

The Prevalence of Ocular Extra-Intestinal Manifestations in Adults Inflammatory Bowel Disease: A Systematic Review and Meta-Analysis

 ,
,  ,
,
Abstract
1. Introduction
2. Methods
2.1. Literature Search
2.2. Study Selection and Data Extraction
2.3. Statistical Analysis
3. Results
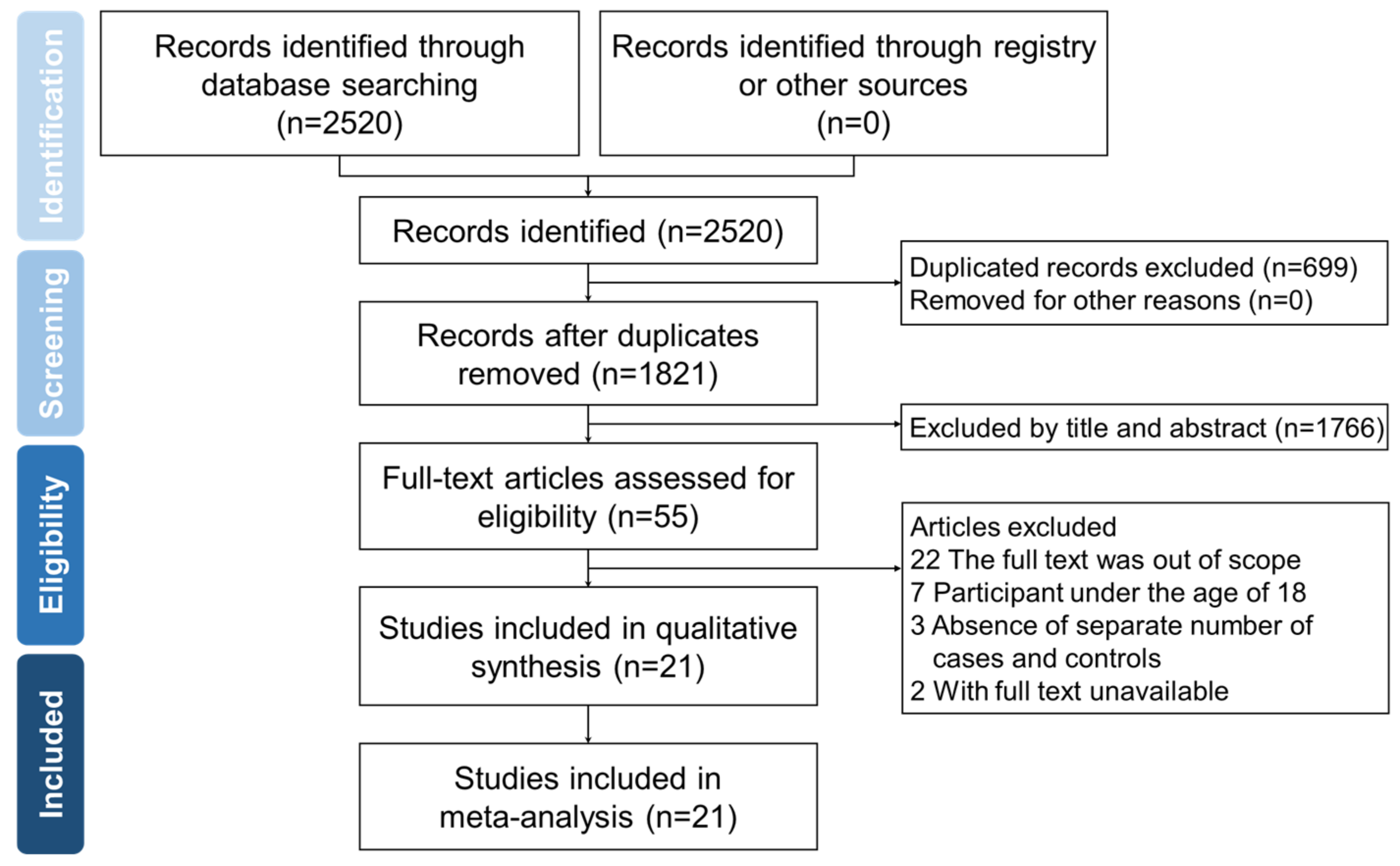
