
Prevalence of Signs of Severity Identified in the Thai Population with Malaria: A Systematic Review and Meta-Analysis


 , ,
, ,
Abstract
1. Background
2. Methods
2.1. Protocol and Registration
2.2. Search Strategy
2.3. Eligibility Criteria
2.4. Study Selection
2.5. Data Extraction
2.6. Quality of the Included Studies
2.7. Data Synthesis
3. Results
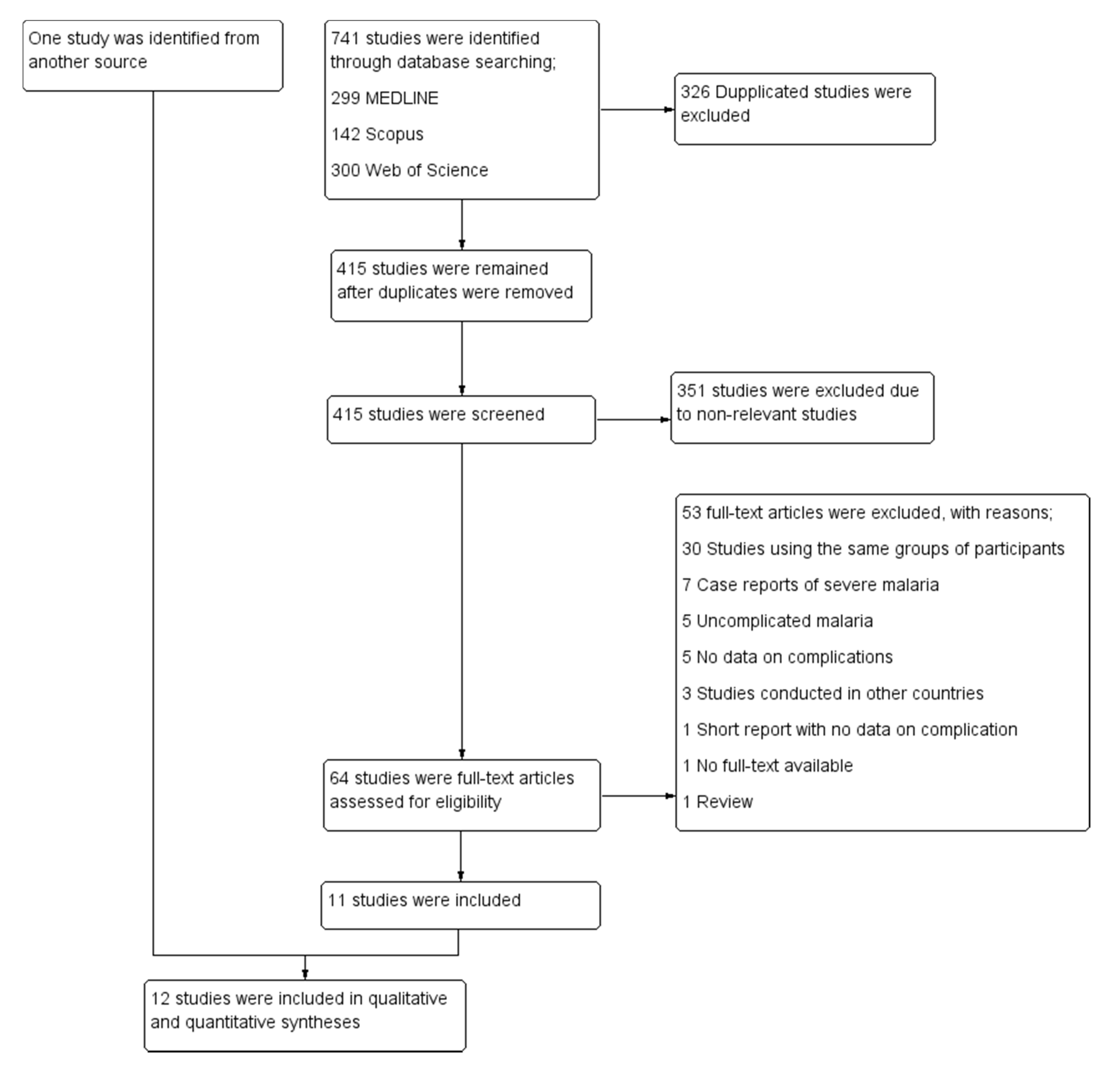
3.1. Search Results
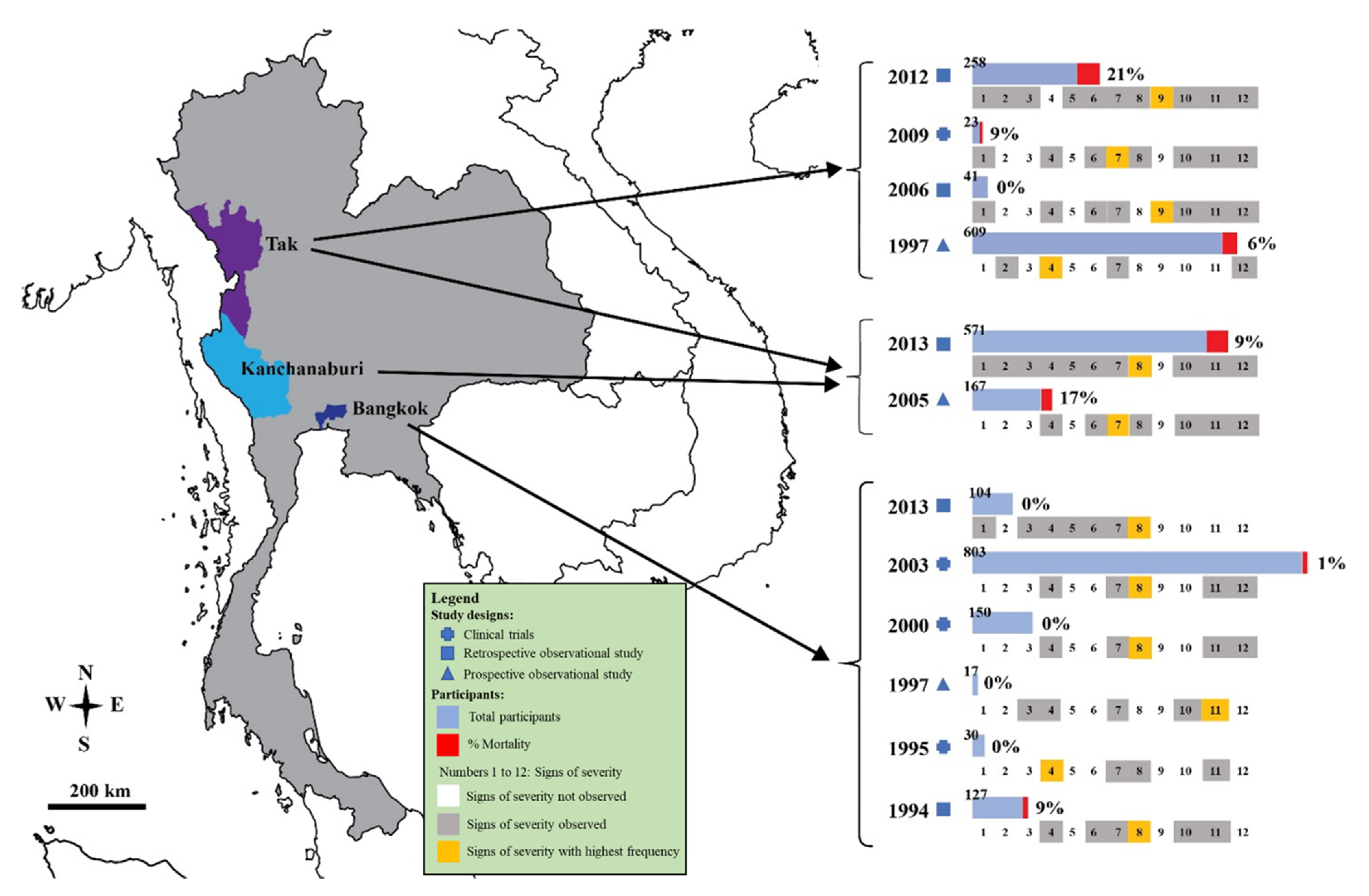
3.2. Characteristics of the Included Studies
3.3. Methodological Quality of the Included Studies
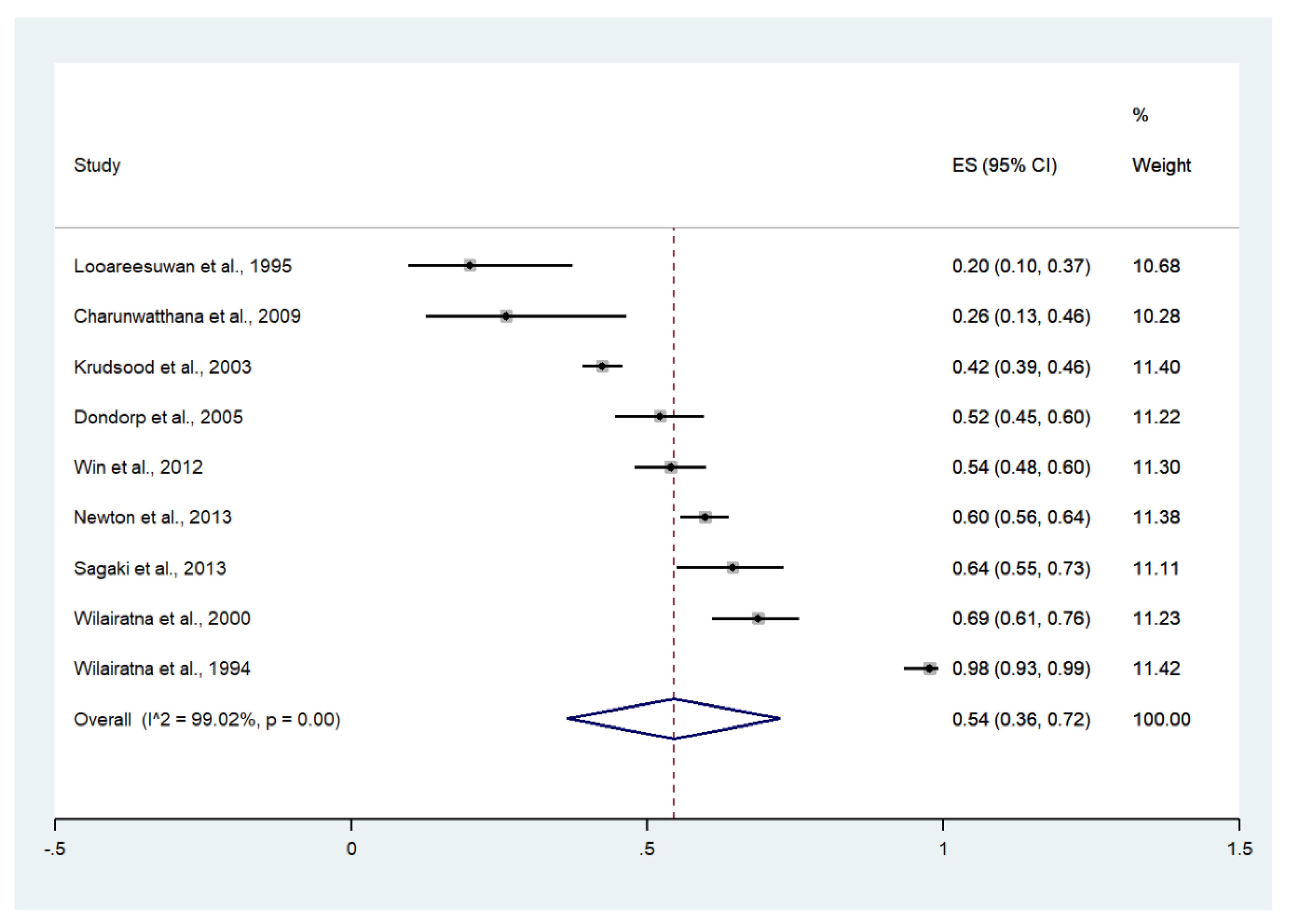
