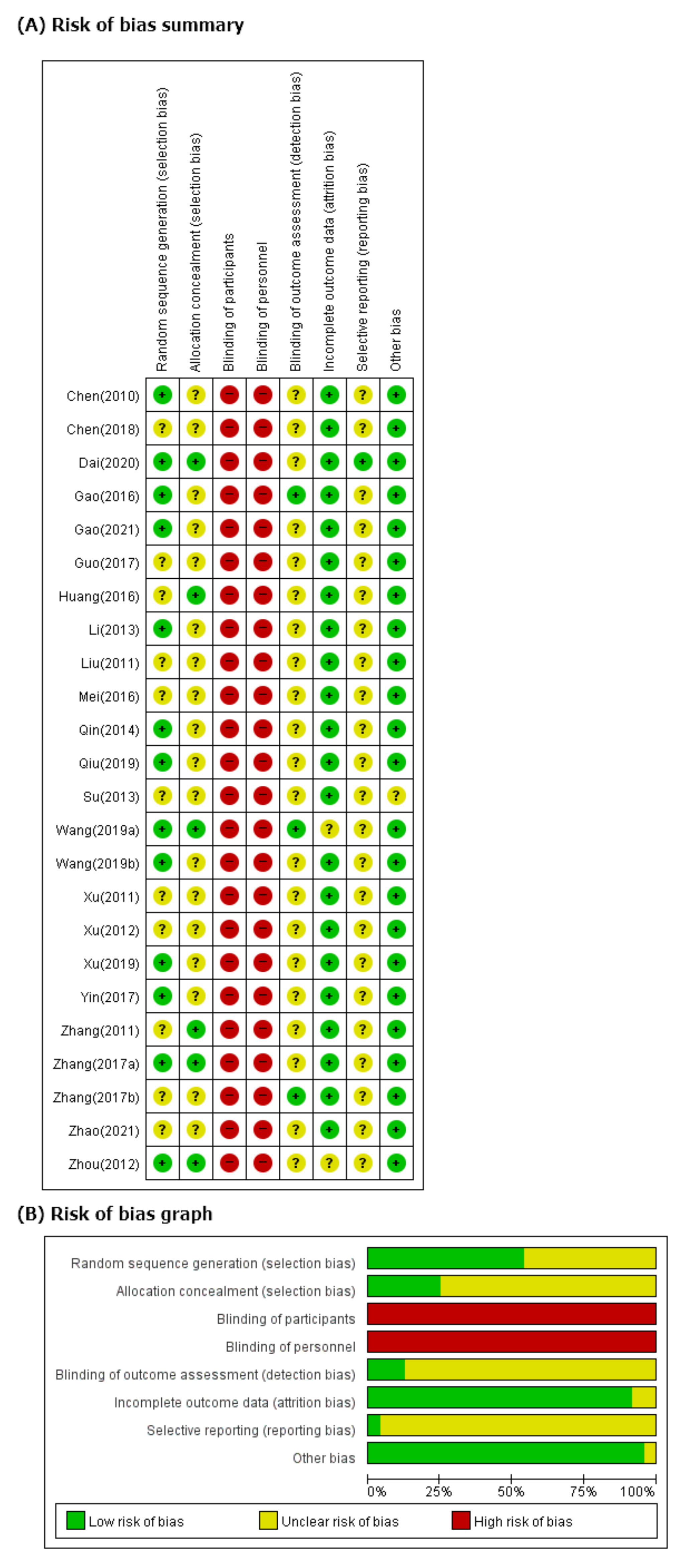
3.3. ROB in Studies
3.4. Effectiveness and Safety of HM
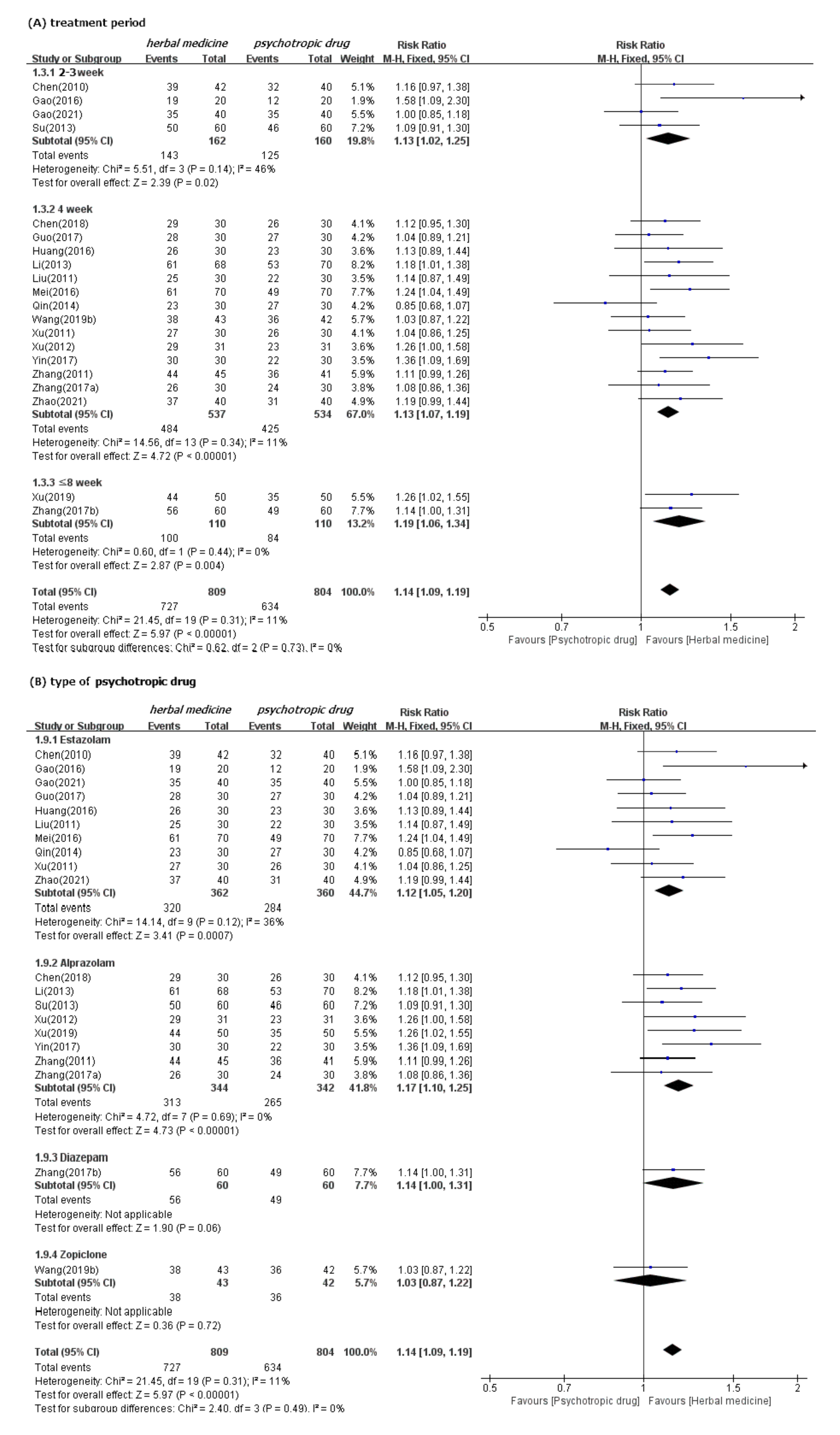
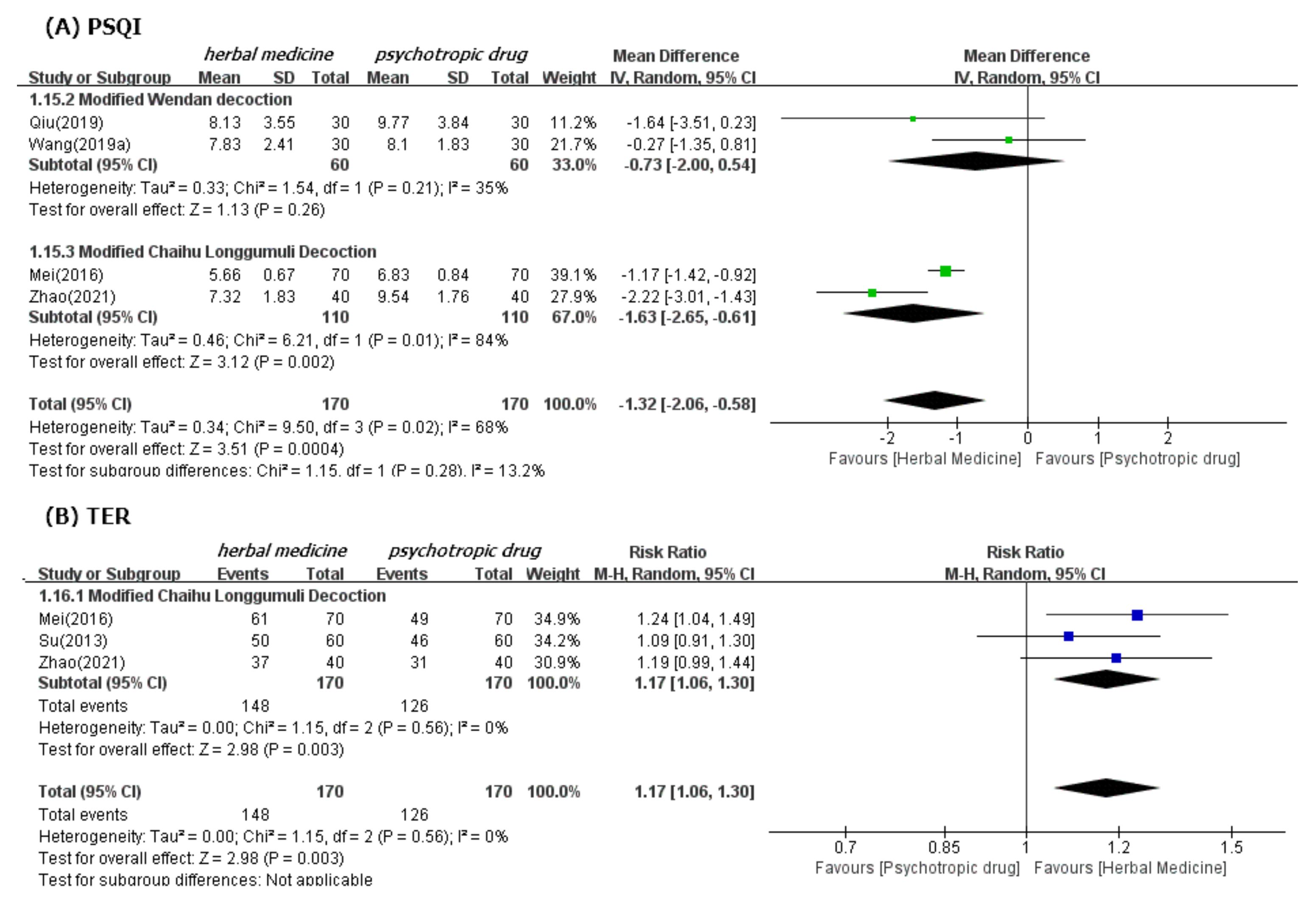
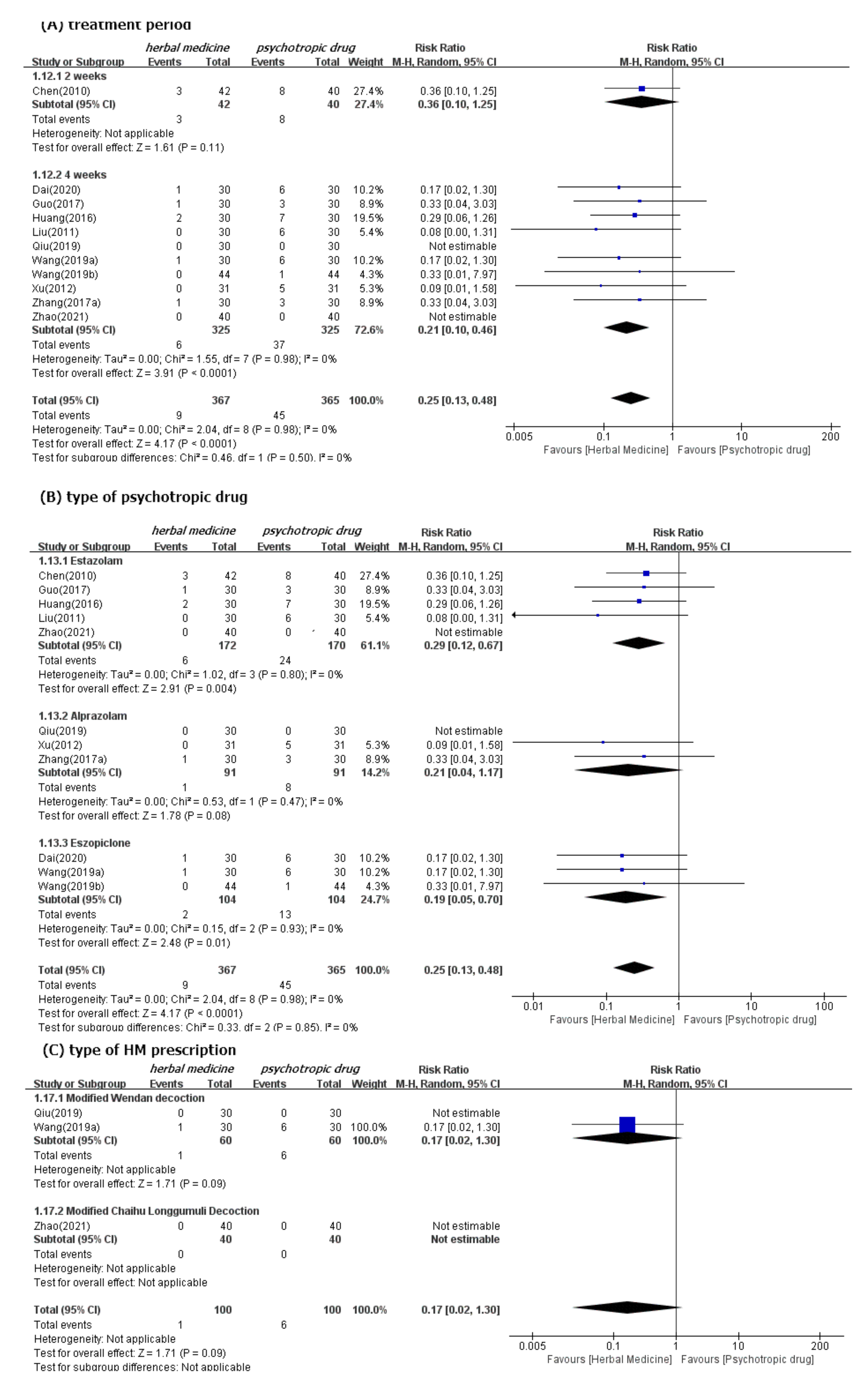
3.4.1. Effectiveness
3.4.2. Safety
3.5. Quality of Evidence
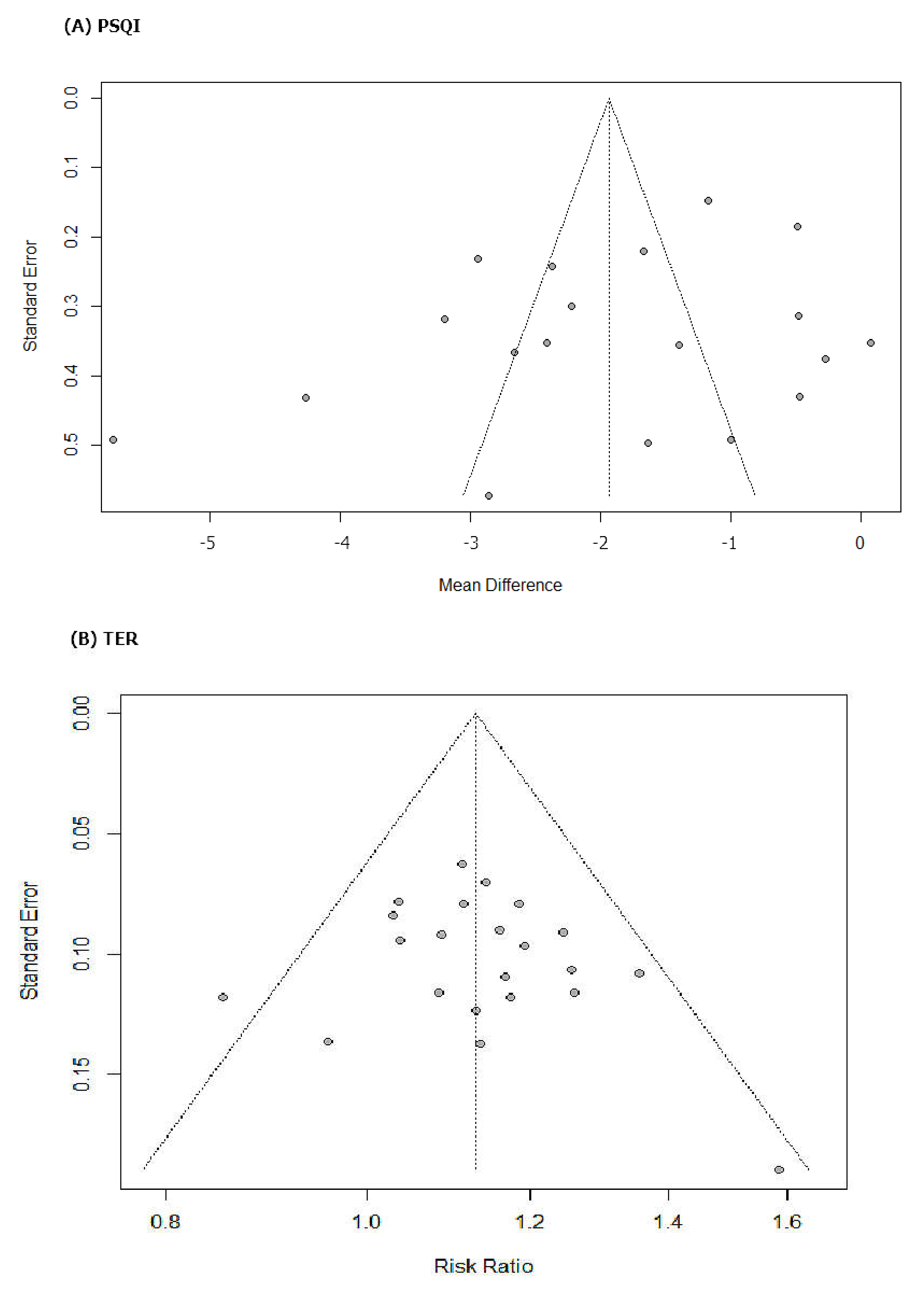
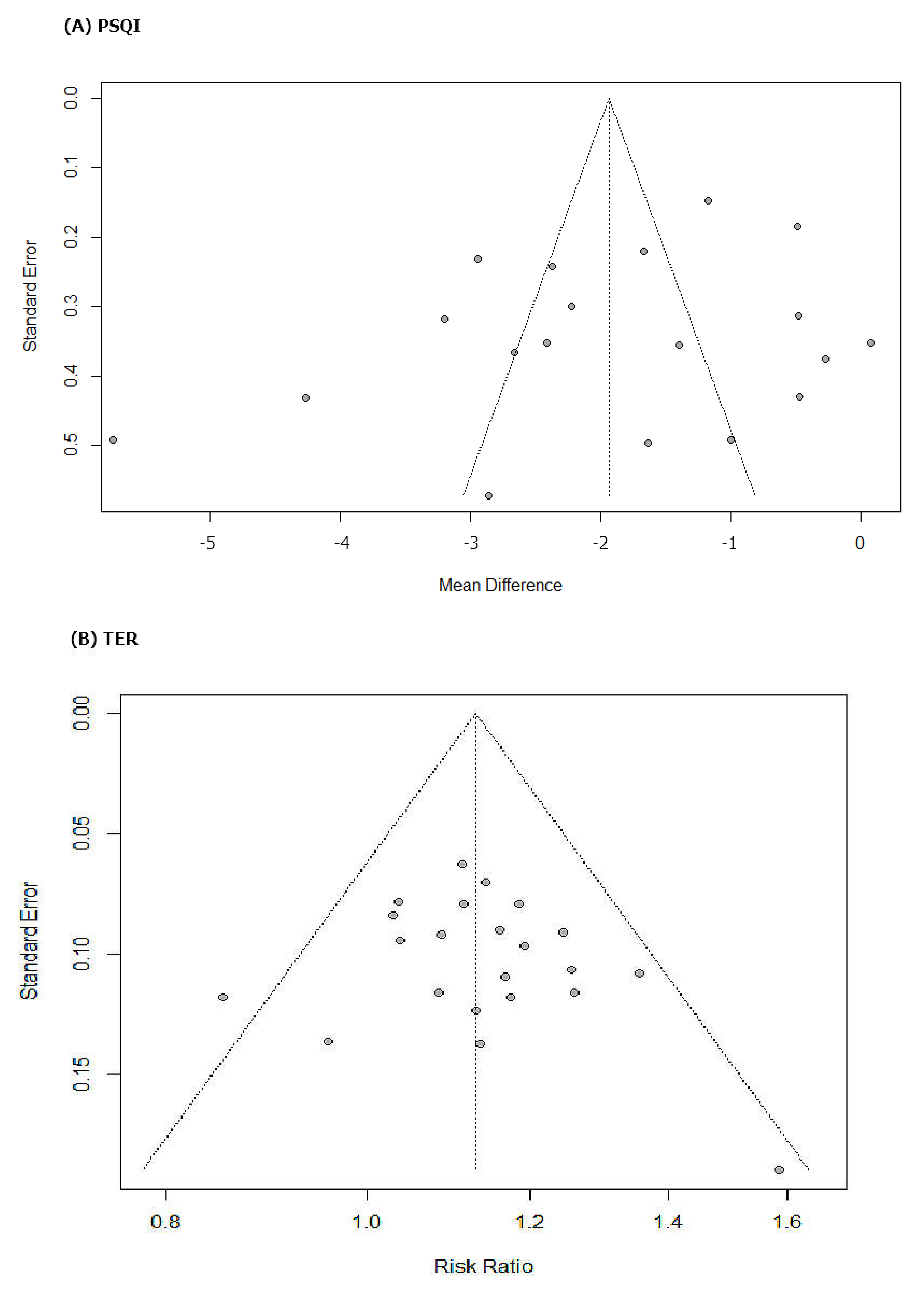
3.6. Publication Bias
4. Discussion
4.1. Summary of Evidence
4.2. Interpretation in Context of Previous Evidences
4.3. Clinical Implications
4.4. The Underlying Mechanism of HM
4.5. Strengths and Limitations
4.6. Implications for Future Research and Practice
5. Conclusions
Supplementary Materials
Author Contributions
Ethics and Dissemination
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- WHO. The Top 10 Causes of Death. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 30 January 2022).
- Benjamin, E.J.; Blaha, M.J.; Chiuve, S.E.; Cushman, M.; Das, S.R.; Deo, R.; de Ferranti, S.D.; Floyd, J.; Fornage, M.; Gillespie, C.; et al. Heart Disease and Stroke Statistics-2017 Update: A Report from the American Heart Association. Circulation 2017, 135, e146–e603. [Google Scholar] [CrossRef]
- Baylan, S.; Griffiths, S.; Grant, N.; Broomfield, N.M.; Evans, J.J.; Gardani, M. Incidence and prevalence of post-stroke insomnia: A systematic review and meta-analysis. Sleep Med. Rev. 2020, 49, 101222. [Google Scholar] [CrossRef] [PubMed]
- Hackett, M.L.; Pickles, K. Part I: Frequency of depression after stroke: An updated systematic review and meta-analysis of observational studies. Int. J. Stroke 2014, 9, 1017–1025. [Google Scholar] [CrossRef]
- Rafsten, L.; Danielsson, A.; Sunnerhagen, K.S. Anxiety after stroke: A systematic review and meta-analysis. J. Rehabil. Med. 2018, 50, 769–778. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association Publishing: Washington, DC, USA, 2013. [Google Scholar]
- Hasan, F.; Gordon, C.; Wu, D.; Huang, H.C.; Yuliana, L.T.; Susatia, B.; Marta, O.F.D.; Chiu, H.Y. Dynamic Prevalence of Sleep Disorders Following Stroke or Transient Ischemic Attack: Systematic Review and Meta-Analysis. Stroke 2021, 52, 655–663. [Google Scholar] [CrossRef]
- Zunzunegui, C.; Gao, B.; Cam, E.; Hodor, A.; Bassetti, C.L. Sleep disturbance impairs stroke recovery in the rat. Sleep 2011, 34, 1261–1269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moon, H.I.; Yoon, S.Y.; Jeong, Y.J.; Cho, T.H. Sleep disturbances negatively affect balance and gait function in post-stroke patients. NeuroRehabilitation 2018, 43, 211–218. [Google Scholar] [CrossRef]
- Joa, K.L.; Kim, W.H.; Choi, H.Y.; Park, C.H.; Kim, E.S.; Lee, S.J.; Kim, S.Y.; Ko, S.H.; Jung, H.Y. The Effect of Sleep Disturbances on the Functional Recovery of Rehabilitation Inpatients Following Mild and Moderate Stroke. Am. J. Phys. Med. Rehabil. 2017, 96, 734–740. [Google Scholar] [CrossRef]
- Glozier, N.; Moullaali, T.J.; Sivertsen, B.; Kim, D.; Mead, G.; Jan, S.; Li, Q.; Hackett, M.L. The Course and Impact of Poststroke Insomnia in Stroke Survivors Aged 18 to 65 Years: Results from the Psychosocial Outcomes in StrokE (POISE) Study. Cerebrovasc. Dis. Extra 2017, 7, 9–20. [Google Scholar] [CrossRef]
- Fulk, G.; Duncan, P.; Klingman, K.J. Sleep problems worsen health-related quality of life and participation during the first 12 months of stroke rehabilitation. Clin. Rehabil. 2020, 34, 1400–1408. [Google Scholar] [CrossRef]
- Tang, W.K.; Grace Lau, C.; Mok, V.; Ungvari, G.S.; Wong, K.S. Insomnia and health-related quality of life in stroke. Top. Stroke Rehabil. 2015, 22, 201–207. [Google Scholar] [CrossRef] [PubMed]