3.1. Literature Search Results
3.2. The Characteristics of Included Studies
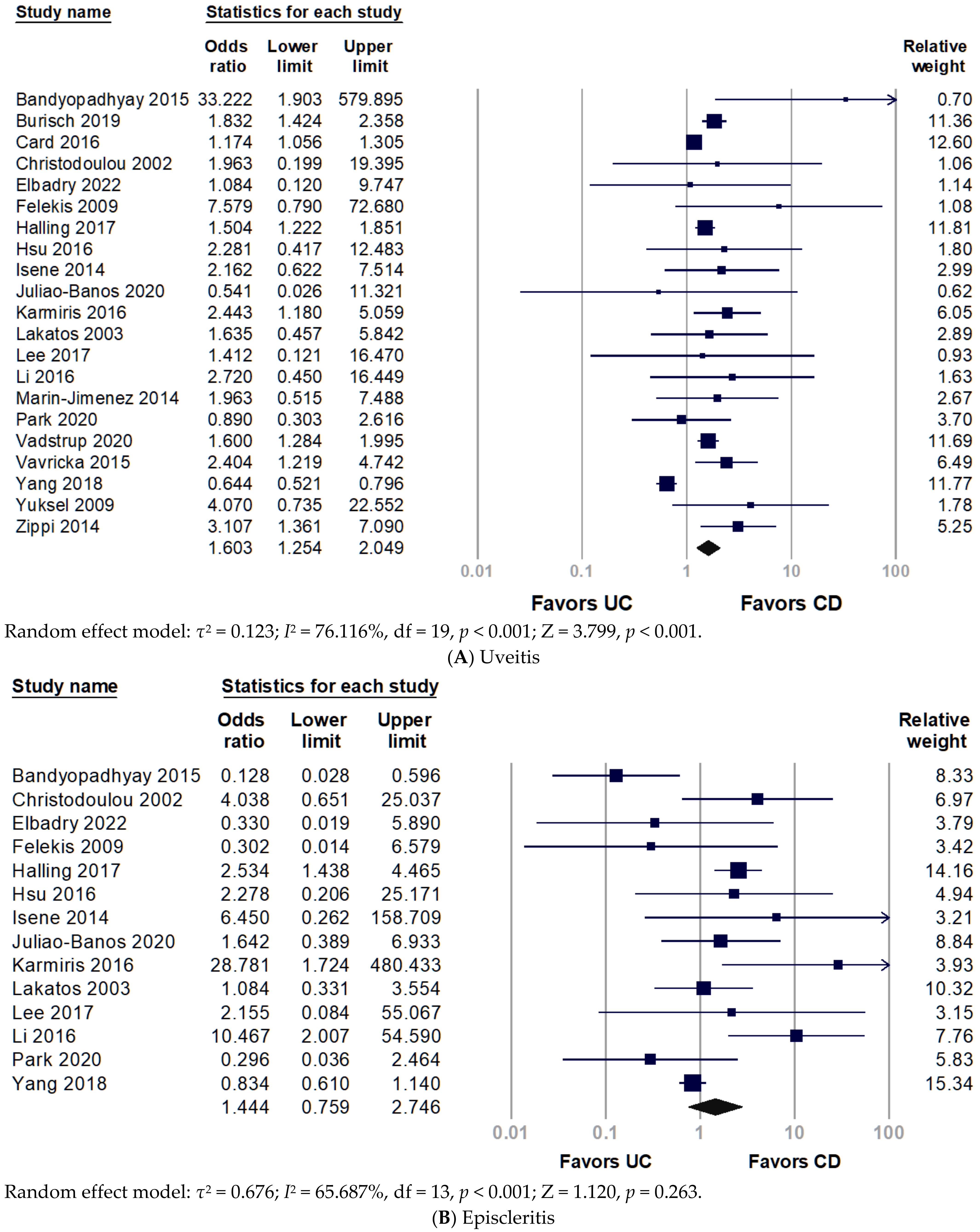
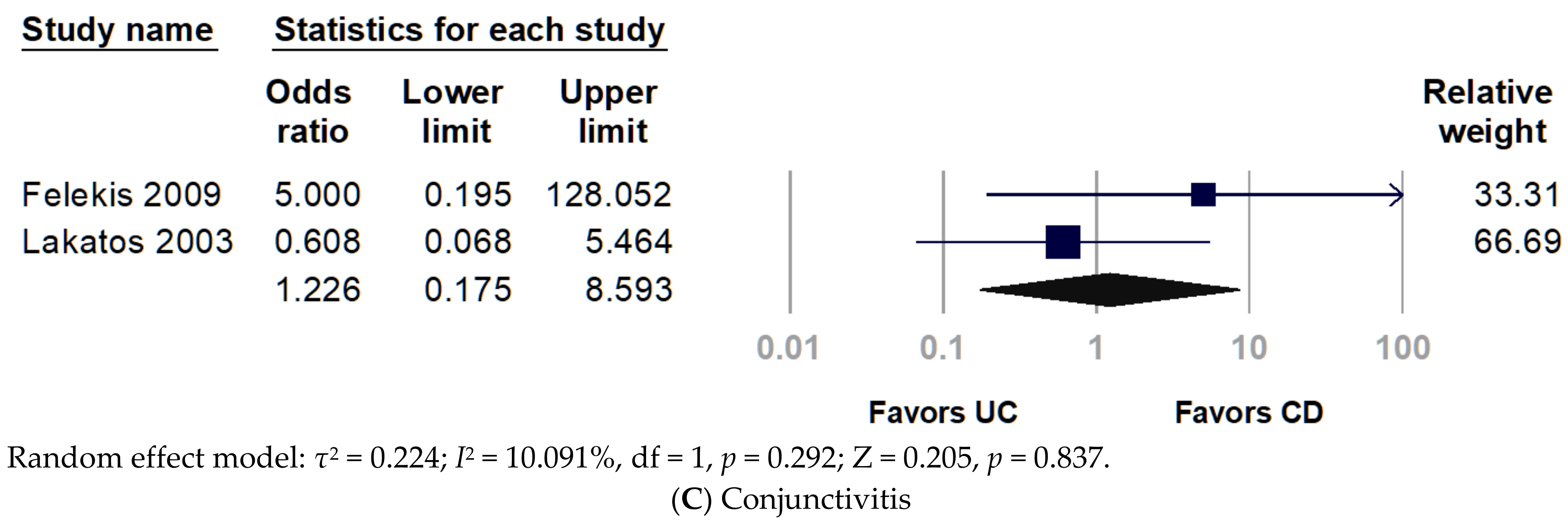
