1. Introduction
Cardiac pacemakers (PMs) are frequently implanted. In Norway in 2019, 699 new PMs per million inhabitants were implanted and approximately 28000 PM patients were followed up for their devices [
1]. The majority of the PM recipients was aged > 60 years at the time of implantation, with 50% of recipients aged 61–80 years and approximately 40% of recipients aged 81 years or older [
1]. A total of 88% of recipients received their PM due to syncope/dizziness/bradycardia or cardiac arrest [
1].
Existing data indicate that adult patients with implantable cardiac devices, such as PM and implantable cardioverter-defibrillator, frequently report on symptoms of depression and anxiety [
2,
3]. For example, the mean baseline scores on the depression and anxiety subscales of the Hospital Anxiety and Depression Scale in a Chinese intervention study indicate that self-reported symptom levels of depression and anxiety among PM recipients are well above those reported in community-based samples [
4,
5].
Posttraumatic stress disorder (PTSD) is a psychiatric disorder with onset after a stressful life event and characterized by a set of specific symptoms, such as persistent remembering of the stressful life event (by intrusive flashbacks, vivid memories, or recurring dreams), avoidance of stimuli that can reactivate the memories, and hyperarousal [
6]. PTSD is often accompanied by different anxiety symptoms [
6] and is therefore often regarded as a form of anxiety disorder. However, PTSD necessitates a somewhat different therapeutic approach compared to other anxiety disorders and it is therefore important to diagnose PTSD specifically. While existing data indicate that a substantial portion of patients with implantable cardioverter-defibrillator report on symptoms of posttraumatic stress [
7], to the best of our knowledge there is a lack of data on the occurrence of such symptomatology among PM patients. As a substantial proportion of PMs are implanted acutely in the aftermath of situations potentially perceived as life-threatening by the recipient (such as after a syncope or presyncope), and as the implantation of and the accommodation to a cardiac device further might be perceived as stressful life events, symptoms of posttraumatic stress have to be expected among PM patients as well.
Symptoms of depression, anxiety and posttraumatic stress/PTSD are not only associated with impaired quality of life, but these symptoms might also be associated with increased morbidity and mortality [
8,
9].
In order to tailor specific psychiatric/psychologic therapeutic interventions for PM patients, we need to increase our knowledge of the pattern and prevalence of clinically significant psychiatric symptomatology, especially of symptoms of posttraumatic stress/PTSD. Such specific interventions, when proven effective, will have the potential to attenuate cardiac intervention-related impairment of quality of life and might also impact positively on morbidity and mortality.
In this pilot study we aimed to explore the prevalence of symptoms of depression, anxiety, and posttraumatic stress measured by self-report among PM patients, who received their PM due to syncope or presyncope. We aimed further to compare the PM group’s symptom levels to those reported by participants of three control groups: (i) a cardiac control group, (ii) a chronic disease control group with known elevated occurrence of psychiatric symptomatology, and (iii) a healthy control group.
2. Materials and Methods
2.1. Study Sample
This pilot study was conducted at Nordland Hospital Trust Bodø (Norway) and included four study groups: PM patients, who had received a PM due to syncope or presyncope (PM group), patients who had received a percutaneous coronary intervention (PCI), patients receiving dialysis due to end-stage renal disease, and blood donors. The latter three study groups representing a cardiac control group (PCI control group), a chronic disease control group with known elevated occurrence of psychiatric symptomatology [
10] (Dialysis control group), and a healthy control group (Healthy control group), respectively.
The study material was mailed to 52 eligible PM patients, 50 eligible PCI patients, and 50 eligible dialysis patients. Response rates were 73.1, 46.0, and 34.0%, respectively, resulting in the inclusion of 38 participants in the PM group, 23 participants in the PCI control group, and 17 participants in the Dialysis control group. Furthermore, 42 blood donors returned answered study material, constituting the Healthy control group. One additional individual returned the answered questionnaires, but this individual could not be included in the analyses due to missing data concerning study group.
