
A Technology-Based Intervention to Support Older Adults in Living Independently: Protocol for a Cross-National Feasibility Pilot

 , , , , , , , and
, , , , , , , and
Abstract
1. Introduction
Study Objectives
2. Methodology
2.1. Study Design
- Prior to the start of the experimentation (T0);
- Ten days into the intervention study, i.e., at the midterm of the trial (T1);
- After 21 days, i.e., at the end of the trial (T2).
2.2. Study Setting
2.3. Participants
2.4. Recruitment
2.5. Trial status
2.6. The Intervention
- Heart rate testing in association with the frequency indicated on the smartwatch;
- Testing the emergency system by pressing the power button 3 times;
- Testing of the flood and door sensors by visualizing the values received by the SAVE cloud app through the SAVE Web App;
- Calling a friend/relative from their smartwatch.
- Kit creation (from the SAVE Admin Centre)—a unique kit key will be generated;
- Adding devices to the kit (1 x Save Sensor Adapter and 1 x Galaxy Watch 3);
- Checking the internet connection of the phone/home router in Romania/Italy and the provided mobile phone in Hungary);
- Verify that the user has a Gmail account; for those users who do not have an account, an account is created;
- User account creation (self-register—from the SAVE Web App) (Figure 1);
- Filling in the user profile, including the Kit Key;
- Installation of the Aqara Home app from the Play Store;
- Installation and placement of Aqara hub and sensors by following the instruction in the Aqara Home app (Figure 2);
- Test the functioning of all sensors through the Aqara Home app;
- Adding a remote control for the Sony projector from the Aqara Home app on the Aqara hub;
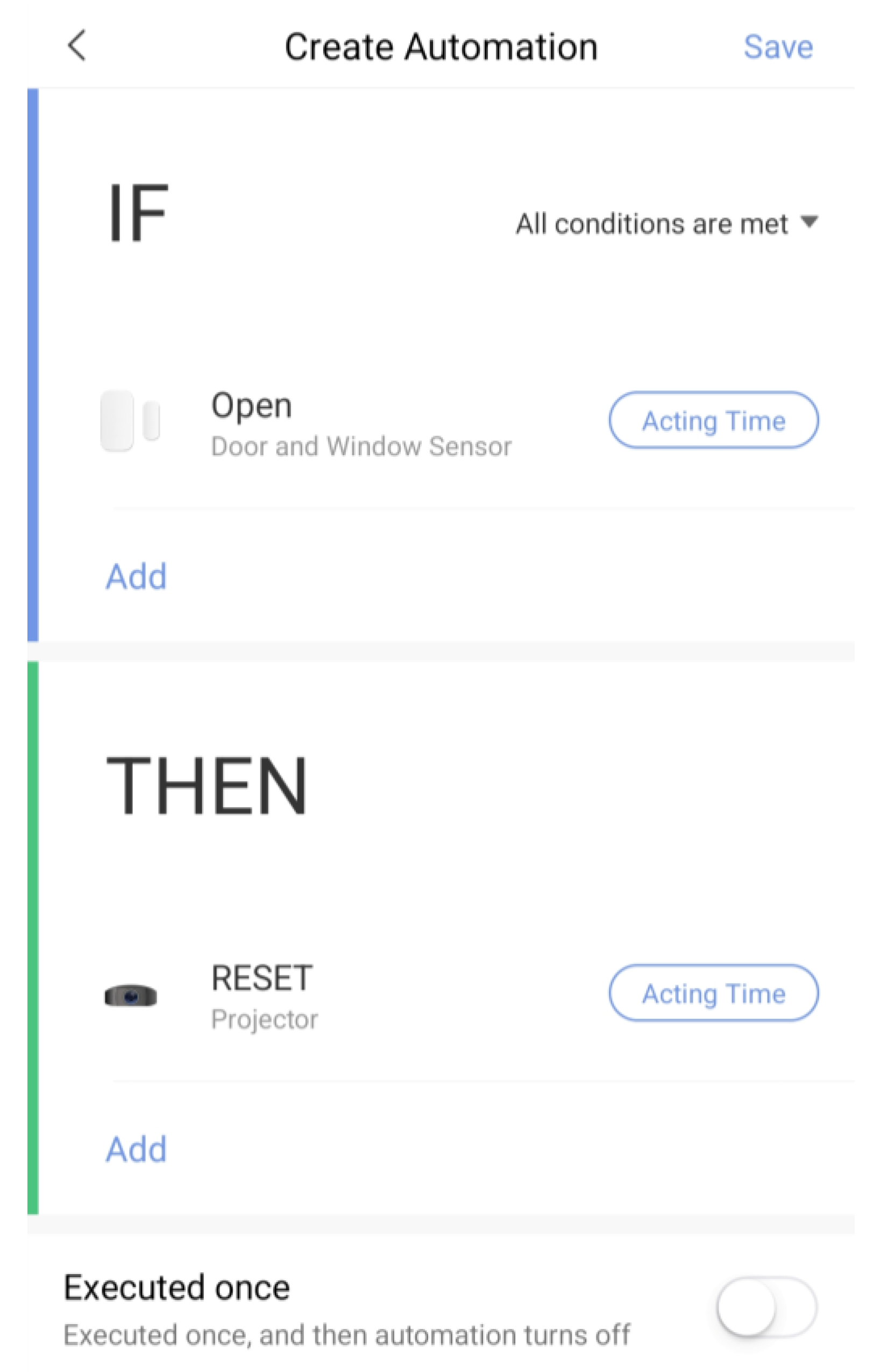
- Adding the SAVE automations in the Aqara Home app by following the instruction in the Aqara Home app and the SAVE installation manual (Figure 3);
- Test the sensors through the SAVE Platform;
- Installation of Galaxy Wear app from the Play Store;