- Li, L.J.; Yang, Y.; Guan, B.Y.; Chen, Q.; Wang, A.X.; Wang, Y.J.; Zhang, N.; Wang, C.X. Insomnia is associated with increased mortality in patients with first-ever stroke: A 6-year follow-up in a Chinese cohort study. Stroke Vasc. Neurol. 2018, 3, 197–202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, W.K.; Lu, J.Y.; Liang, H.; Chan, T.T.; Mok, V.; Ungvari, G.S.; Wong, K.S. Is insomnia associated with suicidality in stroke? Arch. Phys. Med. Rehabil. 2011, 92, 2025–2027. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gottlieb, E.; Landau, E.; Baxter, H.; Werden, E.; Howard, M.E.; Brodtmann, A. The bidirectional impact of sleep and circadian rhythm dysfunction in human ischaemic stroke: A systematic review. Sleep Med. Rev. 2019, 45, 54–69. [Google Scholar] [CrossRef] [PubMed]
- Palomäki, H.; Berg, A.; Meririnne, E.; Kaste, M.; Lönnqvist, R.; Lehtihalmes, M.; Lönnqvist, J. Complaints of poststroke insomnia and its treatment with mianserin. Cerebrovasc. Dis. 2003, 15, 56–62. [Google Scholar] [CrossRef]
- Hiu, T.; Farzampour, Z.; Paz, J.T.; Wang, E.H.; Badgely, C.; Olson, A.; Micheva, K.D.; Wang, G.; Lemmens, R.; Tran, K.V.; et al. Enhanced phasic GABA inhibition during the repair phase of stroke: A novel therapeutic target. Brain 2016, 139, 468–480. [Google Scholar] [CrossRef] [Green Version]
- Oh, M.K.; Yoon, K.J.; Lee, Y.T.; Chae, S.W.; Choi, H.Y.; Shin, H.S.; Park, Y.H.; Chun, S.W.; Park, Y.S. Effect of zolpidem on functional recovery in a rat model of ischemic stroke. J. Int Med. Res. 2018, 46, 249–257. [Google Scholar] [CrossRef]
- Seibt, J.; Aton, S.J.; Jha, S.K.; Coleman, T.; Dumoulin, M.C.; Frank, M.G. The non-benzodiazepine hypnotic zolpidem impairs sleep-dependent cortical plasticity. Sleep 2008, 31, 1381–1391. [Google Scholar]
- Huang, W.S.; Tsai, C.H.; Lin, C.C.; Muo, C.H.; Sung, F.C.; Chang, Y.J.; Kao, C.H. Relationship between zolpidem use and stroke risk: A Taiwanese population-based case-control study. J. Clin. Psychiatry 2013, 74, e433–e438. [Google Scholar] [CrossRef]
- Brandt, J.; Leong, C. Benzodiazepines and Z-Drugs: An Updated Review of Major Adverse Outcomes Reported on in Epidemiologic Research. Drugs R D 2017, 17, 493–507. [Google Scholar] [CrossRef]
- Schifano, F.; Chiappini, S.; Corkery, J.M.; Guirguis, A. An Insight into Z-Drug Abuse and Dependence: An Examination of Reports to the European Medicines Agency Database of Suspected Adverse Drug Reactions. Int. J. Neuropsychopharmacol. 2019, 22, 270–277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qaseem, A.; Kansagara, D.; Forciea, M.A.; Cooke, M.; Denberg, T.D. Management of Chronic Insomnia Disorder in Adults: A Clinical Practice Guideline from the American College of Physicians. Ann. Intern. Med. 2016, 165, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Koffel, E.; Bramoweth, A.D.; Ulmer, C.S. Increasing access to and utilization of cognitive behavioral therapy for insomnia (CBT-I): A narrative review. J. Gen. Intern. Med. 2018, 33, 955–962. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herron, K.; Farquharson, L.; Wroe, A.; Sterr, A. Development and Evaluation of a Cognitive Behavioural Intervention for Chronic Post-Stroke Insomnia. Behav. Cogn. Psychother. 2018, 46, 641–660. [Google Scholar] [CrossRef] [PubMed]
- Frass, M.; Strassl, R.P.; Friehs, H.; Müllner, M.; Kundi, M.; Kaye, A.D. Use and acceptance of complementary and alternative medicine among the general population and medical personnel: A systematic review. Ochsner J. 2012, 12, 45–56. [Google Scholar]
- Ng, J.Y.; Parakh, N.D. A systematic review and quality assessment of complementary and alternative medicine recommendations in insomnia clinical practice guidelines. BMC Complement. Med. Ther. 2021, 21, 54. [Google Scholar] [CrossRef]
- Oña, G.; Bouso, J.C. Therapeutic Potential of Natural Psychoactive Drugs for Central Nervous System Disorders: A Perspective from Polypharmacology. Curr. Med. Chem. 2021, 28, 53–68. [Google Scholar] [CrossRef]
- Zhang, H.; Liu, P.; Wu, X.; Zhang, Y.; Cong, D. Effectiveness of Chinese herbal medicine for patients with primary insomnia: A PRISMA-compliant meta-analysis. Medicine 2019, 98, e15967. [Google Scholar] [CrossRef]
- Wang, J.; Wang, Z.; Wang, X.; Du, G.; Zheng, B.; Li, Y.; Wang, Q. Combination of Alprazolam and Bailemian Capsule Improves the Sleep Quality in Patients with Post-Stroke Insomnia: A Retrospective Study. Front. Psychiatry 2019, 10, 411. [Google Scholar] [CrossRef]