2.1.1. Inclusion Criteria
Participants in the PM group had received a PM due to syncope (defined as temporary loss of consciousness and muscle tone with complete recovery) or presyncope (defined as an episode of near-fainting). Participants in the PCI control group had received an elective or acute PCI due to stable or unstable angina pectoris or myocardial infarction. Participants in the Dialysis control group were treated with haemodialysis or peritoneal dialysis due to end-stage renal disease. Time of the index intervention (i.e., implantation of PM, performance of PCI, and first dialysis, respectively) antedated inclusion with at least 6 months. We chose this strategy in order to include participants with persistent psychiatric symptomatology as opposed to including in addition participants with transient difficulties with psychological adjustment to the intervention and its consequences. Participants in the Healthy control group were blood donors aged 50 years or older. We applied this age criterion as the PM, PCI, and dialysis patients were expected to be older than the majority of the blood donors at our blood bank.
2.1.2. Exclusion Criteria
PM, PCI, and dialysis patients were not eligible for inclusion into the study if serious chronic somatic illness, cognitive impairment, and/or insufficient language skills (Norwegian) were documented in the electronic health record. In addition, we applied specific exclusion criteria regarding PM, PCI, and dialysis. Eligible PM and PCI patients had not received one of the two other interventions after the index intervention. By way of example, an eligible PM patient had not received a PCI after implantation of the PM nor had this patient started on dialysis after implantation of the PM. Eligible dialysis patients had not received a PM nor a PCI during the 6 months antedating inclusion.
For the participants of the Healthy control group no formal exclusion criteria were applied, as inclusion criteria for blood donors are strict.
2.2. Procedures
Eligible cardiac and dialysis patients were identified via electronic health records by a cardiologist (K.T.L.) and a nephrologist (R.I.H.), working at the Departments of Cardiology and Nephrology at Nordland Hospital Trust Bodø, respectively. The presence of inclusion and absence of exclusion criteria was evaluated at this stage, based on information from the electronic health record. Information about the study, the study questionnaires as well as a pre-paid return envelope were then sent to these eligible patients. Personnel at the blood bank approached eligible blood donors while they were at the blood bank, and handed out the study material in case of interest to participate in the study. A reminder was sent to all eligible PM, PCI, and dialysis patients to increase the response rate. Starting date for dispatch of study material was 16 March 2021 and the reminder was dispatched on 8 July 2021. The data base was closed on 27 September 2021.
Data was punched manually into the research data base, which was stored on a designated secure section of the server of Nordland Hospital Trust Bodø.
2.3. Measures
2.3.1. Self-Report of Symptoms of Depression, Anxiety, and Posttraumatic Stress
Symptoms of depression, anxiety, and posttraumatic stress were measured by means of validated self-report scales, namely the Patient Health Questionnaire—9 (PHQ-9; [
11]), the Generalized Anxiety Disorder—7 scale (GAD-7; [
12]), and the Impact of Event Scale—Revised (IES-R; [
13]).
The PHQ-9 is a 9-item self-report measure of depression severity [
11]. Its items are based on the diagnostic criteria of the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) [
11]. Each item is rated from 0 to 3. The total score ranges from 0 to 27 with higher scores indicating more depressive symptoms. For a total score of 10 or higher, a sensitivity of 88% and a specificity of 88% to diagnose major depressive disorder has been reported for a sample of 580 patients, recruited into a primary care study [
11]. A Cronbach’s α of 0.839 in the present sample indicates good internal consistency for the PHQ-9.
The GAD-7 is a 7-item self-report measure, developed to identify probable cases of generalized anxiety disorder and to assess symptom severity [
12]. The final version of the GAD-7 is developed based on 9 items reflecting the DSM-IV diagnostic criteria for generalized anxiety disorder and 4 items based on review of existing anxiety scales [
12]. Each item of the GAD-7 is rated from 0 to 3. The total score ranges from 0 to 21 with higher scores indicating more anxiety symptoms. The GAD-7 is correlated with two other self-report anxiety measures, namely the Beck Anxiety Inventory (r = 0.72) and the anxiety subscale of the Symptom Checklist—90 (r = 0.74) [
12]. The GAD-7 is increasingly used as a measure of anxiety in general [
14]. A total score of 8 has been proposed as threshold for identifying possible cases with anxiety disorder [
14]. A Cronbach’s α of 0.897 in the present sample indicates good internal consistency for the GAD-7.
