
Navigating the LGB Data Landscape: A Review of Appropriate Secondary Data Sources for Sexuality and Substance Use Research in the UK


Abstract
:1. Introduction
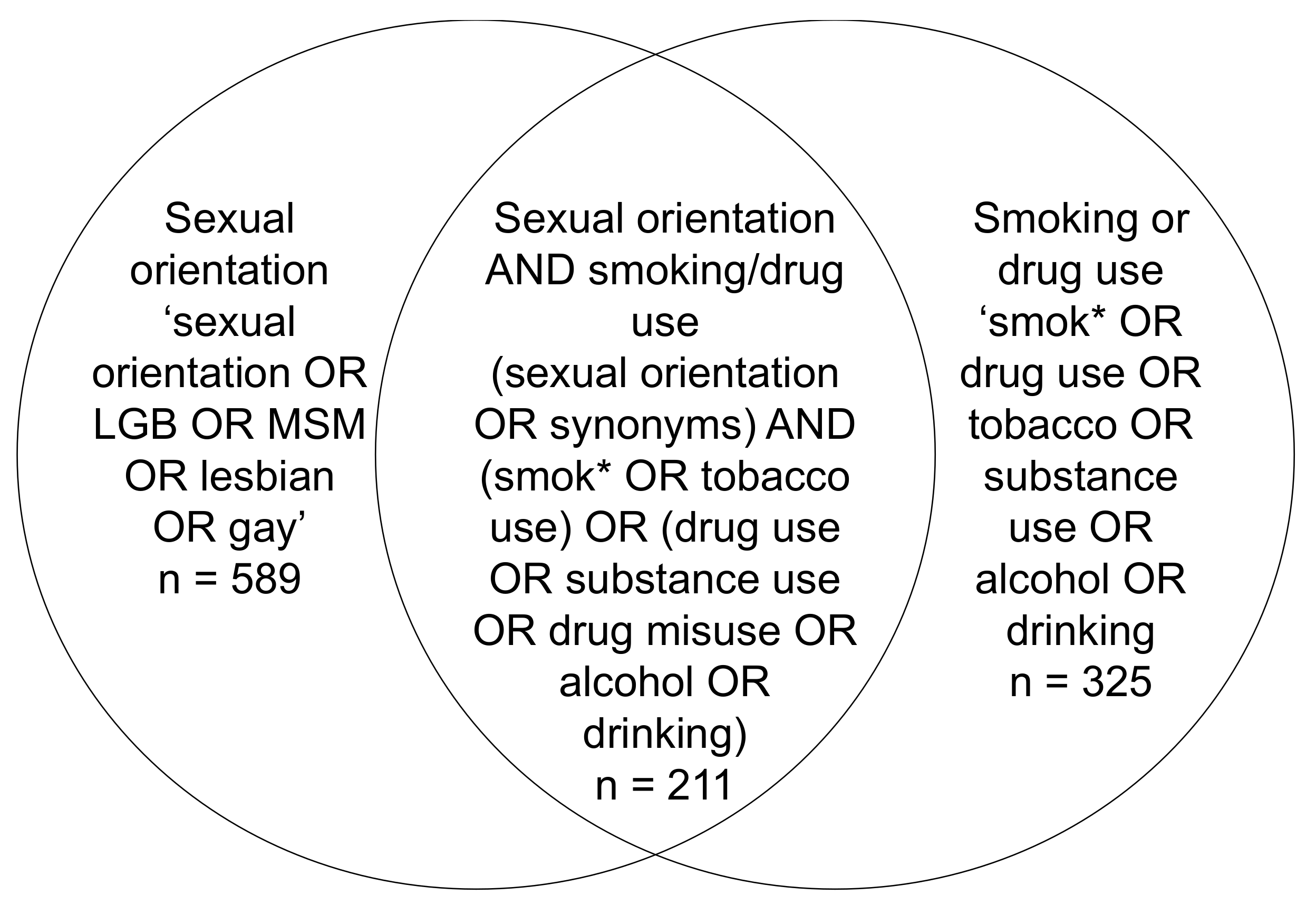
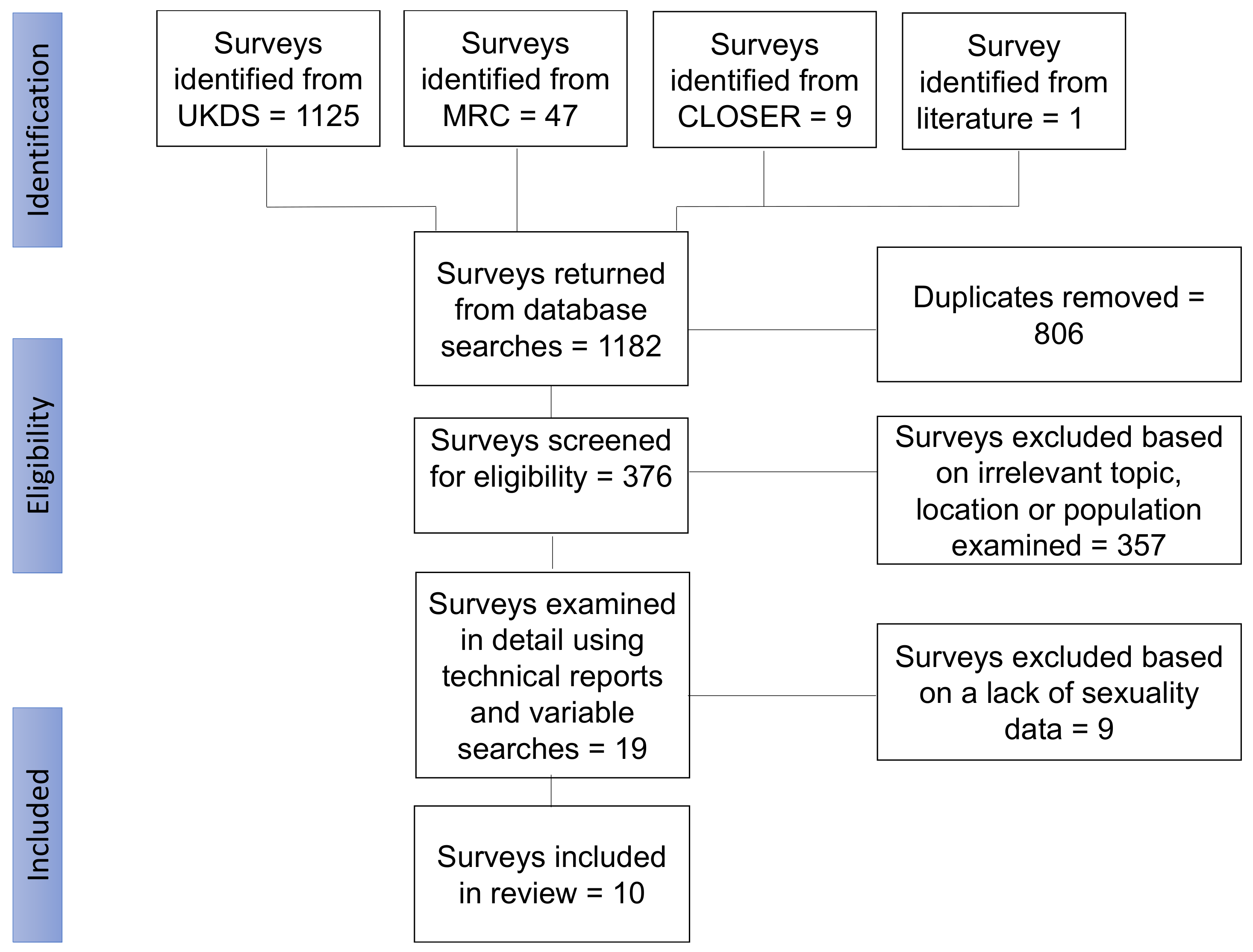
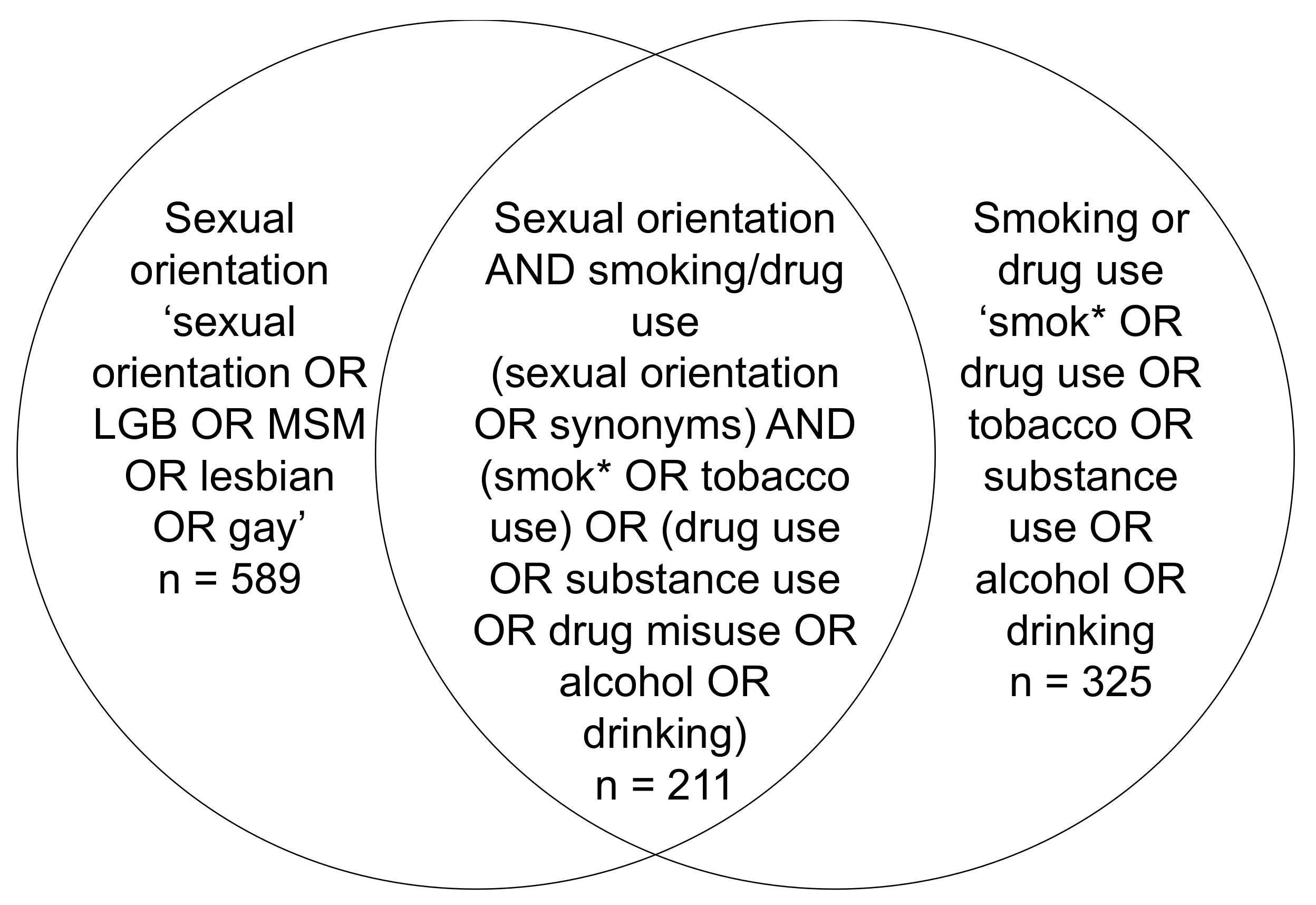
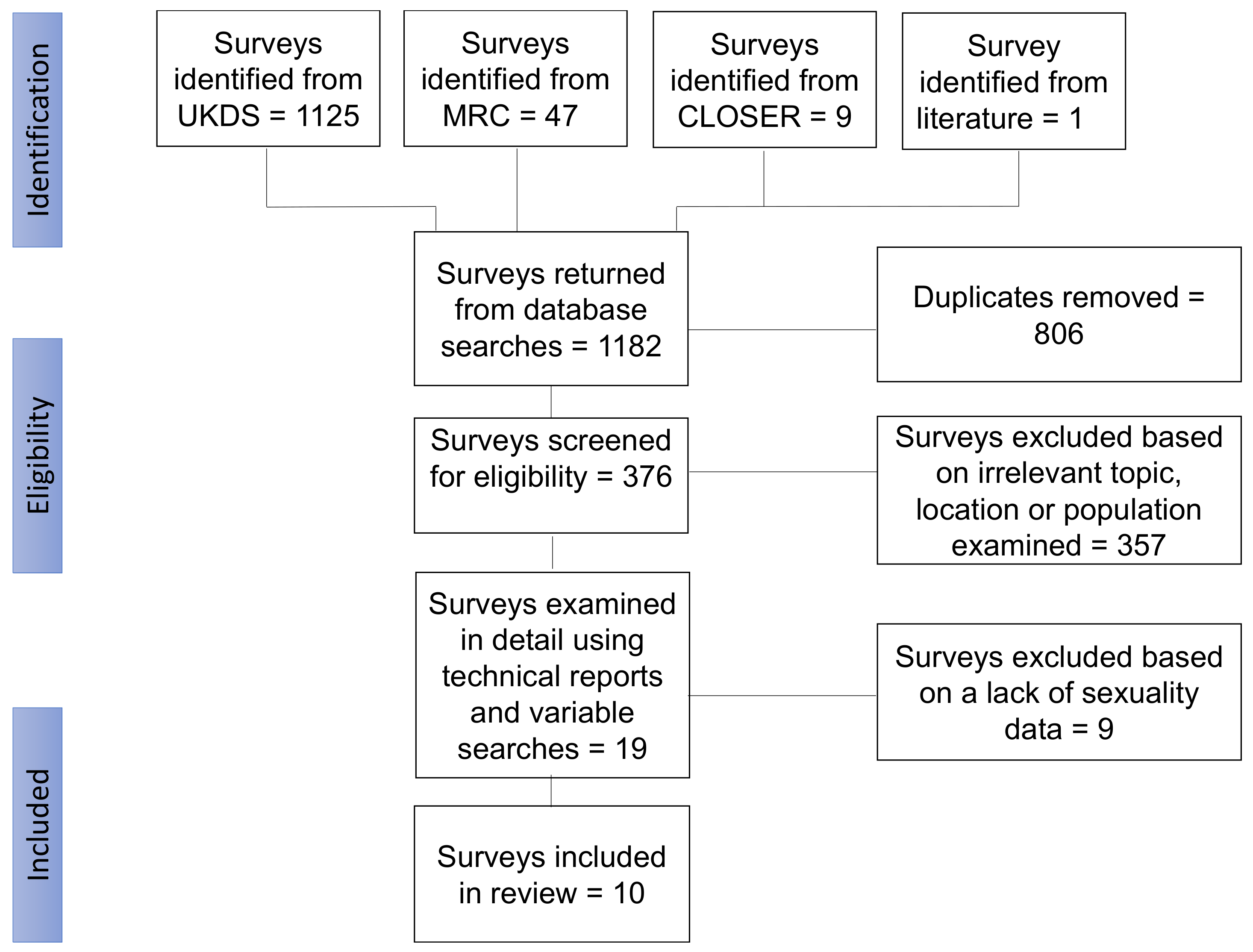
2. Methods
3. Results
3.1. Access Conditions
3.2. Health Surveys
Spatial Units for Geographical Analysis
3.3. General Social and Lifestyle Surveys
Spatial Units for Geographical Analysis
3.4. Sexuality Surveys
Spatial Units for Geographical Analysis
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Glossary of Terms
| APMS | Adult Psychiatric Morbidity Survey |
| APS | Annual Population Survey |
| BHPS | British Household Panel Study |
| CLOSER | Cohort and Longitudinal Studies Enhancement Resources |
| EMIS | European Men Who Have Sex with Men Internet Survey |
| EUL | End user licence |
| GOR | Government office regions |
| GPPS | General Practitioner Patient Survey |
| HSE | Health Survey for England |
| LA | Local authority |
| LGB | Lesbian gay and bisexual |