- Zeng, L.F.Z.Y.; Huang, X.T.; Mi, S.Q.; Kong, L.S.; Wang, Q.; Wang, N.S. Systematic review on clinical efficacy and safety of TCM for post-stroke sleep disorders. China J. Tradit. Chin. Med. Pharm. 2015, 30, 1488–1498. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Backhaus, J.; Junghanns, K.; Broocks, A.; Riemann, D.; Hohagen, F. Test–retest reliability and validity of the Pittsburgh Sleep Quality Index in primary insomnia. J. Psychosom. Res. 2002, 53, 737–740. [Google Scholar] [CrossRef]
- Higgins, J.; Altman, D. Chapter 8: Assessing risk of bias in included studies. In Cochrane Handbook for Systematic Reviews of Interventions, Version 5.1.0; Higgins, J.P.T., Green, S., Eds.; The Cochrane Collaboration: London, UK, 2011; pp. 187–241. [Google Scholar]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- Schünemann, H.J.; Oxman, A.D.; Brozek, J.; Glasziou, P.; Jaeschke, R.; Vist, G.E.; Williams, J.W., Jr.; Kunz, R.; Craig, J.; Montori, V.M.; et al. Grading quality of evidence and strength of recommendations for diagnostic tests and strategies. BMJ 2008, 336, 1106–1110. [Google Scholar] [CrossRef] [Green Version]
- Chen, K.J. Bailemian Capsule in the Treatment of 42 Cases of Post-stroke Insomnia. Hunan J. Tradit. Chin. Med. 2010, 26, 45–46. [Google Scholar]
- Chen, X.F. Observation on Clinical Curative Effect of Modified Buyang Huanwu Decoction in Treating Insomnia of Syndrome of Blood Stasis due to Qi Deficiency after Stroke in the Elderly. Master’s Thesis, Hunan University of Traditional Chinese Medicine, Changsha, China, 2018. [Google Scholar]
- Dai, N.; Li, Y.; Sun, J.; Li, F.; Xiong, H. Self-Designed Ningxin Anshen Formula for Treatment of Post-ischemic Stroke Insomnia: A Randomized Controlled Trial. Front. Neurol. 2020, 11, 537402. [Google Scholar] [CrossRef]
- Gao, X.; Zhang, H.; Chai, J.B.; Zhao, Y.P.; Yu, M.; Zhao, Y.H. Clinical observation of the effect of Yudian Decoction on the treatment of 20 cases of insomnia induced by ischemic stroke with syndrome of the phlegm-heat. China J. Tradit. Chin. Med. Pharm. 2016, 31, 729–730. [Google Scholar]
- Gao, Y.D.; Huang, J.S.; Yin, L.F.; Liang, C.; Lin, W.Z. A Randomized Controlled Trial of Diurnal and Diurnal Treatment for Insomnia after Stroke. World J. Sleep Med. 2021, 8, 570–572. [Google Scholar]
- Guo, H.R. Effect of Chaiqin Wendan Decoction on Insomnia after Ischemic Stroke (Liver and Phlegm Heat Type) Clinical Study. Master’s Thesis, Henan University of Traditional Chinese Medicine, Zhengzhou, China, 2017. [Google Scholar]
- Huang, Y.C.; Cao, X. Clinical observation on treating insomnia following stroke with the Suanzaoren decoction. Clin. J. Chin. Med. 2016, 8, 97–98. [Google Scholar]
- Li, Y.H.; Qin, J.L.; Li, N.; Wang, M.S.; Qi, F.Y. Treatment of 68 Cases of Insomnia after Stroke by Zhuyu Anshen Decoction. Chin. J. Integr. Med. Cardio Cerebrovasc. Dis. 2013, 11, 828–829. [Google Scholar]
- Liu, F.X. Clinical Observation of Xuefu Zhuyu Decoction on 30 Cases of Post-stroke Insomnia of Blood Stasis Type. Master’s Thesis, Guangxi University of Traditional Chinese Medicine, Nanning, China, 2011. [Google Scholar]
- Mei, S.Y. Clinical Observation of 36 Cases of Insomnia after Stroke Treated by Modified Bupleurum Falcatum plus Dragon Bone and Oyster Shell Decodtion. Front. Med. 2016, 6, 348–349. [Google Scholar]
- Qin, X.Y.; Dai, X.Y.; Fang, T.X.; Hong, T. Clinical Observation of Self-made Chinese Herbal Decoction in Improving Insomnia after Stroke. Chin. J. Tradit. Med Sci. Technol. 2014, 21, 573–574. [Google Scholar]
- Qiu, W.J. Clinical study of Changzhi Huanglian Wendan Decoction in the treatment of Insomnia with Phlegm-heat Internal Disturbance Syndrome after Ischemic Stroke. Master’s Thesis, Shandong University of Traditional Chinese Medicine, Jinan, China, 2019. [Google Scholar]