- Pairing the smartwatch to the Galaxy Wear app;
- Activate Debug mode on the smartwatch;
- Installation of the two smartwatch apps using the sdb tool provided by Tizen Studio (save-configuration.wgt and save-tizen-watch-face.wgt);
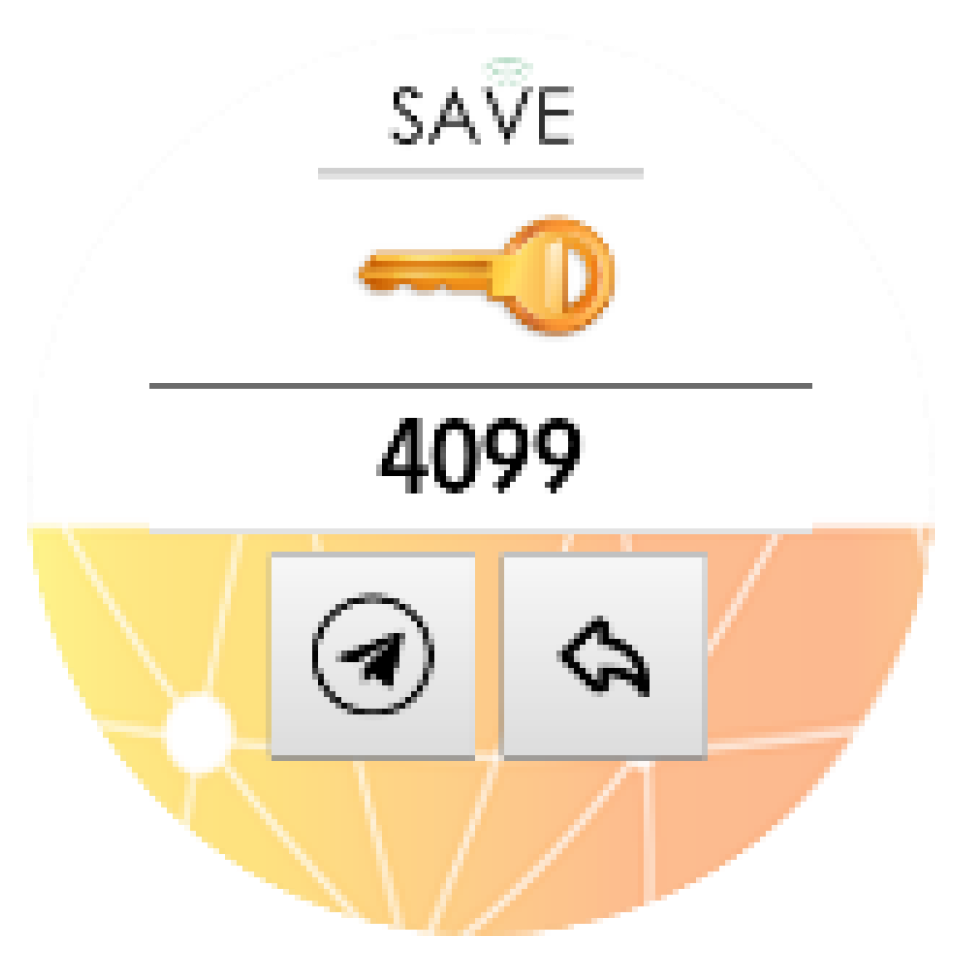
- Configure the smartwatch for SAVE by filling in the native ID into the SAVE configuration app (Figure 6);
- Setting the smartwatch face to the SAVE watch face (Figure 7);
- Configuration of the SOS and fall detection features from the Galaxy Wear app;
- Test the emergency system. Furthermore, test the data sent from the watch together with the data sent from home (Figure 8);
- Creation of caregivers’ SAVE Web accounts;
- Linking the caregivers accounts to the end-user account via the SAVE Web app.
2.7. The Outcomes
2.7.1. The Primary Outcomes
- Learnability of the system, which is seen as a component of usability, is the degree to which an interface is intuitive, and the user can immediately understand how to interact with the system. This result will be measured through the SUS scale [28].
2.7.2. The Secondary Outcomes
- Self-efficacy is the set of beliefs we have about our ability to complete a certain task. This result will be measured through the short version of the GSE self-efficacy scale [32].
2.8. Data Collection
- (A)
- Health and Wellness Condition:
- Mini-Mental State Examination (MMSE) [33] is a neuropsychological test for the evaluation of disorders of intellectual efficiency and the presence of cognitive impairment. The test consists of 30 questions, which refer to various cognitive areas: orientation in time and space, recording of words, attention and calculation, re-enactment, language, and constructive praxis. The total score is between a minimum of 0 and a maximum of 30 points. A score of 26 to 30 is an indication of cognitive normality. The score is adjusted with the coefficient for age and schooling [34].
