
Sedentary Behavioral Studies of Young and Middle-Aged Adults with Hypertension in the Framework of Behavioral Epidemiology: A Scoping Review

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Research Question
2.2. Inclusion and Exclusion Criteria
2.3. Literature Sources and Search Strategies
2.4. Evidence Selection and Information Extraction
3. Results
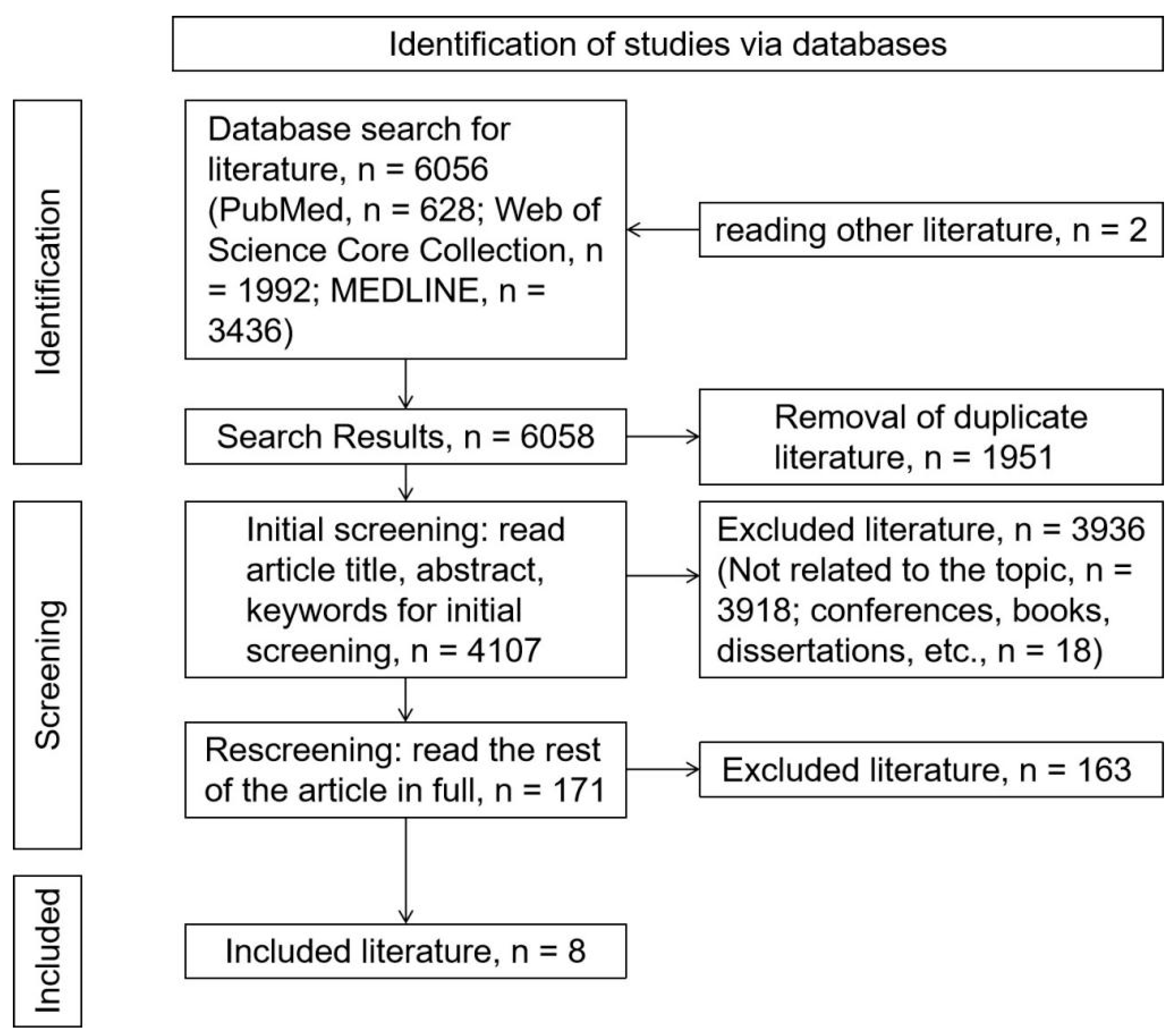
3.1. Literature Search Results
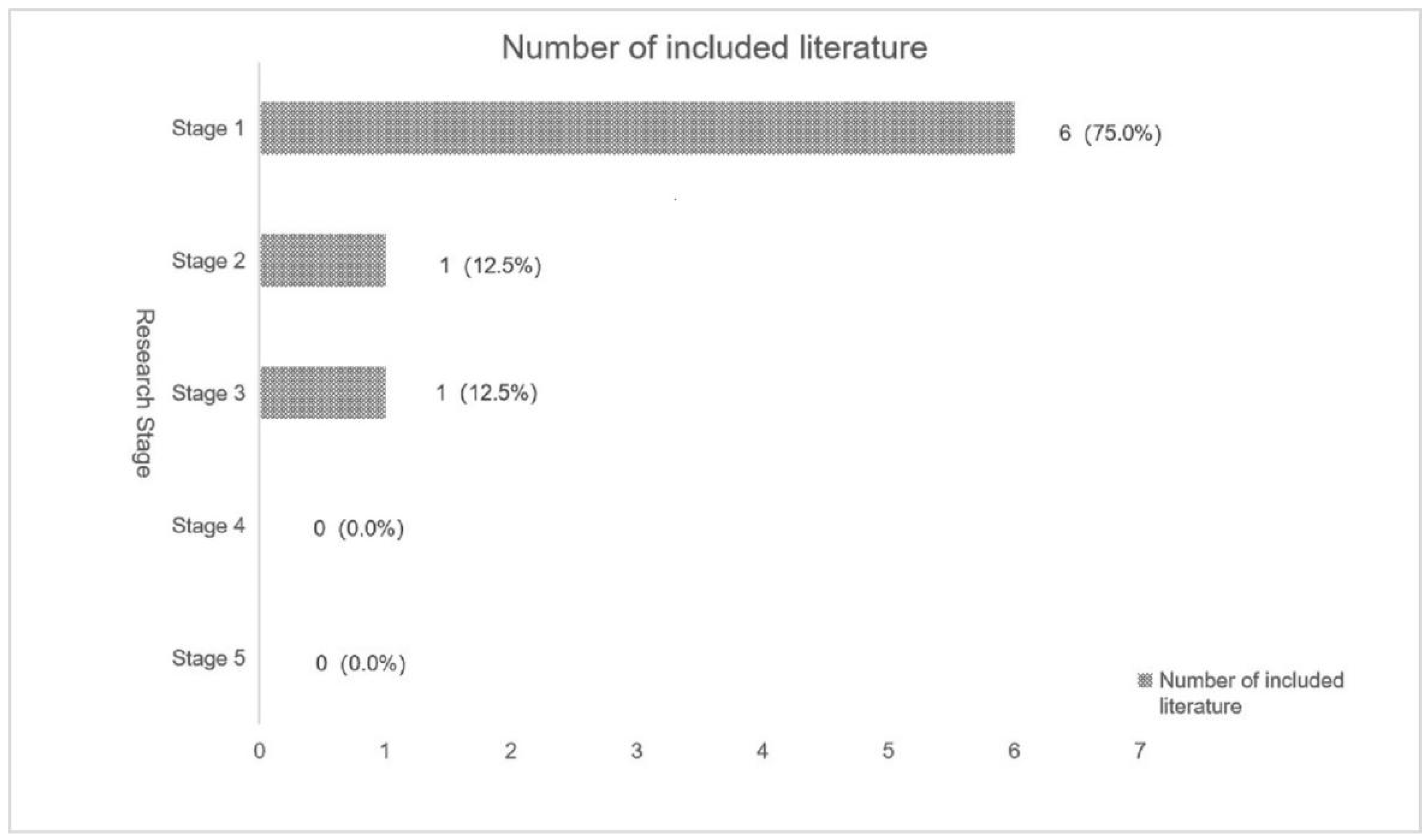
3.2. Characteristics of the Included Literature
3.3. Inclusion of Details from the Literature
3.3.1. Relationships with Health
3.3.2. Measurement Method
3.3.3. Influencing Factors
4. Discussion
4.1. SB and Health
4.2. Diagnosis and Measurement of SB
4.3. Influencing Factors of SB
4.4. General Analysis
4.5. Advantages and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- de Venecia, T.; Lu, M.; Figueredo, V.-M. Hypertension in young adults. Postgrad. Med. 2016, 128, 201–207. [Google Scholar] [CrossRef] [PubMed]
- Arija, V.; Villalobos, F.; Pedret, R.; Vinuesa, A.; Jovani, D.; Pascual, G.; Basora, J. Physical activity, cardiovascular health, quality of life and blood pressure control in hypertensive subjects: Randomized clinical trial. Health Qual. Life Outcomes 2018, 16, 184. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.; Ran, L.; Li, M.; Tan, X. Health-related quality of life of middle-aged and elderly people with hypertension: A cross-sectional survey from a rural area in China. PLoS ONE 2021, 16, e246409. [Google Scholar] [CrossRef] [PubMed]
- Owen, N.; Healy, G.-N.; Dempsey, P.-C.; Salmon, J.; Timperio, A.; Clark, B.-K.; Goode, A.-D.; Koorts, H.; Ridgers, N.-D.; Hadgraft, N.-T.; et al. Sedentary Behavior and Public Health: Integrating the Evidence and Identifying Potential Solutions. Annu. Rev. Public Health 2020, 41, 265–287. [Google Scholar] [CrossRef]