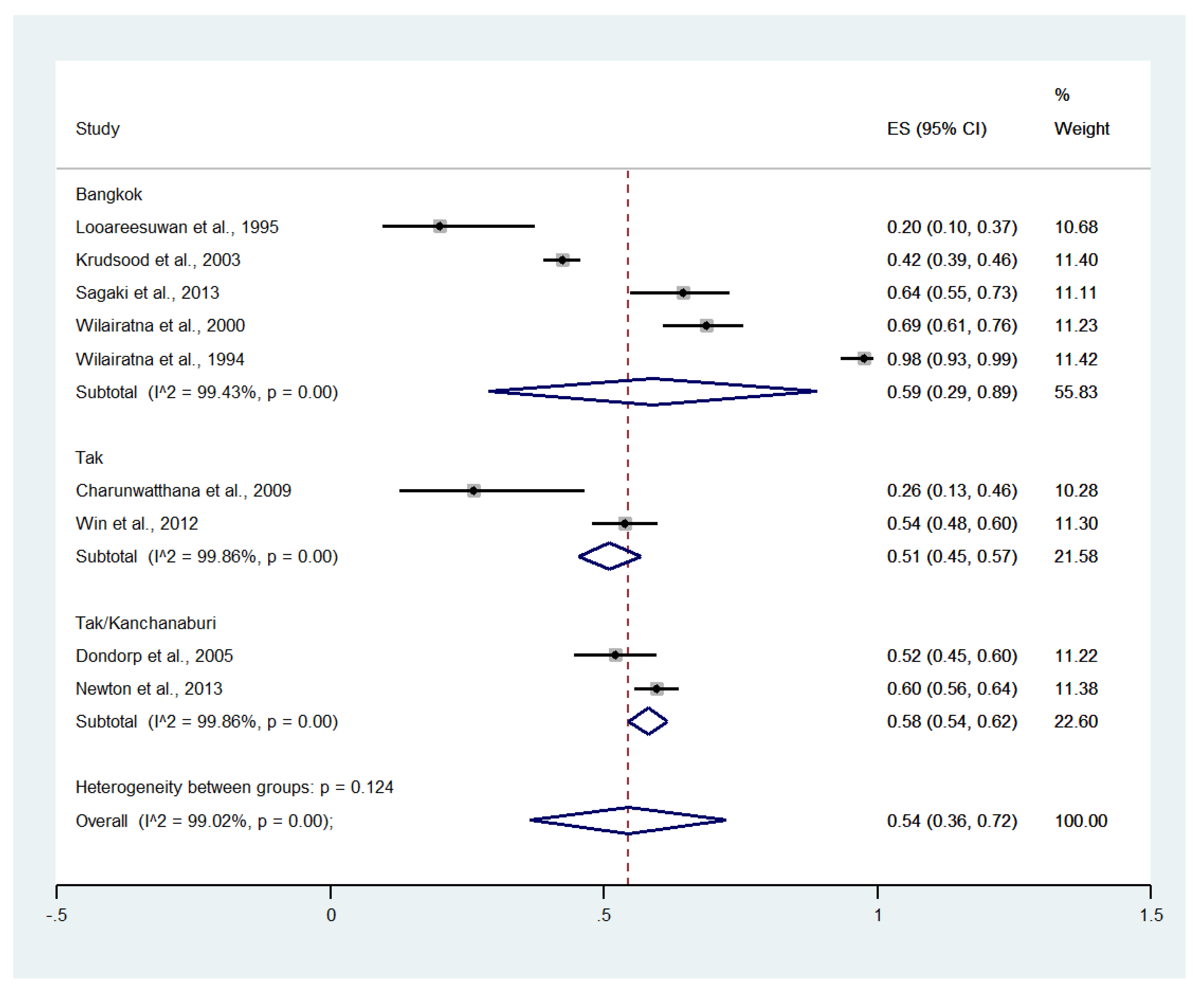
3.4. Jaundice
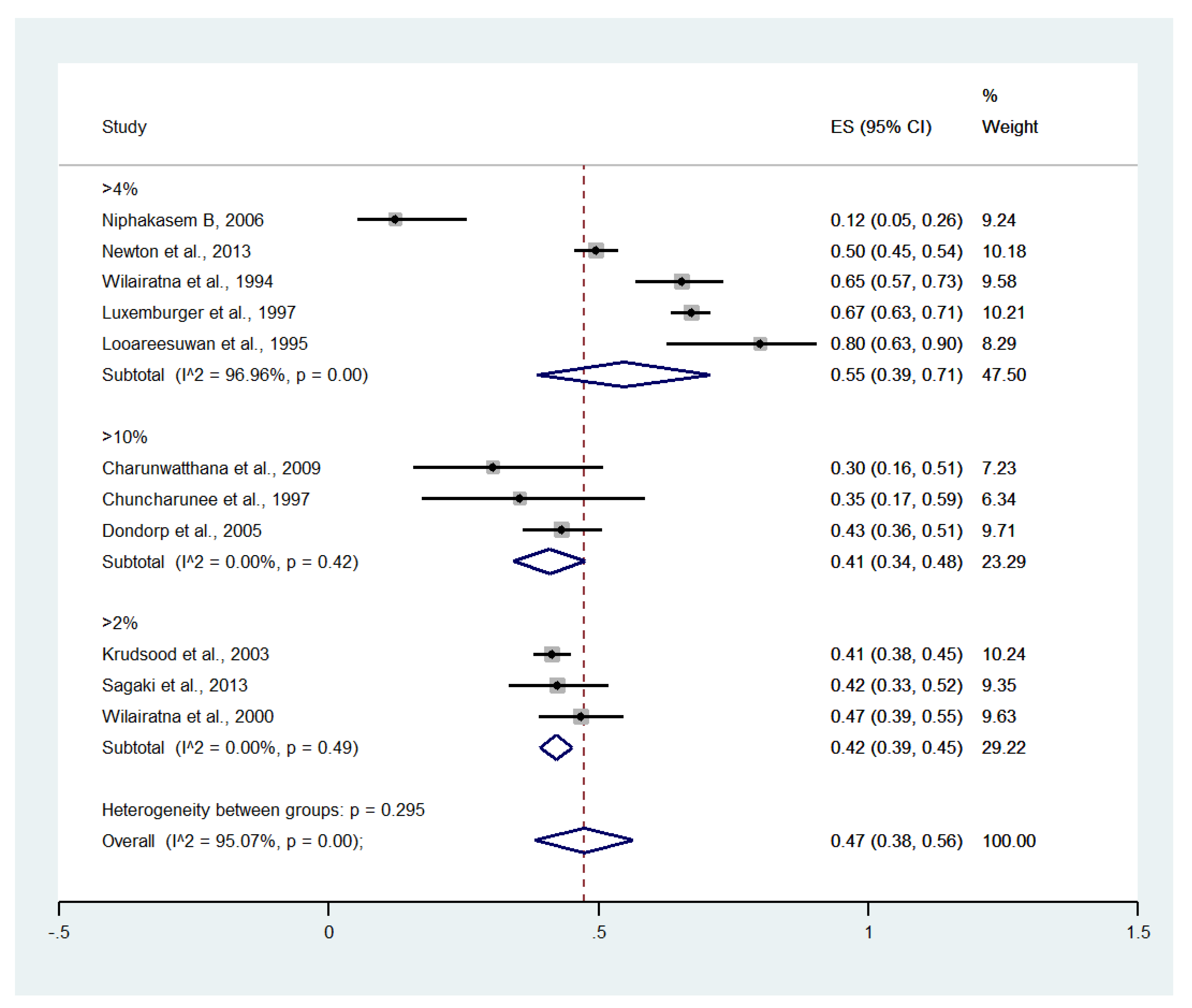
3.5. Hyperparasitemia
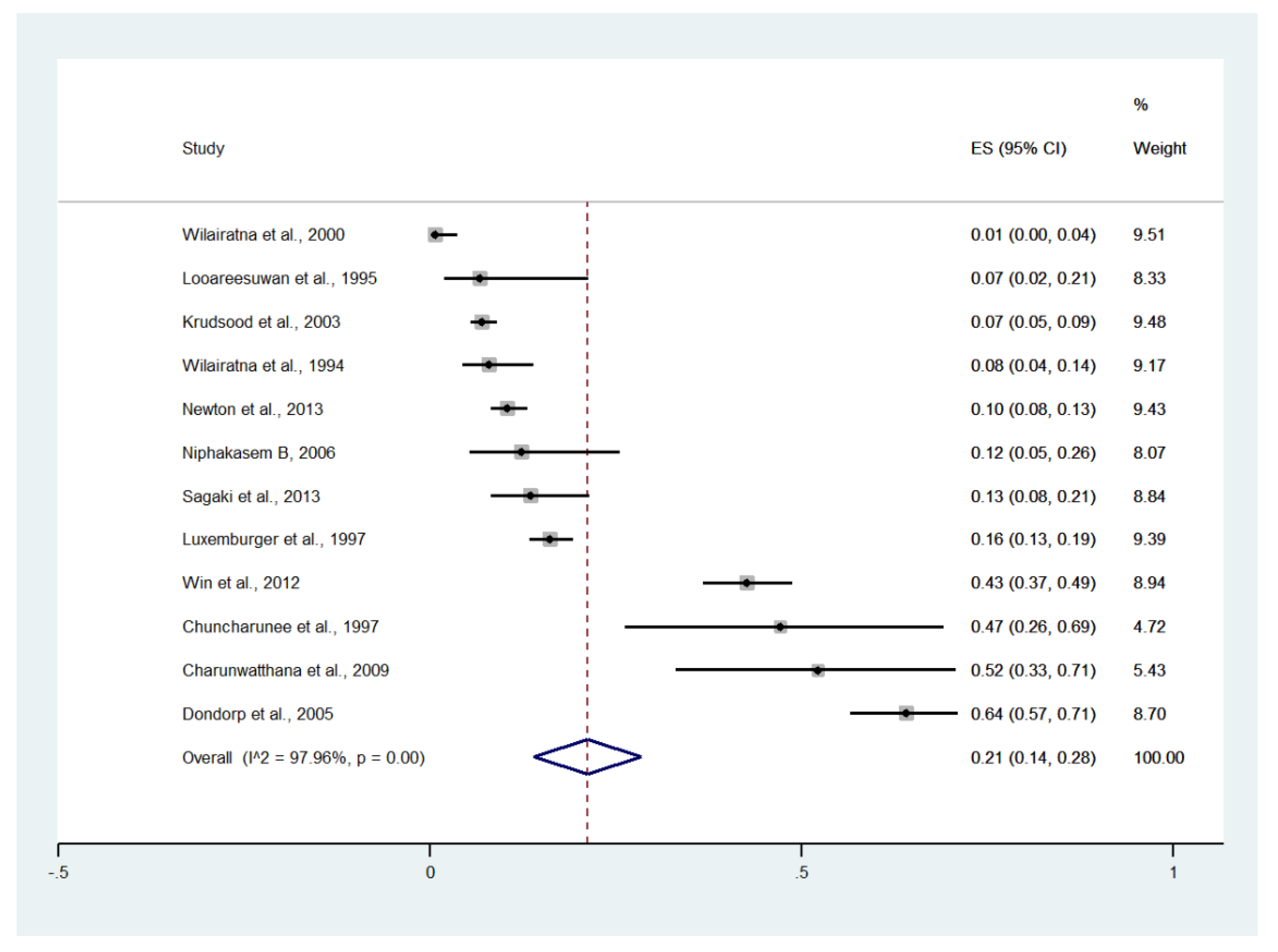
3.6. Impaired Consciousness
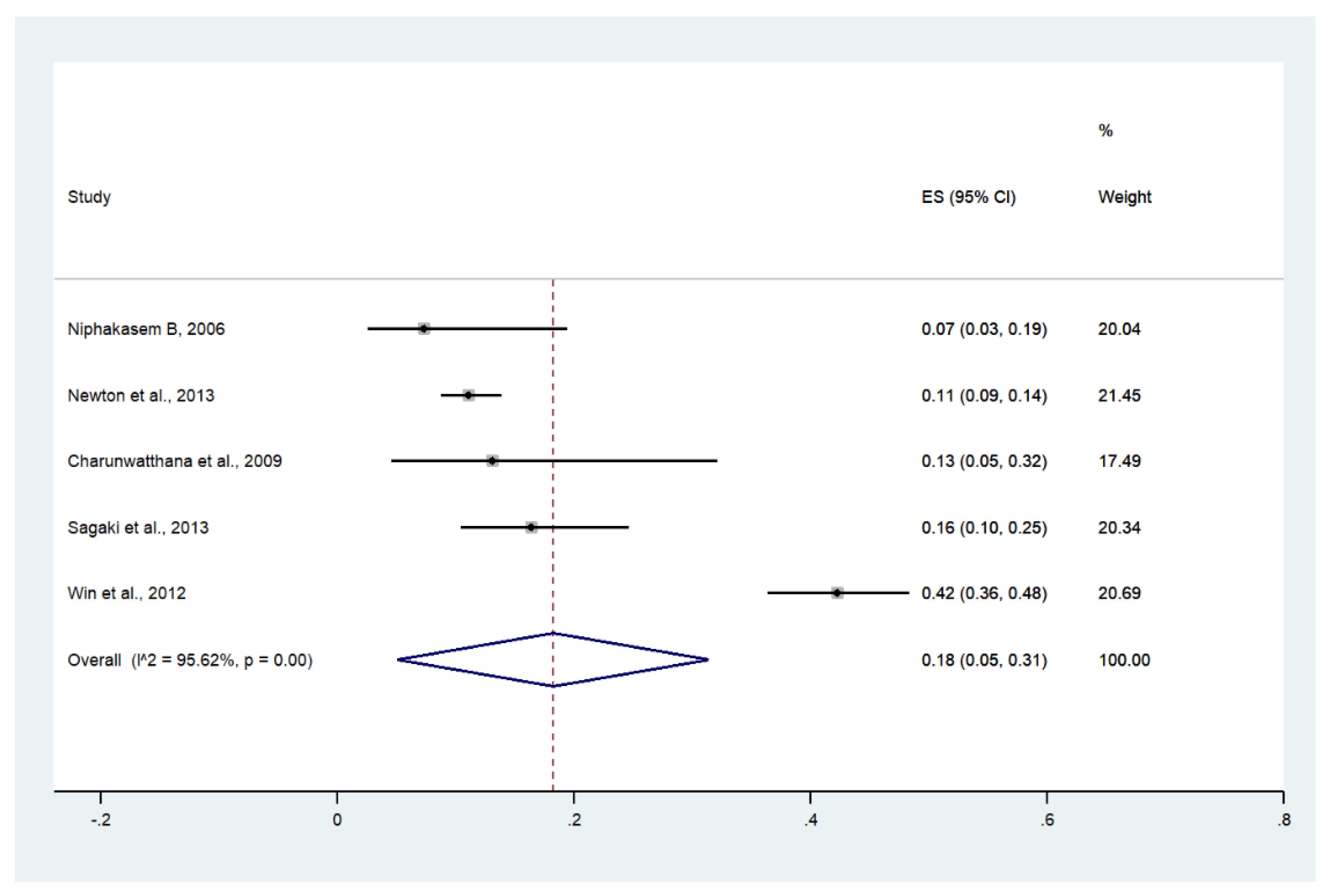
3.7. Acidosis
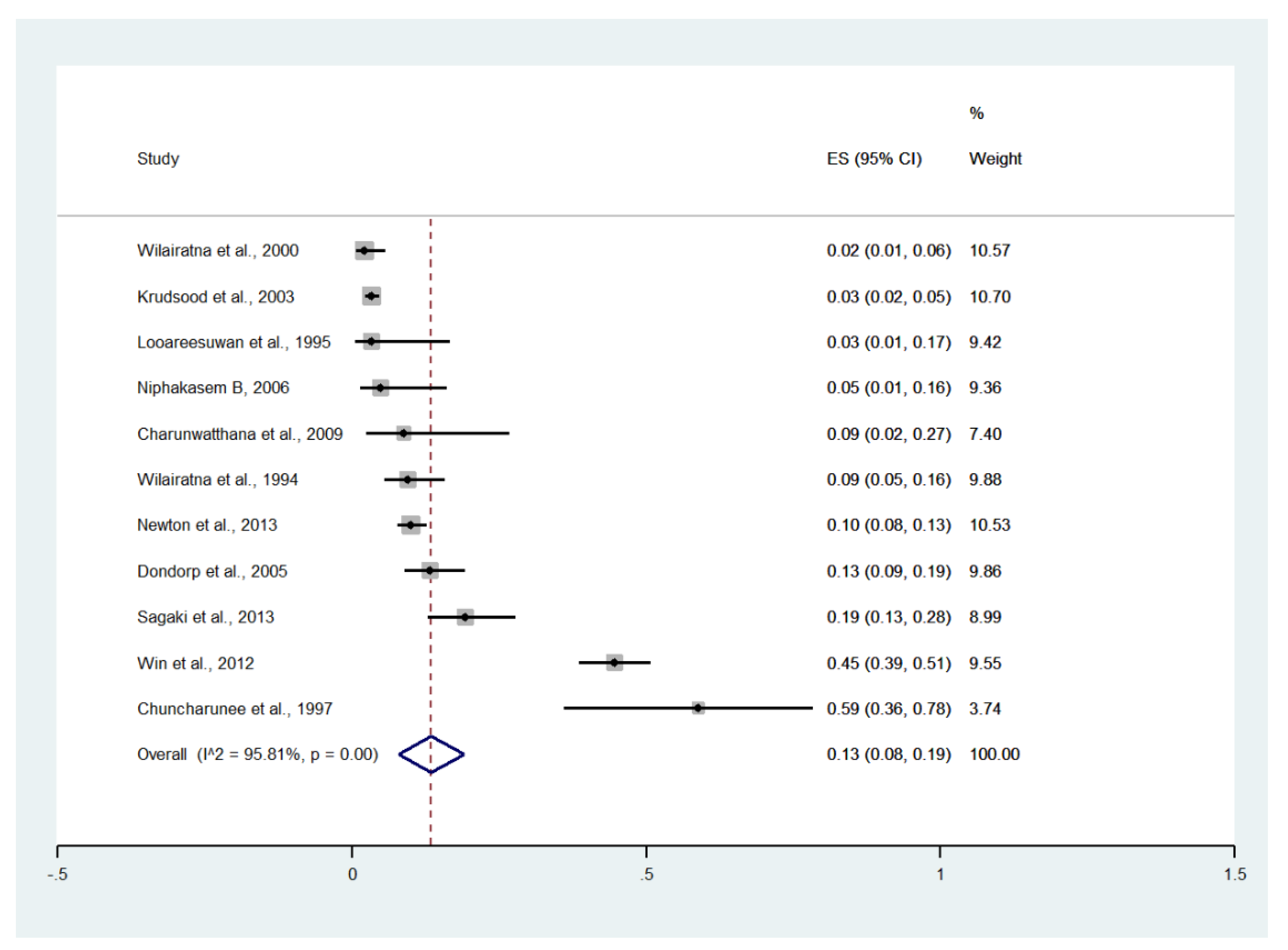
