
Factors Associated with the Willingness to Become a Living Kidney Donor: A National Cross-Sectional Study





Abstract
:1. Introduction
2. Materials and Methods
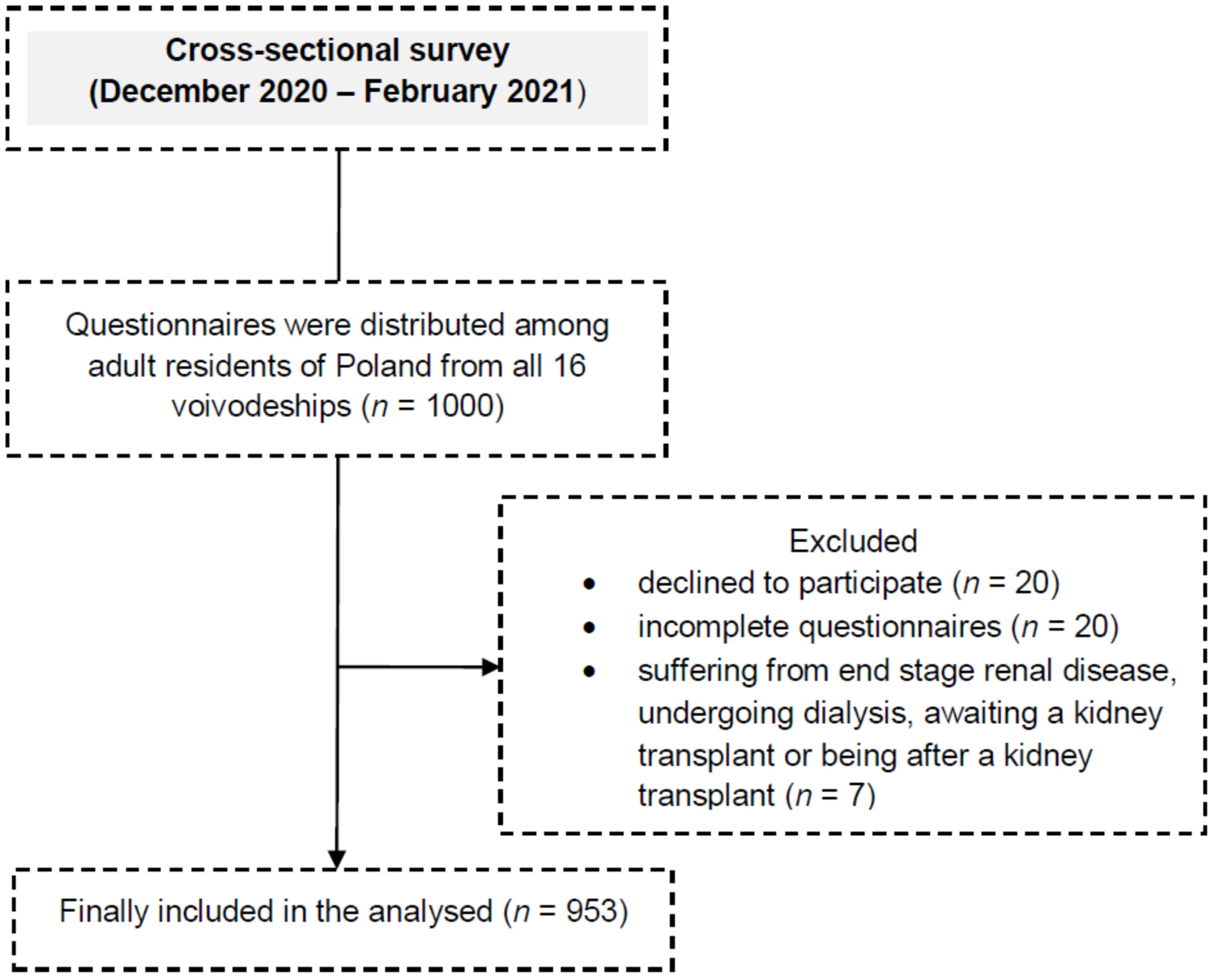
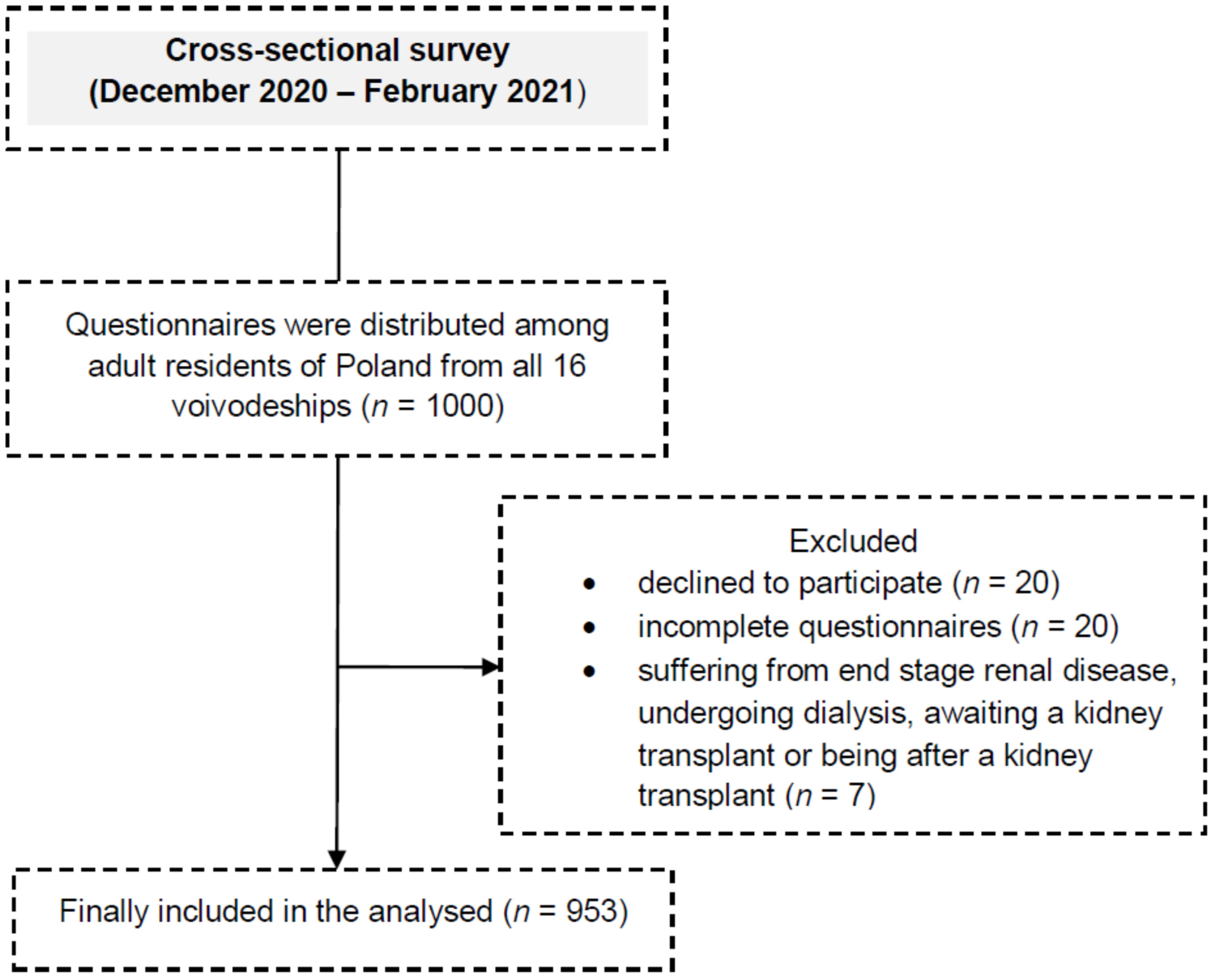
2.1. Study Design, Setting
2.2. Participants
2.3. Instruments
2.4. Outcomes
2.5. Statistical Methods
3. Results
3.1. Sociodemographic Factors
3.2. Willingness to Became a Living Kidney Donor
3.3. List of Personal Values
3.4. Life Satisfaction
3.5. Assessment of Factors Determining Kidney Donation Willingness
3.6. Assessment of Factors Determining Willingness to Donate a Kidney to a Stranger
4. Discussion
5. Strengths and Limitations
6. Conclusions
7. Implications for Clinical Practice
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rodrigue, J.R.; Kazley, A.S.; Mandelbrot, D.A.; Hays, R.; LaPointe Rudow, D.; Baliga, P. American Society of Transplantation. Living Donor Kidney Transplantation: Overcoming Disparities in Live Kidney Donation in the US-Recommendations from a Consensus Conference. Clin. J. Am. Soc. Nephrol. 