
The Effect of Pre-Operative Verbal Confirmation for Interventional Radiology Physicians on Their Use of Personal Dosimeters and Personal Protective Equipment

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Design
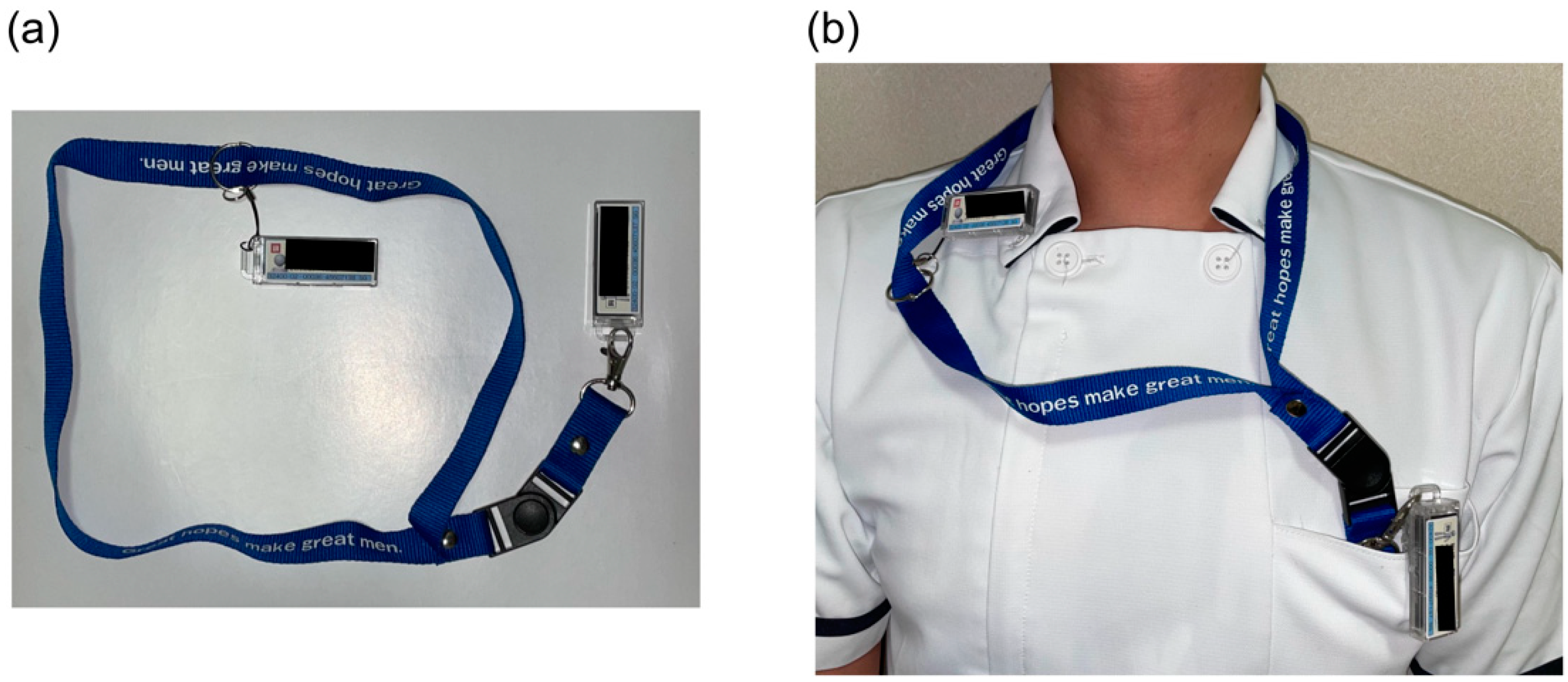
2.2. Survey of Personal Passive Dosimeters and PPE Use Rates
2.3. Survey of Personal Exposure Dose
2.4. Pre-Operative Briefing
2.5. Statistical Analyses
3. Results
3.1. Use Rate of Personal Passive Dosimeters and PPE in the Pre-Intervention Period
3.2. Intervention Effect of Pre-Operative Briefing
4. Discussion
- Improved use rate of personal passive dosimeters
- The personal passive dosimeter management method shifted from single-dosimeter to double-dosimeter.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- International Commission on Radiological Protection. ICRP Statement on Tissue Reactions and Early and Late Effects of Radiation in Normal Tissues and Organs—Threshold Doses for Tissue Reactions in a Radiation Protection Context; ICRP publication 118. Ann.; Elsevier Ltd.: Amsterdam, The Netherlands, 2012; Volume 41, pp. 1–322. [Google Scholar]
- International Commission on Radiological Protection. The 2007 Recommendations of the International Commission on Radiological Protection; ICRP publication 103. Ann.; Elsevier Ltd.: Amsterdam, The Netherlands, 2007; Volume 37, pp. 1–332. [Google Scholar]
- International Commission on Radiological Protection. Occupational Radiological Protection in Interventional Procedures; ICRP publication 139. Ann.; SAGE Publications Ltd.: Thousand Oaks, CA, USA, 2018; Volume 47, pp. 1–118. [Google Scholar]
- International Commission on Radiological Protection. General Principles for the Radiation Protection of Workers; ICRP publication 75. Ann.; Elsevier Ltd.: Amsterdam, The Netherlands, 1997; Volume 27, pp. 1–61. [Google Scholar]
- Mori, K.; Takebayashi, T. The Introduction of an Occupational Health Management System for Solving Issues in Occupational Health Activities in Japan. Ind. Health 2002, 40, 167–174. [Google Scholar] [CrossRef] [PubMed]
- Nagamoto, K.; Moritake, T.; Nakagami, K.; Morota, K.; Matsuzaki, S.; Nihei, S.-I.; Kamochi, M.; Kunugita, N. Occupational radiation dose to the lens of the eye of medical staff who assist in diagnostic CT scans. Heliyon 2021, 7, e06063. [Google Scholar] [CrossRef] [PubMed]
- Kunugita, N. Survey on Workers Who Can Still Be Subject to High Exposure Dose to the Lens of the Eye in Spite of Adequate Radiation Protection Measures. Available online: https://www.mhlw.go.jp/content/11201000/000519683.pdf (accessed on 14 February 2022). (In Japanese).
- International Commission on Radiological Protection. Education and Training in Radiological Protection for Diagnostic and Interventional Procedures; ICRP publication 113. Ann.; Elsevier Ltd.: Amsterdam, The Netherlands, 2010; Volume 39, pp. 1–68. [Google Scholar]
- International Commission on Radiological Protection. Radiological Protection in Fluoroscopically Guided Procedures Performed Outside the Imaging Department; ICRP publication 117. Ann.; Elsevier Ltd.: Amsterdam, The Netherlands, 2012; Volume 40, pp. 1–102. [Google Scholar]