- Su, C.J.; Ren, R.M.; Song, L.Q. Chaihu Longmu Pills in Treating Insomnia after Ischemic Stroke. Guangming J. Chin. Med. 2013, 28, 943–944. [Google Scholar] [CrossRef]
- Wang, Y.Q. Clinical Study on the Treatment of Sleep Disorders after Acute Cerebral Infarction Based on the Method of Clearing Heat and Resolving Phlegm. Master’s Thesis, Beijing University of Chinese Medicine, Beijing, China, 2019. [Google Scholar]
- Wang, Y.X. Clinical Study of Jiawei Jiaotai Decoction in the Treatment of Insomnia after Heart-Kidney Disjunction Stroke. Master’s Thesis, Hubei University of Traditional Chinese Medicine, Wuhan, China, 2019. [Google Scholar]
- Xu, J.P.; Li, R.P. Clinical Observation of Traditional Chinese Medicine Xinlekang in Treating Post-stroke Insomnia. Nei Mongol J. Tradit. Chin. Med. 2012, 31, 23–24. [Google Scholar]
- Xu, W.J.; Jiang, R.C.; Zhou, Y.X.; Qin, Y. Clinical Study on Professor Wang Qiaochu’s Experienced Decoction in Treating Post-stroke Insomnia with Liver Depression and Stasis. Shaanxi Tradit. Chin. Med. 2019, 40, 867–870. [Google Scholar]
- Xu, Y. Clinical Observation on the Treatment of Insomnia after Ischemic Stroke (Kidney Yin Deficiency and Blood Stasis Type) by Tonifying Kidney and Activating Blood. Master’s Thesis, Heilongjiang University of Traditional Chinese Medicine, Harbin, China, 2011. [Google Scholar]
- Yin, S. Treatment of 30 Cases of Insomnia after Ischemic Stroke with Kidney Yin Deficiency and Blood Stasis Type by Tonifying Kidney and Activating Blood. Tradit. Chin. Med. Res. 2017, 30, 28–30. [Google Scholar]
- Zhang, C.Q. Clinical Observation of Guben Jiannao Liquid in Treating Stroke Accompanied by Insomnia. Sichuan Tradit. Chin. Med. 2011, 29, 82–83. [Google Scholar]
- Zhang, J.H. Clinical Observation of Tongluo Yisui Method on Insomnia after Ischemic Stroke. In Proceedings of the Specially Invited Cardiovascular Experts Academic Symposium, Beijing, China; 2017; pp. 88–89. [Google Scholar]
- Zhang, Y.Y. Clinical Observation of Insomnia Granules in Treating Post-stroke Insomnia (Liver Heart Disturbance Type). Master’s Thesis, Shaanxi University of Traditional Chinese Medicine, Xianyang, China, 2017. [Google Scholar]
- Zhao, D.Z. Effect of Chaishaolongmu Decoction on Treating Insomnia after Cerebral Apoplexy with Liver Stagnation and Blood Deficiency. Chin. J. Integr. Med. Cardio Cerebrovasc. Dis. 2021, 19, 1381–1384. [Google Scholar]
- Zhou, J.; Yu, J. Treating 60 Cases of Sleep Disturbance after Cerebral Apoplexy with Yangxin Decoction. Shanxi Tradit. Chin. Med. 2012, 28, 20–21. [Google Scholar]
- Li, J.G.; Xu, H. Incorporating pattern identification of Chinese medicine into precision medicine: An integrative model for individualized medicine. Chin. J. Integr Med. 2015, 21, 807–810. [Google Scholar] [CrossRef]
- Ni, X.; Shergis, J.L.; Guo, X.; Zhang, A.L.; Li, Y.; Lu, C.; Xue, C.C. Updated clinical evidence of Chinese herbal medicine for insomnia: A systematic review and meta-analysis of randomized controlled trials. Sleep Med. 2015, 16, 1462–1481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, M.; Morin, C.M.; Schaefer, K.; Wallenstein, G.V. Interpreting score differences in the Insomnia Severity Index: Using health-related outcomes to define the minimally important difference. Curr. Med. Res. Opin. 2009, 25, 2487–2494. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Ju, J.; Li, J.; Fan, Y.; Xu, H. Chaihu Longgu Muli decoction, a Chinese herbal formula, for the treatment of insomnia: A systematic review and meta-analysis. Medicine 2020, 99, e22462. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Teng, J.; Wang, W.; Yang, N.; Tian, H.; Zhang, W.; Peng, X.; Zhang, J. Clinical efficacy and safety of traditional Chinese medicine Xiao Yao San in insomnia combined with anxiety. Medicine 2021, 100, e27608. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Yang, Y.; Ding, X.; Li, J.; Zhou, X.; Teng, J.; Qi, X. Efficacy and safety of Shumian capsules in treating insomnia: A systematic review and meta-analysis. Medicine 2021, 100, e28194. [Google Scholar] [CrossRef]