2015, 10, 1687–1695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dębska-Ślizień, A.; Bello, A.K.; Johnson, D.W.; Jha, V.; Harris, D.C.H.; Levin, A.; Tonelli, M.; Saad, S.; Zaidi, D.; Osman, M.A.; et al. International Society of Nephrology Global Kidney Health Atlas: Structures, organization, and services for the management of kidney failure in Eastern and Central Europe. Kidney Int. Suppl. 2021, 11, e24–e34. [Google Scholar] [CrossRef] [PubMed]
- Barnieh, L.; Collister, D.; Manns, B.; Lam, N.N.; Shojai, S.; Lorenzetti, D.; Gill, J.S.; Klarenbach, S.A. A Scoping Review for Strategies to Increase Living Kidney Donation. Clin. J. Am. Soc. Nephrol. 2017, 12, 1518–1527. [Google Scholar] [CrossRef] [PubMed]
- Al Ammary, F.; Yu, Y.; Ferzola, A.; Motter, J.D.; Massie, A.B.; Yu, S.; Thomas, A.G.; Crews, D.C.; Segev, D.L.; Muzaale, A.D.; et al. The first increase in live kidney donation in the United States in 15 years. Am. J. Transplant. 2020, 20, 3590–3598. [Google Scholar] [CrossRef] [PubMed]