- Niklason, L.T.; Marx, M.V.; Chan, H.P. Interventional radiologists: Occupational radiation doses and risks. Radiology 1993, 187, 729–733. [Google Scholar] [CrossRef] [PubMed]
- Tsapaki, V.; Ahmed, N.A.; Alsuwaidi, J.S.; Beganovic, A.; Benider, A.; Benomrane, L.; Borisova, R.; Economides, S.; El-Nachef, L.; Faj, D.; et al. Radiation Exposure to Patients During Interventional Procedures in 20 Countries: Initial IAEA Project Results. Am. J. Roentgenol. 2009, 193, 559–569. [Google Scholar] [CrossRef] [PubMed]
- Vano, E.; Kleiman, N.J.; Duran, A.; Romano-Miller, M.; Rehani, M.M. Radiation-associated lens opacities in catheterization personnel: Results of a survey and direct assessments. J. Vasc. Interv. Radiol. 2013, 24, 197–204. [Google Scholar] [CrossRef] [PubMed]
- International Atomic Energy Agency. The Information System on Occupational Exposure in Medicine, Industry and Research (ISEMIR): Interventional Cardiology; INTERNATIONAL ATOMIC ENERGY AGENCY: Vienna, Austria, 2014. [Google Scholar]
- Brun, A.; Mor, R.A.; Bourrelly, M.; Dalivoust, G.; Gazazian, G.; Boufercha, R.; Lehucher-Michel, M.P.; Sari-Minodier, I. Radiation protection for surgeons and anesthetists: Practices and knowledge before and after training. J. Radiol. Prot. 2018, 38, 175–188. [Google Scholar] [CrossRef]
- Altintas, E.; BahÁeci, T.; Batur, A.; Kaynar, M.; KiliÁ, O.; Akand, M.; Goktas, S.; Gul, M. A survey analysis of knowledge levels of urologists about radiation safety and fluoroscopy use. Int. J. Clin. Pract. 2020, 75, e13862. [Google Scholar] [CrossRef]
- Efstathopoulos, E.P.; Pantos, I.; Andreou, M.; Gkatzis, A.; Carinou, E.; Koukorava, C.; Kelekis, N.L.; Brountzos, E. Occupational radiation doses to the extremities and the eyes in interventional radiology and cardiology procedures. Br. J. Radiol. 2011, 84, 70–77. [Google Scholar] [CrossRef]
- Vanhavere, F.; Carinou, E.; Gualdrini, G.; Clairand, I.; Sans Merce, M.; Ginjaume, M.; Nikodemova, D.; Jankowski, J.; Bordy, J.; Rimpler, A. ORAMED: Optimization of Radiation Protection of Medical Staff; European Radiation Dosimetry e. V.: Braunschweig, Germany, 2012; Volume 2, p. 2012. [Google Scholar]
- Lynskey, G.; Powell, D.; Dixon, R.; Silberzweig, J. Radiation Protection in Interventional Radiology: Survey Results of Attitudes and Use. J. Vasc. Interv. Radiol. 2013, 24, 1547–1551.e3. [Google Scholar] [CrossRef]
- Okuyama, Y.; Okuyama, C.; Kawakami, T.; Nakatsugawa, Y.; Yamada, S.; Suzuki, T.; Tomatsuri, N.; Sato, H.; Yoshida, N. Evaluation of Radiation Doses to Medical Staffs During Endoscopic Retrograde CholangioPancreatography (ERCP) and Their Therapeutic Procedures and Decreasing Radiation Exposure to Staff by A Workshop. Gastroenterol. Endosc. 2016, 58, 991–998. [Google Scholar]
- Iwai, K.; Kawabata, K.; Sagane, M.; Kuchii, N. Radiation exposure management by personal dosimeter (glass badge). Med. J. Jpn. Red Cross Wakayama Med. Cent. 2017, 34, 79–87. [Google Scholar]
