
Physical Therapists and Physical Therapist Assistants’ Knowledge and Use of the STEADI for Falls Risk Screening of Older Adults in Physical Therapy Practice in the United States

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Survey
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stevens, J.A.; Lee, R. The potential to reduce falls and avert costs by clinically managing fall risk. Am. J. Prev. Med. 2018, 55, 290–297. [Google Scholar] [CrossRef] [PubMed]
- Force, U.P.S.T.; Grossman, D.C.; Curry, S.J.; Owens, D.K.; Barry, M.J.; Caughey, A.B.; Davidson, K.; Doubeni, C.A.; Epling, J.W.; Kemper, A.R.; et al. Interventions to prevent falls in community-dwelling older adults: US preventive services task force recommendation statement. JAMA 2018, 319, 1696–1704. [Google Scholar] [CrossRef]
- Gell, N.M.; Patel, K.V. Rehabilitation services use of older adults according to fall-risk screening guidelines. J. Am. Geriatr. Soc. 2019, 67, 100–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Avin, K.G.; Hanke, T.A.; Kirk-Sanchez, N.; McDonough, C.M.; Shubert, T.E.; Hardage, J.; Hartley, G. Management of falls in community-dwelling older adults: Clinical guidance statement from the Academy of Geriatric Physical Therapy of the American Physical Therapy Association. Phys. Ther. 2015, 95, 815–834. [Google Scholar] [CrossRef] [PubMed] [Green Version]
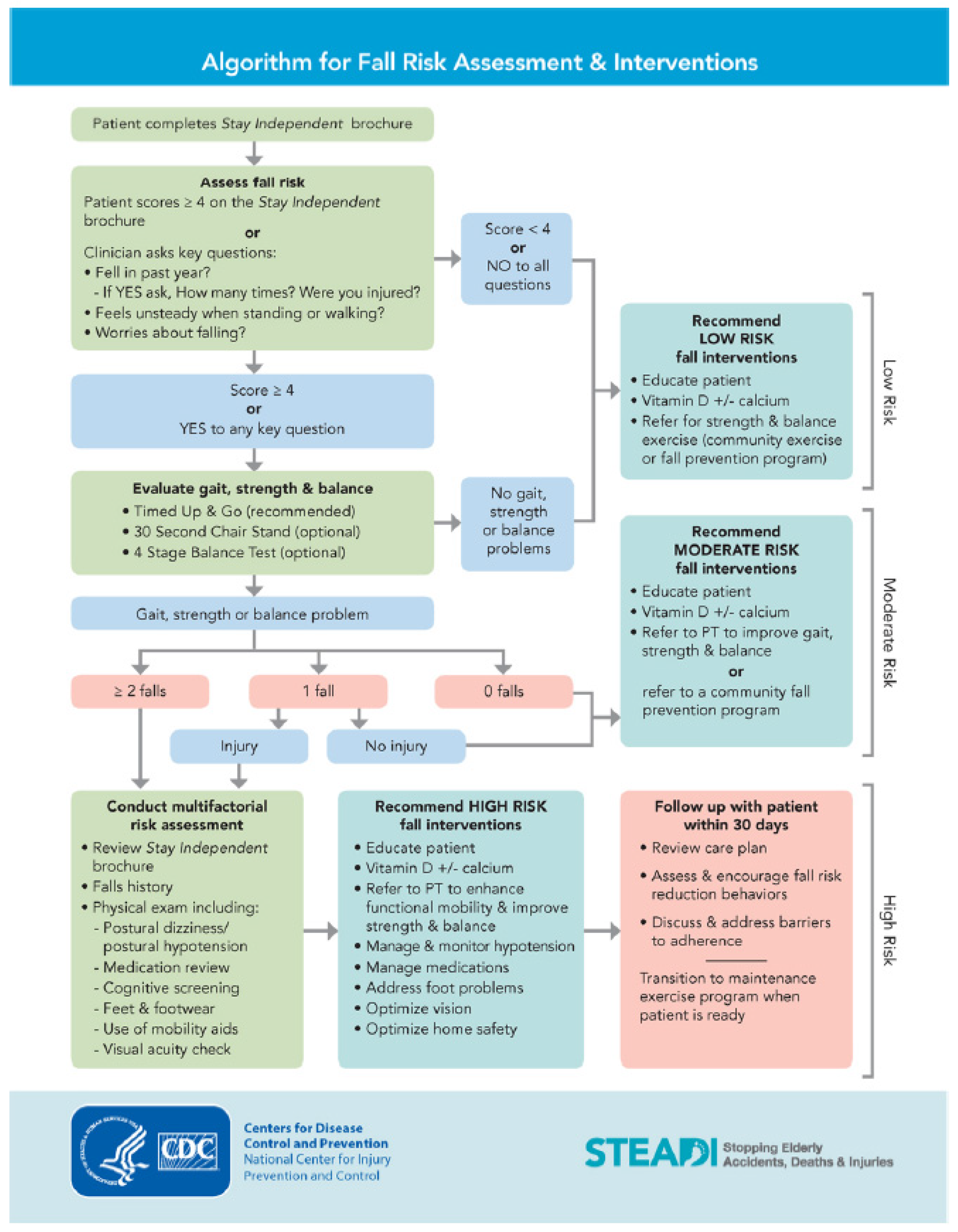
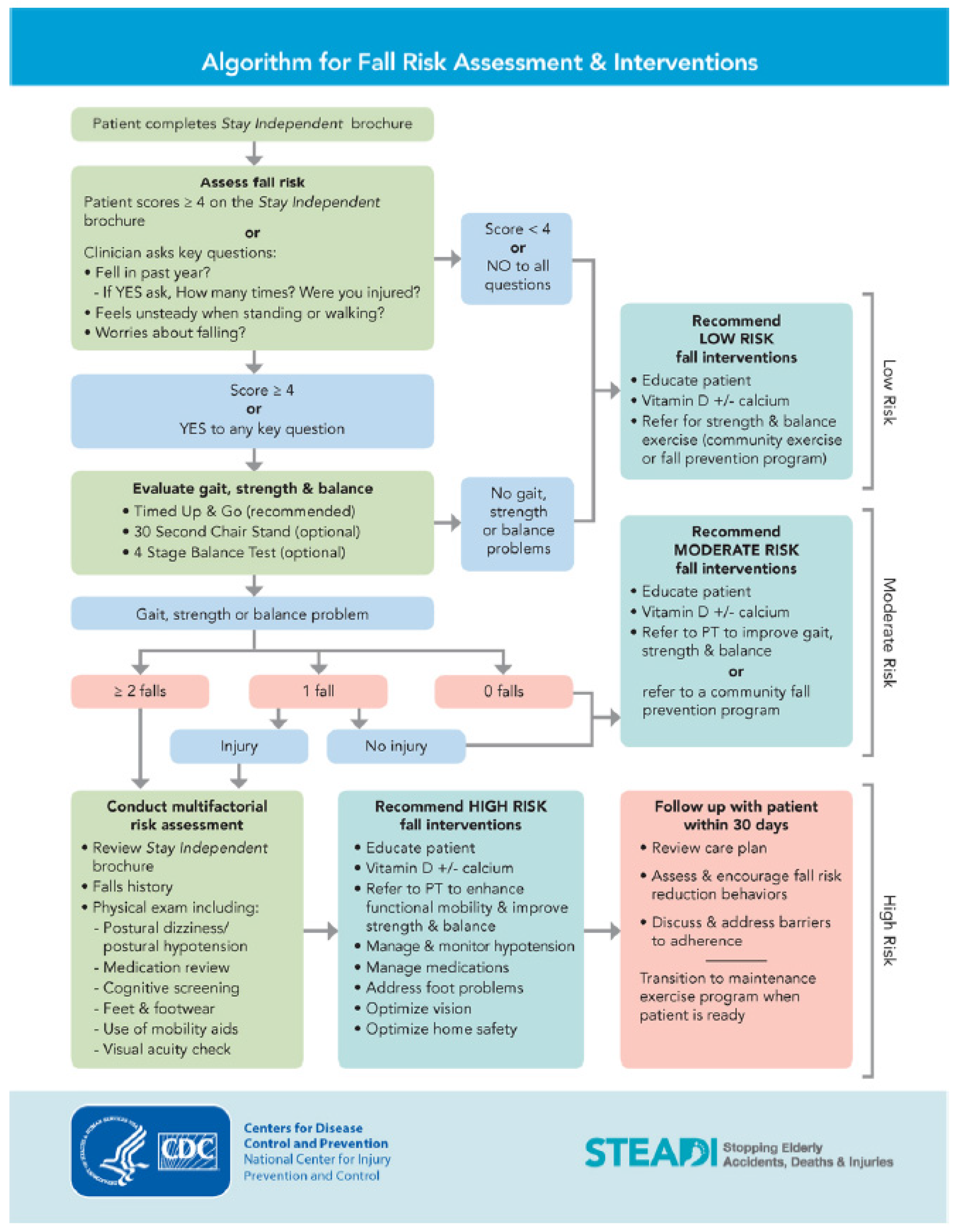
- Centers for Disease Control and Prevention National Center for Injury Prevention and Control. STEADI—Older Adult Fall Prevention. Updated 2020. Available online: https://www.cdc.gov/steadi/index.html (accessed on 4 January 2021).