- Durlik, M. History of kidney transplantation in Poland. G. Ital. Nefrol. 2018, 35, 84–86. [Google Scholar]
- Centrum Organizacyjno-Koordynacyjne do Spraw Transplantacji-Poltransplant. Biul. Inf. 2020. Available online: http://www.poltransplant.pl/Download/Biuletyn2020.pdf (accessed on 2 November 2021).
- Global Observatory on Donation and Transplantation. Available online: http://www.transplant-observatory.org/summary/ (accessed on 10 November 2021).
- Hermanowicz, M.; Borczon, S.; Lewandowska, D.; Przygoda, J.; Podobińska, I.; Danielewicz, R.; Malanowski, P.; Kamiński, A.; Czerwiński, J. Quality System of Kidney Donation for Transplantation from Living Donors in Poland. Transpl. Proc. 2020, 52, 2033–2035. [Google Scholar] [CrossRef]
- Dz. U. 2005 Nr 169 Poz. 1411. Ustawa z Dnia 1 Lipca 2005 r. o Pobieraniu, Przechowywaniu i Przeszczepianiu Komórek, Tkanek i Narządów. 2005. Available online: http://isap.sejm.gov.pl/isap.nsf/download.xsp/WDU20051691411/U/D20051411Lj.pdf (accessed on 1 November 2021).