| LSOA | Lower layer super output area |
| MRC | Medical Research Council |
| MSM | Men who have sex with Men |
| NATSAL | National Survey of Sexual Attitudes and Lifestyle |
| NSW | National Survey for Wales |
| ONS | Office for National Statistics |
| PHE | Public Health England |
| SHS | Scottish Health Survey |
| UKDS | UK Data Service |
| US | Understand Society |
References
- Bourne, A.; Davey, C.; Hickson, F.; Reid, D.; Weatherburn, P. Physical health inequalities among gay and bisexual men in England: A large community-based cross-sectional survey. J. Public Health 2017, 39, 290–296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meads, C.; Carmona, C.; Kelly, M.P. Lesbian, gay and bisexual people’s health in the UK: A theoretical critique and systematic review. Divers. Equal Health Care 2012, 9, 19–32. [Google Scholar]
- Shahab, L.; Brown, J.; Hagger-Johnson, G.; Michie, S.; Semlyen, J.; West, R.; Meads, C. Sexual orientation identity and tobacco and hazardous alcohol use: Findings from a cross-sectional English population survey. BMJ Open 2017, 7, e015058. [Google Scholar] [CrossRef] [PubMed]
- Davies, M.; Lewis, N.M.; Moon, G. Sexuality, space, gender, and health: Renewing geographical approaches to well-being in lesbian, gay, bisexual, transgender, and queer populations. Geogr. Compass 2018, 12, e12369. [Google Scholar] [CrossRef]
- Semlyen, J.; King, M.; Varney, J.; Hagger-Johnson, G. Sexual orientation and symptoms of common mental disorder or low wellbeing: Combined meta-analysis of 12 UK population health surveys. BMC Psychiatry 2016, 16, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Office for National Statistics. 2011 Census Variable and Classification Information: Part 3 - Standard variables. Available online: https://www.ons.gov.uk/census/2011census/2011censusdata/2011censususerguide/variablesandclassifications (accessed on 10 December 2021).
- Cheng, H.G.; Phillips, M.R. Secondary analysis of existing data: Opportunities and implementation. Shanghai Arch. Psychiatry 2014, 26, 371–375. [Google Scholar] [CrossRef]
- Fendrich, M.; Rosenbaum, D.P. Recanting of substance use reports in a longitudinal prevention study. Drug Alcohol Depend. 2003, 70, 241–253. [Google Scholar] [CrossRef]