- Malete, L.; Ricketts, C.; Chen, S.; Jackson, J. Correlates of Physical Activity Among Adults in Botswana: Sociodemographic Factors, Health Status, and Body Image. J. Phys. Act. Health 2022, 19, 599–606. [Google Scholar] [CrossRef]
- Morton, S.; Fitzsimons, C.; Jepson, R.; Saunders, D.-H.; Sivaramakrishnan, D.; Niven, A. What works to reduce sedentary behavior in the office, and could these intervention components transfer to the home working environment?: A rapid review and transferability appraisal. Front. Sports Act. Living 2022, 4, 954639. [Google Scholar] [CrossRef]
- Desai, N.; Unni, G.; Agarwala, R.; Salagre, S.; Godbole, S.; Dengra, A.; Abhyankar, M.-V.; Revankar, S. Risk Factors and Comorbidities in Young Indian Patients with Hypertension: REAL YOUNG (Hypertension) Study. Integr. Blood Press. Control 2021, 14, 31. [Google Scholar] [CrossRef] [PubMed]
- Martins, L.C.G.; Lopes, M.V.D.; Guedes, N.-G.; Teixeira, I.-X.; de Sousa, V.E.C.; Montoril, M.-H. Nursing diagnosis sedentary lifestyle in individuals with hypertension: An analysis of accuracy. Revista Da Escola De Enfermagem Da Usp 2014, 48, 803–808. [Google Scholar] [CrossRef]
- Guedes, N.-G.; Lopes, M.-V.; Moreira, R.-P.; Cavalcante, T.-F.; de Araujo, T.-L. Prevalence of sedentary lifestyle in individuals with high blood pressure. Int. J. Nurs. Terminol. Classif. 2010, 21, 50–56. [Google Scholar] [CrossRef]
- Gavaldà, L.; Ramón, J.-M.; Torras, M.-G.; Amenós, A.M.; Rama, H.; Sarrias, X. The prevalence of cardiovascular risk factors in a population of essential hypertension patients. Rev. Esp. Cardiol. 1993, 46, 626–632. [Google Scholar]
