
Effects of Exercise Programs on Psychoemotional and Quality-of-Life Factors in Adult Patients with Cancer and Hematopoietic Stem Cell Transplantation or Bone Marrow Transplantation: A Systematic Review

 ,
,  ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Systematic Search
2.2. Selection of the Studies
2.3. Data Extraction
2.4. Risk of Bias Assessment
3. Results
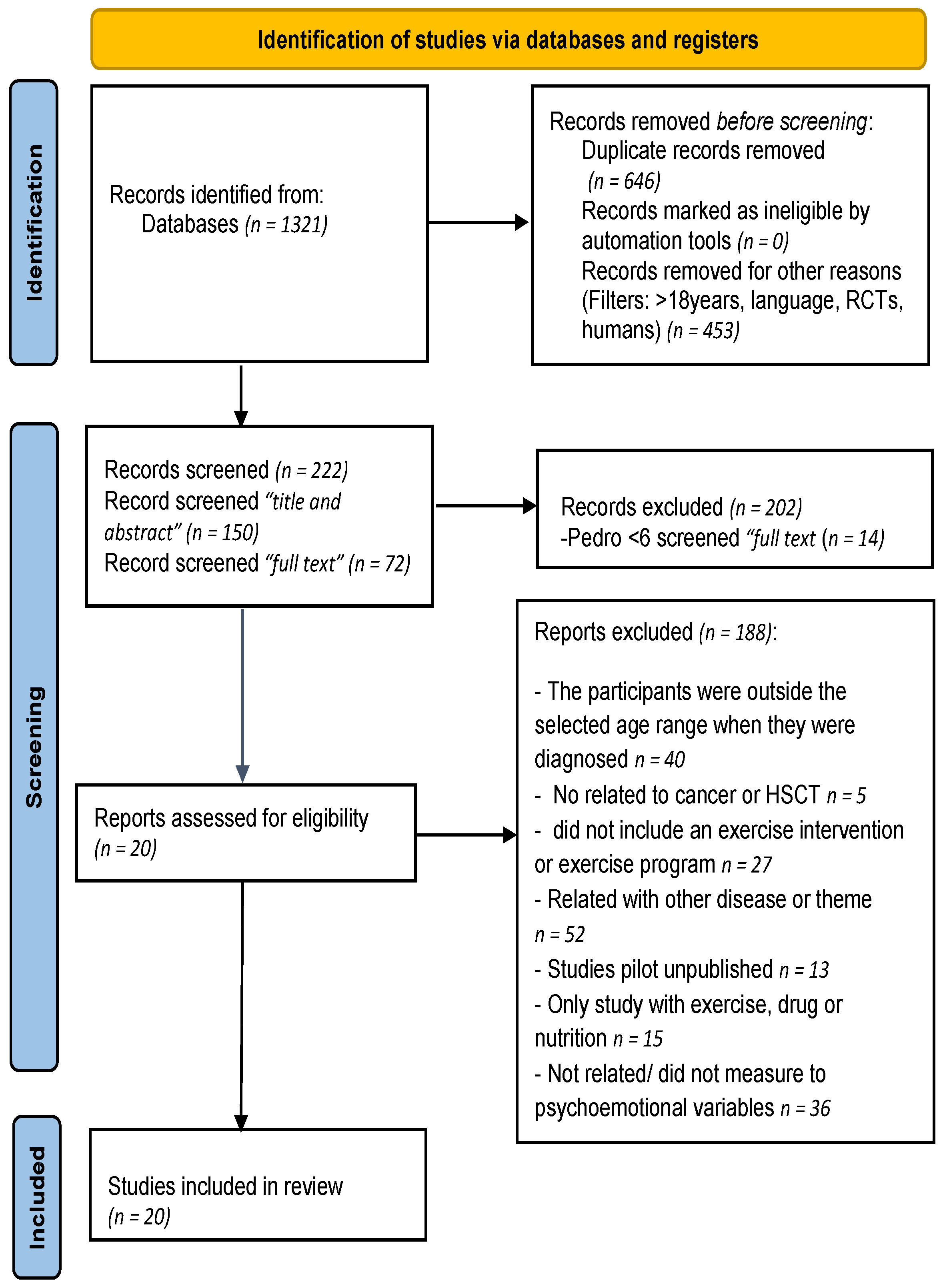
3.1. Study Selection
3.2. Study Characteristics
3.3. Quality Assessment and Publication Bias
3.4. Characteristics of Participants
3.5. Characteristics of Exercise Interventions
3.6. Compliance Rate
3.7. Endpoints and Exercise Intervention Psychoemotional Results
3.7.1. Psychoemotional Variables
3.7.2. Quality of Life Variables
4. Discussion
4.1. Psychoemotional Variables
4.2. Quality of Life Variables
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Battaglini, C.L.; Hackney, A.C.; Garcia, R.; Groff, D.; Evans, E.; Shea, T. The Effects of an Exercise Program in Leukemia Patients. Integr. Cancer Ther. 2009, 8, 130–138. [Google Scholar] [CrossRef]
- Larson, A.G.; Morris, K.J.; Juckett, M.B.; Coe, C.L.; Broman, A.T.; Costanzo, E.S. Mindfulness, Experiential Avoidance, and Recovery From Hematopoietic Stem Cell Transplantation. Ann. Behav. Med. 2019, 53, 886–895. [Google Scholar] [CrossRef]
- Weisdorf, D.; Haake, R.; Blazar, B.; Miller, W.; McGlave, P.; Ramsay, N.; Kersey, J.; Filipovich, A. Treatment of moderate/severe acute graft-versus-host disease after allogeneic bone marrow transplantation: An analysis of clinical risk features and outcome. Blood 1990, 75, 1024–1030. [Google Scholar] [CrossRef] [PubMed]
- Neitzert, C.S.; Ritvo, P.; Dancey, J.; Weiser, K.; Murray, C.; Avery, J. The psychosocial impact of bone marrow transplantation: A review of the literature. Bone Marrow Transplant. 1998, 22, 409–422. [Google Scholar] [CrossRef] [PubMed]
- Fiuza-Luces, C.; Simpson, R.J.; Ramírez, M.; Lucia, A.; Berger, N.A. Physical function and quality of life in patients with chronic GvHD: A summary of preclinical and clinical studies and a call for exercise intervention trials in patients. Bone Marrow Transplant. 2016, 51, 13–26. [Google Scholar] [CrossRef] [PubMed]
- Sun, C.L.; Francisco, L.; Kawashima, T.; Leisenring, W.; Robison, L.L.; Baker, K.S.; Weisdorf, D.J.; Forman, S.J.; Bhatia, S. Prevalence and predictors of chronic health conditions after hematopoietic cell transplantation: A report from the Bone Marrow Transplant Survivor Study. Blood 2010, 116, 3129–3139. [Google Scholar] [CrossRef] [PubMed]
- Courneya, K.S.; Keats, M.R.; Turner, A.R. Physical exercise and quality of life in cancer patients following high dose chemotherapy and autologous bone marrow transplantation. Psychooncology 2000, 9, 127–136. [Google Scholar] [CrossRef]
- Mccourt, O.; Fisher, A.; Ramdharry, G.; Roberts, A.; Land, J.; Rabin, N.; Yong, K. PERCEPT myeloma: A protocol for a pilot randomised controlled trial of exercise prehabilitation before and during autologous stem cell transplantation in patients with multiple myeloma. BMJ Open 2020, 10, e033176. [Google Scholar] [CrossRef] [PubMed]
- Tierney, D.K.; Facione, N.; Padilla, G.; Dodd, M. Response shift: A theoretical exploration of quality of life following hematopoietic cell transplantation. Cancer Nurs. 2007, 30, 125–138. [Google Scholar] [CrossRef] [PubMed]
- CURT, G.A.G.; Breitbart, W.; Cella, D.; Groopman, J.E.; Horning, S.S.J.; Itri, L.M.L.; Johnson, D.H.D.; Miaskowski, C.; Scheer, S.; Portenoy, R.K.R.; et al. Impact of Cancer-Related Fatigue on the Lives of Patients: New Findings From the Fatigue Coalition. Oncologist 2000, 5, 353–360. [Google Scholar] [CrossRef] [PubMed]