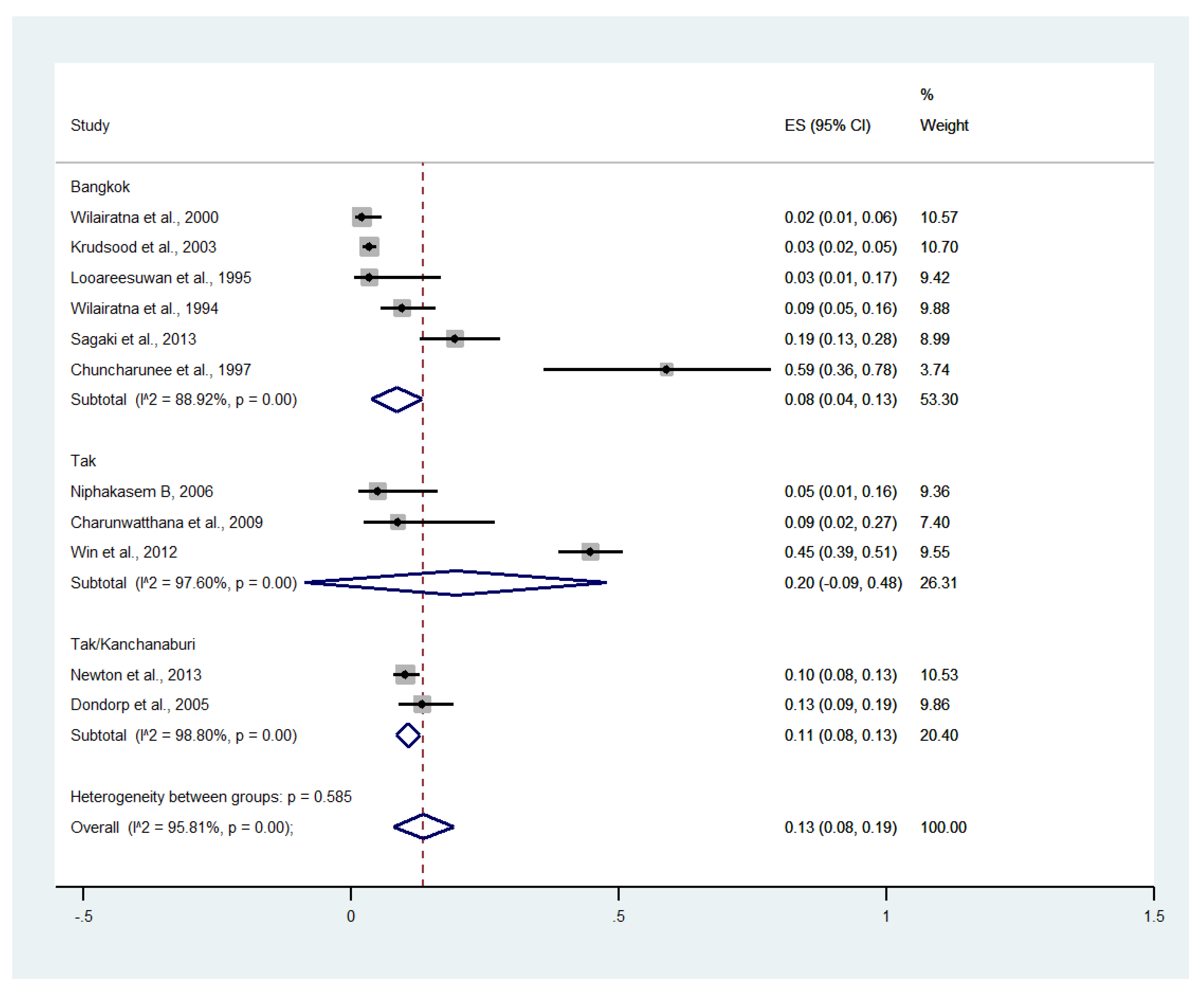
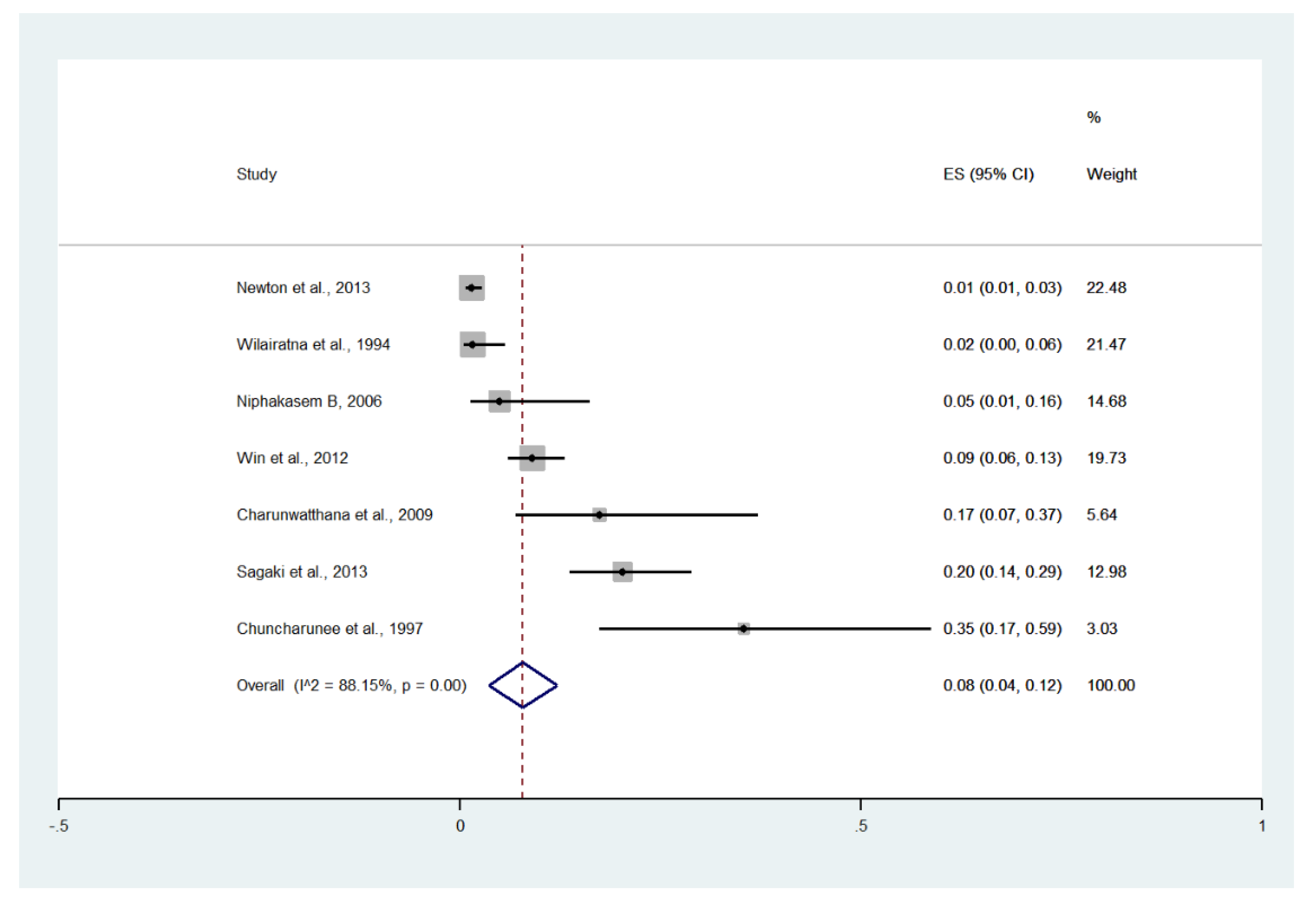
3.8. Renal Impairment
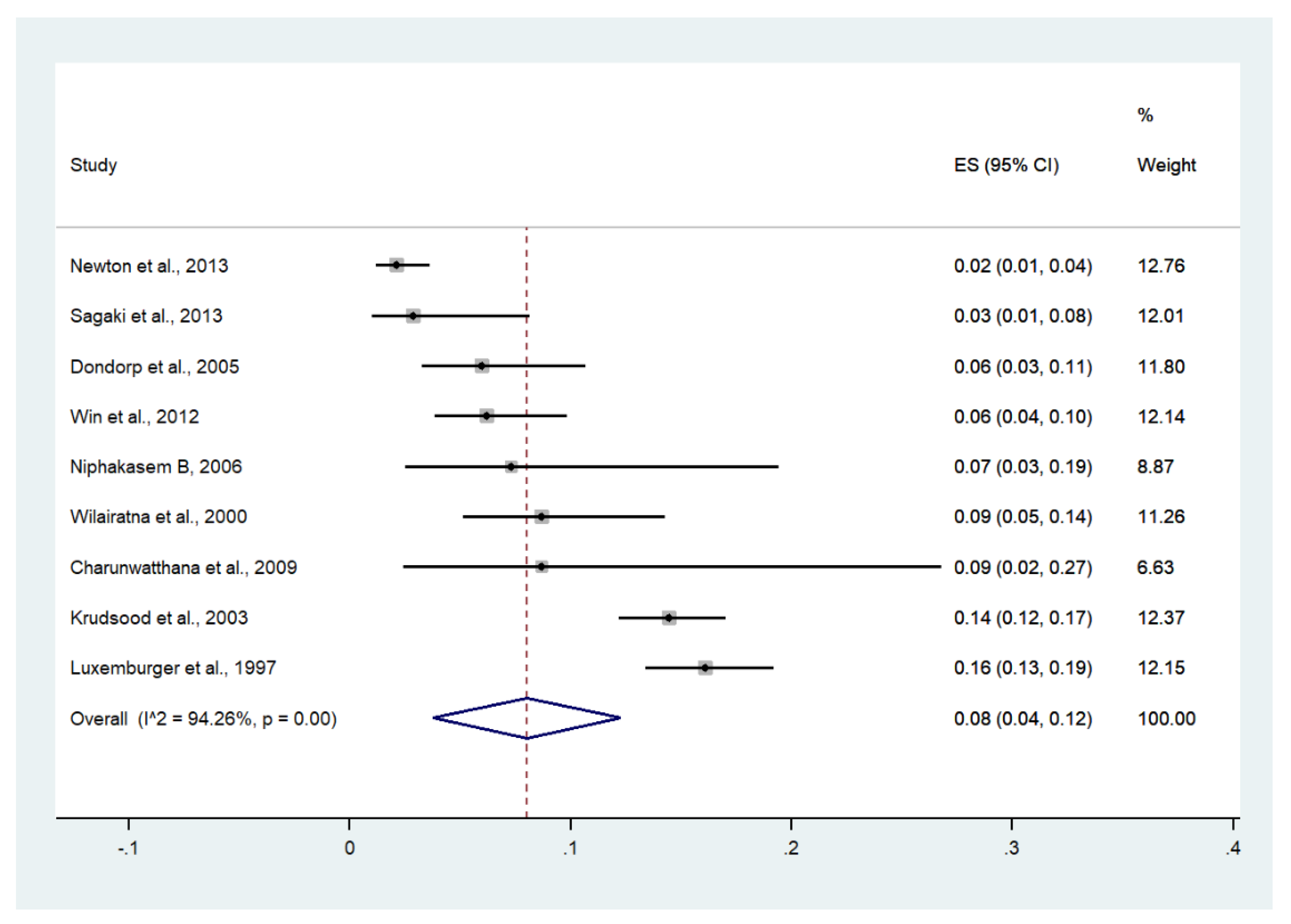
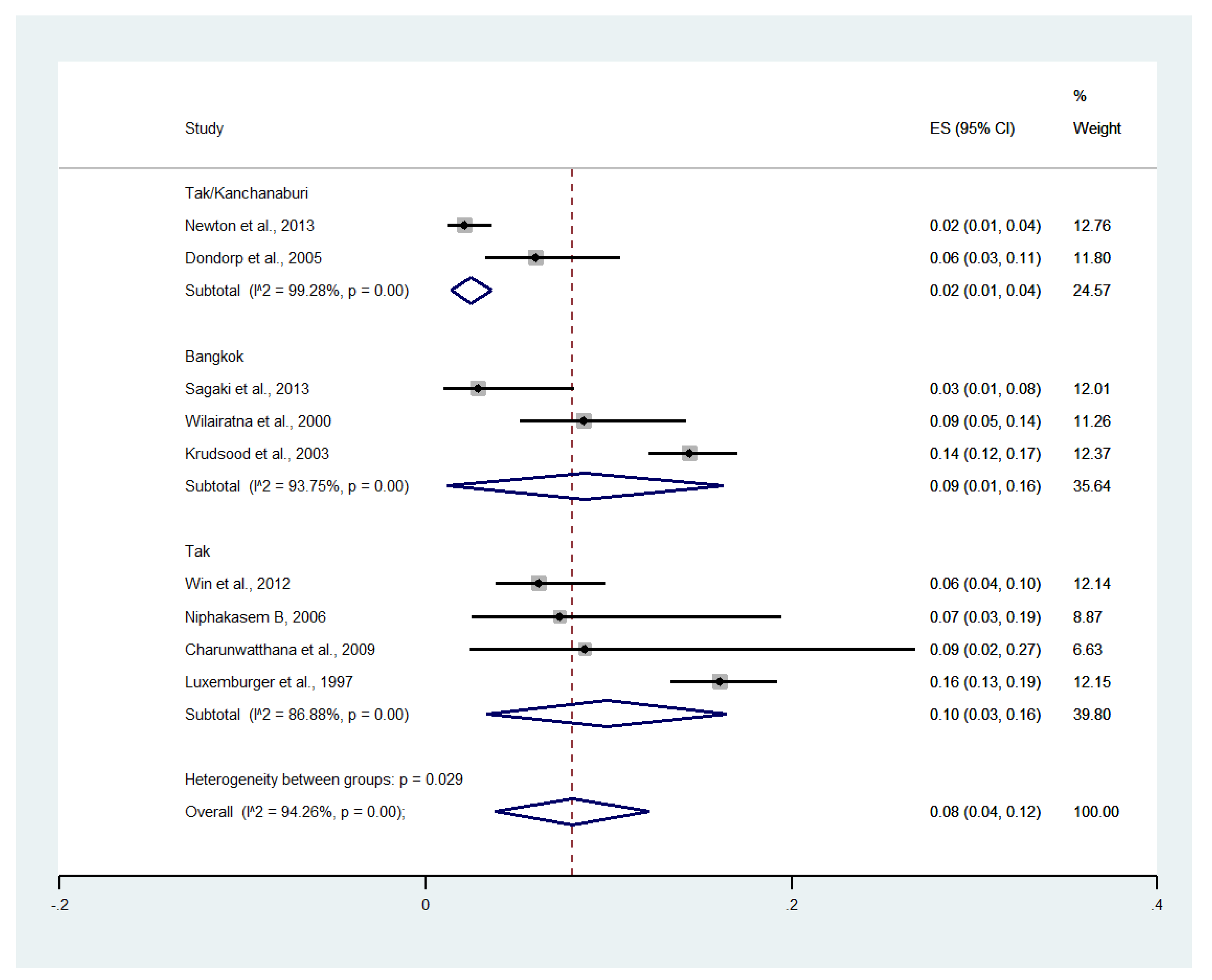
3.9. Severe Anemia
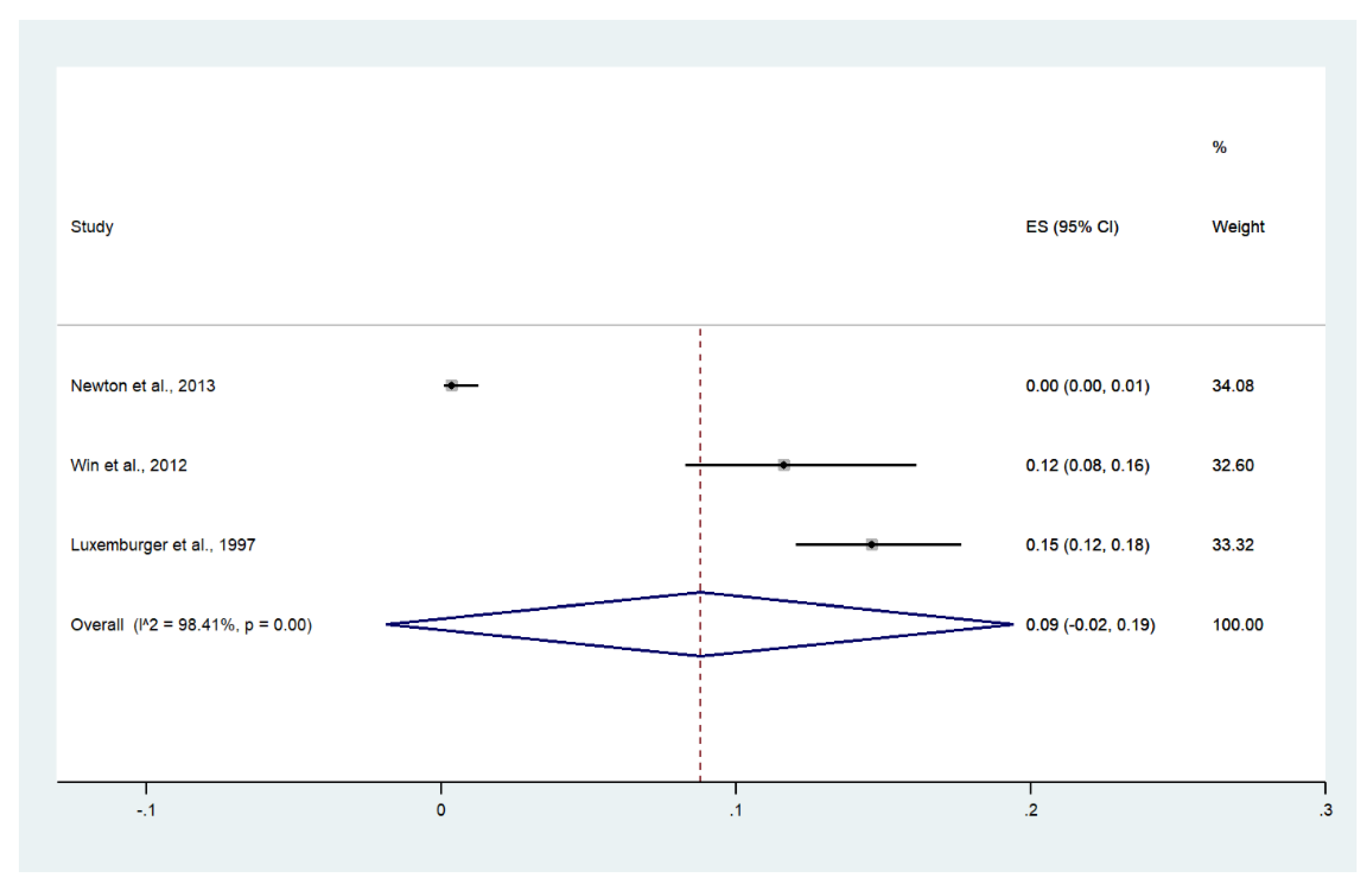
3.10. Convulsions
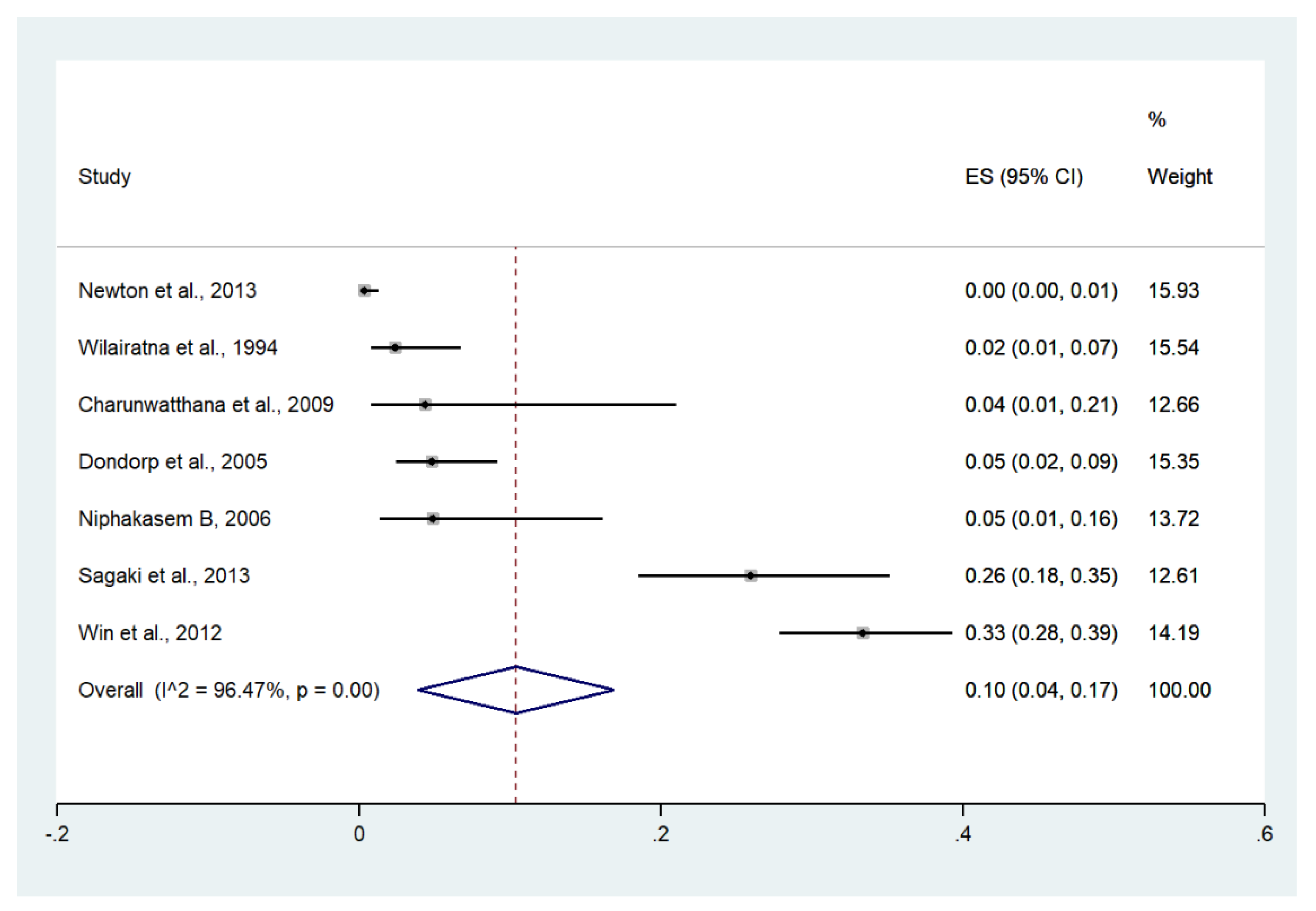
3.11. Shock