The IES-R is a 22-item self-report measure of symptoms of posttraumatic stress/PTSD [
13]. Each item is rated from 0 to 4 with higher scores indicating more distress [
13]. The items parallel the DSM-IV diagnostic criteria for PTSD [
13]. Responses are reported as mean for 3 subscale scores (based on the respective single item ratings), namely the intrusion (8 items), the avoidance (8 items), and the hyperarousal (6 items) subscale [
13]. For a valid self-report of symptoms of posttraumatic stress/PTSD by means of the IES-R, the respondent needs to relate the responses to a specific stressful life event [
13]. Therefore, the stressful life event was explicitly stated on the questionnaire, namely the PM implantation (PM group), the PCI (PCI control group), and the first dialysis (Dialysis control group), respectively. The IES-R was not administrated to the Healthy control group. When evaluating the IES-R scores, the application of cut-offs is deemed inappropriate and this notion is discussed comprehensively elsewhere [
13]. A Cronbach’s α of 0.880, 0.877 and 0.848 in the present sample for the intrusion, avoidance, and hyperarousal subscales, respectively, indicate good internal consistency for the subscales of the IES-R.
2.3.2. Sociodemographic Variables
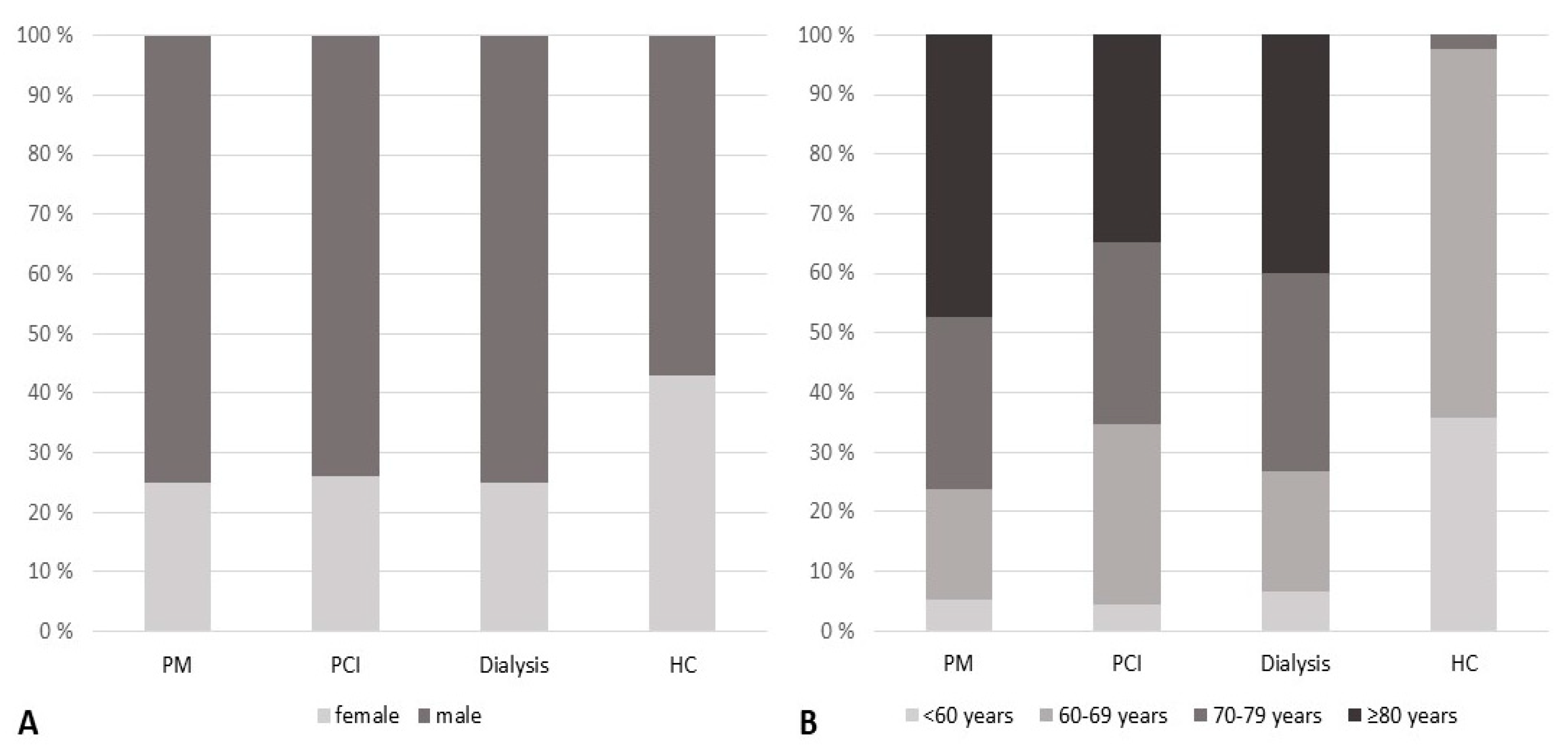
In this pilot study, only a limited number of sociodemographic variables was registered, namely gender, age categorized in 5-year intervals (i.e., <50, 50–54 years, etc.), study group (i.e., PM group, PCI control group, Dialysis control group, Healthy control group), and time since intervention categorized in 12-month intervals (i.e., 6 to <18 months, 18 to <30 months, etc.). For participants in the PM group, it was in addition registered whether they received their PM due to syncope or presyncope.