- Warren, J.R.; Halpern-Manners, A. Panel Conditioning in Longitudinal Social Science Surveys. Sociol Methods Res. 2012, 41, 491–534. [Google Scholar] [CrossRef]
- Geary, R.S.; Tanton, C.; Erens, B.; Clifton, S.; Prah, P.; Wellings, K.; Mitchell, K.R.; Datta, J.; Gravningen, K.; Fuller, E.; et al. Sexual identity, attraction and behaviour in Britain: The implications of using different dimensions of sexual orientation to estimate the size of sexual minority populations and inform public health interventions. PLoS ONE 2018, 13, e0189607. [Google Scholar] [CrossRef] [Green Version]
- Aicken, C.R.; Nardone, A.; Mercer, C.H. Alcohol misuse, sexual risk behaviour and adverse sexual health outcomes: Evidence from Britain’s national probability sexual behaviour surveys. J. Public Health (Oxf) 2011, 33, 262–271. [Google Scholar] [CrossRef]
- Katz-Wise, S.L. Sexual fluidity in young adult women and men: Associations with sexual orientation and sexual identity development. Psychol Sex. 2015, 6, 189–208. [Google Scholar] [CrossRef]
- Macintyre, S.; Ellaway, A.; Cummins, S. Place effects on health: How can we conceptualise, operationalise and measure them? Soc. Sci. Med. 2002, 55, 125–139. [Google Scholar] [CrossRef]
- Duncan, D.T.; Hatzenbuehler, M.L.; Johnson, R.M. Neighborhood-level LGBT hate crimes and current illicit drug use among sexual minority youth. Drug Alcohol Depend. 2014, 135, 65–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davies, M.; Moon, G.; Lewis, N.M. Trends in smoking prevalence over time and space: A comparison between sexual minority and heterosexual populations. Health Place 2020, 65, 102421. [Google Scholar] [CrossRef] [PubMed]
- Hatzenbuehler, M.L.; Wieringa, N.F.; Keyes, K.M. Community-level determinants of tobacco use disparities in lesbian, gay, and bisexual youth: Results from a population-based study. Arch. Pediatr. Adolesc. Med. 2011, 165, 527–532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Office for National Statistics. Exploring Existing Data on Gender Identity and Sexual Orientation. Available online: https://www.ons.gov.uk/methodology/classificationsandstandards/measuringequality/genderidentity/exploringexistingdataongenderidentityandsexualorientation (accessed on 18 November 2021).