3.12. Pulmonary Edema/Acute Respiratory Distress Syndrome (ARDS)
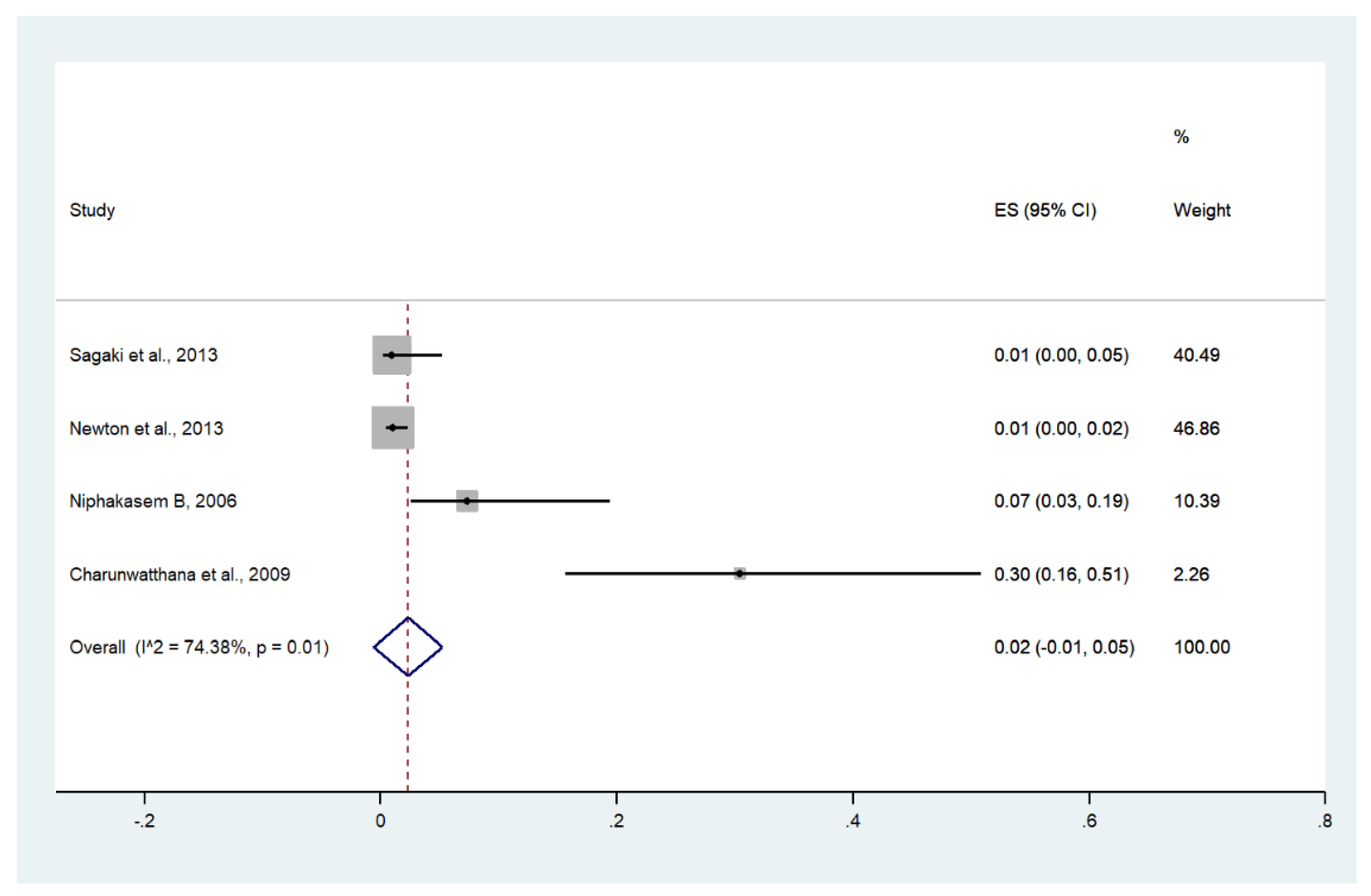
3.13. Bleeding/Disseminated Intravascular Coagulation (DIC)
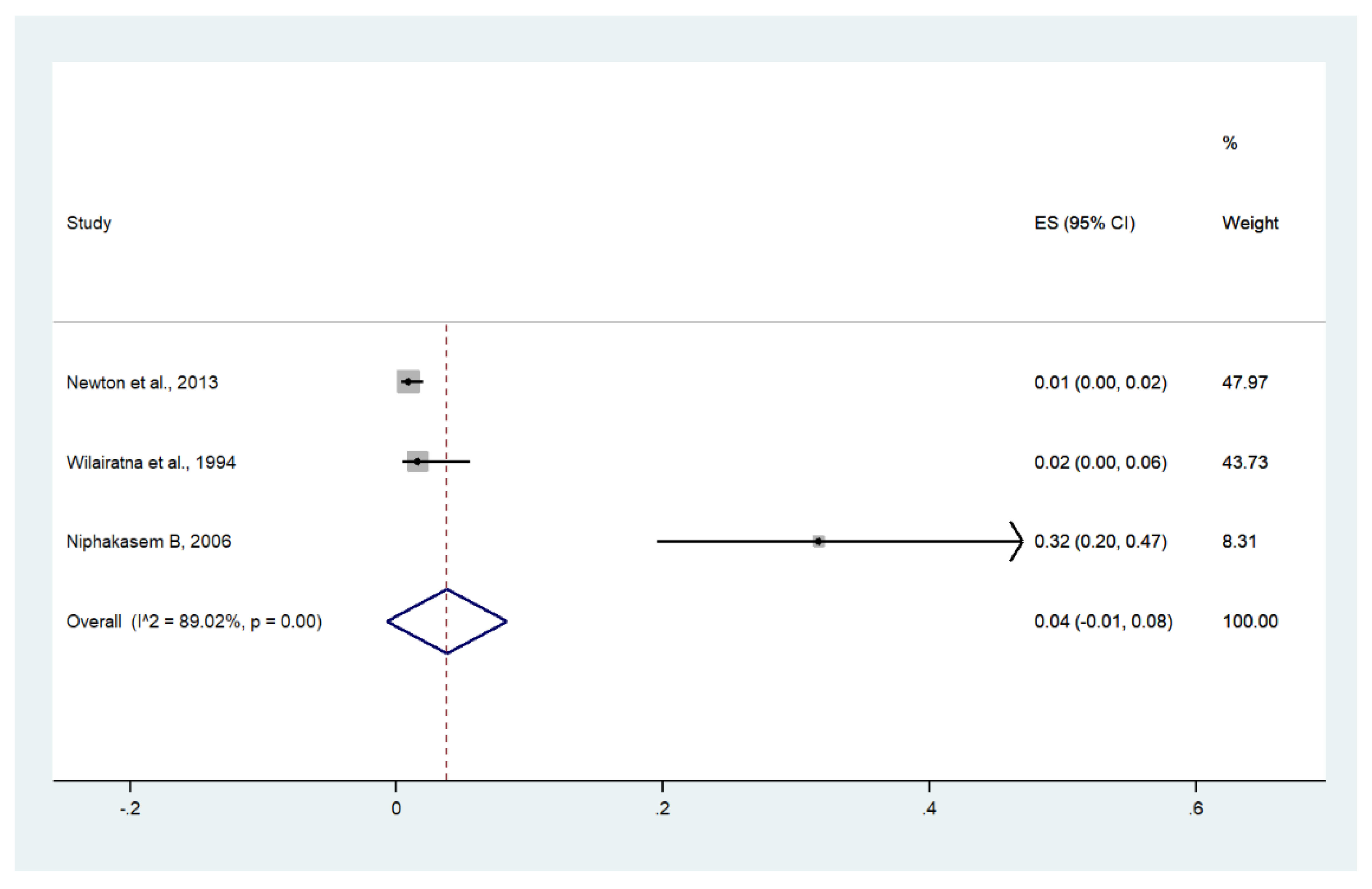
3.14. Hypoglycemia
3.15. Prostration
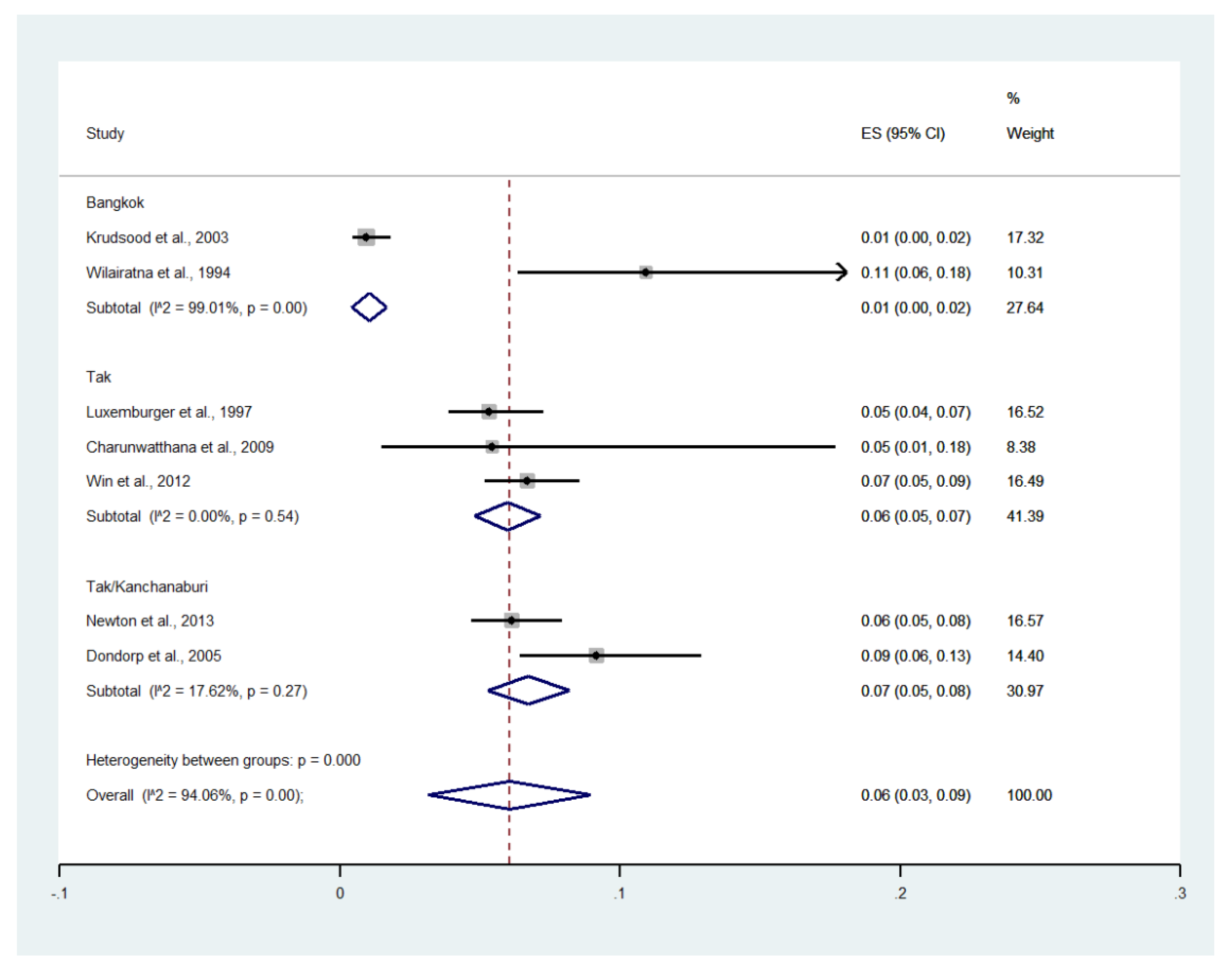