- Wadström, J.; von Zur-Mühlen, B.; Lennerling, A.; Westman, K.; Wennberg, L.; Fehrman Ekholm, I. Living anonymous renal donors do not regret: Intermediate and long-term follow-up with a focus on motives and psychosocial outcomes. Ann. Transplant. 2019, 24, 234–241. [Google Scholar] [CrossRef]
- Wasser, W.G.; Boner, G.; Koslowsky, M.; Lazar, A. Emergence of an Israel faith-based community organization facilitating live donor kidney transplantation. BMC Nephrol. 2018, 19, 128. [Google Scholar] [CrossRef] [Green Version]
- Fry-Revere, S.; Chen, D.; Bastani, B.; Golestani, S.; Agarwal, R.; Kugathasan, H.; Le, M. Coercion, dissatisfaction, and social stigma: An ethnographic study of compensated living kidney donation in Iran. Int. Urol. Nephrol. 2020, 52, 2403–2414. [Google Scholar] [CrossRef]
- Nagi, K.; Srinivasan, M.; Lekamlage, P.B.; Bramstedt, K.A. Exploring the success of Good Samaritan organ donation in New Zealand. Prog. Transplant. 2015, 25, 160–175. [Google Scholar] [CrossRef] [PubMed]
- Faber, D.A.; Joshi, S.; Ciancio, G. Demographic characteristics of non-directed altruistic kidney donors in the United States. J. Kidney 2016, 2, 121. [Google Scholar] [CrossRef] [Green Version]
- García Martínez, M.; Valentín Muñoz, M.O.; Ormeño Gómez, M.; Martínez Alpuente, I.; Dominguez-Gil González, B. Can We Improve the Effectiveness of the Spanish Nondirected Donation Program? Transpl. Proc. 2019, 51, 3030–3033. [Google Scholar] [CrossRef] [PubMed]
- Okita, T.; Hsu, E.; Aizawa, K.; Nakada, H.; Toya, W.; Matsui, K. Quantitative Survey of Laypersons’ Attitudes Toward Organ Transplantation in Japan. Transpl. Proc. 2018, 50, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Colaneri, J.; Billman, R.; Branch, J.; Derkowski, D.; Frey, G.; Woodard, A. Dissolving Disincentives to Living Kidney Donation. Nephrol. Nurs. J. 2021, 48, 481–488. [Google Scholar] [CrossRef] [PubMed]
- Yan, J.; Wang, Y.; Shao, J.; Yuan, H. Attitudes Toward Living Organ Donation and Willingness to Be a Living Organ Donor Among Chinese Citizens in 3 Cities. Transpl. Proc. 2018, 50, 3065–3070. [Google Scholar] [CrossRef]
- Petpichetchian, W.; Kitbunyonglers, S.; Kitrungrote, L. Nurses’ Values, Beliefs and Roles Regarding Organ Donation. PRIJNR 2015, 19, 232–244. Available online: https://he02.tci-thaijo.org/index.php/PRIJNR/article/view/22395 (accessed on 21 January 2022).
- Dalal, A.R. Philosophy of organ donation: Review of ethical facets. World J. Transplant. 2015, 5, 44–51. [Google Scholar] [CrossRef]
- Milaniak, I.; Wilczek-Rużyczka, E.; Przybyłowski, P. Role of Empathy and Altruism in Organ Donation Decision making Among Nursing and Paramedic Students. Transpl. Proc. 2018, 50, 1928–1932. [Google Scholar] [CrossRef]
- Jankowski, K.S. Is the shift in chronotype associated with an alteration in well-being? Biol. Rhythm. Res. 2015, 46, 237–248. [Google Scholar] [CrossRef]
- Messersmith, E.E.; Gross, C.R.; Beil, C.A.; Gillespie, B.W.; Jacobs, C.; Taler, S.J.; Merion, R.M.; Jowsey, S.G.; Leichtman, A.B.; Hong, B.A.; et al. Satisfaction With Life Among Living Kidney Donors: A RELIVE Study of Long-Term Donor Outcomes. Transplantation 2014, 98, 1294–1300. [Google Scholar] [CrossRef] [PubMed]