- Hacker, E.D.; Ferrans, C.; Verlen, E.; Ravandi, F.; Van Besien, K.; Gelms, J.; Dieterle, N.; Bc, F.N.P.; Ravandi, F.; Besien, K.V.; et al. Fatigue and Physical Activity in Patients Undergoing Hematopoietic Stem Cell Transplant. Oncol. Nurs. Forum 2006, 33, 614–625. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.S. Clinical Factors Associated With Cancer-Related Fatigue in Patients Being Treated for Leukemia and Non-Hodgkin’s Lymphoma. J. Clin. Oncol. 2002, 20, 1319–1328. [Google Scholar] [CrossRef]
- Courneya, K.S.; Friedenreich, C.M. Physical exercise and quality of life following cancer diagnosis: A literature review. Ann. Behav. Med. 1999, 21, 171–179. [Google Scholar] [CrossRef] [PubMed]
- Nelson, A.M.; Coe, C.L.; Juckett, M.B.; Rumble, M.E.; Rathouz, P.J.; Hematti, P.; Costanzo, E.S. Sleep quality following hematopoietic stem cell transplantation: Longitudinal trajectories and biobehavioral correlates. Bone Marrow Transplant. 2014, 49, 1405–1411. [Google Scholar] [CrossRef]
- Adler, N.E.; Page, A.E.K. Cancer Care for the Whole Patient: Meeting Psychosocial Health Needs; National Academies Press: Washington, DC, USA, 2008; ISBN 9780309111072. [Google Scholar]
- Baker, K.S.; Ness, K.K.; Weisdorf, D.; Francisco, L.; Sun, C.-L.; Forman, S.; Bhatia, S. Late effects in survivors of acute leukemia treated with hematopoietic cell transplantation: A report from the Bone Marrow Transplant Survivor Study. Leukemia 2010, 24, 2039–2047. [Google Scholar] [CrossRef] [PubMed]
- Boşnak Güçlü, M.; Barğı, G.; Sucak, G.T. Impairments in dyspnea, exercise capacity, physical activity and quality of life of allogeneic hematopoietic stem cell transplantation survivors compared with healthy individuals: A cross sectional study. Physiother. Theory Pract. 2019, 37, 52–63. [Google Scholar] [CrossRef] [PubMed]
- Eyigor, S.; Eyigor, C.; Uslu, R. Assessment of pain, fatigue, sleep and quality of life (QoL) in elderly hospitalized cancer patients. Arch. Gerontol. Geriatr. 2010, 51, e57–e61. [Google Scholar] [CrossRef]
- Kisch, A.; Jakobsson, S.; Forsberg, A. Implementing a Feasible Exercise Programme in an Allogeneic Haematopoietic Stem Cell Transplantation Setting—Impact on Physical Activity and Fatigue. Int. J. Environ. Res. Public Health 2020, 17, 4302. [Google Scholar] [CrossRef]
- Poulson, M.J. Not Just Tired. J. Clin. Oncol. 2001, 19, 4180–4181. [Google Scholar] [CrossRef]
- Park, H.Y.; Jeon, H.J.; Bang, Y.R.; Yoon, I.-Y. Multidimensional Comparison of Cancer-Related Fatigue and Chronic Fatigue Syndrome: The Role of Psychophysiological Markers. Psychiatry Investig. 2019, 16, 71–79. [Google Scholar] [CrossRef] [PubMed]
- Pitman, A.; Suleman, S.; Hyde, N.; Hodgkiss, A. Depression and anxiety in patients with cancer. BMJ 2018, 361, k1415. [Google Scholar] [CrossRef]
- Weng Hong, C.; Ajit Singh, V.; Amar Singh, A.K. Psychological disorders in patients with orthopaedic oncological diseases and their coping strategies. J. Orthop. Surg. 2022, 30, 102255362210934. [Google Scholar] [CrossRef]
- Howell, D.; Olsen, K. Distress—The 6th Vital Sign. Curr. Oncol. 2011, 18, 208–210. [Google Scholar] [CrossRef] [PubMed]
- Sun, H.; Thapa, S.; Wang, B.; Fu, X.; Yu, S. A Systematic Review and Meta-analysis of the Distress Thermometer for Screening Distress in Asian Patients with Cancer. J. Clin. Psychol. Med. Settings 2021, 28, 212–220. [Google Scholar] [CrossRef] [PubMed]
- Carlson, L.E.; Bultz, B.D. Cancer distress screening. J. Psychosom. Res. 2003, 55, 403–409. [Google Scholar] [CrossRef]
- Ghazikhanian, S.E.; Dorfman, C.S.; Somers, T.J.; O’Sullivan, M.L.; Fisher, H.M.; Edmond, S.N.; Wren, A.A.; Kelleher, S.A.; Rowe Nichols, K.A.; Chao, N.; et al. Cognitive problems following hematopoietic stem cell transplant: Relationships with sleep, depression and fatigue. Bone Marrow Transplant. 2017, 52, 279–284. [Google Scholar] [CrossRef]
- National Center for Chronic Disease Prevention and Health Promotion D of PH. HRQOL Concepts|CDC. Centers for Disease Control and Prevention. 2018. Available online: https://www.cdc.gov/hrqol/concept.htm (accessed on 8 November 2022).