- Lin, Y.H.; Chen, C.; Zhao, X.; Mao, Y.F.; Xiang, G.X.; Yang, M.Q.; Song, Y.M. Efficacy and Safety of Banxia Formulae for Insomnia: A Systematic Review and Meta-Analysis of High-Quality Randomized Controlled Trials. Evid Based Complement. Alternat. Med. 2021, 2021, 8833168. [Google Scholar] [CrossRef]
- Kim, E.; Lee, J.H.; Lee, D.H. Zolpidem as a high risk factor for elderly suicide in South Korea. Arch. Suicide Res. 2020, 1–15. [Google Scholar] [CrossRef]
- Taipale, H.; Tolppanen, A.-M.; Koponen, M.; Tanskanen, A.; Lavikainen, P.; Sund, R.; Tiihonen, J.; Hartikainen, S. Risk of pneumonia associated with incident benzodiazepine use among community-dwelling adults with Alzheimer disease. Can. Med Assoc. J. 2017, 189, E519–E529. [Google Scholar] [CrossRef] [Green Version]
- Torres-Bondia, F.; Dakterzada, F.; Galván, L.; Buti, M.; Besanson, G.; Grill, E.; Buil, R.; de Batlle, J.; Piñol-Ripoll, G. Benzodiazepine and Z-drug use and the risk of developing dementia. Int. J. Neuropsychopharmacol. 2021, 2021, pyab073. [Google Scholar] [CrossRef]
- Treves, N.; Perlman, A.; Kolenberg Geron, L.; Asaly, A.; Matok, I. Z-drugs and risk for falls and fractures in older adults—a systematic review and meta-analysis. Age Ageing 2017, 47, 201–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, R.; Guo, X.; Li, J.; You, Q.; Zhang, S. Effect of Suanzaoren decoction on hypothalamus GABA expression and receptors of chronic sleep deprivation senile insomnia rats. Liaoning J. Tradit. Chin. Med. 2018, 45, 845–847. [Google Scholar]
- Zhang, F.; Ran, R.; Zhao, B. Effect of Suanzaoren decoction on expression of circadian genes Clock and Bmal1 in the suprachiasmatic nucleus. J. Hunan Univ. Chin. Med. 2019, 39, 19–22. [Google Scholar]
- Ou, B.Y.; Li, Y.; Yang, Z.M.; Xu, B.Y. Mechanism of Bupleurum Falcatum Plus Dragon Bone and Oyster Shell Decoction (CJLM) on insomnia. Lishizhen Med. Mater. Med. Res. 2010, 21, 1887–1888. [Google Scholar]
- Li, Z.H.; Ma, P.K.; Huang, Y.F.; Zhang, Z.; Zheng, W.; Chen, J.H.; Guo, C.E.; Chen, N.; Bi, X.N.; Zhang, Y.J. Jiaotai Pill Alleviates Insomnia through Regulating Monoamine and Organic Cation Transporters in Rats. Chin. J. Integr. Med. 2021, 27, 183–191. [Google Scholar] [CrossRef]
- Su, H.; Zhang, C.; Zou, X.; Lu, F.; Zeng, Y.; Guan, H.; Ren, Y.; Yuan, F.; Xu, L.; Zhang, M.; et al. Jiao-tai-wan inhibits inflammation of the gut-brain-axis and attenuates cognitive impairment in insomnic rats. J. Ethnopharmacol. 2020, 250, 112478. [Google Scholar] [CrossRef]
- Shergis, J.L.; Ni, X.; Sarris, J.; Zhang, A.L.; Guo, X.; Xue, C.C.; Lu, C.; Hugel, H. Ziziphus spinosa seeds for insomnia: A review of chemistry and psychopharmacology. Phytomedicine 2017, 34, 38–43. [Google Scholar] [CrossRef]
- Fang, X.; Hao, J.F.; Zhou, H.Y.; Zhu, L.X.; Wang, J.H.; Song, F.Q. Pharmacological studies on the sedative-hypnotic effect of Semen Ziziphi spinosae (Suanzaoren) and Radix et Rhizoma Salviae miltiorrhizae (Danshen) extracts and the synergistic effect of their combinations. Phytomedicine 2010, 17, 75–80. [Google Scholar] [CrossRef]
- Luo, H.; Sun, S.J.; Wang, Y.; Wang, Y.L. Revealing the sedative-hypnotic effect of the extracts of herb pair Semen Ziziphi spinosae and Radix Polygalae and related mechanisms through experiments and metabolomics approach. BMC Complement. Med. Ther. 2020, 20, 206. [Google Scholar] [CrossRef]
- Shah, V.K.; Choi, J.J.; Han, J.Y.; Lee, M.K.; Hong, J.T.; Oh, K.W. Pachymic Acid Enhances Pentobarbital-Induced Sleeping Behaviors via GABAA-ergic Systems in Mice. Biomol. Ther. 2014, 22, 314–320. [Google Scholar] [CrossRef] [Green Version]
- Liao, J.F.; Huang, S.Y.; Jan, Y.M.; Yu, L.L.; Chen, C.F. Central inhibitory effects of water extract of Acori graminei rhizoma in mice. J. Ethnopharmacol. 1998, 61, 185–193. [Google Scholar] [CrossRef]