- Ratnaparkhe, V.; Bhangale, A. Left Ventricular Diastolic Dysfunction in Primary Hypertension and its Relation with Leisure Time Physical Activity. J. Assoc. Phys. India 2015, 63, 20–24. [Google Scholar]
- Sampaio, F.-C.; De Oliveira, P.P.; Da Mata, L.R.F.; Moraes, J.T.; Da Fonseca, D.F.; de Sousa Vieira, V.A. Profile of nursing diagnoses in people with hypertension and diabetes. Investig. Educ. Enferm. 2017, 35, 139–153. [Google Scholar] [CrossRef] [PubMed]
- da Silva, P.M.; Maria-Joao, L.; Pedro-Macedo, N.; De Macedo, M.E. Prevalence of cardiovascular risk factors and other comorbidities in patients with hypertension in Portuguese primary health care populations: The PRECISE study. Rev. Port. De Cardiol. 2019, 38, 427–437. [Google Scholar]
- Esteves, D.; Duarte, P.; Pinheiro, P.; Bras, R.; Rodrigues, R.-G.; Gouveia, A.; O’Hara, K. Physical activity and supervised exercise among hypertensives and normotensives: Status and barriers. Sport Sci. Health 2020, 16, 323–330. [Google Scholar] [CrossRef]
- Liang, Z.-D.; Zhang, M.; Wang, C.-Z.; Yuan, Y.; Liang, J.-H. Association between sedentary behavior, physical activity, and cardiovascular disease-related outcomes in adults-A meta-analysis and systematic review. Front. Public Health 2022, 10, 1018460. [Google Scholar] [CrossRef] [PubMed]
- Sackner, M.-A.; Patel, S.; Adams, J.-A. Changes of blood pressure following initiation of physical inactivity and after external addition of pulses to circulation. Eur. J. Appl. Physiol. 2019, 119, 201–211. [Google Scholar] [CrossRef]
- Gerage, A.-M.; Benedetti, T.R.B.; Farah, B.-Q.; Santana, F.-D.; Ohara, D.; Andersen, L.-B.; Ritti-Dias, R.-M. Sedentary Behavior and Light Physical Activity Are Associated with Brachial and Central Blood Pressure in Hypertensive Patients. PLoS ONE 2015, 10, e0146078. [Google Scholar] [CrossRef]