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M. STROBE Initiative. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. Int. J. Surg. 2014, 12, 1500–1524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Juczyński, Z. Measuring tools used in psychology and health promotion and psychology. Pol. Psychol. Soc. 2001, 87, 128. [Google Scholar]
- Diener, E.; Emmons, R.A.; Larsen, R.J.; Griffin, S. The Satisfaction With Life Scale. J. Pers. Assess. 1985, 49, 71–75. [Google Scholar] [CrossRef]
- Daniel, W.W. Biostatistics: A Foundation for Analysis in the Health Sciences, 7th ed.; John Wiley Sons: New York, NY, USA, 1999; pp. 141–142. [Google Scholar]
- Ríos Zambudio, A.; López-Navas, A.I.; Garrido, G.; Ayala-García, M.A.; Sebastián, M.J.; Hernández, A.M.; Ramírez, P.; Parrilla, P. Attitudes of Latin American Immigrants Resident in Florida (United States) Toward Related Living Kidney Do-nation. Prog. Transplant. 2019, 29, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Spital, A. Public attitudes toward kidney donation by friends and altruistic strangers in the United States. Transplantation 2001, 71, 1061–1064. [Google Scholar] [CrossRef]
- Viklicky, O.; Krivanec, S.; Vavrinova, H.; Berlakovich, G.; Marada, T.; Slatinska, J.; Neradova, T.; Zamecnikova, R.; Salat, A.; Hofmann, M.; et al. Crossing borders to facilitate live donor kidney transplantation: The Czech-Austrian kidney paired donation program—a retrospective study. Transpl. Int. 2020, 33, 1199–1210. [Google Scholar] [CrossRef]
- Ríos, A.; López-Navas, A.; Martínez-Alarcón, L.; Ramírez, P.; Parrilla, P. Latin Americans in Spain and their attitude toward living kidney donation. Clin. Transplant. 2015, 29, 1054–1062. [Google Scholar] [CrossRef] [PubMed]
- Meng, O.Y.; Lim, C.; Leng, C.W.; van der Erf, S.; Joshi, V.D.; Sin, S.T.; Hong, S.T.; Chye, P.G.; Seng, G.T.; Yi-Shern, T.K. Factors influencing living kidney donation in Singapore. Prog. Transplant. 2012, 22, 95–101. [Google Scholar] [CrossRef]
- Kurleto, P.; Skorupska-Król, A.; Broniatowska, E.; Bramstedt, K.A. Exploring the motives of Israeli Jews who were living kidney donors to strangers. Clin. Transplant. 2020, 34, e14034. [Google Scholar] [CrossRef] [PubMed]
- Maple, H.; Chilcot, J.; Burnapp, L.; Gibbs, P.; Santhouse, A.; Norton, S.; Weinman, J.; Mamode, N. Motivations, outcomes, and characteristics of unspecified (nondirected altruistic) kidney donors in the United Kingdom. Transplantation 2014, 98, 1182–1189. [Google Scholar] [CrossRef] [PubMed]
- Prasad, G.V.R. Understanding the sex disparity in living kidney donation. J. Eval. Clin. Pract. 2018, 24, 999–1004. [Google Scholar] [CrossRef] [PubMed]
- Nowicki, G.J.; Misztal-Okońska, P.; Ślusarska, B.; Rudnicka-Drożak, E.; Młynarska, M.; Czekierdowski, A. Analysis of Health Behaviors and Personal Values of Childless Women, Pregnant Women and Women Who Recently Delivered. Int. J. Environ. Res. Public Health 2018, 15, 411. [Google Scholar] [CrossRef] [Green Version]
- Andersen, M.H.; Mathisen, L.; Øyen, O.; Wahl, A.K.; Hanestad, B.R.; Fosse, E. Living donors’ experiences 1 wk after donating a kidney. Clin. Transplant. 2005, 19, 90–96. [Google Scholar] [CrossRef]
- McGrath Pun, P.; Holewa, H. Decision-making for living kidney donors: An instinctual response to suffering and death. Mortality 2012, 17, 201–220. [Google Scholar] [CrossRef]
