
Co-Designing a Program to Lower Cardiovascular Disease Risk in Midlife Black Women

 , ,
, , 
Abstract
:1. Introduction
Life’s Simple 7
2. Materials and Methods
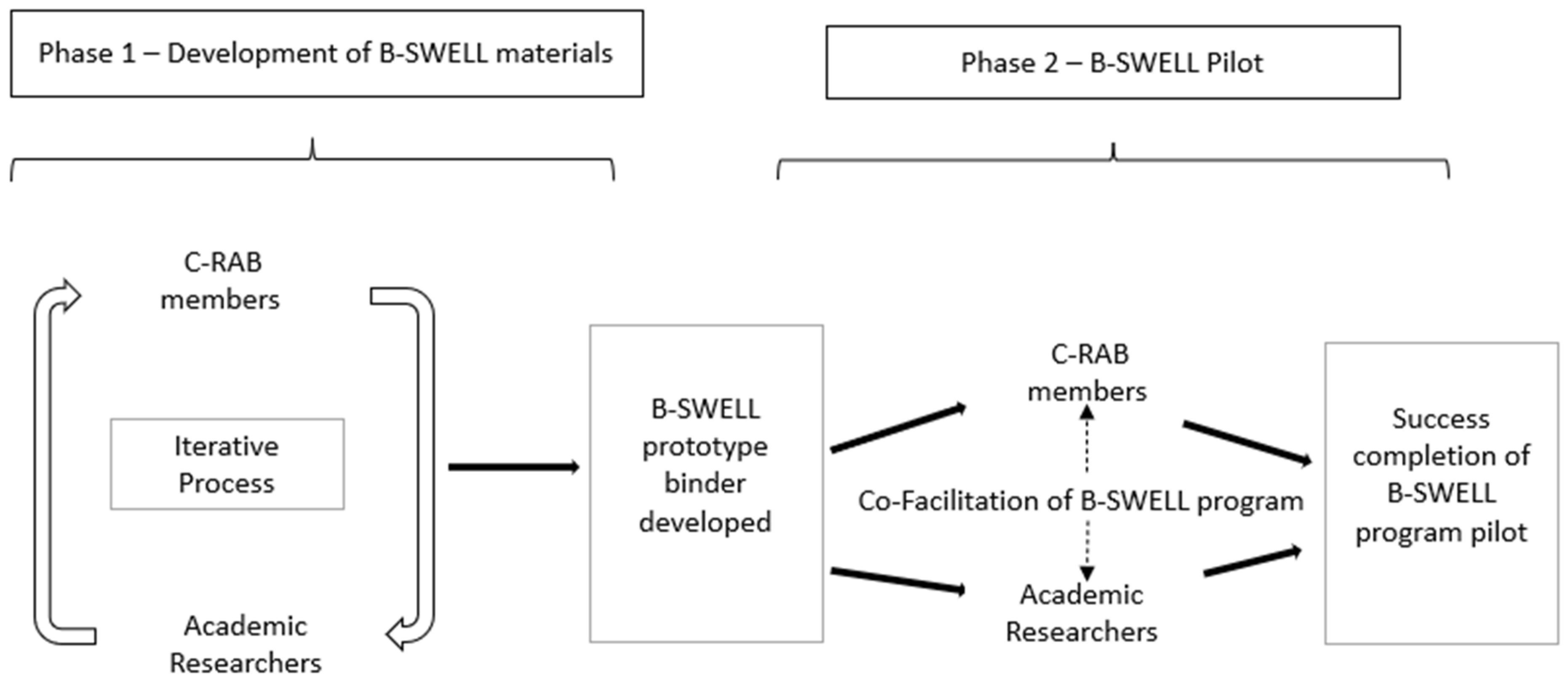
2.1. Program Conceptualization
2.2. Community Participatory Methodology and Setting
3. Results
3.1. Phase 1
3.1.1. Partnership and Recruitment
3.1.2. B-SWELL Materials
3.2. Phase 2
B-SWELL Pilot
3.3. C-RAB Member Feedback
3.4. Strengths and Challenges
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
- Purpose: We understand that the purpose of our partnership is to collaborate to help develop the 8 week B-SWELL program prototype, as well as provide input on recruitment, site locations and marketing for the program. Additionally, at the completion of the program, we will provide feedback and recommendations about the relevance and use of the outcomes from the program and identify the best ways for findings of the program to be shared with the West End community and similar communities in the future.