- Zhong, Y.H.; Jiang, S.; Qu, W.M.; Zhang, W.; Huang, Z.L.; Chen, C.R. Saikosaponin a promotes sleep by decreasing neuronal activities in the lateral hypothalamus. J. Sleep Res. 2021, e13484. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Q.H.; Zhou, X.L.; Xu, M.B.; Jin, T.Y.; Rong, P.Q.; Zheng, G.Q.; Lin, Y. Suanzaoren Formulae for Insomnia: Updated Clinical Evidence and Possible Mechanisms. Front. Pharmacol. 2018, 9, 76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeng, C.; Liu, X.; Hu, L.; Feng, Y.; Xia, N.; Zeng, H.; Luo, L.; Ye, R.; Yuan, Z. Jiao-tai-wan for insomnia symptoms caused by the disharmony of the heart and kidney: A study protocol for a randomized, double-blind, placebo-controlled trial. Trials 2020, 21, 408. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author (year) | Sample Size (Intervention:Control) (Included →Analyzed) | Mean Age (Range) (Years) | Diagnostic Tool for PSI (Severity Criteria for Inclusion)/Stroke Type (Inclusion Criteria) | Pattern Identification | (A) Treatment Intervention | (B) Control Intervention | Treatment Duration/Follow-Up | Outcome and Results (Post-Treatment) | Adverse Events |
|---|---|---|---|---|---|---|---|---|---|
| Chen (2010) [39] | 82 (42:40)→82 (42:40) | (A) 58.79 ± 7.83 (B) 59.87 ± 8.32 | DSM-IV/ Stroke (MRI/CT) | NA | HM | Estazolam 1 mg/day | 3 weeks | ① PSQI: (A) > (B) * ② TER: (A) > (B) * | (A) 3 cases (nausea & upper abdomen discomfort) (B): 8 cases (dizziness 3, sleepiness 5) |
| Chen (2018) [40] | 60 (30:30)→60 (30:30) | (A) 72.43 ± 6.36 (B) 73.13 ± 7.11 | CCMD-3 (PSQI > 7)/ Cerebral infarction or hemorrhage (MRI/CT) | Blood stasis due to qi deficiency | HM, RCS | Alprazolam 0.4 mg/day, RCS | 4 weeks | ① PSQI: (A) > (B) * ② TER: (A) > (B)+ ③ TCM symptom score: (A) > (B)+ | NR |
| Dai (2020) [41] | 60 (30:30:30)→60 (30:30:30) | (A) 59.87 ± 8.32 (B)−1 60.47 ± 9.21 (B)−2 59.10 ± 8.77 | DSM-5 (PSQI > 7)/ Cerebral infarction (MRI/CT) | Blood deficiency and liver-heat syndrome | HM | (B)-1 Zopiclone 3.75–7.5 mg/day, (B)-2 Placebo twice/day | 4 weeks | ① PSQI: (A) > (B)+ ② ISI: (A) > (B)+ | (A): 1 case (dispepsia) (B): 6 cases (fatigue 4, nausea 2) |
| Gao (2016) [42] | 40 (20:20)→40 (20:20) | (A) 61.50 ± 7.25 (B) 59.90 ± 8.72 | CCMD-3 (PSQI > 16)/ Cerebral infarction (MRI/CT) | Internal harassment of phlegm-heat | HM | Estazolam 2 mg/day | 2 weeks | ① PSQI: (A) > (B)+ ② TER: (A) > (B) * | NR |
| Gao (2021) [43] | 80 (40:40)→80 (40:40) | NR NR | GDTICA/ Stroke (GCTNCM) | NA | HM | Estazolam 1 mg/day | 2 weeks | ① PSQI: (A) > (B) * ② TER: (A) > (B) * ③ ISI: (A) > (B) * | NR |
| Guo (2017) [44] | 60 (30:30)→60 (30:30) | (A) 64.8 ± 7.6 (B) 62 ± 8.9 | GDTICA/ Cerebral infarction (MRI/CT) | Liver stagnation and phlegm-heat | HM, RCS | Estazolam 1 mg/day, RCS | 4 weeks/4 weeks | ① PSQI: (A) > (B)+ ② TER: (A) > (B) * | (A): 1 case (diarrhea) (B): 3 cases (fatigue 2, dry mouth 1) |
| Huang (2016) [45] | 60 (30:30)→60 (30:30) | (A) 61.4 ± 2.72 (B) 62.39 ± 3.51 | CCMD-3/ Stroke (MRI/CT) | NA | HM | Estazolam 1 mg/day | 4 weeks | ① TER: (A) > (B) * | (A): 2 cases(stomach discomfort) (B): 7 cases (dizziness & fatigue 3, sleepiness 4) |
| Li (2013) [46] | 138 (68:70)→138 (68:70) | (A) 69.8 ± NR (B) 67.9 ± NR | CCMD-3 (AIS > 6)/ Cerebral infarction (MRI/CT) | NA | HM, RCS | Alprazolam 0.4–0.8 mg/day, RCS | 4 weeks | ① TER: (A) > (B) * ② AIS: (A) > (B) * | NR |
| Liu (2011) [47] | 60 (30:30)→60 (30:30) | (A) 66.57 ± 7.186 (B) 65.80 ± 5.845 | CCMD-3/ Cerebral infarction or hemorrhage (MRI/CT) | Blood stasis | HM | Estazolam 2 mg/day | 4 weeks | ① PSQI: (A) > (B) * ② TER: (A) > (B)* | (A): none (B): 6 cases (dry mouse 4, headache 2) |
| Mei (2016) [48] | 140 (70:70)→140 (70:70) | (A) 66.3 ± 6.4 (B) 65.8 ± 7.7 | GDTICA/ Cerebral infarction (MRI/CT) | NA | HM | Estazolam 1 mg/day | 4 weeks | ① PSQI: (A) > (B)+ ② TER: (A) > (B)+ | NR |
| Qin (2014) [49] | 60 (30:30)→60 (30:30) | (A) 62.3 ± 10.53 (B) 63.85 ± 9.78 | CCMD-3, ICD-10/ Cerebral infarction or hemorrhage (MRI/CT) | NA | HM, RCS | Estazolam 1–2 mg/day, RCS | 4 weeks | ① PSQI: (A) > (B) * ② TER: (A) > (B)* | NR |