- Cherfan, M.; Vallee, A.; Kab, S.; Salameh, P.; Goldberg, M.; Zins, M.; Blacher, J. Unhealthy behaviors and risk of uncontrolled hypertension among treated individuals-The CONSTANCES population-based study. Sci. Rep. 2020, 19, 25. [Google Scholar] [CrossRef]
- Gorostegi-Anduaga, I.; Corres, P.; Jurio-Iriarte, B.; Martinez-Aguirre, A.; Perez-Asenjo, J.; Aispuru, G.-R.; Arenaza, L.; Romaratezabala, E.; Arratibel-Imaz, I.; Mujika, I.; et al. Clinical, physical, physiological, and dietary patterns of obese and sedentary adults with primary hypertension characterized by sex and cardiorespiratory fitness: EXERDIET-HTA study. Clin. Exp. Hypertens. 2018, 40, 141–149. [Google Scholar] [CrossRef]
- Rabi, D.-M.; McBrien, K.-A.; Sapir-Pichhadze, R.; Nakhla, M.; Ahmed, S.-B.; Dumanski, S.-M.; Butalia, S.; Leung, A.-A.; Harris, K.-C.; Cloutier, L.; et al. Hypertension Canada’s 2020 Comprehensive Guidelines for the Prevention, Diagnosis, Risk Assessment, and Treatment of Hypertension in Adults and Children. Can. J. Cardiol. 2020, 36, 596–624. [Google Scholar] [CrossRef]
- Dempsey, P.-C.; Friedenreich, C.-M.; Leitzmann, M.-F.; Buman, M.-P.; Lambert, E.; Willumsen, J.; Bull, F. Global Public Health Guidelines on Physical Activity and Sedentary Behavior for People Living With Chronic Conditions: A Call to Action. J. Phys. Act. Health 2021, 18, 76–85. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, M.-S.; Aubert, S.; Barnes, J.-D.; Saunders, T.-J.; Carson, V.; Latimer-Cheung, A.-E.; Chastin, S.F.M.; Altenburg, T.-M.; Chinapaw, M.J.M. Sedentary Behavior Research Network (SBRN)—Terminology Consensus Project process and outcome. Int. J. Behav. Nutr. Phys. Act 2017, 14, 75. [Google Scholar] [CrossRef] [PubMed]
- WHO. Guidelines on Physical Activity and Sedentary Behaviour; World Health Organization: Geneva, Switzerland, 2020.