2.4. Statistical Analyses
For descriptive purposes, data are presented as frequencies and proportions or as means and standard deviations as appropriate. Symptoms of depression, anxiety, and posttraumatic stress were compared between study groups with the Kruskal–Wallis test (continuous variables) and when appropriate in addition with the Fisher exact test (i.e., PHQ-9 and GAD-7 total scores dichotomized at clinical cut-off; categorial variables). In case of significant group differences, we report results from posthoc analyses (pairwise comparisons) after Bonferroni correction. Level of significance was set to 5%. Statistical analyses were conducted with IBM SPSS Statistics software (IBM Corporation, Armonk, NY, USA) version 27.
4. Discussion
We aimed to extend the knowledge about occurrence of symptoms of depression, anxiety, and posttraumatic stress measured by self-report among PM patients, and compare these findings to those in a cardiac control group, a chronic disease control group with known elevated occurrence of psychiatric symptomatology, and a healthy control group.
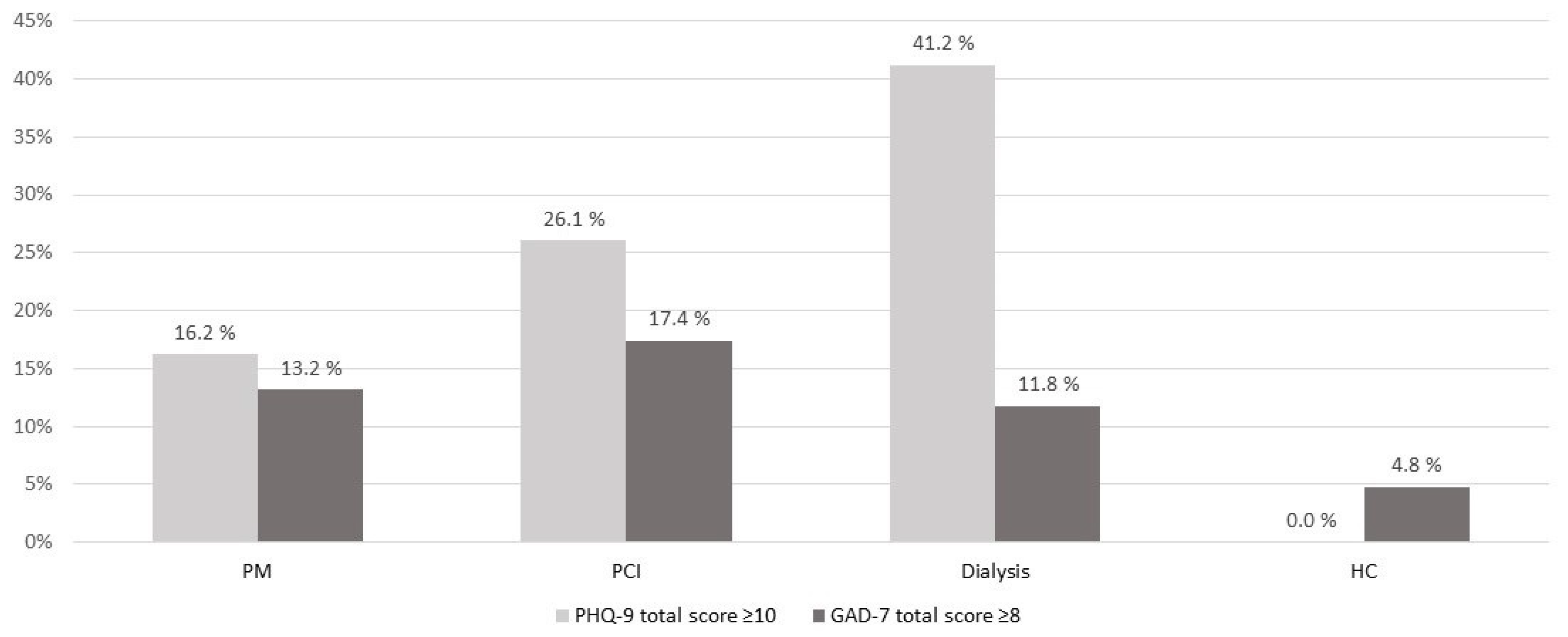
The study groups differed on the group level with regard to depressive symptoms, both when analysing data as continuous as well as dichotomous variable. Posthoc analyses indicated, that the proportion of participants with clinically significant depression (defined as above cut-off self-report) was higher among both the PM, PCI, and dialysis patients compared to the healthy control participants. Occurrence of clinically significant depression tended to be lower among PM patients (16.2%), than among PCI and dialysis patients, with the highest occurrence among dialysis patients (41.2%). A higher proportion of PM patients than healthy control participants with above cut-off self-report of depressive symptoms is in line with the results of a recently published cross-sectional study [
15]. Due to differences in such as assessment methods and applied cut-off as well as differences in sample characteristics, it is difficult to compare previously published prevalence rates of clinically significant depression among PM patients directly to our findings. However, the proportion of PM patients with clinically significant depression included in our study (16.2%) compares fairly well with the absolute figures reported for above cut-off self-report of depressive symptoms in two earlier reports [
16,
17]. The proportion of PM patients with clinically significant depression in our study also seems higher than the sum of the 12-month prevalence for major depressive disorder and dysthymia (5.3%) reported from a Norwegian epidemiological, diagnosis-based study conducted in a rural area [
18]. Relating these epidemiological data [