- Farahani, Z.B.; Esmaeili, M.; Salsali, M.; Nayeri, N. Factors affecting Iranian family donors’ motivation for kidney donation. Acta Med. Mediterranea 2016, 32, 1067–1073. [Google Scholar]
- Ummel, D.; Achille, M. Transplant trajectory and relational experience within living kidney dyads. Qual. Health Res. 2016, 26, 194–203. [Google Scholar] [CrossRef]
- Meyer, K.B.; Bjørk, I.T.; Wahl, A.K.; Lennerling, A.; Andersen, M.H. Long-term experiences of Norwegian live kidney donors: Qualitative in-depth interviews. BMJ Open 2017, 7, e014072. [Google Scholar] [CrossRef] [Green Version]
- Jacobs, C.; Berglund, D.M.; Wiseman, J.F.; Garvey, C.; Larson, D.B.; Voges, M.; Radecki Breitkopf, C.; Ibrahim, H.N.; Matas, A.J. Long-term psychosocial outcomes after nondirected donation: A single-center experience. Am. J. Transplant. 2019, 19, 1498–1506. [Google Scholar] [CrossRef]
- Gaillard, F.; Jacquemont, L.; Roberts, V.; Albano, L.; Allard, J.; Bouvier, N.; Buchler, M.; Titeca-Beauport, D.; Couzi, L.; Delahousse, M.; et al. Temporal trends in living kidney donation in France between 2007 and 2017. Nephrol. Dial. Transplant. 2021, 36, 730–738. [Google Scholar] [CrossRef] [PubMed]
- Bieniasz, M.; Kieszek, R.; Jakubowska-Winecka, A.; Zatorski, M.; Kwapisz, M.; Jędrzejko, K.; Nita, M.; Durlik, M.; Pączek, L.; Kwiatkowski, A. Psychological Aspects of Living Kidney Donation in Poland: Experience of One Center. Transpl. Proc. 2018, 50, 1637–1639. [Google Scholar] [CrossRef] [PubMed]
- Polska w Liczbach 2020. Available online: https://stat.gov.pl/files/gfx/portalinformacyjny/pl/defaultaktualnosci/5501/14/13/1/polska_w_liczbach_2020_pl.pdf (accessed on 9 January 2021).
- Główny Urząd Statystyczny. Analizy Statystyczne. Kapitał Ludzki w Polsce w Latach 2014–2018. Available online: https://stat.gov.pl/files/gfx/portalinformacyjny/pl/defaultaktualnosci/5501/8/7/1/kapital_ludzki_w_polsce_w_latach_2014-2018.pdf (accessed on 9 January 2021).
- Eurostat. Demographic Change in Europe—Country Factsheets: Poland. Available online: https://ec.europa.eu/eurostat/documents/10186/10994376/PL-EN.pdf (accessed on 6 December 2021).
- O’Keeffe, L.M.; Ramond, A.; Oliver-Williams, C.; Willeit, P.; Paige, E.; Trotter, P.; Evans, J.; Wadström, J.; Nicholson, M.; Collett, D.; et al. Mid- and Long-Term Health Risks in Living Kidney Donors: A Systematic Review and Meta-analysis. Ann. Intern. Med. 2018, 168, 276–284. [Google Scholar] [CrossRef] [PubMed]
- Lentine, K.L.; Lam, N.N.; Segev, D.L. Risks of Living Kidney Donation: Current State of Knowledge on Outcomes Important to Donors. Clin. J. Am. Soc. Nephrol. 2019, 14, 597–608. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
| Variable | |
|---|---|
| Age (years, Me, Q25; Q75) | 41 [30; 60] |
| Sex | |
| Female | 497 (52.1%) |
| Male | 456 (47.8%) |
| Marital status: married | 618 (64.8%) |
| Children—yes | 578 (60.6%) |
| Siblings—yes | 798 (83.6%) |
| Education | |
| University | 280 (29.3%) |
| Other (High school/Vocational education/Primary school) | 673 (70.5%) |
| Employment status: employed/pensioner/retired | 682 (71.5%) |
| Place of residence | |
| City | 753 (78.9%) |
| Village | 200 (21.0%) |