- Functional Ambulation Category (FAC) [35] is a scale that evaluates the ability to achieve autonomy in walking. The ambulatory capacity is evaluated with a score ranging from 0 to 5, where 0 indicates total dependence and 5 indicates complete independence. From the score obtained, it can be deduced the amount of support that the patient requires when walking and on what kind of surfaces he is able to walk.
- The Barthel Index [36] is an objective and standardized tool for measuring functional status. The individual is scored in a number of areas depending upon the independence of performance. Total scores range from 0 (complete dependence) to 100 (complete independence).
- SF-12v2 ™ Health Survey [37] is a widely used instrument and is a 12-element subset of the SF-36v2 ™. It is a short and reliable measure of the general state of health. It is useful in health surveys of large populations and has been widely used as a screening tool.
- Five Well-Being (WHO-5) Index [30] is a short self-reported measure of current mental well-being.
- EuroQol-5 Dimension-5 Level (EQ-5D-5L) [31] is a self-report survey that measures the quality of life across 5 domains: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each dimension is scored on a 5-level severity ranking that ranges from ‘No problems’ through ‘Extreme problems’.
- (B)
- Self-efficacy:
- General Self-Efficacy Scale (GSE) [32]. Its abbreviated form of ten entries is a reliable and valid tool for assessing general self-efficacy.
- (C)
- Usability and Acceptance:
- System Usability Scale (SUS) [28] is a reliable tool for measuring usability. It consists of a 10-item questionnaire with five response options for respondents from ‘Strongly agree’ to ‘Strongly disagree’. It allows for evaluating various products and services, including hardware, software, mobile devices, websites, and applications. It is easy to administer to participants, can be used on small sample sizes with reliable results, and can effectively differentiate between usable and unusable systems.