- Reach: We will work with our Academic Partner in the development and implementation of the B-SWELL program which will enroll 50 midlife Black women in the community. We will advocate for the program and ensure effective dissemination of the findings to the larger West End community.
- Commitment: We will…
- (a)
- Designate one WE C-RAB member to attend all quarterly Scientific Advisory Board meetings, with one designated alternate, to problem solve and inform the project. We will encourage our representative to offer his/her opinion respectfully but confidentially and to reach out for outside support when doing so feels challenging.
- (b)
- Have 4–8 WE C-RAB members participate in smaller focus groups to assist in the creation of the B-SWELL program prototype.
- (c)
- Provide feedback about the program as well as recruitment, marketing and location at a WE C-RAB meeting in early 2020.
- (d)
- Advise the Academic Partner on the relevance and use of study outcome measures from the program results (satisfaction, measures of stress and depression, a person’s belief in capacity to adopt healthy behaviors and lifestyle adoption).
- (e)
- Identify best ways for findings of the program to be shared with the West End community and similar communities in the future.
- Community Relevance: We will consider the feasibility, as well as the relevance, of this program for the West End community. We will help ensure that the program is not too complicated and is written in a manner understandable to our community, including that it is written at a 6th grade reading level or less.
- Timeline: We will attempt to keep to the project timeline and share relevant information with our partners in a timely manner if commitments are unable to be kept. Likewise, we will ask them for support as we complete our roles and responsibilities on the project to stay on time.
- Communication: We will…
- (a)
- Stay informed with the planning and follow-up to the best of our ability.
- (b)
- Ask questions and request information as we need it, including any concerns.
- (c)
- Participate in and take responsibility for the decisions/input we have agreed to provide.
- (d)
- Communicate in-person or by phone as appropriate and understand communication responses should be within 2 days.
- Funding: We understand that awarded funds, held by the academic partner, will include compensation for Scientific Advisory Board, focus groups and WE C-RAB meetings at $20/hr in the form of a Clincard or similar payment method.
- Partnership Sustainability: We understand that our partners hope to continue to work with us even after the funding period ends, and we are open to that possibility.
- Dissemination of Findings: We understand that as this is a community-academic partnership, that we will need to help our academic partner report and tailor messages and materials to disseminate the project results and future action steps when the project ends (within 3 months).
- Challenges: If we are not able to fulfill these commitments, we will expect that our partners will contact us about our responsibilities.
- Purpose: I understand that the purpose of our partnership is to collaborate to develop and successfully implement the 8 week B-SWELL program prototype that is relevant and feasibility to the West End community. I plan to work with community residents collaboratively, not on them.
- Reach: I will work with our Community Partner in the development and implementation of the B-SWELL program which will enroll 50 midlife Black women in the community. I will provide our partners access to deidentified data and results to best communicate these results to the greater community.
- Commitment: Dr. Holly Jones will be the contact researcher and her research team will attend all project meetings to co-create and implement the projects. We will encourage our entire research team to offer their opinions respectfully but confidentially and to reach out for outside support when doing so feels challenging.
- Community Relevance: I will consider the feasibility and quality of the program for the West End community. I understand that the tools should not be too burdensome for residents to complete and will be written in a manner that is understandable to our target population, including that it is written at a 5th grade reading level or less.
- Timeline: I will attempt to keep to the project timeline and share relevant information regarding timeline or commitment changes with all our partners in a timely manner. Likewise, I will ask my partners for support as I complete my roles and responsibilities on the project to stay on time.
- Communication: I will…
- (a)
- Stay informed with the planning and follow-up to the best of our ability.