- Martins, L.C.G.; Lopes, M.V.O.; Diniz, C.-M.; Guedes, N.-G. The factors related to a sedentary lifestyle: A meta-analysis review. J. Adv. Nurs. 2021, 77, 1188–1205. [Google Scholar] [CrossRef] [PubMed]
- de Leon, A.-C.; Rodriguez-Perez, M.-D.; Rodriguez-Benjumeda, L.-M.; Ania-Lafuente, B.; Brito-Diaz, B.; de Fuentes, M.-M.; Almeida-Gonzalez, D.; Batista-Medina, M.; Aguirre-Jaime, A. Sedentary lifestyle: Physical activity duration versus percentage of energy expenditure. Rev. Esp. Cardiol. 2007, 60, 244–250. [Google Scholar] [CrossRef]
- Sallis, J.-F.; Owen, N.; Fotheringham, M.-J. Behavioral epidemiology: A systematic framework to classify phases of research on health promotion and disease prevention. Ann. Behav. Med. 2000, 22, 294–298. [Google Scholar] [CrossRef]
- Nery, M.-B.; Driver, S.; Vanderbom, K.-A. Systematic framework to classify the status of research on spinal cord injury and physical activity. Arch. Phys. Med. Rehabil. 2013, 94, 2027–2031. [Google Scholar] [CrossRef]
- Cleveland, S.; Driver, S.; Swank, C.; Macklin, S. Classifying physical activity research following stroke using the behavioral epidemiologic framework. Top. Stroke Rehabil. 2015, 22, 289–298. [Google Scholar] [CrossRef]
- Munn, Z.; Peters, M.D.J.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med. Res. Methodol. 2018, 18, 143. [Google Scholar] [CrossRef]
- Tricco, A.-C.; Lillie, E.; Zarin, W.; O’Brien, K.; Colquhoun, H.; Kastner, M.; Levac, D.; Ng, C.; Sharpe, J.-P.; Wilson, K.; et al. A scoping review on the conduct and reporting of scoping reviews. BMC Med. Res. Methodol. 2016, 16, 15. [Google Scholar] [CrossRef]
- O’Brien, K.-K.; Colquhoun, H.; Levac, D.; Baxter, L.; Tricco, A.-C.; Straus, S.; Wickerson, L.; Nayar, A.; Moher, D.; O’Malley, L. Advancing scoping study methodology: A web-based survey and consultation of perceptions on terminology, definition and methodological steps. BMC Health Serv. Res. 2016, 16, 305. [Google Scholar] [CrossRef]
- Tricco, A.-C.; Lillie, E.; Zarin, W.; O’Brien, K.-K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Gibbs, B.B.; Kowalsky, R.J.; Perdomo, S.J.; Taormina, J.M.; Balzer, J.R.; Jakicic, J.M. Effect of alternating standing and sitting on blood pressure and pulse wave velocity during a simulated workday in adults with overweight/obesity. J. Hypertens. 2017, 35, 2411–2418. [Google Scholar] [CrossRef] [PubMed]
- Alansare, A.-B.; Kowalsky, R.-J.; Jones, M.-A.; Perdomo, S.-J.; Stoner, L.; Gibbs, B.-B. The Effects of a Simulated Workday of Prolonged Sitting on Seated versus Supine Blood Pressure and Pulse Wave Velocity in Adults with Overweight/Obesity and Elevated Blood Pressure. J. Vasc. Res. 2020, 57, 355–366. [Google Scholar] [CrossRef] [PubMed]
- Perdomo, S.-J.; Gibbs, B.-B.; Kowalsky, R.-J.; Taormina, J.-M.; Balzer, J.-R. Effects of Alternating Standing and Sitting Compared to Prolonged Sitting on Cerebrovascular Hemodynamics. Sport Sci. Health 2019, 15, 375–383. [Google Scholar] [CrossRef] [PubMed]
- Hwu, C.-M.; Hsiao, C.-F.; Kuo, S.-W.; Wu, K.-D.; Ting, C.-T.; Quertermous, T.; Rodriguez, B.; Chen, I.; Grove, J.; Chen, P.-Y.; et al. Physical inactivity is an important lifestyle determinant of insulin resistance in hypertensive patients. Blood Press. 2004, 13, 355–361. [Google Scholar] [CrossRef]
- Palatini, P.; Massimo, P.; Marcello, R.; Paolo, P. Effect of regular physical activity on carotid intima-media thickness. Results from a 6-year prospective study in the early stage of hypertension. Blood Press. 2011, 20, 37–44. [Google Scholar] [CrossRef]