- User Experience Questionnaire (UEQ-S) [29]. This short version of the questionnaire measures the subjective impression of users towards the user experience of products. The UEQ is a semantic differential with 26 items. Both classical usability aspects (efficiency, perspicuity, dependability) and user experience aspects (originality, stimulation) are measured.
- Quebec User Evaluation of Satisfaction with assistive Technology (QUEST—Version 2.0) [38] is a 12-item outcome measure that assesses user satisfaction with two components, Device and Services.
- (D)
- Privacy and Stigmatization
- Open questions
- Usefulness of the system,
- Reliability of the system,
- Impact of the system on the reduction in time spent in caregiving activities;
- Impact of the system on the reduction in the cost of caregiving activities;
- Impact of the system on the reduction in the workload.
2.9. Data Analysis
3. Discussion
4. Ethics and Dissemination
4.1. Risk Management, Mitigation, and Possible Limitations for the Users
4.2. Data Management
4.3. Dissemination
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- United Nations; Department of Economic and Social Affairs; Population Division. World Population Prospects. 2022. Available online: https://esa.un.org/unpd/wpp/Download/Standard/Population/ (accessed on 15 March 2022).
- Foster, L.; Walker, A. Active and successful aging: A European policy perspective. Gerontologist 2015, 55, 83–90. [Google Scholar] [CrossRef] [PubMed]
- López-López, R.; Sánchez, M. The institutional active aging paradigm in Europe (2002–2015). Gerontologist 2020, 60, 406–415. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Active Ageing: A Policy Framework. Available online: https://apps.who.int/iris/bitstream/handle/10665/67215/WHO_NMH_NPH_02.8.pdf (accessed on 15 March 2022).
- European Commission. Employment, Social Affairs & Inclusion. Active Ageing. Available online: http://ec.europa.eu/social/main.jsp?catId=1062&langId=en (accessed on 15 March 2022).
- De Angeli, A.; Jovanović, M.; McNeill, A.; Coventry, L. Desires for active ageing technology. Int. J. Hum. Comput. 2020, 138, 102412. [Google Scholar] [CrossRef]
- Iecovich, E. Aging in place: From theory to practice. Anthropol. Noteb. 2014, 20, 21–33. [Google Scholar]
- Kim, K.I.; Gollamudi, S.S.; Steinhubl, S. Digital technology to enable aging in place. Exp. Gerontol. 2017, 88, 25–31. [Google Scholar] [CrossRef]
- The National Academies of Sciences, Engineering, and Medicine. Social Isolation and Loneliness in Older Adults: Opportunities for the Health Care System; National Academies Press: Washington, DC, USA, 2020. [Google Scholar]
- Perissinotto, C.; Holt-Lunstad, J.; Periyakoil, V.S.; Covinsky, K. A practical approach to assessing and mitigating loneliness and isolation in older adults. J. Am. Geriatr. Soc. 2019, 67, 657–662. [Google Scholar] [CrossRef]
- Evans, I.E.M.; Martyr, A.; Collins, R.; Brayne, C.; Clare, L. Social isolation and cognitive function in later life: A systematic review and meta-analysis. J. Alzheimers Dis. 2019, 70, S119–S144. [Google Scholar] [CrossRef]
- Malcolm, M.; Frost, H.; Cowie, J. Loneliness and social isolation causal association with health-related lifestyle risk in older adults: A systematic review and meta-analysis protocol. Syst. Rev. 2019, 8, 48. [Google Scholar] [CrossRef]
- Hauer, K. Quality of assistive technologies in the home care for elderly. Stud. Health Technol. Inform. 2015, 212, 134–140. [Google Scholar]
- Kim, M.H.; Xiang, X. Hospitalization trajectories in home- and community-based services recipients: The influence of physician and social care density. J. Gerontol. B. Psychol. Sci. Soc. Sci. 2021, 76, 1679–1690. [Google Scholar] [CrossRef]