| Religious self-identity: Catholic | 672 (70.4%) |
| Symbols of Happiness | Me [Q25; Q75] | Personal Value | Me [Q25; Q75] |
|---|---|---|---|
| Good health | 5 [5; 5] | Good health, physical and mental fitness | 5 [4; 5] |
| Successful family life | 4 [4; 4] | Love and friendship | 4 [4; 4] |
| Being needed by other people | 3 [2; 3] | Knowledge and wisdom | 3 [1; 3] |
| Doing your favorite job, having fun | 2 [1; 2] | Intelligence, mental acuity | 2 [1; 2] |
| Good material conditions | 1 [0; 2] | Joy, contentment | 1 [0; 2] |
| Scientific and professional success | 0 [0; 0] | Goodness, tenderness | 0 [0; 0] |
| Having a lot of friends | 0 [0; 0] | Courage, decisiveness | 0 [0; 0] |
| A life full of adventures, travels | 0 [0; 0] | Sense of humor, witticism | 0 [0; 0] |
| Fame, popularity | 0 [0; 0] | Nice look, appearance | 0 [0; 0] |
| Wealth, possession | 0 [0; 0] |
| Variables | B | SE (B) | Wald Test | Df | P | OR (Cl95%) |
|---|---|---|---|---|---|---|
| Age | −0.01 | 0.005 | 6.58 | 1 | 0.010 | 0.99 (0.98−0.99) |
| The total score of the Satisfaction with Life Scale | 0.03 | 0.01 | 4.61 | 1 | 0.032 | 1.03 (1.003−1.06) |
| Gender female vs. male | 0.19 | 0.08 | 5.23 | 1 | 0.022 | 1.21 (1.03−1.42) |
| Personal value: goodness and tenderness | 0.19 | 0.07 | 6.95 | 1 | 0.008 | 1.21(1.05−1.40) |
| Symbol of happiness: a life full of adventures, travels | 0.33 | 0.14 | 5.75 | 1 | 0.017 | 1.39 (1.06−1.82) |
| Variables | B | SE (B) | Wald Test | Df | P | OR (Cl95%) |
|---|---|---|---|---|---|---|
| Age | −0.04 | 0.01 | 26.77 | 1 | <0.001 | 0.96 (0.95−0.98) |
| The total score of the Satisfaction with Life Scale | −0.05 | 0.02 | 6.84 | 1 | 0.009 | 0.95 (0.92−0.99) |
| Personal value: a sense of humor/witticism | 0.39 | 0.13 | 8.54 | 1 | 0.003 | 1.48 (1.14−1.92) |
| Support for legalization of unspecified kidney donation in Poland | 0.51 | 0.15 | 11.53 | 1 | 0.001 | 1.66 (1.24−2.23) |
| Belief, that selfless donation of a kidney to a stranger is something positive | 1.34 | 0.22 | 37.75 | 1 | <0.001 | 3.81 (2.49−5.83) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kurleto, P.; Tomaszek, L.; Milaniak, I.; Mędrzycka-Dąbrowska, W. Factors Associated with the Willingness to Become a Living Kidney Donor: A National Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 1313. https://doi.org/10.3390/ijerph19031313
Kurleto P, Tomaszek L, Milaniak I, Mędrzycka-Dąbrowska W. Factors Associated with the Willingness to Become a Living Kidney Donor: A National Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2022; 19(3):1313. https://doi.org/10.3390/ijerph19031313
Chicago/Turabian StyleKurleto, Paulina, Lucyna Tomaszek, Irena Milaniak, and Wioletta Mędrzycka-Dąbrowska. 2022. "Factors Associated with the Willingness to Become a Living Kidney Donor: A National Cross-Sectional Study" International Journal of Environmental Research and Public Health 19, no. 3: 1313. https://doi.org/10.3390/ijerph19031313
APA StyleKurleto, P., Tomaszek, L., Milaniak, I., & Mędrzycka-Dąbrowska, W. (2022). Factors Associated with the Willingness to Become a Living Kidney Donor: A National Cross-Sectional Study. International Journal of Environmental Research and Public Health, 19(3), 1313. https://doi.org/10.3390/ijerph19031313