- (b)
- Ask questions and request information as we need it, including in cases of any concerns.
- (c)
- Participate in and take responsibility for the decisions/input we have agreed to provide.
- (d)
- Communicate in-person or by phone as appropriate and understand communication responses should be within 2 days.
- Funding: I understand that awarded funds, held by the academic partner, will include compensation for Scientific Advisory Board, focus groups and WE C-RAB meetings at $20/hr in the form of a Clincard or similar payment method.
- Partnership Sustainability: I hope to continue to work with my Community Partners even after the funding period ends, and I will work to encourage new ideas and action steps as a result of this project.
- Dissemination of Findings: I understand that I will need to tailor my messages and materials to disseminate the project’s results and future action steps when the project ends (within 3 months).
- Challenges: If I am not able to fulfill these commitments, I will expect that my partners will contact me about my responsibilities. Depending on the situation, we may be asked to remedy unmet commitments.
References
- Williams, R.A. Cardiovascular Disease in African American Women: A Health Care Disparities Issue. J. Natl. Med. Assoc. 2009, 101, 536–540. [Google Scholar] [CrossRef]
- Thorpe, R.J., Jr.; Wynn, A.J.; Walker, J.L.; Smolen, J.R.; Cary, M.P.; Szanton, S.L.; Whitfield, K.E. Relationship Between Chronic Conditions and Disability in African American Men and Women. J. Natl. Med. Assoc. 2016, 108, 90–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mosca, L.; Hammond, G.; Mochari-Greenberger, H.; Towfighi, A.; Albert, M.A. Fifteen-Year Trends in Awareness of Heart Disease in Women: Results of a 2012 American Heart Association National Survey. Circulation 2013, 127, 1254–1263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cushman, M.; Shay, C.M.; Howard, V.J.; Jiménez, M.C.; Lewey, J.; McSweeney, J.C.; Newby, L.K.; Poudel, R.; Reynolds, H.R.; Rexrode, K.M.; et al. Ten-Year Differences in Women’s Awareness Related to Coronary Heart Disease: Results of the 2019 American Heart Association National Survey: A Special Report from The American Heart Association. Circulation 2021, 143, e239–e248. [Google Scholar] [CrossRef]
- Robertson, R.M. Women and Cardiovascular Disease: The Risks of Misperception and The Need for Action. Circulation 2001, 103, 2318–2320. [Google Scholar] [CrossRef] [Green Version]
- Garcia, M.; Mulvagh, S.L.; Bairey Merz, C.N.; Buring, J.E.; Manson, J.E. Cardiovascular Disease in Women: Clinical Perspectives. Circ Res. 2016, 118, 1273–1293. [Google Scholar] [CrossRef]
- Lloyd-Jones, D.M.; Hong, Y.; Labarthe, D.; Mozaffarian, D.; Appel, L.J.; Van Horn, L.; Greenlund, K.; Daniels, S.; Nichol, G.; Tomaselli, G.F.; et al. Defining and Setting National Goals for Cardiovascular Health Promotion and Disease Reduction: The American Heart Association’s Strategic Impact Goal Through 2020 and Beyond. Circulation 2010, 121, 586–613. [Google Scholar] [CrossRef] [Green Version]
- Wayman, J.; Long, T.; Ruoff, B.A.; Temple, S.; Taubenheim, A.M. Creating A Women and Heart Disease Brand: The Heart Truth Campaign’s Red Dress. Soc. Mar. Q. 2008, 14, 40–57. [Google Scholar] [CrossRef]
- American Heart Assoiation. Making and Impact: 8 Years of Go Red for Women. 2021. Available online: https://www.goredforwomen.org/-/media/GRFW-Files/About-Us/Go_Red_for_Women_18_year_impact_2021.pdf (accessed on 1 September 2021).