- Willner, V.; Schneider, C.; Feichtenschlager, M. eHealth 2015 Special Issue: Effects of an assistance service on the quality of life of elderly users. Appl. Clin. Inform. 2015, 6, 429–442. [Google Scholar] [PubMed]
- Fazekas, G.; Tavaszi, I. The future role of robots in neuro-rehabilitation. Expert Rev. Neurother. 2019, 19, 471–473. [Google Scholar] [CrossRef] [PubMed]
- Fazekas, G. Robotics in rehabilitation: Successes and expectations. Int. J. Rehabil. Res. 2013, 36, 95–96. [Google Scholar] [CrossRef] [PubMed]
- Khosravi, P.; Ghapanchi, A.H. Investigating the effectiveness of technologies applied to assist seniors: A systematic literature review. Int. J. Med. Inform. 2016, 85, 17–26. [Google Scholar] [CrossRef] [PubMed]
- Valokivi, H.; Carlo, S.; Kvist, E.; Outila, M. Digital ageing in Europe: A comparative analysis of Italian, Finnish and Swedish national policies on eHealth. Ageing Soc. 2021, 8, 1–22. [Google Scholar] [CrossRef]
- Wilkowska, W.; Offermann, J.; Spinsante, S.; Poli, A.; Ziefle, M. Analyzing technology acceptance and perception of privacy in ambient assisted living for using sensor-based technologies. PLoS ONE 2022, 17, e0269642. [Google Scholar] [CrossRef]
- Aggar, C.; Sorwar, G.; Seton, C.; Penman, O.; Ward, A. Smart home technology to support older people’s quality of life: A longitudinal pilot study. Int. J. Older People Nurs. 2022, e12489. [Google Scholar] [CrossRef]
- Johansson-Pajala, R.-M.; Gusdal, A.; Eklund, C.; Florin, U.; von Heideken Wågert, P. A codesigned web platform for reducing social isolation and loneliness in older people: A feasibility study. Inform. Health Soc. Care 2022, 2070068. [Google Scholar] [CrossRef]
- Piculell, E.; Skär, L.; Sanmartin Berglund, J.; Anderberg, P.; Bohman, D. Using a mobile application for health communication to facilitate a sense of coherence: Experiences of older persons with cognitive impairment. Int. J. Environ. Res. Public Health 2021, 18, 11332. [Google Scholar] [CrossRef]
- Xie, B.; Charness, N.; Fingerman, K.; Kaye, J.; Kim, M.T.; Khurshid, A. When going digital becomes a necessity: Ensuring older adults’ needs for information, services, and social inclusion during COVID-19. J. Aging Soc. Policy 2020, 32, 460–470. [Google Scholar] [CrossRef]
- Mooses, K.; Camacho, M.; Cavallo, F.; Burnard, M.-D.; Dantas, C.; D’Onofrio, G.; Fernandes, A.; Fiorini, L.; Gama, A.; Perandrés Gómez, A.; et al. Involving older adults during COVID-19 restrictions in developing an ecosystem supporting Active Aging: Overview of alternative elicitation methods and common requirements from five European Countries. Front. Psychol. 2022, 13, 818706. [Google Scholar] [CrossRef]
- Cuffaro, L.; Di Lorenzo, F.; Bonavita, S.; Tedeschi, G.; Leocani, L.; Lavorgna, L. Dementia care and COVID-19 pandemic: A necessary digital revolution. Neurol. Sci. 2020, 41, 1977–1979. [Google Scholar] [CrossRef] [PubMed]
- Rampioni, M.; Moșoi, A.A.; Rossi, L.; Moraru, S.A.; Rosenberg, D.; Stara, V. A qualitative study toward technologies for Active and Healthy Aging: A thematic analysis of perspectives among primary, secondary, and tertiary end users. Int. J. Environ. 2021, 18, 7489. [Google Scholar] [CrossRef] [PubMed]
- Brooke, J. SUS: A ‘Quick and Dirty’ Usability Scale. In Usability Evaluation in Industry, 1st ed.; Jordan, W.P., Thomas, B., McClelland, I.L., Weerdmeester, B., Eds.; CRC Press: London, UK, 1996; ISBN 9780429157011. [Google Scholar]