- Davies, M.; Lewis, N.M.; Moon, G. Differential pathways into smoking among sexual orientation and social class groups in England: A structural equation model. Drug Alcohol Depend. 2019, 201, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Berg, R.C.; Ross, M.W.; Weatherburn, P.; Schmidt, A.J. Structural and environmental factors are associated with internalised homonegativity in men who have sex with men: Findings from the European MSM Internet Survey (EMIS) in 38 countries. Soc. Sci. Med. 2013, 78, 61–69. [Google Scholar] [CrossRef] [Green Version]
- Public Health England. Producing Modelled Estimates of the Size of the Lesbian, Gay and Bisexual (LGB) Population of England: Final Report. Available online: https://www.gov.uk/government/publications/producing-estimates-of-the-size-of-the-lgb-population-of-england (accessed on 21 November 2021).
- Fish, J.N.; Watson, R.J.; Gahagan, J.; Porta, C.M.; Beaulieu-Prévost, D.; Russell, S.T. Smoking behaviours among heterosexual and sexual minority youth? Findings from 15 years of provincially representative data. Drug Alcohol Rev. 2019, 38, 101–110. [Google Scholar] [CrossRef] [Green Version]
- Watson, R.J.; Goodenow, C.; Porta, C.; Adjei, J.; Saewyc, E. Substance Use among Sexual Minorities: Has it Actually Gotten Better? Subst. Use Misuse 2018, 53, 1221–1228. [Google Scholar] [CrossRef]
- NHS Digital. Health and Health-Related Behaviours of Lesbian, Gay and Bisexual Adults. Available online: https://www.gov.uk/government/statistics/health-survey-england-additional-analyses-health-and-health-related-behaviours-of-lesbian-gay-and-bisexual-adults (accessed on 24 October 2021).
- Chakraborty, A.; McManus, S.; Brugha, T.S.; Bebbington, P.; King, M. Mental health of the non-heterosexual population of England. Br. J. Psychiatry 2011, 198, 143–148. [Google Scholar] [CrossRef] [Green Version]
- Hayes, J.; Chakraborty, A.T.; McManus, S.; Bebbington, P.; Brugha, T.; Nicholson, S.; King, M. Prevalence of same-sex behavior and orientation in England: Results from a national survey. Arch. Sex. Behav 2012, 41, 631–639. [Google Scholar] [CrossRef]
- Urwin, S.; Whittaker, W. Inequalities in family practitioner use by sexual orientation: Evidence from the english general practice patient survey. BMJ Open 2016, 6, e011633. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saunders, C.L.; MacCarthy, S.; Meads, C.; Massou, E.; Mant, J.; Saunders, A.M.; Elliott, M.N. Long-term conditions among sexual minority adults in England: Evidence from a cross-sectional analysis of responses to the English GP Patient Survey. BJGP Open 2021, 5, BJGPO.2021.0067. [Google Scholar] [CrossRef] [PubMed]
- Ganna, A.; Verweij, K.J.H.; Nivard, M.G.; Maier, R.; Wedow, R.; Busch, A.S.; Abdellaoui, A.; Guo, S.; Sathirapongsasuti, J.F.; 23andMe Research Team; et al. Large-scale GWAS reveals insights into the genetic architecture of same-sex sexual behavior. Science 2019, 365, eaat7693. [Google Scholar] [CrossRef] [PubMed]
- Booker, C.L.; Rieger, G.; Unger, J.B. Sexual orientation health inequality: Evidence from Understanding Society, the UK Longitudinal Household Study. Prev. Med. 2017, 101, 126–132. [Google Scholar] [CrossRef] [Green Version]
- Mercer, C.H.; Prah, P.; Field, N.; Tanton, C.; Macdowall, W.; Clifton, S.; Hughes, G.; Nardone, A.; Wellings, K.; Johnson, A.M.; et al. The health and well-being of men who have sex with men (MSM) in Britain: Evidence from the third National Survey of Sexual Attitudes and Lifestyles (Natsal-3). BMC Public Health 2016, 16, 525. [Google Scholar] [CrossRef] [Green Version]
- Davies, M.; Moon, G.; Lewis, N.M. Substance use and sexuality: Comparing sexual identity and attraction using a multilevel multivariate model. Wellbeing Space Soc. 2021, 2, 100052. [Google Scholar] [CrossRef]
- Daly, F.P.; O’Donnell, K.; Davoren, M.P.; Noone, C.; Weatherburn, P.; Quinlan, M.; Foley, B.; Igoe, D.; Barrett, P.M. Alcohol use disorder among MSM in Ireland—Findings from the European MSM internet survey (EMIS 2017). Drug Alcohol Depend. 2021, 223, 108698. [Google Scholar] [CrossRef]
- Glass, R.; Hope, V.D.; Tanner, C.; Desai, M. ‘Slamming’ among men who have sex with men accessing general drug services, in response to Schmidt, AJ et al., 2016, Illicit drug use among gay and bisexual men in 44 cities: Findings from the European MSM Internet Survey (EMIS). Int J. Drug Policy 2017, 49, 24–25. [Google Scholar] [CrossRef]