- Nithman, R.W.; Vincenzo, J.L. How steady is the STEADI? Inferential analysis of the CDC fall risk toolkit. Arch. Gerontol. Geriatr. 2019, 83, 185–194. [Google Scholar] [CrossRef] [PubMed]
- Vincenzo, J.L.; Patton, S.K. Older adults’ experience with fall prevention recommendations derived from the STEADI. Health Promot. Pract. 2019, 22, 236–247. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, L.; Doe, K.; Gerry, M.; Moore, B.; Wingood, M.; Renfro, M.; Gell, N. Outcomes of a physical therapist-led, statewide, community-based fall risk screening. J. Geriatr. Phys. Ther. 2019, 43, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef] [PubMed]
- Ackerman, I.N.; Soh, S.; Barker, A.L. Physiotherapists’ falls prevention knowledge, beliefs and practices in osteoarthritis care: A national cross-sectional study. Arthritis Care Res. 2020, 72, 1087–1095. [Google Scholar] [CrossRef] [PubMed]
- Lusardi, M.M.; Fritz, S.; Middleton, A.; Allison, L.; Wingood, M.; Phillips, E.; Criss, M.; Verma, S.; Osborne, J.; Chui, K.K. Determining risk of falls in community dwelling older adults: A systematic review and meta-analysis using posttest probability. J. Geriatr. Phys. Ther. 2017, 40, 1–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bullock, H.L.; Lavis, J.N.; Wilson, M.G.; Mulvale, G.; Miatello, A. Understanding the implementation of evidence-informed policies and practices from a policy perspective: A critical interpretive synthesis. Implement. Sci. 2021, 16, online. [Google Scholar] [CrossRef] [PubMed]
- Kruse, C.S.; Stein, A.; Thomas, H.; Kaur, H. The use of electronic health records to support population health: A systematic review of the literature. J. Med. Syst. 2018, 42, 1–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Physical Therapy Association. APTA Guide to Physical Therapist Practice. Available online: https://guide.apta.org/ (accessed on 2 June 2021).
- Commission on Accreditation in Physical Therapy Education. Accreditation Handbook. Available online: https://www.capteonline.org/about-capte/policies-and-procedures/accreditation-handbook (accessed on 2 June 2021).

{kind=link}
| Conduct Fall-Risk Screening Mean ± SD or n (%) (n = 379) | Does Not Conduct Fall-Risk Screening Mean ± SD or n (%) (n = 46) | p-Value | |
|---|---|---|---|
| Age | 46.9 ± 11.7 | 48.4 ± 11.9 | 0.4032 |
| Gender | 0.1461 | ||
| Male | 65 (17.2) | 8 (17.4) | |
| Female | 311 (82.1) | 36 (78.3) | |
| Prefer not to report | 3 (0.8) | 2 (4.4) | |
| Occupation | 0.0605 | ||
| Physical therapist | 340 (89.7) | 37 (80.4) | |
| Physical therapist assistant | 39 (10.3) | 9 (19.6) | |
| Degree | 0.59 | ||
| Associate | 24 (6.3) | 6 (13.0) | |
| BS | 67 (17.7) | 9 (19.6) | |
| MS | 67 (17.7) | 8 (17.4) | |
| DPT | 181 (47.8) | 18 (39.1) | |
| EdD/PhD | 30 (7.9) | 4 (8.7) | |
| other | 10 (2.6) | 1 (2.2) | |
| Years in practice | 0.277 | ||
| ≤5 | 38 (10.0) | 8 (17.4) | |
| 6–10 | 71 (18.7) | 5 (10.9) | |
| 11–20 | 88 (23.2) | 9 (19.6) | |
| >20 | 182 (48.0) | 24 (52.2) | |
| APTA member | 0.5234 | ||
| Yes | 286 (75.5) | 33 (71.7) | |
| No | 87 (23.0) | 13 (28.3) | |
| N/A | 6 (1.6) | 0 (0.0) | |
| APTA academy/section member | |||