- Schrepp, M.; Hinderks, A.; Thomaschewski, J. Design and evaluation of a short version of the user experience questionnaire (UEQ-S). IJIMAI 2017, 4, 103–108. [Google Scholar] [CrossRef]
- Bech, P. Measuring the dimension of psychological general well-being by the WHO-5. QoL Newsletter 2004, 15–16. [Google Scholar]
- Group, The EuroQol. EuroQol-A new facility for the measurement of health-related quality of life. Health Policy 1990, 16, 199–208. [Google Scholar] [CrossRef]
- Schwarzer, R.; Jerusalem, M. Generalized Self-efficacy Scale. In Measures in Health Psychology: A User’s Portfolio. Causal and Control Beliefs; Weinman, J., Wright, S., Johnston, M., Eds.; NFER-Nelson: Windsor, Berkshire, UK, 1995; pp. 35–37. [Google Scholar]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-Mental State”: A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Magni, E.; Binetti, G.; Bianchetti, A.; Rozzini, R.; Trabucchi, M. Mini-Mental State Examination: A normative study in Italian elderly population. Eur. J. Neurol. 1996, 3, 198–202. [Google Scholar] [CrossRef]
- Mehrholz, J.; Wagner, K.; Rutte, K.; Meiβner, D.; Pohl, M. Predictive validity and responsiveness of the functional ambulation category in hemiparetic patients after stroke. Arch. Phys. Med. Rehabil. 2007, 88, 1314–1319. [Google Scholar] [CrossRef]
- Collin, C.; Wade, D.T.; Davies, S.; Horne, V. The Barthel ADL Index: A reliability study. Int. Disabil. 1988, 10, 61–63. [Google Scholar] [CrossRef]
- Ware, J.E.; Kosinski, M.; Keller, S.D. A 12-item short-form health survey: Construction of scale and preliminary tests of reliability and validity. Med. Care 1996, 34, 220–233. [Google Scholar] [CrossRef] [PubMed]
- Demers, L.; Weiss-Lambrou, R.; Ska, B. The Quebec User Evaluation of Satisfaction with assistive Technology (QUEST 2.0): An overview and recent progress. Technol. Disabil. 2002, 14, 101–105. [Google Scholar] [CrossRef]
- Kang, H. Sample size determination and power analysis using the G*Power software. J. Educ. Eval. Health Prof. 2021, 18, 17. [Google Scholar] [CrossRef] [PubMed]
- Del Barrio, E.; Marsillas, S.; Buffel, T.; Smetcoren, A.-S.; Sancho, M. From active aging to active citizenship: The role of (age) friendliness. Soc. Sci. 2018, 7, 134. [Google Scholar] [CrossRef]
- Ahn, M.; Kwon, H.J.; Kang, J. Supporting aging-in-place well: Findings from a cluster analysis of the reasons for aging-in-place and perceptions of well-being. J. Appl. Gerontol. 2020, 39, 3–15. [Google Scholar] [CrossRef]
- Czaja, S.J.; Boot, W.R.; Charness, N.; Rogers, W.A. Designing for Older Adults: Principles and Creative Human Factors Approaches, 3rd ed.; CRC Press: Boca Raton, FL, USA, 2019. [Google Scholar]
- Lindeman, D.A. Improving the independence of older adults through technology: Directions for public policy. Public Policy Aging Rep. 2017, 27, 49–52. [Google Scholar] [CrossRef][Green Version]
- Machón, M.; Larrañaga, I.; Dorronsoro, M.; Vrotsou, K.; Vergara, I. Health-related quality of life and associated factors infunctionally independent older people. BMC Geriatr. 2017, 17, 1–9. [Google Scholar] [CrossRef]
- Rogers, W.A.; Mitzner, T.L. Envisioning the future for older adults: Autonomy, health, well-being, and social connectedness with technology support. Futures 2017, 87, 133–139. [Google Scholar] [CrossRef]
- Astell, A.J.; McGrath, C.; Dove, E. ‘That’s for old so and so’s!’: Does identity influence older adults’ technology adoption decisions? Ageing Soc. 2020, 40, 1550–1576. [Google Scholar] [CrossRef]
- Mannheim, I.; Schwartz, E.; Xi, W.; Buttigieg, S.C.; McDonnell-Naughton, M.; Wouters, E.J.M.; van Zaalen, Y. Inclusion of older adults in the research and design of digital technology. Int. J. Environ. Res. Public Health 2019, 16, 3718. [Google Scholar] [CrossRef]