- Prah, P.; Hickson, F.; Bonell, C.; McDaid, L.M.; Johnson, A.M.; Wayal, S.; Clifton, S.; Sonnenberg, P.; Nardone, A.; Erens, B.; et al. Men who have sex with men in Great Britain: Comparing methods and estimates from probability and convenience sample surveys. Sex. Transm Infect. 2016, 92, 455–463. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
| Survey | Accessibility and Year | Background and Design | Types of Sexuality Variables Available | Types of Substance Use Covered | Other Considerations |
|---|---|---|---|---|---|
| Adult Psychiatric Morbidity Survey (APMS) | Available through the UKDS, years 2007 and 2014 are the latest available | This survey aims to give insight into psychiatric disorders, including mood disorders, substance use disorders, personality disorders and anxiety disorders in adults over 16 in England. The methodology used a multi-stage stratified sample of individuals in private households, with one adult randomly selected from households with more than one adult. | Self-reported sexual orientation and past sexual behaviours | Tobacco consumption, alcohol use and illicit substances | Survey looks at England only |
| Annual Population Survey (APS) | Quarterly waves since 2004 | This survey encompasses variables from the labour force survey, which measures employment and unemployment in the UK population .Data is collected quarterly from random households. A rotational sampling design is used, where households, not people, are selected for five consecutive quarters. Data is available in annual waves, containing quarterly datasets for that year. | Self-reported sexual orientation | Smoking | |
| British Household Panel Survey/Understanding Society (BHPS/US) | Available through the UKDS. BHPS wave available from 1991 until 2009, understanding Society continued the sample from wave 2; latest available wave is for 2018 | The BHPS and US are general household surveys The sample design for BHPS used a stratified cluster design, with 250 PSUs in GB, with all adults interviewed in a household. More households and boost samples were added in later waves. The first wave of BHPS in 1991 was 9092 adults interviewed within households. The former BHPS sample was included from wave 2 of US, with those who were still part of BHPS at wave 18 and gave consent to being contacted for taking part in US. US also had a general population sample, which again used postcode sectors as PSUs, where addresses were then selected from these. | Self-reported sexual orientation | Smoking only in BHPS. Smoking, alcohol, both illicit and legal recreational drug use in US | Sexual orientation available in waves 3 and 5 of Understanding Society only |
| European Men who have sex with men Internet Survey (EMIS) | Accessible through the data owner at the London School of Hygiene and Tropical Medicine; two waves in 2010 and 2017 | Two cross-sectional waves. EMIS was an online-administered survey, translated into 25 languages. EMIS was accessible in 38 countries, though the UK-only data was made accessible from the data owner at the London School of Hygiene and Tropical Medicine. EMIS was promoted through social networking sites, blogs, NGO websites and via posters in gay venues. Promotion through the website was either paid or unpaid, depending on the agreement. | Sexuality variables were captured through self-reported sexual identity, past sexual behaviour and sexual attraction | Tobacco consumption, alcohol use, both illicit and legal recreational drug use | Only data on men who have sex with men; women and heterosexual men were excluded |
| Health Survey for England (HSE) | Accessible through the UKDS, with frequent waves since 1991; latest available wave is from 2018 | This survey was administered to adults over 16 to identify general health issues amongst the English population, including physical health, mental health and health risk behaviours. This is a cross-sectional survey repeated annually. The design is a multi-stage stratified random sample collected from primary sampling units. The survey was collected from a mix of completed face-to-face interviews, self-completed questionnaires and a nurse visit to collect biometric data. | Self-reported sexual orientation | Smoking, tobacco, e-cigarettes and alcohol | |