- World Health Organization. WHO Guidelines for Safe Surgery 2009; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Porter, A.J.; Narimasu, J.Y.; Mulroy, M.F.; Koehler, R.P. Sustainable, Effective Implementation of a Surgical Preprocedural Checklist: An “Attestation” Format for All Operating Team Members. Jt. Comm. J. Qual. Patient Saf. 2014, 40, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Haynes, A.B.; Edmondson, L.; Lipsitz, S.R.; Molina, G.; Neville, B.A.; Singer, S.J.; Moonan, A.T.; Childers, A.K.; Foster, R.; Gibbons, L.R.; et al. Mortality Trends After a Voluntary Checklist-based Surgical Safety Collaborative. Ann. Surg. 2017, 266, 923–929. [Google Scholar] [CrossRef] [PubMed]
- Martin, L.; Langell, J. Improving on-time surgical starts: The impact of implementing pre-OR timeouts and performance pay. J. Surg. Res. 2017, 219, 222–225. [Google Scholar] [CrossRef]
- Pham, J.C.; Laupola, T.M.T.; Figueira, A.; Bala, J.; Chun, L. Perceived Value of the Daily Safety Briefing. J. Healthc. Manag. 2019, 64, 44–51. [Google Scholar] [CrossRef]
- The Joint Commission Universal Protocol for Preventing Wrong Site, Wrong Procedure, Wrong Person Surgery. Available online: http://www.jointcommission.org/PatientSafety/UniversalProtocol/ (accessed on 14 February 2022).
- Gottumukkala, R.; Street, M.; Fitzpatrick, M.; Tatineny, P.; Duncan, J.R. Improving Team Performance During the Preprocedure Time-Out in Pediatric Interventional Radiology. Jt. Comm. J. Qual. Patient Saf. 2012, 38, 387–394. [Google Scholar] [CrossRef]
- Corso, R.; Vacirca, F.; Patelli, C.; Leni, D. Use of “Time-Out” checklist in interventional radiology procedures as a tool to enhance patient safety. La Radiol. Med. 2014, 119, 828–834. [Google Scholar] [CrossRef]
- Aizer, A.; Qiu, J.; Cheng, A.; Wu, P.; Holmes, D.; Wagner, S.; Bernstein, S.; Park, D.; Cartolano, B.; Barbhaiya, C.; et al. Utilization of a Radiation Safety Time-Out Reduces Radiation Exposure During Electrophysiology Procedures. JACC Clin. Electrophysiol. 2019, 5, 626–634. [Google Scholar] [CrossRef]
- Choi, B.H.; Yaya, K.; Prabhu, V.; Fefferman, N.; Mitchell, B.; Kuenzler, K.A.; Ginsburg, H.B.; Fisher, J.C.; Tomita, S. Simple preoperative radiation safety interventions significantly lower radiation doses during central venous line placement in children. J. Pediatr. Surg. 2019, 54, 170–173. [Google Scholar] [CrossRef]
- Barakat, M.T.; Thosani, N.C.; Huang, R.J.; Choudhary, A.; Kochar, R.; Kothari, S.; Banerjee, S. Effects of a Brief Educational Program on Optimization of Fluoroscopy to Minimize Radiation Exposure During Endoscopic Retrograde Cholangiopancreatography. Clin. Gastroenterol. Hepatol. 2018, 16, 550–557. [Google Scholar] [CrossRef]
- Boyum, J.H.; Rosier, A.S.; Tibor, L.C.; Turner, M.A.; Hess, A.R.; Kurup, A.N. Improving Universal Protocol Performance in Radiology through Implementation of a Standardized Time-out. RadioGraphics 2020, 40, 1182–1187. [Google Scholar] [CrossRef] [PubMed]
- International Commission on Radiological Protection. Ethical Foundations of the System of Radiological Protection; ICRP Publication 138. Ann.; SAGE Publications Ltd.: Thousand Oaks, CA, USA, 2018; Volume 47, pp. 1–65. [Google Scholar]