- MacVicar, M.G.; Winningham, M.L.; Nickel, J.L. Effects of aerobic interval training on cancer patients functional capacity. Nurs. Res. 1989, 38, 348–351. [Google Scholar] [CrossRef]
- Dimeo, F.; Bertz, H.; Finke, J.; Fetscher, S.; Mertelsmann, R.; Keul, J. An aerobic exercise program for patients with haematological malignancies after bone marrow transplantation. Bone Marrow Transplant. 1996, 18, 1157–1160. [Google Scholar] [PubMed]
- Decker, W.; McTurner-McGlade, J.; Fehir, K.; Decker, W.A.; Turner-McGlade, J.F.K.; Decker, W.; McTurner-McGlade, J.; Fehir, K. Psychosocial aspects and the physiological effects of a cardiopulmonary exercise program in patients undergoing bone marrow transplantation (BMT) for acute leukemia (AL). Transplant. Proc. 1989, 21, 3068–3069. [Google Scholar] [PubMed]
- Mock, V.; Burke, M.B.; Sheehan, P.; Creaton, E.M.; Winningham, M.L.; McKenney-Tedder, S.; Schwager, L.P.; Liebman, M. A nursing rehabilitation program for women with breast cancer receiving adjuvant chemotherapy. Oncol. Nurs. Forum 1994, 21, 899–907; discussion 908. [Google Scholar] [CrossRef]
- Dimeo, F.C.; Tilmann, M.H.M.; Bertz, H.; Kanz, L.; Mertelsmann, R.; Keul, J. Aerobic exercise in the rehabilitation of cancer patients after high dose chemotherapy and autologous peripheral stem cell transplantation. Cancer 1997, 79, 1717–1722. [Google Scholar] [CrossRef]
- Baumann, F.T.; Kraut, L.; Schüle, K.; Bloch, W.; Fauser, A.A. A controlled randomized study examining the effects of exercise therapy on patients undergoing haematopoietic stem cell transplantation. Bone Marrow Transplant. 2010, 45, 355–362. [Google Scholar] [CrossRef]
- Hayes, S.; Davies, P.S.W.; Parker, T.; Bashford, J.; Newman, B. Quality of life changes following peripheral blood stem cell transplantation and participation in a mixed-type, moderate-intensity, exercise program. Bone Marrow Transplant. 2004, 33, 553–558. [Google Scholar] [CrossRef] [PubMed]
- Shobeiri, F.; Masoumi, S.Z.; Nikravesh, A.; Heidari Moghadam, R.; Karami, M. The Impact of Aerobic Exercise on Quality of Life in Women with Breast Cancer: A Randomized Controlled Trial. J. Res. Health Sci. 2016, 16, 127–132. [Google Scholar] [CrossRef]
- Ballard-Barbash, R.; Blair, A.; Blair, S.N.; Byers, T.; Hoffman-Goetz, L.; Lee, I.M.; Troiano, R.; Westerlind, K. Physical activity across the cancer continuum: Report of a workshop: Review of existing knowledge and innovative designs for future research. Cancer 2002, 95, 1134–1143. [Google Scholar] [CrossRef]
- Adamsen, L.; Quist, M.; Andersen, C.; Møller, T.; Herrstedt, J.; Kronborg, D.; Baadsgaard, M.T.; Vistisen, K.; Midtgaard, J.; Christiansen, B.; et al. Effect of a multimodal high intensity exercise intervention in cancer patients undergoing chemotherapy: Randomised controlled trial. BMJ 2009, 339, 895–898. [Google Scholar] [CrossRef]
- Yang, B.; Wang, J.; Yang, B.; Wang, J. Effects of Exercise on Cancer-related Fatigue and Quality of Life in Prostate Cancer Patients Undergoing Androgen Deprivation Therapy: A Meta-analysis of Randomized Clinical Trials. Chin. Med. Sci. J. 2017, 32, 13–21. [Google Scholar] [CrossRef]
- Wiskemann, J.; Dreger, P.; Schwerdtfeger, R.; Bondong, A.; Huber, G.; Kleindienst, N.; Ulrich, C.M.; Bohus, M. Effects of a partly self-administered exercise program before, during, and after allogeneic stem cell transplantation. Blood 2011, 117, 2604–2613. [Google Scholar] [CrossRef]
- Hacker, E.D.; Larson, J.; Kujath, A.; Peace, D.; Rondelli, D.; Gaston, L. Strength Training Following Hematopoietic Stem Cell Transplantation. Cancer Nurs. 2011, 34, 238–249. [Google Scholar] [CrossRef]
- Jarden, M.; Nelausen, K.; Hovgaard, D.; Boesen, E.; Adamsen, L. The Effect of a Multimodal Intervention on Treatment-Related Symptoms in Patients Undergoing Hematopoietic Stem Cell Transplantation: A Randomized Controlled Trial. J. Pain Symptom Manag. 2009, 38, 174–190. [Google Scholar] [CrossRef]
- Oechsle, K.; Aslan, Z.; Suesse, Y.; Jensen, W.; Bokemeyer, C.; de Wit, M. Multimodal exercise training during myeloablative chemotherapy: A prospective randomized pilot trial. Support. Care Cancer 2014, 22, 63–69. [Google Scholar] [CrossRef]
- Prins, M.C.; van Hinte, G.; Koenders, N.; Rondel, A.L.; Blijlevens, N.M.A.; van den Berg, M.G.A. The effect of exercise and nutrition interventions on physical functioning in patients undergoing haematopoietic stem cell transplantation: A systematic review and meta-analysis. Support. Care Cancer 2021, 29, 7111–7126. [Google Scholar] [CrossRef] [PubMed]
- Abo, S.; Denehy, L.; Ritchie, D.; Lin, K.-Y.; Edbrooke, L.; McDonald, C.; Granger, C.L. People With Hematological Malignancies Treated With Bone Marrow Transplantation Have Improved Function, Quality of Life, and Fatigue Following Exercise Intervention: A Systematic Review and Meta-Analysis. Phys. Ther. 2021, 101, pzab130. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, T.P. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Nelson, N.L. Breast Cancer–Related Lymphedema and Resistance Exercise: A Systematic Review. J. Strength Cond. Res. 2016, 30, 2656–2665. [Google Scholar] [CrossRef]