- Palatini, P.; Graniero, G.-R.; Mormino, P.; Nicolosi, L.; Mos, L.; Visentin, P.; Pessina, A.-C. Relation between physical training and ambulatory blood pressure in stage I hypertensive subjects. Results of the HARVEST Trial. Hypertension and Ambulatory Recording Venetia Study. Circulation 1994, 90, 2870–2876. [Google Scholar] [CrossRef] [PubMed]
- Palatini, P.; Visentin, P.; Dorigatti, F.; Guarnieri, C.; Santonastaso, M.; Cozzio, S.; Pegoraro, F.; Bortolazzi, A.; Vriz, O.; Mos, L.; et al. Regular physical activity prevents development of left ventricular hypertrophy in hypertension. Eur. Heart J. 2009, 30, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Castelo, G.; De Oliveira Lopes, M.V.; Guedes, N.G.; De Menezes, A.P.; de Oliveira Farias, O.; Dos Santos, N.A. Classification tree for the assessment of sedentary lifestyle among hypertensive. Investig. Educ. Enferm. 2016, 34, 113–119. [Google Scholar]
- Martins, L.-C.; Lopes, M.-V.; Guedes, N.-G.; Nunes, M.-M.; Diniz, C.-M.; Carvalho, P.-M. Sedentary lifestyle in individuals with hypertension. Rev. Bras. Enferm. 2015, 68, 1005–1012. [Google Scholar] [CrossRef]
- Guedes, N.-G.; Lopes, M.-V.; Cavalcante, T.-F.; Moreira, R.-P.; de Araujo, T.-L. Review of nursing diagnosis sedentary lifestyle in individuals with hypertension: Conceptual analysis. Rev. Esc. Enferm. USP 2013, 47, 742–749. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Lopes, M.-V.; Silva, V.-M.; Araujo, T.-L. Methods for establishing the accuracy of clinical indicators in predicting nursing diagnoses. Int. J. Nurs. Knowl. 2012, 23, 134–139. [Google Scholar] [CrossRef] [PubMed]
- Lavôr, L.C.d.C.; de Sousa, R.R.; Rodrigues, L.A.R.L.; Rodrigues Filho, O.d.S.; Paiva, A.d.A.; Frota, K.d.M.G. Prevalence of arterial hypertension and associated factors: A population-based study. Rev. Assoc. Med. Bras. 2020, 66, 630–636. [Google Scholar] [CrossRef] [PubMed]
- Wei, Q. The five-year effects of physical activity and sedentary behaviour on chronic disease morbidity of Chinese adults. Int. J. Serv. Technol. Manag. 2019, 25, 302–310. [Google Scholar] [CrossRef]
- Koyama, T.; Kuriyama, N.; Ozaki, E.; Tomida, S.; Uehara, R.; Nishida, Y.; Shimanoe, C.; Hishida, A.; Tamura, T.; Tsukamoto, M.; et al. Sedentary Time is Associated with Cardiometabolic Diseases in A Large Japanese Population: A Cross-Sectional Study. J. Atheroscler. Thromb. 2020, 27, 1097–1107. [Google Scholar] [CrossRef]
- Vancampfort, D.; Stubbs, B.; Koyanagi, A. Physical chronic conditions, multimorbidity and sedentary behavior amongst middle-aged and older adults in six low- and middle-income countries. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 147. [Google Scholar] [CrossRef]
- Katzmarzyk, P.-T.; Powell, K.-E.; Jakicic, J.-M.; Troiano, R.-P.; Piercy, K.; Tennant, B. Sedentary Behavior and Health: Update from the 2018 Physical Activity Guidelines Advisory Committee. Med. Sci. Sport Exerc. 2019, 51, 1227–1241. [Google Scholar] [CrossRef]
- Kim, Y.; Wilkens, L.-R.; Park, S.-Y.; Goodman, M.-T.; Monroe, K.-R.; Kolonel, L.-N. Association between various sedentary behaviours and all-cause, cardiovascular disease and cancer mortality: The Multiethnic Cohort Study. Int. J. Epidemiol. 2013, 42, 1040–1056. [Google Scholar] [CrossRef]