3.16. Prevalence and Proportion of Severe Malaria in Thailand
3.17. Deaths
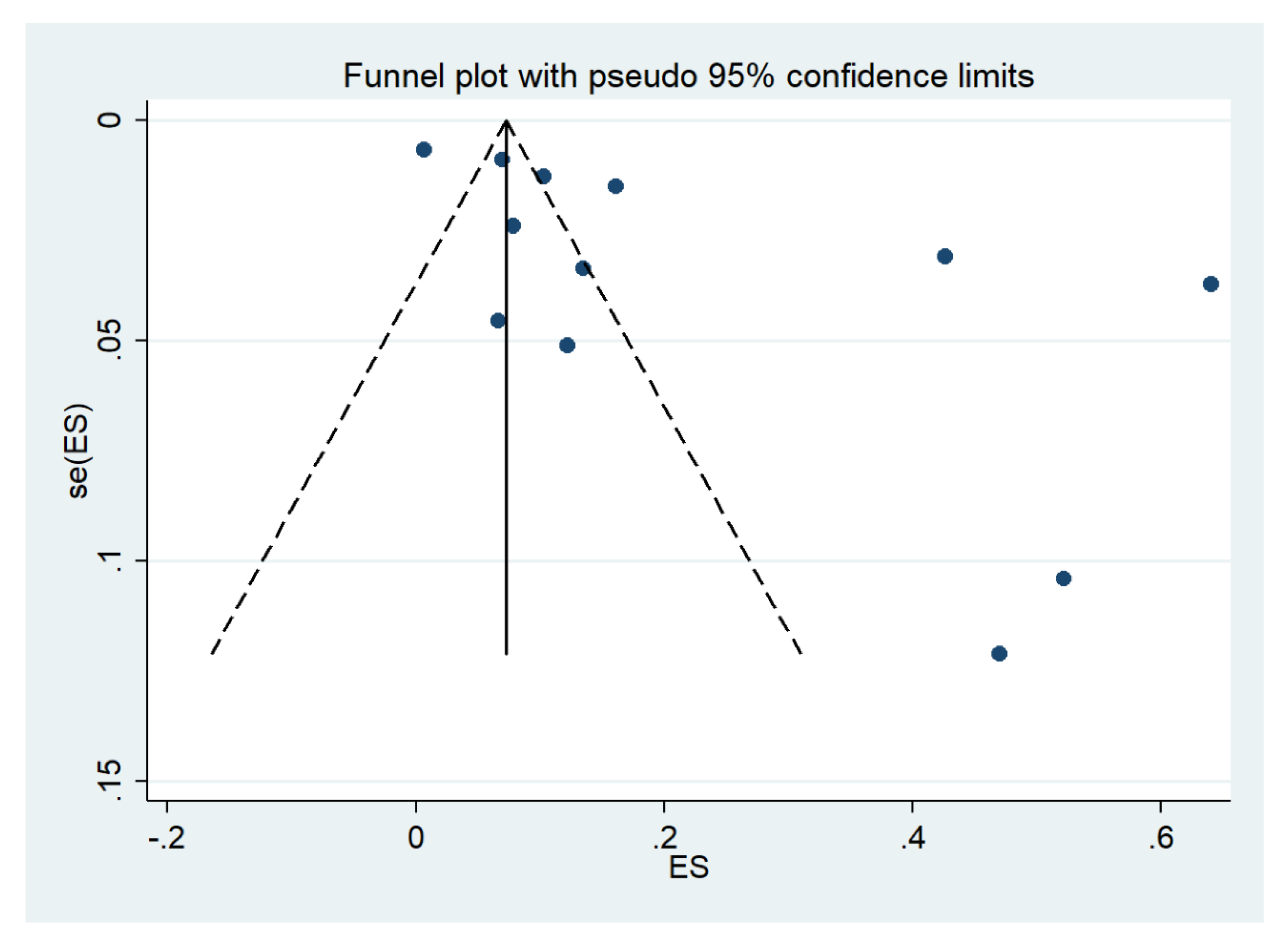
3.18. Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. World Malaria Report 2020. 2020. Available online: https://www.who.int/publications/i/item/9789240015791 (accessed on 21 November 2021).