- Lee, L.N.; Kim, M.J. A critical review of smart residential environments for older adults with a focus on pleasurable experience. Front. Psychol. 2020, 10, 3080. [Google Scholar] [CrossRef] [PubMed]
- Quan-Hasse, A.; Williams, C.; Kicevski, M.; Elueze, I.; Wellman, B. Dividing the grey divide: Deconstructing myths about older adults’ online activities, skills, and attitudes. Am. Behav. Sci. 2018, 62, 1207–1228. [Google Scholar] [CrossRef]
- Schreurs, K.; Quan-Haase, A.; Martin, K. Problematizing the digital literacy paradox in the context of older adults’ ICT use. Can. J. Commun. 2017, 42, 259–377. [Google Scholar] [CrossRef]
- Goethals, L.; Barth, N.; Guyot, J.; Hupin, D.; Celarier, T.; Bongue, B. Impact of home quarantine on physical activity among older adults living at home during the COVID-19 pandemic: Qualitative interview study. JMIR Aging 2020, 3, e19007. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| End User Type | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Primary users |
|
|
| Secondary users |
|
|
| Tertiary users |
|
|
| Type of End Users | Dimensions | Scales | Timing of Data Collection | ||
|---|---|---|---|---|---|
| T0 | T1 | T2 | |||
| Primary users | Health and Wellness Condition | MMSE | X | ||
| FAC | X | ||||
| Barthel Index | X | ||||
| SF-12v2 | X | X | X | ||
| WHO-5 Index | X | X | X | ||
| EQ-5D-5L | X | X | X | ||
| Self-efficacy | GSE | X | X | X | |
| Usability and Acceptance | SUS | X | X | ||
| UEQ-S | X | X | |||
| QUEST 2.0 | X | X | |||
| Privacy and Stigma | Open questions | X | X | X | |
| Secondary users | Usefulness | X | X | X | |
| Reliability | X | X | X | ||
| Tertiary users | Reduction in time | X | X | X | |
| Reduction in cost | X | X | X | ||
| Reduction in workload | X | X | X | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stara, V.; Rampioni, M.; Moșoi, A.A.; Kristaly, D.M.; Moraru, S.-A.; Paciaroni, L.; Paolini, S.; Raccichini, A.; Felici, E.; Rossi, L.; et al. A Technology-Based Intervention to Support Older Adults in Living Independently: Protocol for a Cross-National Feasibility Pilot. Int. J. Environ. Res. Public Health 2022, 19, 16604. https://doi.org/10.3390/ijerph192416604
Stara V, Rampioni M, Moșoi AA, Kristaly DM, Moraru S-A, Paciaroni L, Paolini S, Raccichini A, Felici E, Rossi L, et al. A Technology-Based Intervention to Support Older Adults in Living Independently: Protocol for a Cross-National Feasibility Pilot. International Journal of Environmental Research and Public Health. 2022; 19(24):16604. https://doi.org/10.3390/ijerph192416604
Chicago/Turabian StyleStara, Vera, Margherita Rampioni, Adrian Alexandru Moșoi, Dominic M. Kristaly, Sorin-Aurel Moraru, Lucia Paciaroni, Susy Paolini, Alessandra Raccichini, Elisa Felici, Lorena Rossi, and et al. 2022. "A Technology-Based Intervention to Support Older Adults in Living Independently: Protocol for a Cross-National Feasibility Pilot" International Journal of Environmental Research and Public Health 19, no. 24: 16604. https://doi.org/10.3390/ijerph192416604
APA StyleStara, V., Rampioni, M., Moșoi, A. A., Kristaly, D. M., Moraru, S.-A., Paciaroni, L., Paolini, S., Raccichini, A., Felici, E., Rossi, L., Vizitiu, C., Nistorescu, A., Marin, M., Tónay, G., Tóth, A., Pilissy, T., & Fazekas, G. (2022). A Technology-Based Intervention to Support Older Adults in Living Independently: Protocol for a Cross-National Feasibility Pilot. International Journal of Environmental Research and Public Health, 19(24), 16604. https://doi.org/10.3390/ijerph192416604