- Song, Y.-Y.; Lu, Y. Decision tree methods: Applications for classification and prediction. Shanghai Arch. Psychiatry 2015, 27, 130–135. [Google Scholar]
- Dempsey, P.-C.; Owen, N.; Biddle, S.-J.; Dunstan, D.-W. Managing sedentary behavior to reduce the risk of diabetes and cardiovascular disease. Curr. Diab. Rep. 2014, 14, 522. [Google Scholar] [CrossRef]
- Lopes, M.-V.; da Silva, V.M.; de Araujo, T.-L.; Guedes, N.-G.; Martins, L.-C.; Teixeira, I.-X. Instrument for evaluation of sedentary lifestyle in patients with high blood pressure. Rev. Bras. Enferm. 2015, 68, 445–451. [Google Scholar] [CrossRef] [PubMed]
- Islam, F.M.A.; Bhowmik, J.; Camera, D.-M.; Maddison, R.; Lambert, G.-W. Concordance between Different Criteria for Self-Reported Physical Activity Levels and Risk Factors in People with High Blood Pressure in a Rural District in Bangladesh. Int. J. Environ. Res. Public Health 2021, 18, 10487. [Google Scholar] [CrossRef] [PubMed]
- Ainsworth, B.; Cahalin, L.; Buman, M.; Ross, R. The current state of physical activity assessment tools. Prog. Cardiovasc. Dis. 2015, 57, 387–395. [Google Scholar] [CrossRef] [PubMed]
- Chu, A.H.Y.; Ng, S.H.X.; Koh, D.; Müller-Riemenschneider, F. Domain-Specific Adult Sedentary Behaviour Questionnaire (ASBQ) and the GPAQ Single-Item Question: A Reliability and Validity Study in an Asian Population. Int. J. Env. Res Public Health 2018, 15, 739. [Google Scholar] [CrossRef]
- Wienert, J.; Kuhlmann, T.; Fink, S.; Hambrecht, R.; Lippke, S. Motivational and Volitional Correlates of Physical Activity in Participants Reporting No, Past, and Current Hypertension: Findings from a Cross-Sectional Observation Study. Int. J. Behav. Med. 2017, 24, 908–914. [Google Scholar] [CrossRef]
- Martins, L.C.G.; Lopes, M.V.D.; Diniz, C.-M.; Matos, N.-C.; Magalhaes, L.-D.; Furtado, M.-A. Clinical indicators and aetiological factors of sedentary lifestyle in patients with arterial hypertension. J. Clin. Nurs. 2021, 30, 3330–3341. [Google Scholar] [CrossRef]
- Guedes, N.-G.; Lopes, M.-V.; Araujo, T.-L.; Moreira, R.-P.; Martins, L.-C. Predictive factors of the nursing diagnosis sedentary lifestyle in people with high blood pressure. Public Health Nurs. 2011, 28, 193–200. [Google Scholar] [CrossRef]
- Delfino, L.-D.; Tebar, W.-R.; Tebar, F.C.S.G.; DE Souza, J.-M.; Romanzini, M.; Fernandes, R.-A.; Christofaro, D.G.D. Association between sedentary behavior, obesity and hypertension in public school teachers. Ind. Health 2020, 58, 345–353. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Author (Time of Publication) | Stage 1 | Number of Samples (Age 2) | Country/Region | Research Type | Tools for Measuring SB (Definition/Program 3) | Result Indicators |
|---|---|---|---|---|---|---|
| Gibbs et al. [33] (2017) | 1 | 25 (average age: 42; 20–65 years old) | United States of America | Randomized controlled trials | activPAL3 micro (two periods of 3 h and 40 min of continuous seated desk work). | BP 4; PWV 5 |
| Alansare et al. [34] (2020) | 1 | 25 (20–65 years old) | United States of America | Randomized controlled trials | activPAL3 micro (except for required bathroom breaks, participants worked at a conventional desk while sitting still during the sitting period, with their feet flat on the floor). | BP; PWV |
| Perdomo et al. [35] (2019) | 1 | 25 (average age: 42; 20–65 years old) | United States of America | Randomized controlled trials | Global Physical Activity Questionnaire (the SB group was required to sit continuously). | BP; CBFv 6 |