- Juvet, L.K.; Thune, I.; Elvsaas, I.K.Ø.; Fors, E.A.; Lundgren, S.; Bertheussen, G.; Leivseth, G.; Oldervoll, L.M. The effect of exercise on fatigue and physical functioning in breast cancer patients during and after treatment and at 6 months follow-up: A meta-analysis. Breast 2017, 33, 166–177. [Google Scholar] [CrossRef]
- Hidalgo, B.; Hall, T.; Bossert, J.; Dugeny, A.; Cagnie, B.; Pitance, L. The efficacy of manual therapy and exercise for treating non-specific neck pain: A systematic review. J. Back Musculoskelet. Rehabil. 2018, 30, 1149–1169. [Google Scholar] [CrossRef]
- Morales-Rodriguez, E.; Pérez-Bilbao, T.; San Juan, A.F.; Calvo, J.L. Effects of Exercise Programs on Physical Factors and Safety in Adult Patients with Cancer and Haematopoietic Stem Cell Transplantation: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 1288. [Google Scholar] [CrossRef]
- Morales, J.S.; Valenzuela, P.L.; Herrera-Olivares, A.M.; Baño-Rodrigo, A.; Castillo-García, A.; Rincón-Castanedo, C.; Martín-Ruiz, A.; San-Juan, A.F.; Fiuza-Luces, C.; Lucia, A. Exercise Interventions and Cardiovascular Health in Childhood Cancer: A Meta-analysis. Int. J. Sports Med. 2020, 41, 141–153. [Google Scholar] [CrossRef]
- Elkins, M.R.; Moseley, A.M.; Sherrington, C.; Herbert, R.D.; Maher, C.G. Growth in the Physiotherapy Evidence Database (PEDro) and use of the PEDro scale. Br. J. Sports Med. 2013, 47, 188–189. [Google Scholar] [CrossRef]
- Knols, R.H.; de Bruin, E.D.; Uebelhart, D.; Aufdemkampe, G.; Schanz, U.; Stenner-Liewen, F.; Hitz, F.; Taverna, C.; Aaronson, N.K. Effects of an outpatient physical exercise program on hematopoietic stem-cell transplantation recipients: A randomized clinical trial. Bone Marrow Transplant. 2011, 46, 1245–1255. [Google Scholar] [CrossRef]
- Persoon, S.; ChinAPaw, M.J.M.; Buffart, L.M.; Liu, R.D.K.; Wijermans, P.; Koene, H.R.; Minnema, M.C.; Lugtenburg, P.J.; Marijt, E.W.A.; Brug, J.; et al. Randomized controlled trial on the effects of a supervised high intensity exercise program in patients with a hematologic malignancy treated with autologous stem cell transplantation: Results from the EXIST study. PLoS ONE 2017, 12, e0181313. [Google Scholar] [CrossRef] [PubMed]
- Barğı, G.; Güçlü, M.B.; Arıbaş, Z.; Akı, Ş.Z.; Sucak, G.T. Inspiratory muscle training in allogeneic hematopoietic stem cell transplantation recipients: A randomized controlled trial. Support. Care Cancer 2016, 24, 647–659. [Google Scholar] [CrossRef]
- Hacker, E.D.; Richards, R.L.; Abu Zaid, M.; Chung, S.-Y.; Perkins, S.; Farag, S.S. STEPS to Enhance Physical Activity After Hematopoietic Cell Transplantation for Multiple Myeloma. Cancer Nurs. 2022, 45, 211–223. [Google Scholar] [CrossRef]
- Pahl, A.; Wehrle, A.; Kneis, S.; Gollhofer, A.; Bertz, H. Whole body vibration training during allogeneic hematopoietic cell transplantation—The effects on patients’ physical capacity. Ann. Hematol. 2020, 99, 635–648. [Google Scholar] [CrossRef]
- Schumacher, H.; Stüwe, S.; Kropp, P.; Diedrich, D.; Freitag, S.; Greger, N.; Junghanss, C.; Freund, M.; Hilgendorf, I. A prospective, randomized evaluation of the feasibility of exergaming on patients undergoing hematopoietic stem cell transplantation. Bone Marrow Transplant. 2018, 53, 584–590. [Google Scholar] [CrossRef]
- Wiskemann, J.; Kuehl, R.; Dreger, P.; Schwerdtfeger, R.; Huber, G.; Ulrich, C.M.; Jaeger, D.; Bohus, M. Efficacy of exercise training in SCT patients-who benefits most? Bone Marrow Transplant. 2014, 49, 443–448. [Google Scholar] [CrossRef]
- Bird, L.; Arthur, A.; Niblock, T.; Stone, R.; Watson, L.; Cox, K. Rehabilitation programme after stem cell transplantation: Randomized controlled trial. J. Adv. Nurs. 2010, 66, 607–615. [Google Scholar] [CrossRef]
- Van Dongen, J.M.; Persoon, S.; Jongeneel, G.; Bosmans, J.E.; Kersten, M.J.; Brug, J.; Nollet, F.; Chinapaw, M.J.M.; Buffart, L.M. Long-term effectiveness and cost-effectiveness of an 18-week supervised exercise program in patients treated with autologous stem cell transplantation: Results from the EXIST study. J. Cancer Surviv. 2019, 13, 558–569. [Google Scholar] [CrossRef]
- Shelton, M.L.; Lee, J.Q.; Morris, G.S.; Massey, P.R.; Kendall, D.G.; Munsell, M.F.; Anderson, K.O.; Simmonds, M.J.; Giralt, S.A. A randomized control trial of a supervised versus a self-directed exercise program for allogeneic stem cell transplant patients. Psychooncology 2009, 18, 353–359. [Google Scholar] [CrossRef]
- Baumann, F.; Zopf, E.M.; Nykamp, E.; Kraut, L.; Schüle, K.; Elter, T.; Fauser, A.; Bloch, W. Physical activity for patients undergoing an allogeneic hematopoietic stem cell transplantation: Benefits of a moderate exercise intervention. Eur. J. Haematol. 2011, 87, 148–156. [Google Scholar] [CrossRef] [PubMed]
- Coleman, E.A.; Coon, S.; Hall-Barrow, J.; Richards, K.; Gaylor, D.; Stewart, B. Feasibility of Exercise During Treatment for Multiple Myeloma. Cancer Nurs. 2003, 26, 410–419. [Google Scholar] [CrossRef]
- Jarden, M.; Baadsgaard, M.; Hovgaard, D.; Boesen, E.; Adamsen, L. A randomized trial on the effect of a multimodal intervention on physical capacity, functional performance and quality of life in adult patients undergoing allogeneic SCT. Bone Marrow Transplant. 2009, 43, 725–737. [Google Scholar] [CrossRef] [PubMed]