| Qiu (2019) [50] | 60 (30:30)→60 (30:30) | (A) 62.57 ± 6.40 (B) 61.07 ± 7.52 | GDTICA/ Cerebral infarction (MRI/CT) | Internal harassment of phlegm-heat | HM, RCS | Alprazolam 0.4 mg/day, RCS | 4 weeks | ① PSQI: (A) > (B) * | none (B): none |
| Su (2013) [51] | 120 (60:60)→120 (60:60) | (A) NR (B) NR | CCMD-3/ Cerebral infarction (MRI/CT) | NA | HM, RCS | Alprazolam 1 mg/day, RCS | 2 weeks | ① TER: (A) > (B) * | NR |
| Wang (2019a) [52] | 60 (30:30)→NR | (A) 60.67 ± 8.63 (B) 61 ± 8.67 | CCMD-3/ Cerebral infarction (MRI/CT) | Internal harassment of phlegm-heat | HM, RCS | Zopiclone 7.5 mg/day, RCS | 4 weeks | ① PSQI: N.S ② PSG: N.S (all parameters)③ TCM symptom score: (A) > (B)+ | (A): none(B): 1 case (sleepiness) |
| Wang (2019b) [53] | 88 (44:44)→85 (43:42) | (A) 61.89 ± 8.56 (B) 62.02 ± 6.31 | CCMD-3/ Cerebral infarction or hemorrhage (MRI/CT) | Heart-kidney non-interaction | HM, RCS | Zopiclone 3 mg/day, RCS | 4 weeks | ① PSQI: N.S② TER: N.S③ TCM symptom score: (A) > (B) * | (A): 1 case (diarrhea) (B): 6 cases (dry mouse 4, headache 2) |
| Xu (2011) [54] | 60 (30:30)→60 (30:30) 30 | (A) 66.1 ± 7.8 (B) 65.8 ± 7.2 | DSM(PSQI > 7)/ Cerebral infarction (MRI/CT) | Kidney yin deficiency and blood stasis | HM, RCS | Estazolam 1 mg/day, RCS | 4 weeks | ① PSQI: N.S② TER: N.S ③ TCM symptom score: (A) > (B) * | TESS: (A) > (B)* |
| Xu (2012) [55] | 62 (31:31)→62 (31:31) | (A) 72.2 ± 4.8 (B) 70.2 ± 3.9 | CCMD-3 (PSQI > 7)/ Cerebral infarction(MRI/CT) | NA | HM, RCS | Alprazolam 0.8 mg/day, RCS | 4 weeks | ① PSQI: (A) > (B)+ ② TER: (A) > (B) * | (A): none (B): 5 cases (dizziness) |
| Xu (2019) [56] | 100 (50:50)→100 (50:50) | (A) 66.32 ±4.37 (B) 66.67 ± 4.42 | CCMD-3(SSQ > 12)/ Cerebral infarction (MRI/CT) | Liver stagnation and blood stasis | HM, RCS | Alprazolam 1mg/day, RCS | 12 weeks | ① PSQI: (A) > (B) * ② TER: (A) > (B) * ③ SSQ: (A) > (B) * | NR |
| Yin (2017) [57] | 60 (30:30)→60 (30:30) | (A) 64.2 ± 6.3 (B) 62.8 ± 6.9 | GPCRNDTCM/ Cerebral infarction or hemorrhage (MRI/CT) | Kidney yin deficiency and blood stasis | HM, RCS | Alprazolam 2 mg/day, RCS | 4 weeks | ① PSQI: (A) > (B)+ ② TER: (A) > (B) * | NR |
| Zhang (2011) [58] | 86 (45:41)→86 (45:41) | (A) NR (B) NR | CCMD-3/ Cerebral infarction or hemorrhage (MRI/CT) | NA | HM | Alprazolam 0.4 mg/day | 4 weeks | ① TER: (A) > (B) * | NR |
| Zhang (2017a) [60] | 64 (32:32)→60 (30:30) | (A) 53.50 ±9.52 (B) 54.10 ± 9.78 | GDTICA (PSQI > 7)/ Cerebral infarction or hemorrhage (MRI/CT) | Disturbing heart due to liver burning | HM, RCS | Alprazolam 0.5–1.5 mg/day, RCS | 4 weeks | ① PSQI: (A) > (B) * ② TER: N.S③ TCM symptom score: (A) > (B) * | (A): 1 case (stomach discomfort) (B): 3 cases (dizziness 2, fatigue 1) |
| Zhang (2017b) [59] | 120 (60:60)→120 (60:60) | (A) NR (B) NR | ICSD-2/ Cerebral infarction (MRI/CT) | NA | HM | Diazepam 5~10 mg/day | 8 weeks | ① TER: (A) > (B) * | NR |
| Zhao (2021) [61] | 80 (40:40)→80 (40:40) | (A) 52.7 ± 6.1 (B) 53.5 ± 5.9 | DSM-5/ Cerebral infarction or hemorrhage (MRI/CT) | Liver stagnation and blood deficiency | HM | Estazolam 1 mg/day | 4 weeks/4 weeks | ① PSQI: (A) > (B) * PSQI(f/u): (A) > (B) * ② TER: (A) > (B) * ③ SS-QOL: A) > (B) * SS-QOL (f/u): (A) > (B) * | none (B): none |
| Zhou (2012) [62] | 142 (60:62)→NR | (A) 60.19 ± 4.80 (B) 59.72 ± 10.71 | CCMD-3/ Cerebral infarction or hemorrhage (MRI/CT) | NA | HM | Diazepam 2 mg/day | 4 weeks/4 weeks | ① PSQI: N.S PSQI (f/u): (A) > (B) * | NR |
| Outcomes | No. Participants (RCTs) | Anticipated Absolute Effects (95% CI) | Quality of Evidence (GRADE) | ||
|---|---|---|---|---|---|
| Risk with Pharmacotherapy | Risk with Herbal Medicine | ||||
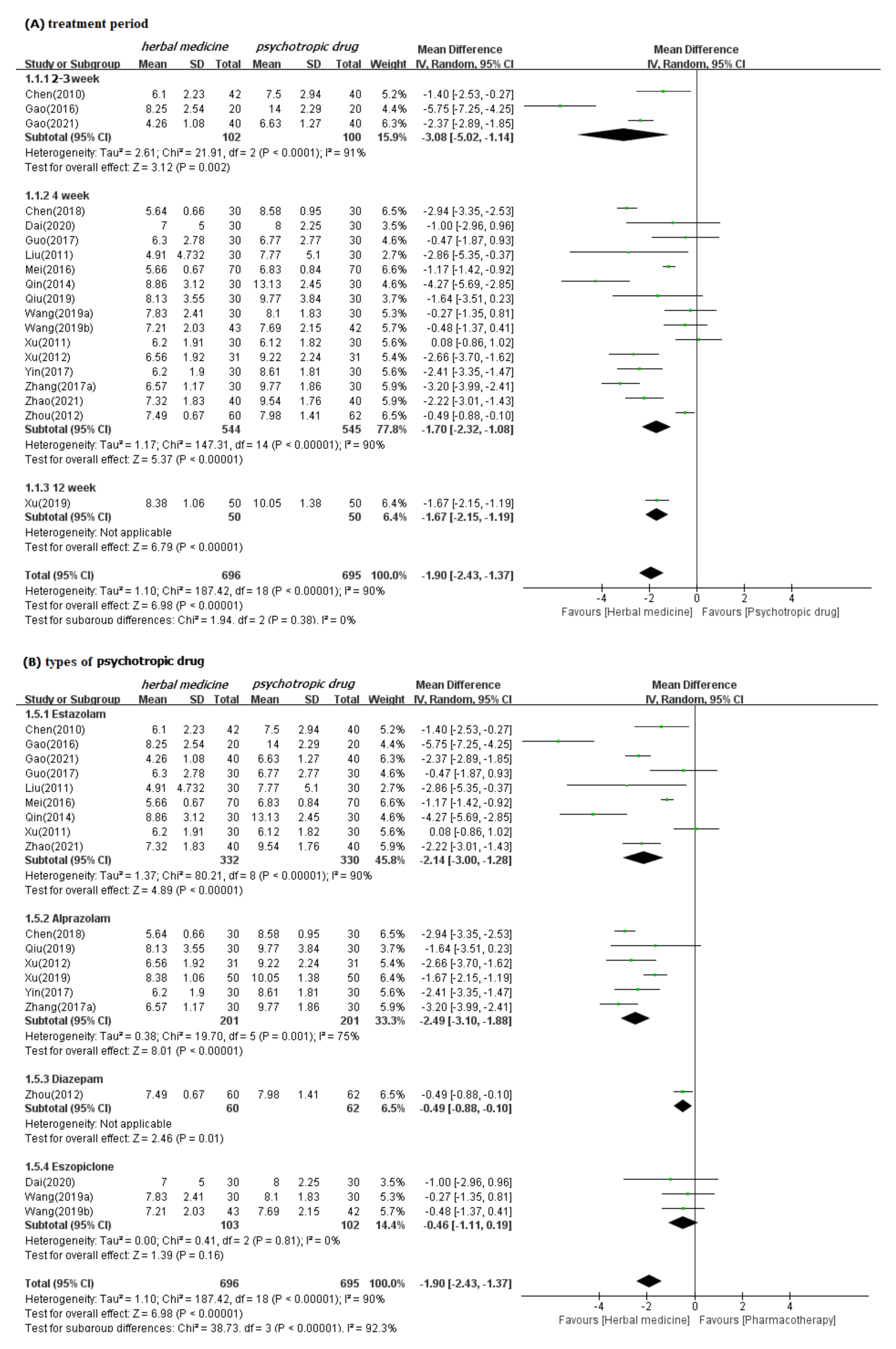
| PSQI | Total | 1391 (19) | - | MD 1.9 lower (2.43 to 1.37 lower) | ⊕⊕⊕◯ MODERATE a |
| Subgroup 1 | 2–3 week | 202 (3) | - | MD 3.08 lower (5.02 to 1.14lower) | ⊕⊕◯◯ LOW ab |
| 4 week | 1089 (15) | - | MD 1.7 lower (2.32 to 1.08 lower) | ⊕⊕⊕◯ MODERATE a | |