18] to our findings in the Healthy control group indicates that our healthy control participants might be positively selected. Our results concerning self-report of depressive symptoms among the cardiac control group and the chronic disease control group seem in concordance with published data. The proportion of PCI patients with clinically significant depression (26.1%), compares well with the prevalence rate of depression mentioned in a review on depression among patients with cardiac disease (primarily based on data of patients with coronary artery disease) [
19]. Our finding, indicating that 41.2% of the included dialysis patients were clinically depressed, is in line with what is reported in a review on depression among dialysis patients (i.e., 39.3% clinically depressed when depression was measured by self- or clinician-administered rating scales) [
20].
The study groups did not differ statistically significant with regard to anxiety symptoms, neither when conducting the analysis with continuous nor with dichotomous variable. However, the proportion of PM, PCI, and dialysis patients with clinically significant anxiety (defined as above cut-off self-report) tended to be higher than the proportion of healthy control participants with clinically significant anxiety (11.8 to 17.4 vs. 4.8%). The 12-month prevalence for the specific anxiety disorders which were assessed in the aforementioned Norwegian epidemiological diagnosis-based study ranged from 1.1 to 5.0% (GAD vs. both specific phobia and social phobia, respectively) [
18]. The 12-month prevalence for at least one anxiety disorder would be lower than the sum of the prevalence rates of the specific anxiety disorders (i.e., 13.9%) due to occurrence of comorbidity, but well above 5.0%. Contrasting these figures to our results indicates again that our healthy control participants might be positively selected. Even if a direct comparison is difficult, as outlined earlier, it seems as if above cut-off self-report of anxiety symptoms among included PM patients in our study (13.2%) is, in contrast to our expectations, somewhat lower than reported of others (i.e., 19.4 to 27.2%) [
15,
16,
17]. Factors such as sociodemographic differences of the study samples (i.e., gender and age distribution), time since intervention, and recruitment strategies might contribute to these inconsistencies of results. The 17.4% of PCI participants with above cut-off self-report of anxiety symptoms in our study seems consistent with the notion in a review on anxiety disorders and cardiovascular disease, stating that 20 to 30% of patients experience elevated levels of anxiety following an acute coronary syndrome and that in half of cases anxiety persists for up to one year after the event [
21]. Anxiety in dialysis patients seems less studied and reported prevalence rates vary greatly, ranging from 12 to 52% among haemodialysis patients [
22]. Prevalence rate of anxiety disorders in a Norwegian diagnosis-based study in dialysis patients was 17% [
23], compared to the 11.8% of dialysis patients with above cut-off self-report of anxiety symptoms in our study.