- Vimercati, L.; De Maria, L.; Mansi, F.; Caputi, A.; Ferri, G.; Luisi, V.; Lovreglio, P.; Cannone, E.; Lorusso, P.; Gatti, M.; et al. Prevalence of Thyroid Diseases in an Occupationally Radiation Exposed Group: A Cross-Sectional Study in a University Hospital of Southern Italy. Endocr. Metab. Immune Disord. Drug Targets 2019, 19, 803–808. [Google Scholar] [CrossRef] [PubMed]
- Cioffi, D.; Fontana, L.; Leso, V.; Dolce, P.; Vitale, R.; Vetrani, I.; Galdi, A.; Iavicoli, I. Low dose ionizing radiation exposure and risk of thyroid functional alterations in healthcare workers. Eur. J. Radiol. 2020, 132, 109279. [Google Scholar] [CrossRef] [PubMed]
- Chida, K.; Kaga, Y.; Haga, Y.; Kataoka, N.; Kumasaka, E.; Meguro, T.; Zuguchi, M. Occupational Dose in Interventional Radiology Procedures. AJR Am. J. Roentgenol. 2013, 200, 138–141. [Google Scholar] [CrossRef]

{kind=link}
| Forms of Occupational Health Management | Management Content |
|---|---|
| General management | Construction of safety management system related to radiation medical care, etc. |
| Work environment management | Measurement of radiation doses in the radiation clinic, personal monitoring implementation, etc. |
| Work management | Preparation of radiation treatment procedure manuals, maintenance of PPE *, etc. |
| Health management | Implementation of special radiation health examinations, etc. |
| Occupational health training | Regular education and training before and after placement of radiation work, etc. |
| Authors | Country | Physicians’ Personal Protective Equipment Use Rate (%) | |||
|---|---|---|---|---|---|
| Personal Passive Dosimeters | Lead Aprons | Lead Glasses | Thyroid Protection Collars | ||
| Niklason et al. (1993) [10] | N/A * | 40 | N/A * | 10 | 47 |
| Tsapaki et al. (2009) [11] | Algeria, Kenya, Morocco, Sudan, Tunisia, Kuwait, Lebanon, Syria, Thailand, United Arab Emirates, Pakistan, Armenia, Bosnia and Herzegovina, Bulgaria, Croatia, Greece, Lithuania, Moldova, Slovenia, Tajikistan | 96 | 100 | 73 | N/A* |
| Efstathopoulos et al. (2011) [16] | Greece | N/A * | 100 | 71–83 | 100 |
| Vanhavere F et al. (2012) [17] | Belgium, Greece, France, Switzerland, Poland, Slovakia | N/A * | 98–100 | 31–36 | 91–92 |
| Vano et al. (2013) [12] | Argentine Republic | 48–52 | N/A * | 41–52 | N/A * |
| Lynskey III et al. (2013) [18] | N/A * | N/A * | 99.4 | 54.2 | 94 |
| International Atomic Energy Agency (2014) [13] | Global | 70–77 | 97 | 24–47 | N/A * |
| Brun et al. (2018) [14] | France | 45.7–54.0 | 88–97.1 | 0–4 | 40–62.9 |
| Kunugita (2019) [7] | Japan | 17–100 | N/A * | N/A * | N/A * |
| Altintas et al. (2020) [15] | N/A * | 17.3 | 96.2 | 32.7 | 80.8 |
| Survey Content | Pre-Intervention Period (April 2017–August 2017) | Intervention Period (October 2017–February 2018) | |
|---|---|---|---|
| All radiological treatments conducted by survey target physicians | 549 cases | 415 cases | |
| Visual inspection of use status | Conducted by an inspector during the daytime | Conducted by an inspector at the pre-operative briefing during the daytime The inspector obtained verbal conformation and encouraged the physicians to wear proper equipment | |
| Personal passive dosimeter | Main dosimeter | 340 cases (61.9%) | 321 cases (77.3%) |
| Additional dosimeter | |||
| Lead apron | |||
| Lead glasses | |||