- Bairey Merz, C.N.; Andersen, H.; Sprague, E.; Burns, A.; Keida, M.; Walsh, M.N.; Greenberger, P.; Campbell, S.; Pollin, I.; McCullough, C.; et al. Knowledge, Attitudes, and Beliefs Regarding Cardiovascular Disease in Women: The Women’s Heart Alliance. J. Am. Coll. Cardiol. 2017, 70, 123–132. [Google Scholar] [CrossRef]
- Conrad, P.; Barker, K.K. The Social Construction of Illness: Key Insights and Policy Implications. J. Health Soc. Behav. 2010, 51, S67–S79. [Google Scholar] [CrossRef]
- Noonan, A.S.; Velasco-Mondragon, H.E.; Wagner, F.A. Improving the Health of African Americans in the USA: An Overdue Opportunity for Social Justice. Public Health Rev. 2016, 37, 1–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Israel, B.A.; Schulz, A.J.; Parker, E.P.; Becker, A.B. Community-Based Participatory Research: Policy Recommendations for Promoting A Partnership Approach in Health Research. Educ Health Change Learn Pract. 2001, 14, 182–197. [Google Scholar]
- Adelman, C. Kurt Lewin and the origins of action research. Educ Action Res. 1993, 1, 7–24. [Google Scholar] [CrossRef]
- Balazs, C.L.; Morello-Frosch, R. The Three Rs: How Community-Based Participatory Research Strengthens the Rigor, Relevance, and Reach of Science. Environ. Justice 2013, 6, 9–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Folsom, A.R.; Shah, A.M.; Lutsey, P.L.; Roetker, N.S.; Alonso, A.; Avery, C.L.; Miedema, M.D.; Konety, S.; Chang, P.P.; Solomon, S.D. American Heart Association’s Life’s Simple 7: Avoiding Heart Failure and Preserving Cardiac Structure and Function. Am. J. Med. 2015, 128, 970–976. [Google Scholar] [CrossRef] [Green Version]
- Kulshreshtha, A.; Vaccarino, V.; Judd, S.E.; Howard, V.J.; McClellan, W.M.; Muntner, P.; Hong, Y.; Safford, M.M.; Goyal, A.; Cushman, M. Life’s Simple 7 and Risk of Incident Stroke: The Reasons for Geographic and Racial Differences in Stroke Study. Stroke 2013, 44, 1909–1914. [Google Scholar] [CrossRef] [Green Version]
- Han, L.; You, D.; Ma, W.; Astell-Burt, T.; Feng, X.; Duan, S.; Qi, L. National Trends in American Heart Association Revised Life’s Simple 7 Metrics Associated with Risk of Mortality Among US Adults. JAMA Netw. Open 2019, 2, e1913131. [Google Scholar]
- Ogunmoroti, O.; Allen, N.B.; Cushman, M.; Michos, E.D.; Rundek, T.; Rana, J.S.; Blankstein, R.; Blumenthal, R.S.; Blaha, M.J.; Veledar, E.; et al. Association between Life’s Simple 7 and Noncardiovascular Disease: The Multi—Ethnic Study of Atherosclerosis. J. Am. Heart Assoc. 2016, 5, e003954. [Google Scholar] [CrossRef] [Green Version]
- Elgazzar, R.; Nolan, T.S.; Joseph, J.J.; Aboagye-Mensah, E.B.; Azap, R.A.; Gray, D.M. Community-Engaged and Community-Based Participatory Research to Promote American Heart Association Life’s Simple 7 Among African American Adults: A Systematic Review. PLoS ONE 2020, 15, e0238374. [Google Scholar] [CrossRef]
- Jones, H.J.; Norwood, C.R.; Bankston, K.; Bakas, T. Stress Reduction Strategies Used by Midlife Black Women to Target Cardiovascular Risk. J Cardiovasc Nurs. 2019, 34, 483–490. [Google Scholar] [CrossRef]
- Jones, H.J.; Sternberg, R.M.; Janson, S.L.; Lee, K.A. A Qualitative Understanding of Midlife Sources of Stress and Support in African-American Women. J. Natl. Black Nurses Assoc. 2016, 27, 24–30. [Google Scholar] [PubMed]
- Jones, H.J.; Norwood, C.R.; Bankston, K. Leveraging Community Engagement to Develop Culturally Tailored Stress Management Interventions in Midlife Black Women. J. Psychosoc. Nurs. Ment. Health Serv. 2019, 57, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Kidd, S.A.; Kral, M.J. Practicing Participatory Action Research. J. Couns. Psychol. 2005, 52, 187–195. [Google Scholar] [CrossRef]