Symptom levels of posttraumatic stress did not differ statistically significant between PM, PCI, and dialysis patients in our study. However, it is noteworthy that the proportions of participants reporting on average at least ‘moderate’ distress on two of the three subscales of the IES-R were highest in the PM group. To the best of our knowledge, posttraumatic stress/PTSD has not been studied specifically in PM patients earlier. A 12% prevalence rate of PTSD secondary to acute coronary syndromes is mentioned in a review [
24], thus indicating that the level of self-report of posttraumatic stress among the included PCI patients in our study is lower. This inconsistency might partly be explained by the fact that our PCI control group included patients with both acute and elective PCI. Prevalence rate of PTSD related to haemodialysis was 10.4% in a cross-sectional study [
25]. This indicates that PTSD occurred more frequently in that study than among dialysis patients included in our study. This inconsistency can hardly be explained through differences in sociodemographic characteristics and assessment methods alone, and remains thus unexplained.
Limitations
Our pilot study has several limitations that need to be discussed. First, we included only participants in the PM group that had received their PM due to syncope or presyncope. Thus, our results are not necessarily generalizable to all PM patients. However, at least the age distribution of the participants in the PM group seems to resemble the Norwegian population of PM recipients [
1]. Second, the exclusion criteria differed slightly between the PM group, PCI control group, and the Dialysis control group. While PM and PCI patients were excluded if they had received one of the two other interventions after the index intervention (in order to be able to demonstrate the potential effect of the intervention in question), dialysis patients were only excluded if they had received a PM or a PCI during the 6 months antedating inclusion. This adaption was necessary to avoid selection bias in the Dialysis control group due to the higher occurrence of comorbidity in the dialysis population. This minor difference in exclusion criteria might have influenced on our results. Third, even though we excluded patients for whom cognitive impairment was documented in the electronic health record, we must expect that some of our included patients might have some degree of cognitive impairment (due to for example advanced age), which might have influenced on self-report and thus our results. Fourth, our participants were not diagnosed after a structured psychiatric interview of an experienced clinician (which is the gold standard), which makes it for example difficult to draw firm conclusions regarding the lower-than-expected occurrence of above cut-off self-report of anxiety symptoms among the PM patients in our study. Fifth, the response rates varied between the eligible PM, PCI, and dialysis patients, with a response rate as high as 73.1% in the PM group and as low as 34.0% in the Dialysis control group. Against the background that psychiatric symptomatology seems to occur most frequently among dialysis patients and that patients with psychiatric symptomatology might be less prone to participate in a study like ours, the occurrence of symptoms of depression, anxiety, and posttraumatic stress might be underestimated in our study, especially among the included dialysis patients. Sixth, as prevalence rates of depression and anxiety disorders in general are higher in females than in males [
18], it would have been interesting to re-analyse our data controlling for gender. However, we deemed our sample too little to conduct these analyses. In the same line, it would have been interesting to analyse the effect of age (especially with regard to self-report of depressive symptoms) and time since intervention on the occurrence of symptoms of depression, anxiety and posttraumatic stress.
5. Conclusions
At 6 months or more after the intervention, the included PM, PCI, and dialysis patients reported more frequently on depressive symptoms above clinical cut-off than the healthy control participants. Furthermore, the occurrence of above cut-off self-report of depressive symptoms in these patient groups seems to be higher than expected in the general population. Thus, even if clinically significant depression seems to occur more frequently among dialysis patients than among PM and PCI patients, it seems necessary to focus on identifying relevant patients in all three patient populations in clinical routine. Patients with depressive symptomatology of suspected clinical relevance should be referred to a mental health professional for adequate diagnostic evaluation and treatment, with the aim to increase quality of life and possibly contribute to alleviate depression’s negative impact on clinical outcomes. It is, as outlined above, difficult to draw firm conclusions of our findings regarding anxiety symptoms in the PM group. However, together with our finding that a non-negligible proportion of PM patients reported on symptoms of posttraumatic stress of anticipated clinical relevance, it seems advisable with further studies in the field. These studies should in a first step aim to establish stable estimates of prevalence of PTSD among PM patients, based on the diagnostic criteria of the latest (i.e., fifth) version of the Diagnostic and Statistical Manual of Mental Disorders, as well as of posttraumatic stress symptoms of insufficient severity to render a formal diagnosis (i.e., sub-diagnostic symptom level).






{kind=link}
{kind=link}