| Geriatrics | 229 (60.4) | 21 (45.7) | 0.0546 |
| Neurologic | 81 (21.4) | 6 (13.0) | 0.1862 |
| Orthopedic | 40 (10.6) | 7 (15.2) | 0.3409 |
| Home health | 44 (11.6) | 2 (4.4) | 0.2054 |
| Health policy and administration | 11 (2.9) | 2 (4.4) | 0.6407 |
| Acute care | 29 (7.7) | 2 (4.4) | 0.5581 |
| Aquatic | 4 (1.1) | 1 (2.2) | 0.4377 |
| Cardiovascular/pulmonary | 15 (4.0) | 0 (0.0) | 0.3882 |
| Electrophysiology and wound | 11 (2.9) | 1 (2.2) | 1 |
| Education | 40 (10.6) | 5 (10.9) | 1 |
| Federal | 4 (1.1) | 2 (4.4) | 0.1297 |
| Hand and upper extremity | 1 (0.3) | 0 (0.0) | 1 |
| Oncologic | 10 (2.6) | 1 (2.2) | 1 |
| Pediatric | 3 (0.8) | 2 (4.4) | 0.0928 |
| Private practice | 7 (1.9) | 2 (4.4) | 0.2532 |
| Research | 17 (4.5) | 1 (2.2) | 0.7069 |
| Sports | 2 (0.5) | 4 (8.7) | 0.0015 |
| Women’s health | 10 (2.6) | 0 (0.0) | 0.6097 |
| Board-certified clinical specialist | 176 (46.4) | 15 (32.6) | 0.075 |
| Cardiovascular and pulmonary | 0 (0.0) | 1 (2.2) | 0.1082 |
| Geriatrics | 129 (34.0) | 8 (17.4) | 0.0225 |
| Neurology | 32 (8.4) | 1 (2.2) | 0.2365 |
| Oncology | 1 (0.3) | 0 (0.0) | 1 |
| Orthopedics | 11 (2.9) | 5 (10.9) | 0.0209 |
| Sports | 3 (0.8) | 0 (0.0) | 1 |
| Women’s health | 0 (0.0) | 0 (0.0) | ----- |
| Clinical electrophysiology | 0 (0.0) | 0 (0.0) | ----- |
| Pediatrics | 1 (0.3) | 0 (0.0) | 1 |
| Practice setting | |||
| Outpatient/wellness | 178 (47.0) | 24 (52.2) | 0.5042 |
| Acute care | 53 (14.0) | 8 (17.4) | 0.5337 |
| Assisted living | 60 (15.8) | 6 (13.0) | 0.622 |
| Inpatient rehab | 28 (7.4) | 1 (2.2) | 0.3465 |
| Skilled nursing facility | 132 (34.8) | 15 (32.6) | 0.765 |
| Home health | 86 (22.7) | 3 (6.5) | 0.0113 |
| Academic program | 37 (9.8) | 5 (10.9) | 0.7938 |
| Other | 32 (8.4) | 2 (4.4) | 0.5621 |
| Employment status | 0.4846 | ||
| Full-time | 308 (81.3) | 40 (87.0) | |
| Part-time/per diem/other | 70 (18.5) | 6 (13.0) | |
| No response | 1 (0.3) | 0 (0.0) | |
| Percent of time in patient care | 0.1567 | ||
| 0–25% | 96 (25.3) | 17 (37.0) | |
| 30–50% | 36 (9.5) | 4 (8.7) | |
| 55–75% | 67 (17.7) | 3 (6.5) | |
| 80–100% | 180 (47.5) | 22 (47.8) | |
| Percent of caseload 65+ years | 0.0004 | ||
| 0–25% | 17 (4.5) | 6 (13.0) | |
| 30–50% | 33 (8.7) | 6 (13.0) | |
| 55–75% | 83 (21.9) | 7 (15.2) | |
| 80–100% | 244 (64.4) | 23 (50.0) | |
| No response | 2 (0.5) | 4 (8.7) |
| How Familiar Are You with the STEADI as a Tool for Fall-Risk Screening? | n (%) |
|---|---|
| Very familiar | 132 (31.1) |
| Familiar | 84 (19.8) |
| Somewhat familiar | 116 (27.3) |
| Not familiar at all | 92 (21.7) |
| No response | 1 (0.2) |
| How did you learn about STEADI? (Could select more than 1) | n (%) |
| School | 30 (7.1) |
| Colleague | 93 (21.9) |
| Continuing education | 145 (34.1) |
| Other | 79 (18.6) |
| Not aware of STEADI | 15 (3.5) |
| Other | 12 (2.8) |
| Do you use the STEADI tool for fall-risk screening? (Question only posed to respondents who indicated they were very familiar with the STEADI) (n = 132) | |
| Yes | 111 (84.1) |
| No | 11 (8.3) |
| Other | 10 (7.6) |