- Potiaumpai, M.; Cutrono, S.; Medina, T.; Koeppel, M.; Pereira, D.L.; Pirl, W.F.; Jacobs, K.A.; Eltoukhy, M.; Signorile, J.F. Multidirectional Walking in Hematopoietic Stem Cell Transplant Patients. Med. Sci. Sports Exerc. 2021, 53, 258–266. [Google Scholar] [CrossRef]
- DeFor, T.E.; Burns, L.J.; Gold, E.A.; Weisdorf, D.J. A Randomized Trial of the Effect of a Walking Regimen on the Functional Status of 100 Adult Allogeneic Donor Hematopoietic Cell Transplant Patients. Biol. Blood Marrow Transplant. 2007, 13, 948–955. [Google Scholar] [CrossRef] [PubMed]
- Hacker, E.D.; Larson, J.L.; Peace, D. Exercise in patients receiving hematopoietic stem cell transplantation: Lessons learned and results from a feasibility study. Oncol. Nurs. Forum 2011, 38, 216–223. [Google Scholar] [CrossRef]
- Xu, W.; Yang, L.; Wang, Y.; Wu, X.; Wu, Y.; Hu, R. Effects of exercise interventions for physical fitness, fatigue, and quality of life in adult hematologic malignancy patients without receiving hematopoietic stem cell transplantation: A systematic review and meta-analysis. Support. Care Cancer 2022, 30, 7099–7118. [Google Scholar] [CrossRef]
- Smets, E.M.A.; Garssen, B.; Bonke, B.; De Haes, J.C.J.M. The multidimensional Fatigue Inventory (MFI) psychometric qualities of an instrument to assess fatigue. J. Psychosom. Res. 1995, 39, 315–325. [Google Scholar] [CrossRef]
- Terry, P.; Lane, A.; Fogarty, G. Construct validity of the Profile of Mood States—Adolescents for use with adults. Psychol. Sport Exerc. 2003, 4, 125–139. [Google Scholar] [CrossRef]
- Blackburn, R.; Presson, K.; Laufman, R.; Tomczak, N.; Brassil, K. Establishing an Inpatient Gym for Recipients of Stem Cell Transplantation: A Multidisciplinary Collaborative. Clin. J. Oncol. Nurs. 2016, 20, 66–71. [Google Scholar] [CrossRef]
- Abo, S.; Ritchie, D.; Denehy, L.; Panek-Hudson, Y.; Irving, L.; Granger, C.L. Feasibility of early-commencing group-based exercise in allogeneic bone marrow transplantation: The BOOST study. Bone Marrow Transplant. 2021, 56, 2788–2796. [Google Scholar] [CrossRef] [PubMed]
- Dimeo, F.C. Effects of exercise on cancer-related fatigue. Cancer 2001, 92, 1689–1693. [Google Scholar] [CrossRef]
- Hacker, E.D.; Mjukian, M. Review of attrition and adherence in exercise studies following hematopoietic stem cell transplantation. Eur. J. Oncol. Nurs. 2014, 18, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Garratt, A.; Schmidt, L.; Mackintosh, A.; Fitzpatrick, R. Quality of life measurement: Bibliographic study of patient assessed health outcome measures. BMJ 2002, 324, 1417. [Google Scholar] [CrossRef] [PubMed]
- Cankurtaran, E.S.; Ozalp, E.; Soygur, H.; Ozer, S.; Akbiyik, D.I.; Bottomley, A. Understanding the reliability and validity of the EORTC QLQ-C30 in Turkish cancer patients. Eur. J. Cancer Care 2007, 17, 98–104. [Google Scholar] [CrossRef]
- Rivera-Fong, L.; Benjet, C.; Robles García, R.; Traeger, L.; Aguilar Ponce, J.L.; Valero Saldaña, L.M.; Acosta Maldonado, B.L.; Rivas Vera, S.; Galindo Vázquez, O.; Riveros Rosas, A. Patients’ quality of life: Validation of the functional assessment of cancer therapy-bone marrow transplant (FACT-BMT) instrument for the Mexican population. Palliat. Support. Care 2020, 18, 557–568. [Google Scholar] [CrossRef]
- Persoon, S.; Kersten, M.J.; van der Weiden, K.; Buffart, L.M.; Nollet, F.; Brug, J.; Chinapaw, M.J.M. Effects of exercise in patients treated with stem cell transplantation for a hematologic malignancy: A systematic review and meta-analysis. Cancer Treat. Rev. 2013, 39, 682–690. [Google Scholar] [CrossRef] [PubMed]
- Van Haren, I.E.P.M.; Timmerman, H.; Potting, C.M.; Blijlevens, N.M.A.; Staal, J.B.; Nijhuis-van der Sanden, M.W.G. Physical exercise for patients undergoing hematopoietic stem cell transplantation: Systematic review and meta-analyses of randomized controlled trials. Phys. Ther. 2013, 93, 514–528. [Google Scholar] [CrossRef]
- Ramírez-Vélez, R.; Zambom-Ferraresi, F.; García-Hermoso, A.; Kievisiene, J.; Rauckiene-Michealsson, A.; Agostinis-Sobrinho, C. Evidence-Based Exercise Recommendations to Improve Mental Wellbeing in Women with Breast Cancer during Active Treatment: A Systematic Review and Meta-Analysis. Cancers 2021, 13, 264. [Google Scholar] [CrossRef]
- Wood, W.A.; Weaver, M.; Smith-Ryan, A.E.; Hanson, E.D.; Shea, T.C.; Battaglini, C.L. Lessons learned from a pilot randomized clinical trial of home-based exercise prescription before allogeneic hematopoietic cell transplantation. Support. Care Cancer 2020, 28, 5291–5298. [Google Scholar] [CrossRef]
- Huang, F.F.; Yang, Q.; Wang, A.N.; Zhang, J.P. Psychometric properties and performance of existing self-efficacy instruments in cancer populations: A systematic review. Health Qual. Life Outcomes 2018, 16, 241. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Items | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Study | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | Total Score |
| (Knols et al., 2011) [53] | + | + | + | + | + | − | + | + | + | + | + | 10 |
| (Persoon et al., 2017) [54] | + | + | + | + | + | + | + | + | + | + | + | 10 |
| (Barğı et al., 2016) [55] | + | + | + | + | + | + | − | + | + | + | + | 9 |