| National Survey for Wales (NSW) | Available through the UKDS; waves since 2013, latest available wave is from 2020 | This survey is administered to adults over 16 annually to randomly selected households, with one adult randomly selected from each household, corresponding to approximately 12,000 individuals each year. | Self-reported sexual orientation | Smoking, e-cigarettes and alcohol use | Sexual orientation included only until 2019 due to a shorter telephone survey in 2020 due to the COVID-19 pandemic |
| National Survey of Sexual Attitudes and Lifestyle (NATSAL) | Three waves from 1990–2010 | NATSAL is a survey about sexual behaviours in Great Britain that has been widely used in research and to inform sexual health interventions and programmes NATSAL used multi-stage, clustered and stratified probability design, whereby an individual was selected at random from addresses that were selected within primary sampling units. | Sexuality variables captured through self-reported sexual identity, past sexual behaviour and sexual attraction | Smoking, alcohol use, both illicit and legal recreational drug use | |
| Scottish Health Survey (SHS) | Started in 1995, with a wave in 1998 and 2003, then annual waves since 2008 | This survey was administered to adults over 16 to identify general health issues amongst the Scottish population including physical health, mental health and health risk behaviours. This is a cross-sectional survey repeated annually. The design is a multi-stage stratified random sample. The addresses were drawn by the Scottish Government since 2012. The survey was collected from a mix of completed face-to-face interviews and self-completed questionnaires. | Self-reported sexual orientation | Smoking, tobacco, e-cigarettes and alcohol use | Sexual orientation variable not available from 2014 due to confidentiality concerns; looks at Scotland only |
| The General Practitioner Patient Survey (GPPS) | Access through contacting survey team at https://www.gp-patient.co.uk accessed on 20 January 2022 | Cross-sectional survey with annual waves since 2007. A sample of eligible patients (had a valid NHS number, registered with a GP practice for at least 6 months before, registered with a GP practice in England, aged 16 and over) from practices that opted in to receive the survey were sent invites. | Self-reported sexual orientation | Smoking | Looks at GP practices in England only |
| UK Biobank | Accessible through the UK Biobank website. Two time periods of 2006–2010 and a follow up of 2011–2012 are available | Longitudinal survey looking at the link between diet and multiple health outcomes in middle-aged individuals across the UK. Individuals registered with the NHS aged 40–69 living in a certain proximity to assessment centres were invited to take part. | Sexual behaviour only—number of same-sex sexual partners during lifetime | Smoking, alcohol use and illicit drug use | Costs associated with access, which might not be available to all researchers |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Davies, M.; Moon, G.; Sabel, C.E. Navigating the LGB Data Landscape: A Review of Appropriate Secondary Data Sources for Sexuality and Substance Use Research in the UK. Int. J. Environ. Res. Public Health 2022, 19, 1329. https://doi.org/10.3390/ijerph19031329
Davies M, Moon G, Sabel CE. Navigating the LGB Data Landscape: A Review of Appropriate Secondary Data Sources for Sexuality and Substance Use Research in the UK. International Journal of Environmental Research and Public Health. 2022; 19(3):1329. https://doi.org/10.3390/ijerph19031329
Chicago/Turabian StyleDavies, Megan, Graham Moon, and Clive E. Sabel. 2022. "Navigating the LGB Data Landscape: A Review of Appropriate Secondary Data Sources for Sexuality and Substance Use Research in the UK" International Journal of Environmental Research and Public Health 19, no. 3: 1329. https://doi.org/10.3390/ijerph19031329
APA StyleDavies, M., Moon, G., & Sabel, C. E. (2022). Navigating the LGB Data Landscape: A Review of Appropriate Secondary Data Sources for Sexuality and Substance Use Research in the UK. International Journal of Environmental Research and Public Health, 19(3), 1329. https://doi.org/10.3390/ijerph19031329