| What components of the STEADI do you use? (Could select more than 1 answer) (Question only posed to respondents who answered ‘Yes’ or ‘Other’ to using the STEADI) (n = 122) | |
| Screening—Stay Independent Brochure and Questionnaire | 57 (46.7) |
| Screening—3 key questions | 89 (72.9) |
| Functional mobility—Timed Up and Go test | 80 (65.6) |
| Functional mobility—30 s chair—stand test | 82 (67.2) |
| Functional mobility—4 Stage Balance Test | 67 (54.9) |
| Functional mobility—All 3 tests | 79 (64.8) |
| Assessment—Multifactorial process | 75 (61.5) |
| Education/intervention—e.g., ways to decrease fall risk based on results and recommendations in algorithms and referrals | 105 (86.1) |
| When did you first implement STEADI? (Question only posed to respondents who answered ‘Yes’ to using the STEADI) (n = 111) | |
| <1 year ago | 14 (7.9) |
| 1–2 year ago | 18 (16.2) |
| 2–3 years ago | 23 (20.7) |
| 3–4 years ago | 14 (12.6) |
| More than 4 years ago | 42 (37.8) |
| Was it your choice to integrate STEADI into your practice or an expectation? (Question only posed to respondents who answered ‘Yes’ or ‘Other’ to using the STEADI) (n = 121) | |
| My choice | 92 (76.0) |
| Employer mandate | 10 (8.3) |
| Employer recommendation | 13 (10.7) |
| Other | 6 (5.0) |
| Is the STEADI screen embedded in your practice/documentation workflow? (Question only posed to respondents who answered ‘Yes’ or ‘Other’ to using the STEADI) (n = 121)? | |
| Yes | 52 (43.0) |
| No | 63 (52.1) |
| Unsure | 3 (2.5) |
| Other | 3 (2.5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vincenzo, J.L.; Schrodt, L.A.; Hergott, C.; Perera, S.; Tripken, J.; Shubert, T.E.; Brach, J.S. Physical Therapists and Physical Therapist Assistants’ Knowledge and Use of the STEADI for Falls Risk Screening of Older Adults in Physical Therapy Practice in the United States. Int. J. Environ. Res. Public Health 2022, 19, 1354. https://doi.org/10.3390/ijerph19031354
Vincenzo JL, Schrodt LA, Hergott C, Perera S, Tripken J, Shubert TE, Brach JS. Physical Therapists and Physical Therapist Assistants’ Knowledge and Use of the STEADI for Falls Risk Screening of Older Adults in Physical Therapy Practice in the United States. International Journal of Environmental Research and Public Health. 2022; 19(3):1354. https://doi.org/10.3390/ijerph19031354
Chicago/Turabian StyleVincenzo, Jennifer L., Lori A. Schrodt, Colleen Hergott, Subashan Perera, Jennifer Tripken, Tiffany E. Shubert, and Jennifer S. Brach. 2022. "Physical Therapists and Physical Therapist Assistants’ Knowledge and Use of the STEADI for Falls Risk Screening of Older Adults in Physical Therapy Practice in the United States" International Journal of Environmental Research and Public Health 19, no. 3: 1354. https://doi.org/10.3390/ijerph19031354
APA StyleVincenzo, J. L., Schrodt, L. A., Hergott, C., Perera, S., Tripken, J., Shubert, T. E., & Brach, J. S. (2022). Physical Therapists and Physical Therapist Assistants’ Knowledge and Use of the STEADI for Falls Risk Screening of Older Adults in Physical Therapy Practice in the United States. International Journal of Environmental Research and Public Health, 19(3), 1354. https://doi.org/10.3390/ijerph19031354