| Thyroid protection collar | |||
| Medical record survey | Conducted by researchers | Conducted by researchers | |
| Personal exposure dose | Effective dose | 549 cases (100%) | 415 cases (100%) |
| Lens equivalent dose | |||
| Exposure-related indicators | Number of times radiation medical treatment was conducted | ||
| Fluoroscopy time | |||
| Personal Passive Dosimeter/PPE | Pre-Intervention Period | Intervention Period | p Value † | ||
|---|---|---|---|---|---|
| Mean (%) | Median [Range] (%) | Mean (%) | Median [Range] (%) | ||
| Main dosimeter (under the lead apron) | 47 | 57 [0–100] | 97 | 100 [67–100] | 0.002 |
| Additional dosimeter (over the lead apron) | 30 | 0 [0–100] | 65 | 85 [0–100] | 0.008 |
| Lead apron | 100 | 100 | 100 | 100 | 1.000 |
| Lead glasses | 37 | 15 [0–100] | 97 | 100 [67–100] | 0.003 |
| Thyroid protection collar | 52 | 69 [0–100] | 97 | 100 [89–100] | 0.008 |
| Personal Exposure Dose/Dose Rate | Pre-Intervention Period | Intervention Period | p Value † | ||
|---|---|---|---|---|---|
| Mean | Median [Range] | Mean | Median [Range] | ||
| Effective dose (mSv) | 1.1 | 0.4 [0.0–6.3] | 1.4 | 1.1 [0.0–4.8] | 0.345 |
| Effective dose rate * (μSv/min) | 2.3 | 1.3 [0.0–13.6] | 7.3 | 3.1 [0.0–33.0] | 0.033 |
| Lens equivalent dose (mSv) | 3.2 | 0.7 [0.0–23.7] | 4.2 | 1.7 [0.1–13.9] | 0.124 |
| Lens equivalent dose rate ** (μSv/min) | 3.7 | 2.4 [0.0–15.9] | 28.7 | 7.5 [3.1–167.0] | 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matsuzaki, S.; Moritake, T.; Sun, L.; Morota, K.; Nagamoto, K.; Nakagami, K.; Kuriyama, T.; Hitomi, G.; Kajiki, S.; Kunugita, N. The Effect of Pre-Operative Verbal Confirmation for Interventional Radiology Physicians on Their Use of Personal Dosimeters and Personal Protective Equipment. Int. J. Environ. Res. Public Health 2022, 19, 16825. https://doi.org/10.3390/ijerph192416825
Matsuzaki S, Moritake T, Sun L, Morota K, Nagamoto K, Nakagami K, Kuriyama T, Hitomi G, Kajiki S, Kunugita N. The Effect of Pre-Operative Verbal Confirmation for Interventional Radiology Physicians on Their Use of Personal Dosimeters and Personal Protective Equipment. International Journal of Environmental Research and Public Health. 2022; 19(24):16825. https://doi.org/10.3390/ijerph192416825
Chicago/Turabian StyleMatsuzaki, Satoru, Takashi Moritake, Lue Sun, Koichi Morota, Keisuke Nagamoto, Koichi Nakagami, Tomoko Kuriyama, Go Hitomi, Shigeyuki Kajiki, and Naoki Kunugita. 2022. "The Effect of Pre-Operative Verbal Confirmation for Interventional Radiology Physicians on Their Use of Personal Dosimeters and Personal Protective Equipment" International Journal of Environmental Research and Public Health 19, no. 24: 16825. https://doi.org/10.3390/ijerph192416825
APA StyleMatsuzaki, S., Moritake, T., Sun, L., Morota, K., Nagamoto, K., Nakagami, K., Kuriyama, T., Hitomi, G., Kajiki, S., & Kunugita, N. (2022). The Effect of Pre-Operative Verbal Confirmation for Interventional Radiology Physicians on Their Use of Personal Dosimeters and Personal Protective Equipment. International Journal of Environmental Research and Public Health, 19(24), 16825. https://doi.org/10.3390/ijerph192416825