| 12 week | 100 (1) | - | MD 1.67 lower (2.15 to 1.19 lower) | ⊕⊕◯◯ LOW ab | |
| Subgroup 2 | Estazolam | 662 (9) | - | MD 2.14 lower (3 to 1.28 lower) | ⊕⊕⊕◯ MODERATE a |
| Alprazolam | 402 (6) | - | MD 2.49 lower (3.1 to 1.88 lower) | ⊕⊕⊕◯ MODERATE a | |
| Diazepam | 122 (1) | - | MD 0.49 lower (0.88 to 0.1 lower) | ⊕⊕◯◯ LOW ab | |
| Eszopiclone | 205 (3) | - | MD 0.46 lower (1.11 lower to 0.19 higher) | ⊕⊕◯◯ LOW ac | |
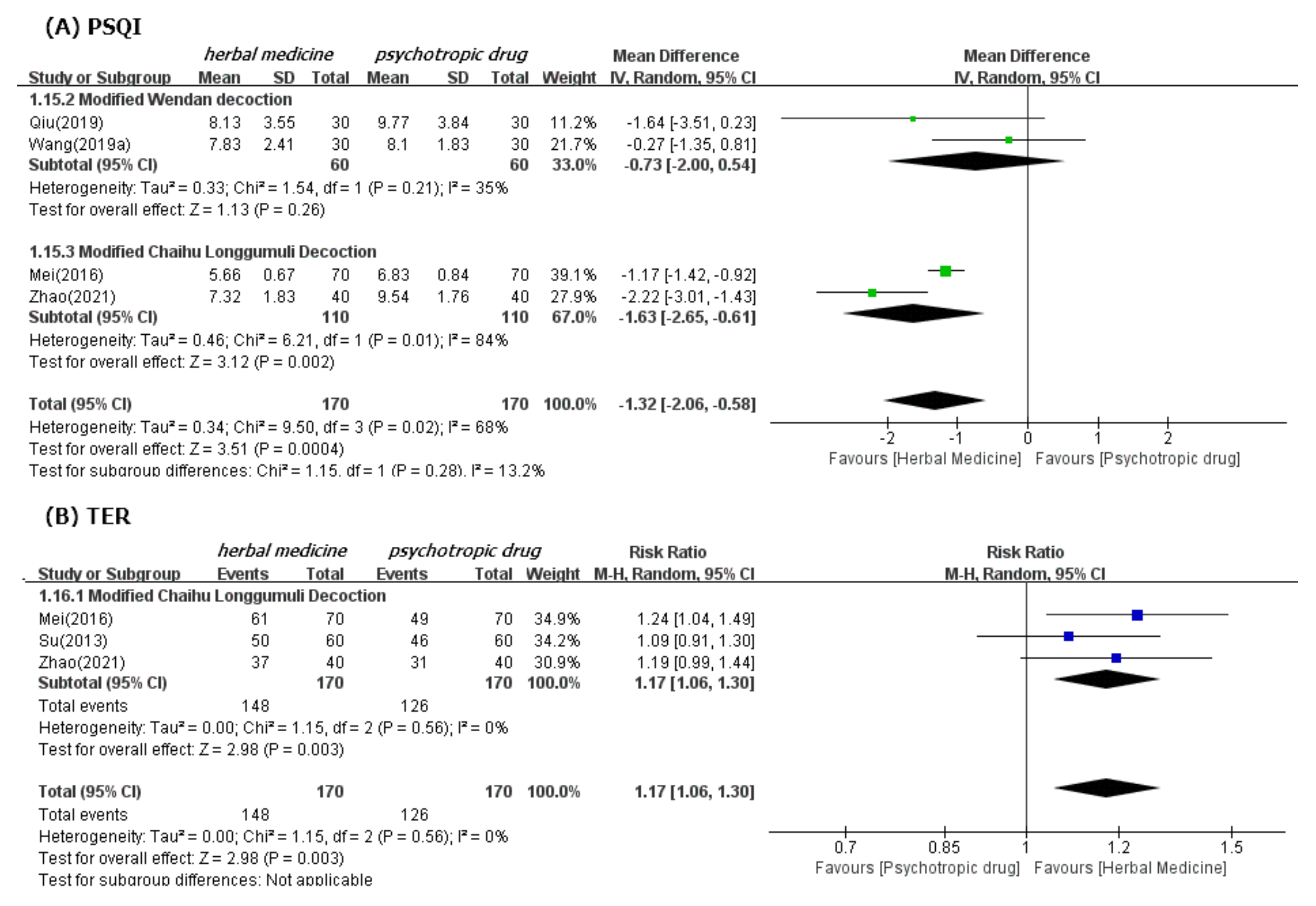
| Subgroup 3 | Wendan decoction | 120 (2) | MD 0.73 lower (2.00 lower to 0.54 higher) | ⊕⊕◯◯ LOW ac | |
| Chaihu Longgumuli Decoction | 220 (2) | MD 1.63 lower (2.65 to 0.61 lower) | ⊕⊕◯◯ LOW ab | ||
| PSQI (4 weeks f/u) | Total | 262 (3) | MD 3.08 lower (3.52 to 2.64 lower) | ⊕⊕◯◯ LOW ab | |
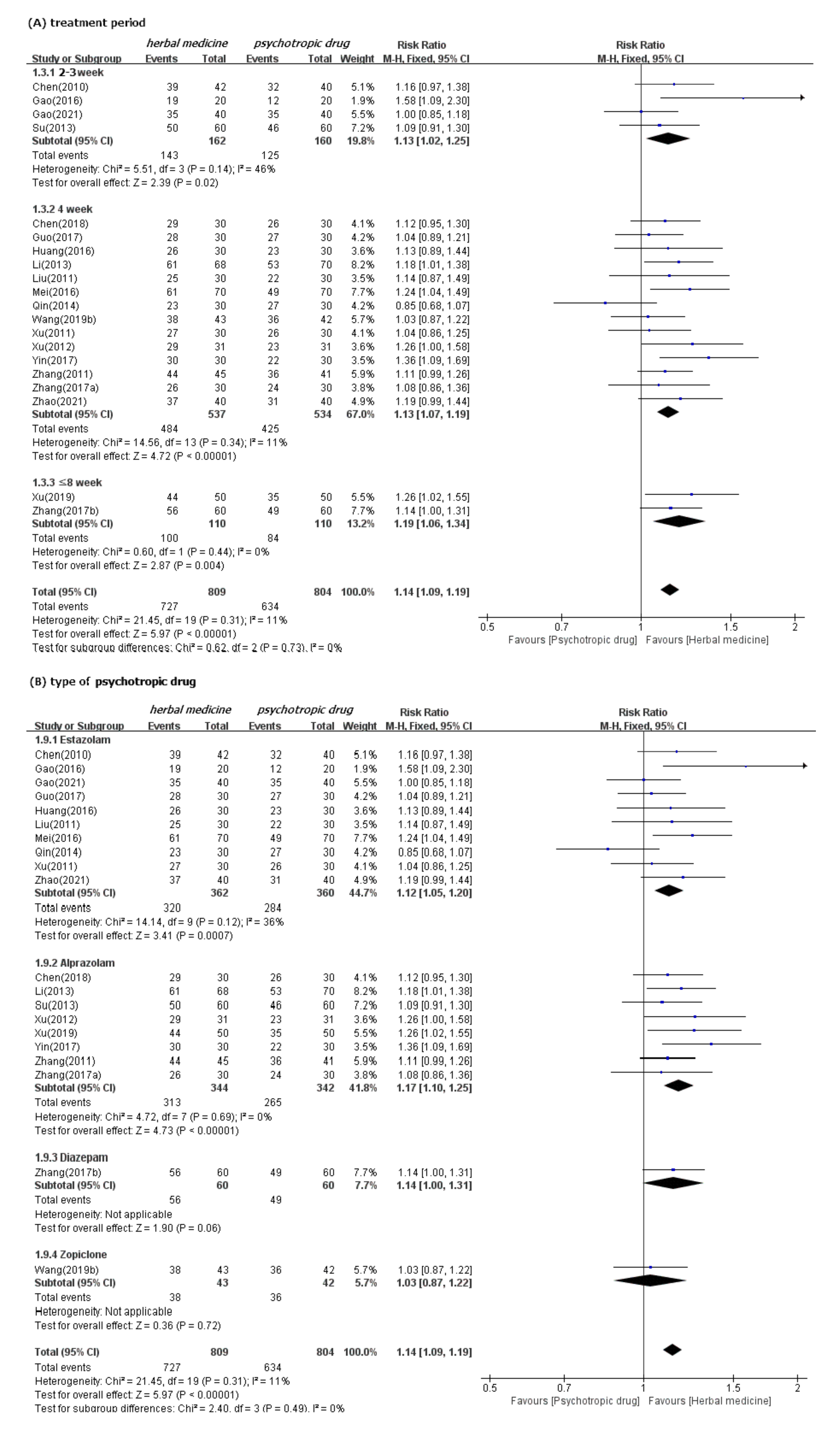
| TER | Total | 1673 (21) | 783 per 1.000 | 110 more per 1.000 (70 to 149) | ⊕⊕⊕◯ MODERATE a |
| Subgroup 1 | 2–3 week | 322 (4) | 781 per 1.000 | 102 more per 1.000 (16 to 195) | ⊕⊕◯◯ LOW ac |
| 4 week | 1071 (14) | 796 per 1.000 | 103 more per 1.000 (56 to 151) | ⊕⊕⊕◯ MODERATE a | |
| ≤8 week | 220 (2) | 764 per 1.000 | 145 more per 1.000 (46 to 260) | ⊕⊕◯◯ LOW ab | |
| Subgroup 2 | Estazolam | 722 (10) | 775 per 1.000 | 108 more per 1.000 (54 to 170) | ⊕⊕⊕◯ MODERATE a |
| Alprazolam | 686 (8) | 775 per 1.000 | 132 more per 1.000 (77 to194) | ⊕⊕⊕◯ MODERATE a | |
| Diazepam | 120 (1) | 817 per 1.000 | 114 more per 1.000 (0 to 253) | ⊕⊕◯◯ LOW ac | |
| Eszopiclone | 145 (2) | 833 per 1.000 | 0 fewer per 1.000 (108 fewer to 133 more) | ⊕⊕◯◯ LOW ac | |
| Subgroup 3 | Chaihu Longgumuli Decoction | 340 (3) | 741 per 1.000 | 126 more per 1.000 (44 to 222) | ⊕⊕◯◯ LOW ab |
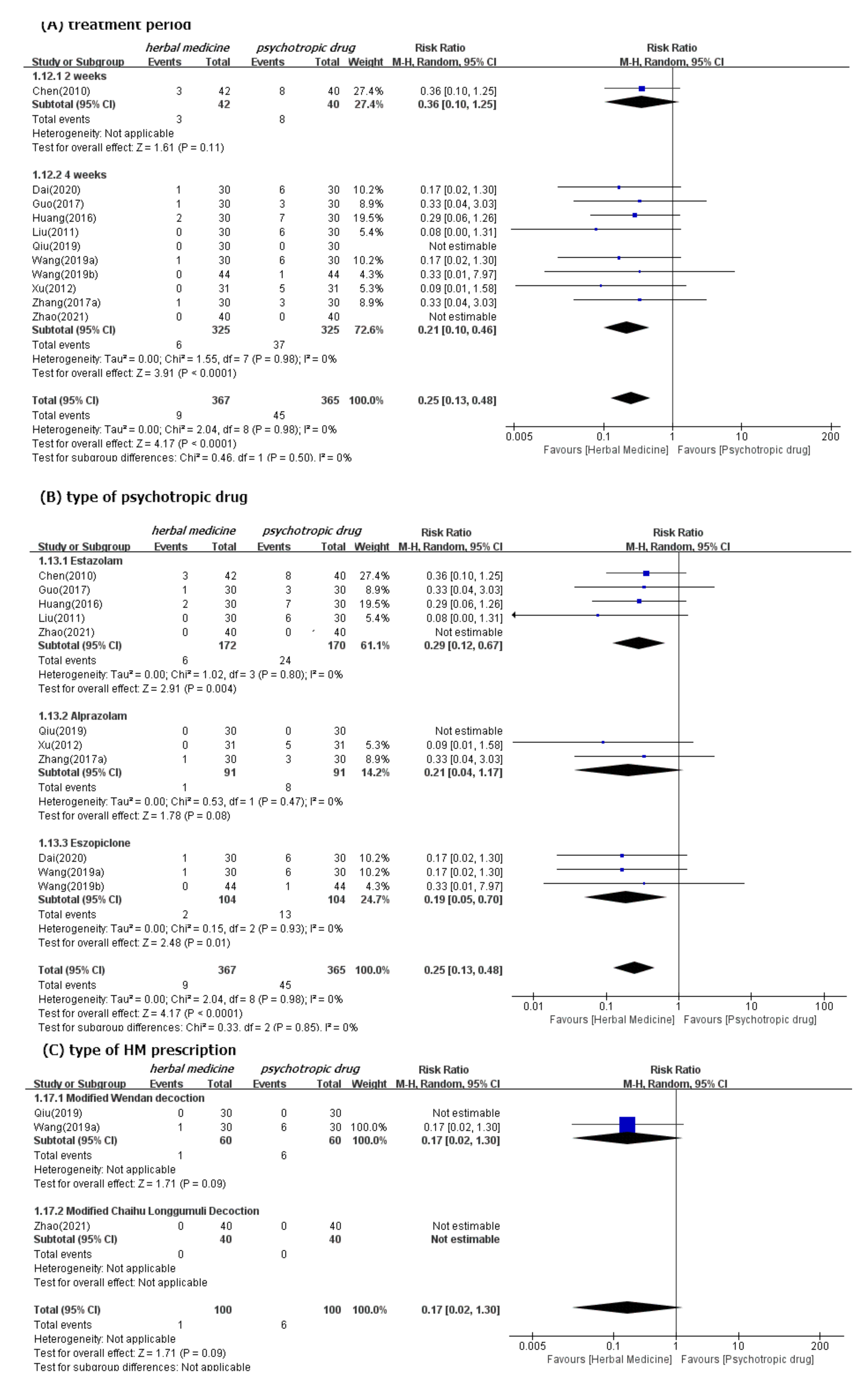
| Adverse effects | Total | 792 (12) | 114 per 1.000 | 89 fewer per 1.000 (100 to 65) | ⊕⊕⊕◯ MODERATE a |
| Subgroup 1 | 2 week | 82 (1) | 200 per 1.000 | 128 fewer per 1.000 (180 fewer to 50 more) | ⊕⊕◯◯ LOW ac |
| 4 week | 710 (11) | 104 per 1.000 | 84 fewer per 1.000 (95 to 60) | ⊕⊕⊕◯ MODERATE a | |
| Subgroup 2 | Estazolam | 402 (6) | 120 per 1.000 | 89 fewer per 1.000 (107 to 48) | ⊕⊕⊕◯ MODERATE a |
| Alprazolam | 182 (3) | 88 per 1.000 | 72 fewer per 1.000 (85 to 3) | ⊕⊕◯◯ LOW ac | |
| Eszopiclone | 208 (3) | 125 per 1.000 | 101 fewer per 1.000 (119 to 39) | ⊕⊕◯◯ LOW ab | |
| Subgroup 3 | Wendan decoction | 120 (2) | 100 per 1.000 | 83 fewer per 1.000 (98 fewer to 30 more) | ⊕⊕◯◯ LOW ac |
| Chaihu Longgumuli Decoction | 80 (1) | 0 per 1.000 | NA | ⊕⊕◯◯ LOW ac | |
| (a) PSQI. | |||
| Test Result: | |||
| t | df | p-Value | □ |
| −1.45 | 17 | 0.1656 | □ |
| Sample Estimates: | |||
| bias | se.bias | intercept | se.intercept |
| −3.6094 | 2.4915 | −0.6967 | 0.7193 |
| (b) TER | |||
| Test Result: | |||
| t | df | p-Value | □ |
| 0.83 | 20 | 0.4157 | □ |
| Sample Estimates: | |||
| bias | se.bias | intercept | se.intercept |
| 0.7602 | 0.9147 | 0.0516 | 0.0872 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.-H.; Lim, J.-H. Traditional East Asian Herbal Medicine for Post-Stroke Insomnia: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2022, 19, 1754. https://doi.org/10.3390/ijerph19031754
Kim S-H, Lim J-H. Traditional East Asian Herbal Medicine for Post-Stroke Insomnia: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. International Journal of Environmental Research and Public Health. 2022; 19(3):1754. https://doi.org/10.3390/ijerph19031754
Chicago/Turabian StyleKim, Sang-Ho, and Jung-Hwa Lim. 2022. "Traditional East Asian Herbal Medicine for Post-Stroke Insomnia: A Systematic Review and Meta-Analysis of Randomized Controlled Trials" International Journal of Environmental Research and Public Health 19, no. 3: 1754. https://doi.org/10.3390/ijerph19031754
APA StyleKim, S.-H., & Lim, J.-H. (2022). Traditional East Asian Herbal Medicine for Post-Stroke Insomnia: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. International Journal of Environmental Research and Public Health, 19(3), 1754. https://doi.org/10.3390/ijerph19031754