| Hwu et al. [36] (2004) | 1 | 872 (35–60 years old; SB subjects averaged 51.8 ± 8.5 years old; non-SB subjects averaged 52.7 ± 8.8 years old) | Asia-Pacific | Cross-sectional studies | Total physical activity was measured by keeping track of how many hours a day were spent engaging in physical activity. (Sedentary activity hours)/(24 h—base activity hours) was used to calculate physical inactivity (participants were referred to as “SB” if their physical activity score was higher than 0.5). | Insulin resistance |
| Palatini et al. [37] (2011) | 1 | 87 (SB subjects averaged 33.2 ± 8.7 years old; non-SB subjects averaged 29.7 ± 8.6 years old) | Italy | Prospective studies | A standardized questionnaire was used to measure physical activity [38] (participants were categorized as sedentary if they did not regularly engage in any physical activity). | Carotid intima–media thickness |
| Palatini et al. [39] (2009) | 1 | 454 (18–45 years old; average age: 33.1 ± 8.4 years old) | Italy | Prospective studies | A standardized questionnaire was used to measure physical activity [38] (participants were categorized as sedentary if they did not regularly engage in any physical activity). | LV 7 mass; LV hypertrophy |
| Castelo et al. [40] (2016) | 2 | 285 (19–59 years old) | Brazil | Cross-sectional studies | An instrument was used with variables related to identification, related factors, and signs and symptoms. The diagnostic inference was made by four nurses who had received prior training in an 8-h course [40] (definition based on NANDA-I 9). | SB 8 |
| Martins et al. [41] (2015) | 3 | 285 (19–59 years old) | Brazil | Cross-sectional studies | A tool that was created based on previously validated clinical signs and related factors was used to collect the data [42] (individuals with SB were defined as those who do not exercise at the recommended frequency, duration, and intensity or do not expend significant energy to improve their physical condition). | SB; PA 10 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, K.; Huang, S.; Feng, D.; Lang, X.; Wang, Q.; Liu, Y. Sedentary Behavioral Studies of Young and Middle-Aged Adults with Hypertension in the Framework of Behavioral Epidemiology: A Scoping Review. Int. J. Environ. Res. Public Health 2022, 19, 16796. https://doi.org/10.3390/ijerph192416796
Zhang K, Huang S, Feng D, Lang X, Wang Q, Liu Y. Sedentary Behavioral Studies of Young and Middle-Aged Adults with Hypertension in the Framework of Behavioral Epidemiology: A Scoping Review. International Journal of Environmental Research and Public Health. 2022; 19(24):16796. https://doi.org/10.3390/ijerph192416796
Chicago/Turabian StyleZhang, Kexin, Sufang Huang, Danni Feng, Xiaorong Lang, Quan Wang, and Yuchen Liu. 2022. "Sedentary Behavioral Studies of Young and Middle-Aged Adults with Hypertension in the Framework of Behavioral Epidemiology: A Scoping Review" International Journal of Environmental Research and Public Health 19, no. 24: 16796. https://doi.org/10.3390/ijerph192416796
APA StyleZhang, K., Huang, S., Feng, D., Lang, X., Wang, Q., & Liu, Y. (2022). Sedentary Behavioral Studies of Young and Middle-Aged Adults with Hypertension in the Framework of Behavioral Epidemiology: A Scoping Review. International Journal of Environmental Research and Public Health, 19(24), 16796. https://doi.org/10.3390/ijerph192416796