| (Hacker et al., 2022) [56] | + | + | + | + | + | − | − | + | + | + | + | 8 |
| (Pahl et al., 2020) [57] | + | + | + | + | + | − | − | + | + | + | + | 8 |
| (Jarden et al., 2009) [42] | + | + | + | + | + | − | − | + | + | + | + | 8 |
| (Schumacher et al., 2018) [58] | + | + | + | + | + | ? | ? | + | + | + | + | 8 |
| (Wiskemann et al., 2014) [59] | + | + | + | + | + | − | − | + | + | + | + | 8 |
| (Bird et al., 2010) [60] | + | + | + | + | − | − | − | + | + | + | + | 7 |
| (Van Dongen et al., 2019) [61] | + | + | + | + | − | − | − | + | + | + | + | 7 |
| (Baumann et al., 2010) [34] | + | + | + | + | − | − | − | + | + | + | + | 7 |
| (Wiskemann et al., 2011) [40] | + | + | + | + | ? | ? | ? | + | + | + | + | 7 |
| (Hacker et al., 2011) [41] | + | + | + | + | ? | ? | ? | + | + | + | + | 7 |
| (Shelton et al., 2009) [62] | + | + | + | + | − | − | − | + | + | + | + | 7 |
| (Baumann et al., 2011) [63] | + | + | + | + | − | − | − | + | + | + | + | 7 |
| (Coleman et al., 2003) [64] | + | + | + | + | ? | ? | ? | + | + | + | + | 7 |
| (Jarden et al., 2009) [65] | + | + | + | + | − | − | − | + | + | + | + | 7 |
| (Potiaumpai et al., 2021) [66] | + | + | + | + | − | − | − | + | + | + | + | 7 |
| (Oechsle et al., 2014) [43] | + | + | − | + | − | − | − | + | + | + | + | 6 |
| (Defor et al., 2007) [67] | + | + | + | ? | ? | ? | ? | + | + | + | + | 6 |
| Study | Study Design | Sample Size by Group (Sex), Age (Mean ± SD; Range), Sample Size | Primary Cancer | Intervention | Main Results in Psychoemotional Variables. Tests/Scales | Main Results in QoL Variables. Tests/Scales |
|---|---|---|---|---|---|---|
| (Hacker et al., 2022) [56] | RCT T1: Pre HSCT (A) T2: Post HSCT (7 weeks D) PEDro score 8 | EXP: n = 17 (8 female), 62.21 ± 8.50 b years CT: n = 15 (3 female), 63.44 ± 6.30 b years | MM | Type: AT, ST Duration: 6 weeks Intensity and volume: AT 7 days a week (increase steps by 10% weekly), ST 5 Ib (female) 8 Ib (male) Supervised: Yes Setting: Home/hospital | T1-T2:
| T1-T2:
|
| (Pahl et al., 2020) [57] | RCT T1: Pre HSCT (A) T2: Post HSCT (D) T3: PostHSCT (180 days D) PEDro score 8 | EXP: n = 18 (7 female), 55 years (50–63) CT: n = 26 (7 female), 56 years (32–63) | ALL, AML, CLL, CML, lymphoma, MDS, MF, MM, SAA, septic granulomatosis | Type: AT, ST with vibration (EXP), mobilization of the spine and stretching (CT) Duration: N/R Intensity: N/R Volume: AT/WBV/ST (EXP) 5 days a week (20 min), mobilization and stretching (CT) 5 days a week (20 min) Supervised: Yes Setting: Hospital | T2-T3: -MFI: ↓EXP/↑CT | T1-T3: -QLQ-C30:
-QLQ-C30:
|
| (Jarden et al., 2009) [42] | RCT T1: Pre HSCT (A) T2: Post HSCT (6 weeks) PEDro score 8 | EXP: n = 21 (8 female), 40.9 years (18–60) CT: n = 21 (8 female), 37.4 years (18–55) | AA, ALL, AML, CML, MDS, MF, PNH, WM | Type: AT, ST, stretching, relaxation Duration: 4–6 weeks Intensity and volume: AT 5 days a week (HRmax 50–75% low to moderate RPE 10/13), stretching (dynamic: 1–2 sets of 10–12 reps; static: 1 set/15–30 seg), ST 3 days a week (1–2 sets of 10–12 reps at low to moderate, RPE 10/13) and relaxation twice a week (low RPE 6/9) Cadence: 30–70 cycles/min and range at 30–75 W Supervised: Yes Setting: Hospital | T1-T2: -HADS: =EXP/=CT | T1-T2: -FACT-BMT: =EXP/=CT -KPS: =EXP/=CT -QLQ-C30: =EXP/=CT |
| (Wiskemann et al., 2014) [59] | Multicenter RCT T1: Pre HSCT (baseline)—pre HSCT (A) T2: Pre HSCT (A)–post HSCT (D) T3: Post HSCT (D)–post HSCT (6–8 weeks) PEDro score 8 | EXP: n = 52 (21 female), 47.6 years (18–70) CT: n = 53 (13 female), 50 years (20–71) | AA, ALL, AML, CLL, CML, Lymphoma, MDS, MM | Type: AT, ST Duration: 8 weeks Frequency: AT: T1 (3 days a week), T2 (5 days a week), T3 (3 days a week). ST: T1, T2, and T3 (twice a week). Intensity and volume: Not specified Supervised: Yes Setting: Home/hospital | T1-T3: -MFI: =EXP/=CT -DT: =EXP/=CT | T1-T3: -QLQ-C30: =EXP/=CT |
| (Baumann et al., 2010) [34] | RCT T1: Pre HSCT (A) T2: Post HSCT (D) PEDro score 7 | EXP: n = 32 (11 female), 44.9 ± 12.4 b years CT: n = 32 (18 female), 44.1 ± 14.2 b years | ALL, AML, CLL, CML, LHN, MDS, MM, Solid tumor, immuno-deficiency | Type: AT, ADL Duration: 7 weeks Volume: AT twice a week (80% HRmax), ADL 5 days a week (5 × 20 steps with 1 min break RPE “slightly strenuous” to ‘strenuous’. CT 5 days a week Cadence: AT (increase 25 W/2 min) Supervised: Yes Setting: Hospital | -No measurement | T1-T2: -QLQ-C30:
|
| (Wiskemann et al., 2011) [40] | RCT T1: Pre HSCT (medical checkup)—pre HSCT (4 week A) T2: Post HSCT (H)—post HSCT (D) T3: Post HSCT (D)—post HSCT (D 6–8 weeks) PEDro score 7 | EXP: n = 52 (21 female), 47.6 years (18–70) CT: n = 53 (13 female), 50 years (20–71) | AA, ALL, AML, CLL, CML, MDS, MM, MPS, Others | Type: AT, ST Duration: 18 weeks Intensity and volume: AT 1–4 week to (A) 3 days a week, from (H) 3–5 days a week RPE (12–14/20), DCT: color codes (red 15–20 min, yellow 20–30 min, green 30–40 min), from 1–8 week rehabilitation 3 days a week. ST 1–4 week to (A) twice a week, from (H) twice a week (2–3 sets of 8–20 reps RPE 14–16/20), from 1–8 week rehabilitation twice a week. Supervised: Yes T2 and self-directed T1 and T3 Setting: Home/hospital | T2: -MFI: GF (↑EXP), Pf (↑EXP) -POMS: Fatigue (↓EXP), Anger/hostility (↓EXP) T3: -MFI: GF (↓CT), Pf (↓CT), -HADS: Anxiety (↑EXP) -POMS: Depression (↓EXP), fatigue (↑CT), anger/hostility (↑CT) | T3: -QLQ-C30: PF (↓EXP), pain (↑EXP) |