- Baum, F.; MacDougall, C.; Smith, D. Participatory Action Research. J. Epidemiol. Community Health 2006, 60, 854–857. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
Reach/Scope of the Research
|
Responsibilities of the Community Partner and the Academic Partner
|
Community Relevance
|
Communication
|
Funding
|
Partnership Sustainability
|
Dissemination of Results
|
Challenges
|
| Statement of Acknowledgement of Partnership Agreement |
| Signatures of Designated C-RAB Partner and Designated Academic Partner |
| Content Description | Rationale/Cultural Relevance |
|---|---|
| Objectives | Guide use of materials and provide details of what will be learned using a culturally appropriate lens. |
| Glossary of terms | Improve access through clarity. |
| Heart disease information | Increase understanding and awareness of heart disease and heart disease risk. Provide facts and statistics about Black women and heart disease. |
| Stress and LS7 behavior | Describe the effect of stress on heart disease risk, highlighting unique stressors experienced by Black women. |
| Stress reduction strategies | Provide culturally appropriate strategies for stress. |
| Strategies to adopt LS7 | Provide culturally appropriate strategies for LS7 and information about the effect of stress on each LS7 behavior. |
| Case study | Illustrate challenges associated with the adoption of LS7 health behaviors through culturally appropriate storytelling. |
| Goal setting forms | Guide to setting realistic goals for healthy behaviors. |
| Images of midlife Black women | Improve appeal through culturally appropriate images. |
| Training Area | C-RAB Duties |
|---|---|
| B-SWELL modular content | Guide participants to resources and information available in the program materials. |
| Data collection forms | Accurate documentation of participant attendance and engagement. |
| Facilitation | Co-facilitation of group sessions with PI. Independent facilitation of break out rooms in Zoom. |
| Data Management | Confidential storage of paper documents and notes. Safe and confidential transfer of paper documents to PI. Confidential management of Zoom meeting room. |
| Technology | Use of tablet devices. Accessing Zoom meeting room. Management of Zoom breakout room and group participants. Management of Zoom audio recordings. Trouble shooting of common Zoom issues. |
| Questions for Post-Session Self-Evaluation |
|---|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jones, H.J.; Bakas, T.; Nared, S.; Humphries, J.; Wijesooriya, J.; Butsch Kovacic, M. Co-Designing a Program to Lower Cardiovascular Disease Risk in Midlife Black Women. Int. J. Environ. Res. Public Health 2022, 19, 1356. https://doi.org/10.3390/ijerph19031356
Jones HJ, Bakas T, Nared S, Humphries J, Wijesooriya J, Butsch Kovacic M. Co-Designing a Program to Lower Cardiovascular Disease Risk in Midlife Black Women. International Journal of Environmental Research and Public Health. 2022; 19(3):1356. https://doi.org/10.3390/ijerph19031356
Chicago/Turabian StyleJones, Holly J., Tamilyn Bakas, Sheila Nared, Jacqueline Humphries, Julie Wijesooriya, and Melinda Butsch Kovacic. 2022. "Co-Designing a Program to Lower Cardiovascular Disease Risk in Midlife Black Women" International Journal of Environmental Research and Public Health 19, no. 3: 1356. https://doi.org/10.3390/ijerph19031356
APA StyleJones, H. J., Bakas, T., Nared, S., Humphries, J., Wijesooriya, J., & Butsch Kovacic, M. (2022). Co-Designing a Program to Lower Cardiovascular Disease Risk in Midlife Black Women. International Journal of Environmental Research and Public Health, 19(3), 1356. https://doi.org/10.3390/ijerph19031356