- Mahittikorn, A.; Masangkay, F.R.; Kotepui, K.U.; Milanez, G.J.; Kotepui, M. Comparison of Plasmodium ovale curtisi and Plasmodium ovale wallikeri infections by a meta-analysis approach. Sci. Rep. 2021, 11, 6409. [Google Scholar] [CrossRef]
- Kotepui, M.; Kotepui, K.U.; Milanez, G.D.; Masangkay, F.R. Prevalence of severe Plasmodium knowlesi infection and risk factors related to severe complications compared with non-severe Plasmodium knowlesi and severe Plasmodium falciparum malaria: A systematic review and meta-analysis. Infect. Dis. Poverty 2020, 9, 106. [Google Scholar] [CrossRef]
- Kotepui, M.; Masangkay, F.R.; Kotepui, K.U.; Milanez, G.J. Preliminary review on the prevalence, proportion, geographical distribution, and characteristics of naturally acquired Plasmodium cynomolgi infection in mosquitoes, macaques, and humans: A systematic review and meta-analysis. BMC Infect. Dis. 2021, 21, 259. [Google Scholar] [CrossRef]
- WHO. WHO Guidelines for Malaria 2021. Available online: https://www.who.int/publications/i/item/guidelines-for-malaria (accessed on 21 November 2021).
- Kotepui, M.; Kotepui, K.U.; Milanez, G.D.; Masangkay, F.R. Global prevalence and mortality of severe Plasmodium malariae infection: A systematic review and meta-analysis. Malar. J. 2020, 19, 274. [Google Scholar] [CrossRef]
- Kotepui, M.; Kotepui, K.U.; Milanez, G.D.; Masangkay, F.R. Severity and mortality of severe Plasmodium ovale infection: A systematic review and meta-analysis. PLoS ONE 2020, 15, e0235014. [Google Scholar] [CrossRef] [PubMed]
- Kotepui, M.; Kotepui, K.U.; Milanez, G.J.; Masangkay, F.R. Prevalence and risk factors related to poor outcome of patients with severe Plasmodium vivax infection: A systematic review, meta-analysis, and analysis of case reports. BMC Infect. Dis. 2020, 20, 363. [Google Scholar] [CrossRef] [PubMed]
- Wilairatana, P.; Masangkay, F.R.; Kotepui, K.U.; Milanez, G.J.; Kotepui, M. Prevalence and characteristics of malaria among COVID-19 individuals: A systematic review, meta-analysis, and analysis of case reports. PLoS Negl. Trop. Dis. 2021, 15, e0009766. [Google Scholar] [CrossRef] [PubMed]
- Kotepui, M.; Kotepui, K.U.; De Jesus Milanez, G.; Masangkay, F.R. Plasmodium spp. mixed infection leading to severe malaria: A systematic review and meta-analysis. Sci. Rep. 2020, 10, 11068. [Google Scholar] [CrossRef]
- Kotepui, M.; Kotepui, K.U.; Milanez, G.D.; Masangkay, F.R. Prevalence of and risk factors for severe malaria caused by Plasmodium and dengue virus co-infection: A systematic review and meta-analysis. Infect. Dis. Poverty 2020, 9, 14. [Google Scholar] [CrossRef]
- Rosenthal, P.J. Artesunate for the treatment of severe falciparum malaria. N. Engl. J. Med. 2008, 358, 1829–1836. [Google Scholar] [CrossRef]
- Department of Communicable Disease Control. Thailand Malaria Elimination Program; Department of Communicable Disease Control: Bangkok, Thailand, 2021. [Google Scholar]
- Luxemburger, C.; Ricci, F.; Nosten, F.; Raimond, D.; Bathet, S.; White, N.J. The epidemiology of severe malaria in an area of low transmission in Thailand. Trans. R. Soc. Trop. Med. Hyg. 1997, 91, 256–262. [Google Scholar] [CrossRef]
- Lawpoolsri, S.; Sattabongkot, J.; Sirichaisinthop, J.; Cui, L.; Kiattibutr, K.; Rachaphaew, N.; Suk-Uam, K.; Khamsiriwatchara, A.; Kaewkungwal, J. Epidemiological profiles of recurrent malaria episodes in an endemic area along the Thailand-Myanmar border: A prospective cohort study. Malar. J. 2019, 18, 124. [Google Scholar] [CrossRef]
- Shimizu, S.; Chotirat, S.; Dokkulab, N.; Hongchad, I.; Khowsroy, K.; Kiattibutr, K.; Maneechai, N.; Manopwisedjaroen, K.; Petchvijit, P.; Phumchuea, K.; et al. Malaria cross-sectional surveys identified asymptomatic infections of Plasmodium falciparum, Plasmodium vivax and Plasmodium knowlesi in Surat Thani, a southern province of Thailand. Int. J. Infect. Dis. 2020, 96, 445–451. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Tufanaru, C.M.Z.; Aromataris, E.; Campbell, J.; Hopp, L.C. Chapter 3: Systematic reviews of effectiveness. In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; JBI: Adelaide, Australia, 2020; Available online: https://synthesismanual.jbi.global (accessed on 5 November 2021).
- Charunwatthana, P.; Faiz, M.A.; Ruangveerayut, R.; Maude, R.J.; Rahman, M.R.; Roberts, L.J.; Moore, K.; Yunus, E.B.; Hoque, M.G.; Hasan, M.U.; et al. N-acetylcysteine as adjunctive treatment in severe malaria: A randomized, double-blinded placebo-controlled clinical trial. Crit. Care Med. 2009, 37, 516–522. [Google Scholar] [CrossRef] [PubMed]
- Chuncharunee, S.; Jootar, S.; Leelasiri, A.; Archararit, N.; Prayoonwiwat, W.; Mongkonsritragoon, W.; Polvicha, P.; Srichaikul, T. Levels of serum tumor necrosis factor alpha in relation to clinical involvement and treatment among Thai adults with Plasmodium falciparum malaria. J. Med. Assoc. Thail. 1997, 80, S71–S75. [Google Scholar]
- Dondorp, A.M.; Desakorn, V.; Pongtavornpinyo, W.; Sahassananda, D.; Silamut, K.; Chotivanich, K.; Newton, P.N.; Pitisuttithum, P.; Smithyman, A.M.; White, N.J.; et al. Estimation of the total parasite biomass in acute falciparum malaria from plasma PfHRP2. PLoS Med. 2005, 2, 788–797. [Google Scholar] [CrossRef] [PubMed]
- Krudsood, S.; Wilairatana, P.; Vannaphan, S.; Treeprasertsuk, S.; Silachamroon, U.; Phomrattanaprapin, W.; Gourdeuk, V.R.; Brittenham, G.M.; Looareesuwan, S. Clinical experience with intravenous quinine, intramuscular artemether and intravenous artesunate for the treatment of severe malaria in Thailand. Southeast Asian J. Trop. Med. Public Health 2003, 34, 54–61. [Google Scholar]
- Looareesuwan, S.; Wilairatana, P.; Vanijanonta, S.; Viravan, C.; Andrial, M. Efficacy and tolerability of a sequential, artesunate suppository plus mefloquine, treatment of severe falciparum malaria. Ann. Trop. Med. Parasitol. 1995, 89, 469–475. [Google Scholar] [CrossRef]
- Newton, P.N.; Stepniewska, K.; Dondorp, A.; Silamut, K.; Chierakul, W.; Krishna, S.; Davis, T.M.; Suputtamongkol, Y.; Angus, B.; Pukrittayakamee, S.; et al. Prognostic indicators in adults hospitalized with falciparum malaria in Western Thailand. Malar. J. 2013, 12, 229. [Google Scholar] [CrossRef]
- Niphakasem, B. Severe falciparum malaria in children at Somdejt Prachaotaksin Maharaj Hospital. J. Med. Assoc. Thail. 2006, 89, 2091–2096. [Google Scholar]
- Sagaki, P.; Thanachartwet, V.; Desakorn, V.; Sahassananda, D.; Chamnanchanunt, S.; Chierakul, W.; Pitisuttithum, P.; Ruangkanchanasetr, P. Clinical factors for severity of Plasmodium falciparum malaria in hospitalized adults in Thailand. PLoS ONE 2013, 8, e71503. [Google Scholar] [CrossRef]
- Wilairatna, P.; Krudsood, S.; Silachamroon, U.; Singhasivanon, P.; Vannaphan, S.; Faithong, S.; Klabprasit, M.; Bangchang, S.N.; Olliaro, P.; Looareesuwan, S. Clinical trial of sequential treatments of moderately severe and severe malaria with dihydroartemisinin suppository followed by mefloquine in Thailand. Am. J. Trop. Med. Hyg. 2000, 63, 290–294. [Google Scholar] [CrossRef][Green Version]
- Win, K.; Thanachartwet, V.; Wattanagoon, Y.; Jerraksuwan, S.; Ruangweerayut, R.; Desakorn, V. Factors associated with acute renal failure in adults with severe falciparum malaria. Southeast Asian J. Trop. Med. Public Health 2012, 43, 1071–1079. [Google Scholar]
- Wilairatna, P.; Looareesuwan, S.; Charoenlarp, P. Liver profile changes and complications in jaundiced patients with falciparum malaria. Trop. Med. Parasitol. 1994, 45, 298–302. [Google Scholar]
- Bureau of Vector Borne Diseases. The Digital Surveillance System for Thailand Malaria Elimination; MOPH: Bangkok, Thailand, 2020. [Google Scholar]
- Lertpiriyasuwat, C.; Sudathip, P.; Kitchakarn, S.; Areechokchai, D.; Naowarat, S.; Shah, J.A.; Sintasath, D.; Pinyajeerapat, N.; Young, F.; Thimasarn, K.; et al. Implementation and success factors from Thailand’s 1-3-7 surveillance strategy for malaria elimination. Malar. J. 2021, 20, 201. [Google Scholar] [CrossRef]
- The Hospital for Tropical Diseases. Available online: https://www.tm.mahidol.ac.th/hospital/hospital-aboutus-en.php (accessed on 5 November 2021).