| (Baumann et al., 2011) [63] | RCT T1: Pre HSCT(A) T2: Post HSCT(7–8 weeks) PEDro score 7 | EXP: n = 17 (6 female), 41.41 ± 11.78 b years CT: n = 16 (11 female), 42.81 ± 14.04 b years | ALL, AML, CLL, CML, MDS, MM, MPS, PID | Type: AT, ADL, stretching, coordination Duration: 7–8 weeks Volume and intensity: AT (H) once–twice a week (10–20 min/day uninterrupted or interval training at HRmax 80%); ADL-training (H) 5 days a day (20 min at day, 5 × 20 steps with 1 min break of slightly strenuous or strenuous); mobilization until 1 day before discharge daily except on weekend low intensity; or not strenuous (CT) 20 min at day Cadence: AT cycle (since 25 W with 25 W increment every 2 min) Supervised: Yes Setting: Hospital | -No measurement | T1-T2: -QLQ-C30: Fatigue (↑CT); PF (↓EXP/↓CT); emotional state (↑EXP) |
| (Coleman et al., 2003) [64] | RCT with RM T1:Pre HSCT (A) T2: Post HSCT (3 months) PEDro score 7 | EXP: n = 14 CT: n = 10 (10 female), 55 years (42–74) | MM | Type: AT, ST Duration: 6 months Intensity and volume: AT 3 days a week CT (18 min fast paced walking at RPE 12–15/20), ST 3 days a week with color bands (1 set of 8 red 9–15 Ib, 1 set of 8 green 5–9 Ib) and (2 sets of 8 chair stands of 1 RM) Supervised: Not Setting: Home | T1-T2: -POMS: ↓EXP/↓CT; fatigue: ↓EXP | |
| (Jarden et al., 2009) [65] | RCT T1: Pre HSCT (A) T2: PostHSCT (D) PEDro score 7 | EXP: n = 21 (8 female), 45.0 years (18–60) CT: n = 21 (8 female), 38.0 years (18–55) | AA, ALL, AML, CML, MDS, MF, PNH, WM | Type: AT, ST, stretching, relaxation Duration: 4–6 weeks Intensity and volume: AT 5 days a week low to moderate (HRmax 50–75% of RPE 10/13), stretching (dynamic: 1–2 sets of 10–12 reps; static: 1 set/15–30 sg), ST 3 days a week low to moderate (1–2 sets of 10–12 reps at RPE 10/13) and relaxation twice a week (Low RPE 6/9) Cadence: 30–70 cycles/min and range of 30–75 W Volume: ST, stretching, and relaxation (dynamic: (1–2 sets of 10–12 reps); static: (1 set 15–30 sg)) Supervised: Yes Setting: Hospital | T1–T2: -No measurement. | T1–T2: - FACT-BMT: = EXP/ = CT - KPS: = EXP/ = CT - QLQ-C30: = EXP/ = CT |
| (Potiaumpai et al., 2021) [66] | RCT T1: Pre HSCT (1–3 days A) T2: Pre HSCT (3–5 days D) T3: Post HSCT (30 days D) PEDro score 7 | EXP: n = 19 (8 female), 59.3 ± 7.9 b years CT: n = 16 (11 female), 58.2 ± 7.4 b years | ALL, AML, CLL, MDS, MM, Others | Type: AT Duration: 30 days Intensity and volume: AT 3 days a week (5–30 min at RPE 7–8/13) Supervised: Yes Setting: Hospital | - No measurement | T2-T3 - QOLS: ↑ EXP - FACT-BMT: ↑ EXP |
| (DeFor et al., 2007) [67] | RCT T1: Pre HSCT (A) T2: Post HSCT (100 days) PEDro score 6 | EXP: n = 51 (22 female), 46 years (18–68) CT: n = 49 (17 female), 49 years (22–64) | AA, ALL, AML, CML, HL, LHN, MDS | Type: AT Duration: 100 days Intensity: Comfortable speed Supervised: Not Frequency: 7 days/week Setting: Clinic/home | T1–T2: - Emotional Score: ↑ EXP/↓ CT | T1-T2: - KPS: ↑ EXP |
| Study | Study Design | Sample Size by Group (Sex), Age (Mean ± SD; Range) | Primary Cancer | Intervention | Main Results in Psychoemotional Variables | Main Results in QoL Variables |
|---|---|---|---|---|---|---|
| (Knols et al., 2011) [53] | RCT T1: Pre HSCT (A)—post HSCT (D) T2: Post HSCT (D)—post HSCT (3 months) PEDro score 10 | EXP: n = 64 (26 female), 46.7 ± 13.7 years (18–75) a CT: n = 67 (28 female), 46.6 ± 12 years (20–67) a Sample Size: d = 0.5 | ALL, AML, amyloidosis, CLL, HL, LHN, lymphoma, MM, osteomyelofibrosis, testicular cancer | Type: AT, ST Frequency: 2 days/week Duration: 12 weeks Intensity and volume: AT twice a time (50–70% to 80% HRmax) Supervised: Yes Setting: Fitness center/physiotherapy practice | -No measurement | T1-T2: -HRQOL: Emotional function: ↑EXP/↑CT |
| (Persoon et al., 2017) [54] | RCT T1: Post HSCT (A) T2: Post HSCT (18 weeks) PEDro score 10 | EXP: n = 54 (22 female), 53.5 years (20–67) CT: n = 55 (18 female), 56 years (19–67) | HL, MM | Type: AT, ST Duration: 18 weeks Intensity and volume: AT 1–8 weeks twice a week (blocks of 30 sg at 65% MSEC alternated with blocks of 60 s at 30% MSEC), from 9 to 18 weeks (blocks of 30 s at 65% MSEC alternated with blocks of 30 sg at 30% MSEC), ST 1–12 weeks twice a week (2 sets/10 reps 60–80% 1 RM, from 13–18 weeks once a week (1 set/20 reps 35–40% 1 RM). Supervised: Yes Setting: Local physiotherapy | T1–T2: -No changes | T1–T2: -No changes |
| (Bargi et al., 2016) [55] | RCT T1: Pre HSCT (A) T2: Post HSCT (6 weeks) PEDro score 9 | EXP: n = 20 (8 female), 34.10 ± 12.65 a years CT: n = 18, (6 female), 39.11 ± 12.57 a years | AA, ALL, AML, CML, Fanconi anemia, MDS, MM, LHN, PNH | Type: AT and respiratory muscle Duration: 6 weeks Volume and intensity: AT: 7 days a week (speed progressively increased at 1 min intervals walking at 12 stages/30 min rest between 2 test with FIS (1–4). Diaphragmatic breaths: 7 days a week (EXP) (15 sg/25–30 breaths/5–10 resting IMT at 40% of MIP), (CT) (received sham IMT at fixed workload, 5% of baseline MIP with MMRC (0–4)) Supervised: Yes Setting: Hospital/home | T1–T2: -FIS: ↓EXP (Effect size: d = −0.27) -MADRS: ↓EXP | T1–T2: -QLQ-C30:
|
| (Schumacher et al., 2018) [58] | RCT T1: Pre HSCT (A)—post HSCT (14 days) T2: Pre HSCT (A)—post HSCT (100 days) PEDro score 8 | EXP: n = 19 (3 female), 56 years (21–65) b CT: n = 23 (14 female), 56.5 years (23–69) b | AML, CLL, CML, LHN, MDS, MM, teratoma | Type: AT, ST, stretching, Wii sports, Wii fit program, Wii balance Duration: 100 days Intensity: N/R Frequency: 5 days/week Supervised: Yes Setting: Hospital | T1–T2: -SF36: Vitality: ↑EXP -HADS: ↓EXP/↓CT -Distress thermometer: ↑EXP | T1–T2: -FACT-BMT:
|
| (Bird et al., 2010) [60] | RCT T1: Post HSCT (A) T2: Post HSCT(6 months) PEDro score 7 | EXP: n = 29 (13 female), 57 years (44–53.5) CT: n = 29 (7 female), 52 years (42.5–63) | Leukemia, lymphoma, myeloma | Type: AT, relaxation Duration: 10 weeks Intensity and volume: AT (EXP) 1–10 week (a series of circuit training exercises), relaxation (guided imagery). AT (CT) 1–10 weeks 3 days a week (home-based exercise program) Supervised: Yes Setting: Hospital/home | T1–T2: -SF36: =EXP/=CT | T1–T2: -QoL: =EXP/=CT - GHQ-12: =EXP/=CT |
| (Van Dongen et al., 2019) [61] | Multicenter RCT T1: Post HSCT (baseline) T2: Post HSCT (after exercise or similar time point in the CT) T3: Post HSCT (12 months later) PEDro score 7 | EXP: n = 54 (22 female), 52 ± 11 b years CT: n = 55 (2 female), 53 ± 12 b years | HL, MM | Type: AT, ST Duration: 18 weeks Intensity and volume: AT 1–8 weeks twice a week (2 × 8 min, alternating 30 sg at 65% and 60 sg at 30% MSEC), 9–12 weeks twice a week (2 × 8 min, alternating 30 sg at 65% and 30 sg at 30% MSEC), 13–18 weeks once a week (2 × 8 min, alternating 30 s at 65% and 30 sg at 30% MSEC), ST: 1–12 weeks twice a week (2 sets of 10 reps at 65–80% of 1-RM), 13–18 week once a week (2 sets of 20 reps at 35–40% of 1-RM) Supervised: Yes Setting: Hospital | T1–T3: -MFI: =EXP/=CT | T1–T3: -HRQoL: =EXP/=CT |
| (Hacker et al., 2011) [41] | RCT T1: Pre HSCT—post-HSCT (after 8 days) T2: H-post HSCT (1–6 weeks) PEDro score 7 | EXP: n = 9 CT: n = 10 (5 female), 46.26 years (16.23) b | AML, lymphoma | Type: ST Duration: 6 weeks Volume and intensity: ST 1–6 week 3 days a week (1–2 sets of 8–10 reps of RPE (13/20) Supervised: Yes Setting: Hospital/home | T2: -No measurement | T2: -QLQ-C30: =EXP/=CT -QLI: =EXP/=CT |
| (Shelton et al., 2009) [62] | RCT T1: Pre HSCT (A) T2: Post HSCT (4 weeks) PEDro score 7 | Supervised: n = 26 (9 female), 43.65 ±13.18 a years Self-directed: n = 27 (11 female), 48,93 ± 11.66 a years | ALL, AML, CLL, CML, HD, LHN | Type: AT, ST Duration: 4 weeks Volume and intensity: AT: 3 days a week (20– 30 min 60–75% HR max and BFI: 0–10), ST: 3 days a week EXP supervised (1–3 sets of 10 reps), EXP self-directed (1–3 sets of 10–15 reps). The AT and ST increased every third visit, if extreme fatigue, resistance was reduced to the previous level. Supervised: Yes Setting: Hospital/home | T1–T2: -BFI: =EXP/=CT | -No measurement |
| (Oechsle et al., 2014) [43] | RCT T1: Post HSCT (A) T2: Post HSCT (after intervention) PEDro score 6 | EXP: n = 17 (7 female), years 51.7 ± 13.3 b CT: n = 17 (7 female), years 52.9 ± 15.4 b | AML, LHN, MM, germ cell tumor | Type: AT, ST Duration: 21 days Intensity and volume: AT 5 days a week (10–20 min), ST 5 days a week (20 min, 2 sets of 16–25 reps at 40–60% of 1 RM) Rest: AT (regular pauses until recuperated to 66.6%) Supervised: Yes Setting: Hospital | T1–T2: - MFI:
| T1–T2: -QLQ-C30:
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morales Rodríguez, E.; Lorenzo Calvo, J.; Granado-Peinado, M.; Pérez-Bilbao, T.; San Juan, A.F. Effects of Exercise Programs on Psychoemotional and Quality-of-Life Factors in Adult Patients with Cancer and Hematopoietic Stem Cell Transplantation or Bone Marrow Transplantation: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 15896. https://doi.org/10.3390/ijerph192315896
Morales Rodríguez E, Lorenzo Calvo J, Granado-Peinado M, Pérez-Bilbao T, San Juan AF. Effects of Exercise Programs on Psychoemotional and Quality-of-Life Factors in Adult Patients with Cancer and Hematopoietic Stem Cell Transplantation or Bone Marrow Transplantation: A Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(23):15896. https://doi.org/10.3390/ijerph192315896
Chicago/Turabian StyleMorales Rodríguez, Erica, Jorge Lorenzo Calvo, Miriam Granado-Peinado, Txomin Pérez-Bilbao, and Alejandro F. San Juan. 2022. "Effects of Exercise Programs on Psychoemotional and Quality-of-Life Factors in Adult Patients with Cancer and Hematopoietic Stem Cell Transplantation or Bone Marrow Transplantation: A Systematic Review" International Journal of Environmental Research and Public Health 19, no. 23: 15896. https://doi.org/10.3390/ijerph192315896
APA StyleMorales Rodríguez, E., Lorenzo Calvo, J., Granado-Peinado, M., Pérez-Bilbao, T., & San Juan, A. F. (2022). Effects of Exercise Programs on Psychoemotional and Quality-of-Life Factors in Adult Patients with Cancer and Hematopoietic Stem Cell Transplantation or Bone Marrow Transplantation: A Systematic Review. International Journal of Environmental Research and Public Health, 19(23), 15896. https://doi.org/10.3390/ijerph192315896