- Tangpukdee, N.; Krudsood, S.; Wilairatana, P. Schizontemia as an indicator of severe malaria. Southeast Asian J. Trop. Med. Public Health 2013, 44, 740–743. [Google Scholar]
- Tangpukdee, N.; Krudsood, S.; Thanachartwet, V.; Duangdee, C.; Paksala, S.; Chonsawat, P.; Srivilairit, S.; Looareesuwan, S.; Wilairatana, P. Predictive score of uncomplicated falciparum malaria patients turning to severe malaria. Korean J. Parasitol. 2007, 45, 273–282. [Google Scholar] [CrossRef][Green Version]
- Mohanty, S.; Mishra, S.K.; Pati, S.S.; Pattnaik, J.; Das, B.S. Complications and mortality patterns due to Plasmodium falciparum malaria in hospitalized adults and children, Rourkela, Orissa, India. Trans. R. Soc. Trop. Med. Hyg. 2003, 97, 69–70. [Google Scholar] [CrossRef]
- Kochar, D.K.; Kochar, S.K.; Agrawal, R.P.; Sabir, M.; Nayak, K.C.; Agrawal, T.D.; Purohit, V.P.; Gupta, R.P. The changing spectrum of severe falciparum malaria: A clinical study from Bikaner (Northwest India). J. Vector Borne Dis. 2006, 43, 104–108. [Google Scholar]
- Patil, V. Complicated falciparum malaria in Western Maharashtra. Trop. Parasitol. 2012, 2, 49–54. [Google Scholar] [CrossRef]
- Chung, S.J.; Low, J.G.; Wijaya, L. Malaria in a tertiary hospital in Singapore--clinical presentation, treatment and outcome: An eleven year retrospective review. Travel Med. Infect. Dis. 2014, 12, 738–744. [Google Scholar] [CrossRef]
- Barber, B.E.; William, T.; Grigg, M.J.; Menon, J.; Auburn, S.; Marfurt, J.; Anstey, N.M.; Yeo, T.W. A prospective comparative study of knowlesi, falciparum, and vivax malaria in Sabah, Malaysia: High proportion with severe disease from Plasmodium knowlesi and Plasmodium vivax but no mortality with early referral and artesunate therapy. Clin. Infect. Dis. 2013, 56, 383–397. [Google Scholar] [CrossRef]
- Lon, C.; Timmermans, A.; Buathong, N.; Nou, S.; Se, Y.; Sitthy, N.; Chann, S.; Kraesub, S.; Wongstitwilairoong, T.; Walsh, D.S.; et al. Severe malaria in Battambang Referral Hospital, an area of multidrug resistance in Western-Cambodia: A retrospective analysis of cases from 2006–2009. Malar. J. 2013, 12, 217. [Google Scholar] [CrossRef]
- Nyein, P.P.; Aung, N.M.; Kyi, T.T.; Htet, Z.W.; Anstey, N.M.; Kyi, M.M.; Hanson, J. High frequency of clinically significant bacteremia in adults hospitalized with falciparum malaria. Open Forum Infect. Dis. 2016, 3, ofw028. [Google Scholar] [CrossRef]
- Thien, H.V.; Chien, V.T.; Anh, T.K. Severe malaria in a provincial hospital in Vietnam. Lancet 1990, 336, 1316. [Google Scholar]
- Ha, V.; Nguyen, N.H.; Tran, T.B.; Bui, M.C.; Nguyen, H.P.; Tran, T.H.; Phan, T.Q.; Arnold, K.; Tran, T.H. Severe and complicated malaria treated with artemisinin, artesunate or artemether in Viet Nam. Trans. R. Soc. Trop. Med. Hyg. 1997, 91, 465–467. [Google Scholar] [CrossRef]
- Changpradub, D.; Mungthin, M. Severe vivax malaria: A case report and a literature review. J. Med. Assoc. Thail. 2014, 97 (Suppl. 2), S243–S246. [Google Scholar]
- Ketema, T.; Bacha, K. Plasmodium vivax associated severe malaria complications among children in some malaria endemic areas of Ethiopia. BMC Public Health 2013, 13, 637. [Google Scholar] [CrossRef]
- Geleta, G.; Ketema, T. Severe malaria associated with Plasmodium falciparum and Plasmodium vivax among children in Pawe Hospital, Northwest Ethiopia. Malar. Res. Treat. 2016, 2016, 1240962. [Google Scholar] [CrossRef]
- Rizvi, I.; Tripathi, D.K.; Chughtai, A.M.; Beg, M.; Zaman, S.; Zaidi, N. Complications associated with Plasmodium vivax malaria: A retrospective study from a tertiary care hospital based in Western Uttar Pradesh, India. Ann. Afr. Med. 2013, 12, 155–159. [Google Scholar] [CrossRef]
- Nakaviroj, S.; Kobasa, T.; Teeranaipong, P.; Putaporntip, C.; Jongwutiwes, S. An autochthonous case of severe Plasmodium knowlesi malaria in Thailand. Am. J. Trop. Med. Hyg. 2015, 92, 569–572. [Google Scholar] [CrossRef]





















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year Conducted | Study Sites | Province | Study Design | N Participants | Age Group | % Male | Died | Prostration | Impaired Con/Coma | Convulsion | Severe Anemia | Jaundice | Renal Impairment | Shock/Hypotension | Hyperparasitemia | Acidosis | Pulmonary edema/ARDS | DIC/Bleeding | Hypoglycemia | Total Signs of Severity | %Cutoff Parasitemia |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Charunwatthana et al., 2009 | 2003–2005 | Mae Sot Hospital | Tak | RCT | 23 | Adults patients | NS | 2 | NS | 12 | NS | 2 | 6 | 2 | 1 | 7 | 3 | 4 | NS | NS | 37 | >10% |
| Chuncharunee et al., 1997 | 1992–1994 | Ramathibodi Hospital, Pramongkutklao Hospital | Bangkok | Prospective observational study | 17 | Adults patients | 100 | NS | NS | 8 | NS | NS | NS | 10 | NS | 6 | NS | 6 | 1 | NS | 31 | >10% |
| Dondorp et al., 2005 | NS | Sangklaburi Hospital, Mae Sot Hospital | Tak/ Kanchanaburi | Prospective observational study | 167 | Adults patients | NS | 28 | NS | 107 | NS | 10 | 87 | 22 | 8 | 72 | NS | NS | NS | NS | 306 | >10% |
| Krudsood et al., 2003 | 1993–1996 | Hospital for Tropical Diseases | Bangkok | Clinical trials | 803 | Adults patients | NS | 8 | NS | 56 | NS | 116 | 340 | 26 | NS | 332 | NS | NS | NS | NS | 870 | >2% |
| Looareesuwan et al., 1995 | 1994 | Hospital for Tropical Diseases | Bangkok | Clinical trials | 30 | Adults patients | 76.7 | NS | NS | 2 | NS | NS | 6 | 1 | NS | 24 | NS | NS | NS | NS | 33 | >4% |
| Luxemburger et al., 1997 | 1994 | Shoklo hospital | Tak | Prospective observational study | 609 | Children and adults | 56 | 37 | NS | 98 | 89 | 98 | NS | NS | NS | 409 | NS | NS | NS | NS | 694 | >4% |
| Newton et al., 2013 | 1986–2002 | Hospitals in Kanchanaburi (1986–1993), Hospitals in Sangklaburi (1994–1995), Hospitals in Mae Sot (1995–2002) | Tak/ Kanchanaburi | Retrospective observational study | 571 | Adults patients | 51 | NS | 59 | 2 | 12 | 341 | 57 | 2 | 283 | 63 | 8 | 3 | 5 | 835 | >4% | |
| Niphakasem B, 2006 | 2003–2006 | Somdejt Prachaotaksin Maharaj Hospital | Bangkok | Retrospective observational study | 41 | Children | NS | 24 | 5 | 1 | 3 | NS | 2 | 2 | 5 | 3 | 2 | NS | NS | 23 | >4% | |
| Sagaki et al., 2013 | 2006–2012 | Hospital for Tropical Diseases | Bangkok | Retrospective case–control study | 104 | Adults patients | NS | NS | 14 | NS | 3 | 67 | 20 | 27 | 44 | 17 | 21 | 6 | 2 | 221 | >2% | |
| Wilairatna et al., 1994 | 1991 | Hospital for Tropical Diseases | Bangkok | Retrospective observational study | 127 | Children and adults | 12 | NS | 10 | NS | NS | 124 | 12 | 3 | 83 | NS | 2 | NS | NS | 110 | >4% | |
| Wilairatna et al., 2000 | 1999 | Hospital for Tropical Diseases | Bangkok | Clinical trials | 150 | Children and adults | 66.7 | NS | NS | 1 | NS | 13 | 103 | 3 | NS | 70 | NS | NS | NS | NS | 190 | >2% |
| Win et al., 2012 | 2004–2008 | Mae Sot Hospital | Tak | Retrospective observational study | 258 | Adults patients | 73.6 | 55 | 178 | 110 | 30 | 16 | 139 | 115 | 86 | NS | 109 | 23 | 7 | 13 | 826 | NS |
| Signs of Severity * | Estimated Prevalence (%) ** | 95% CI (%) | I2 | Number of Patients in Each Sign of Severity | Number of Patients with Severe Malaria | Number of Studies for Estimation |
|---|---|---|---|---|---|---|
| Jaundice | 54 | 36–72 | 99.02 | 1213 | 2233 | 9 |
| Hyperparasitemia | 47 | 38–56 | 95.07 | 1335 | 2642 | 11 |
| >2% | 42 | 39–45 | 0 | 446 | 1057 | 3 |
| >4% | 55 | 39–71 | 96.96 | 804 | 1378 | 5 |
| >10% | 41 | 34–48 | 0 | 85 | 207 | 3 |
| Impaired consciousness/coma | 21 | 14–28 | 97.96 | 482 | 2900 | 12 |
| Acidosis | 18 | 5–31 | 95.62 | 195 | 997 | 5 |
| Renal impairment | 13 | 8–19 | 95.81 | 270 | 2291 | 11 |
| Shock | 10 | 4–17 | 96.47 | 129 | 1291 | 7 |
| Convulsions | 9 | 2–19 | 98.41 | 121 | 1479 | 3 |
| Severe anemia | 8 | 4–12 | 94.26 | 273 | 2726 | 9 |
| Pulmonary edema/ARDS | 8 | 4–12 | 88.15 | 66 | 1141 | 7 |
| Hypoglycemia | 4 | 1–8 | 89.02 | 20 | 933 | 3 |
| Bleeding/DIC | 2 | 1–5 | 74.38 | 17 | 950 | 4 |
| Signs of Severity * | Estimated Proportion (%) ** | 95% CI (%) | I2 | Number of Each Sign of Severity | Total Number of Signs of Severity for Estimation | Number of Studies for Estimation |
|---|---|---|---|---|---|---|
| Hyperparasitemia | 33 | 25–42 | 97.29 | 1335 | 3498 | 11 |
| >2% | 32 | 20–44 | 94.20 | 446 | 1281 | 3 |
| >4% | 42 | 26–58 | 97.72 | 804 | 1843 | 5 |
| >10% | 23 | 18–27 | 0 | 85 | 374 | 3 |
| Jaundice | 33 | 24–43 | 97.07 | 1213 | 3552 | 9 |
| Impaired consciousness/coma | 12 | 8–16 | 96.55 | 482 | 4324 | 12 |
| Acidosis | 9 | 6–12 | 75.27 | 195 | 1966 | 5 |
| Renal impairment | 7 | 4–9 | 90.32 | 270 | 3630 | 11 |
| Severe anemia | 6 | 3–9 | 95.57 | 273 | 4026 | 9 |
| Convulsions | 5 | 0–11 | 98.32 | 121 | 2355 | 3 |
| Shock | 5 | 2–8 | 95.21 | 129 | 2506 | 7 |
| Pulmonary edema/ARDS | 3 | 1–5 | 83.21 | 66 | 1141 | 7 |
| Bleeding/DIC | 1 | 0–2 | 52.70 | 17 | 1913 | 4 |
| Hypoglycemia | 1 | 0–2 | 45.60 | 20 | 1882 | 3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mala, W.; Wilairatana, P.; Samerjai, C.; Masangkay, F.R.; Kotepui, K.U.; Kotepui, M. Prevalence of Signs of Severity Identified in the Thai Population with Malaria: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 1196. https://doi.org/10.3390/ijerph19031196
Mala W, Wilairatana P, Samerjai C, Masangkay FR, Kotepui KU, Kotepui M. Prevalence of Signs of Severity Identified in the Thai Population with Malaria: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2022; 19(3):1196. https://doi.org/10.3390/ijerph19031196
Chicago/Turabian StyleMala, Wanida, Polrat Wilairatana, Chutharat Samerjai, Frederick Ramirez Masangkay, Kwuntida Uthaisar Kotepui, and Manas Kotepui. 2022. "Prevalence of Signs of Severity Identified in the Thai Population with Malaria: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 19, no. 3: 1196. https://doi.org/10.3390/ijerph19031196
APA StyleMala, W., Wilairatana, P., Samerjai, C., Masangkay, F. R., Kotepui, K. U., & Kotepui, M. (2022). Prevalence of Signs of Severity Identified in the Thai Population with Malaria: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 19(3), 1196. https://doi.org/10.3390/ijerph19031196