3.3. Association of O-EIMs with IBD
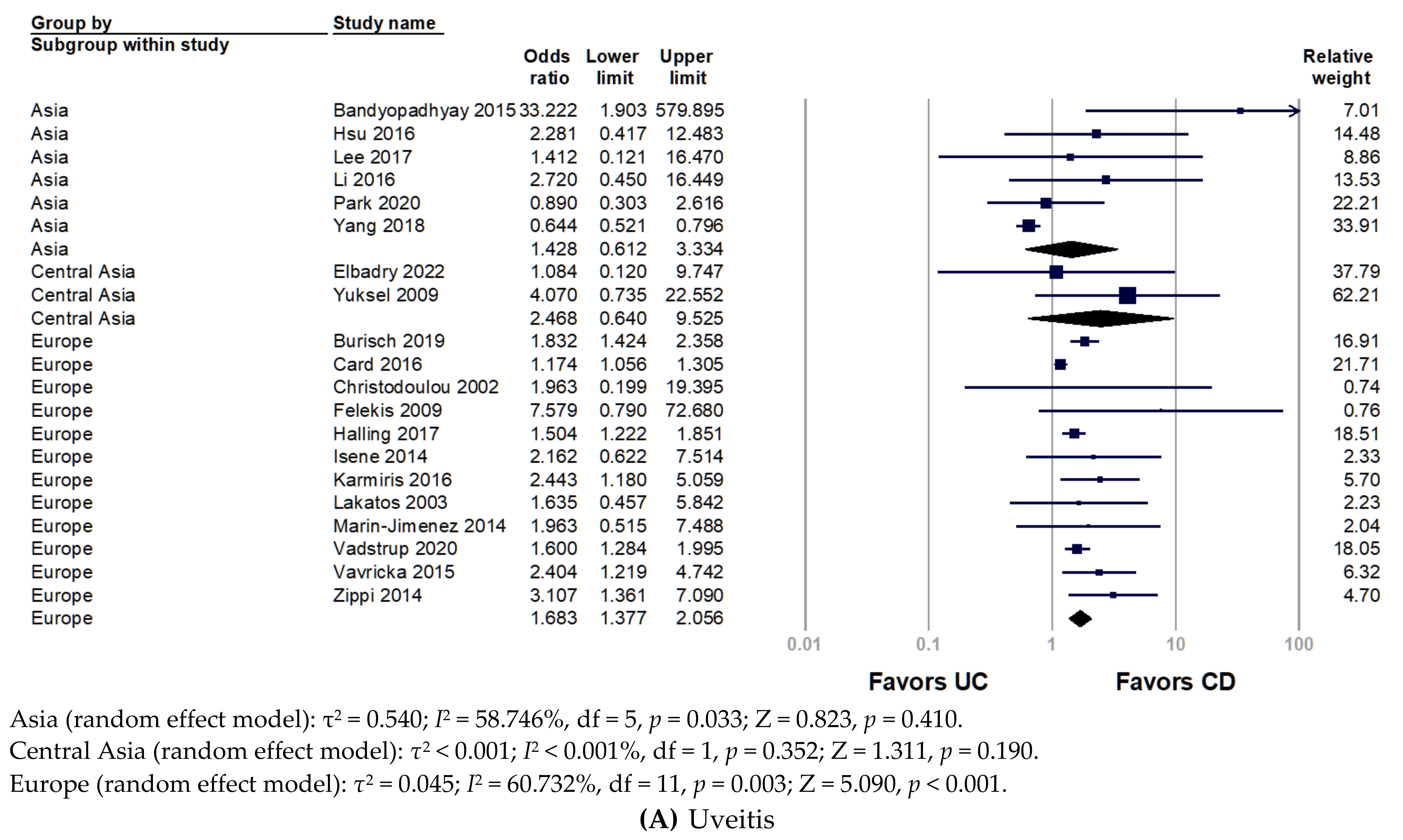
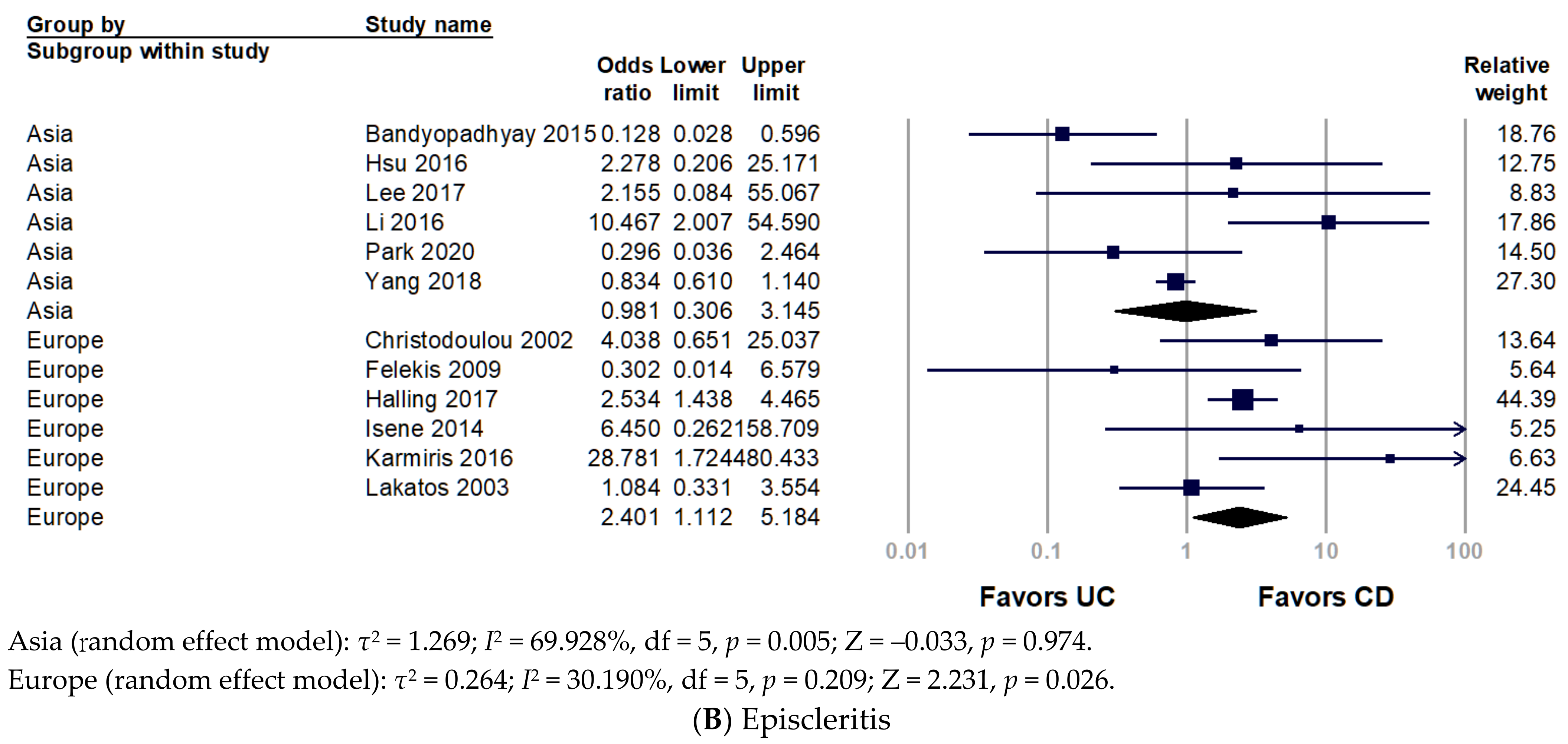
3.4. Stratification with World Regions
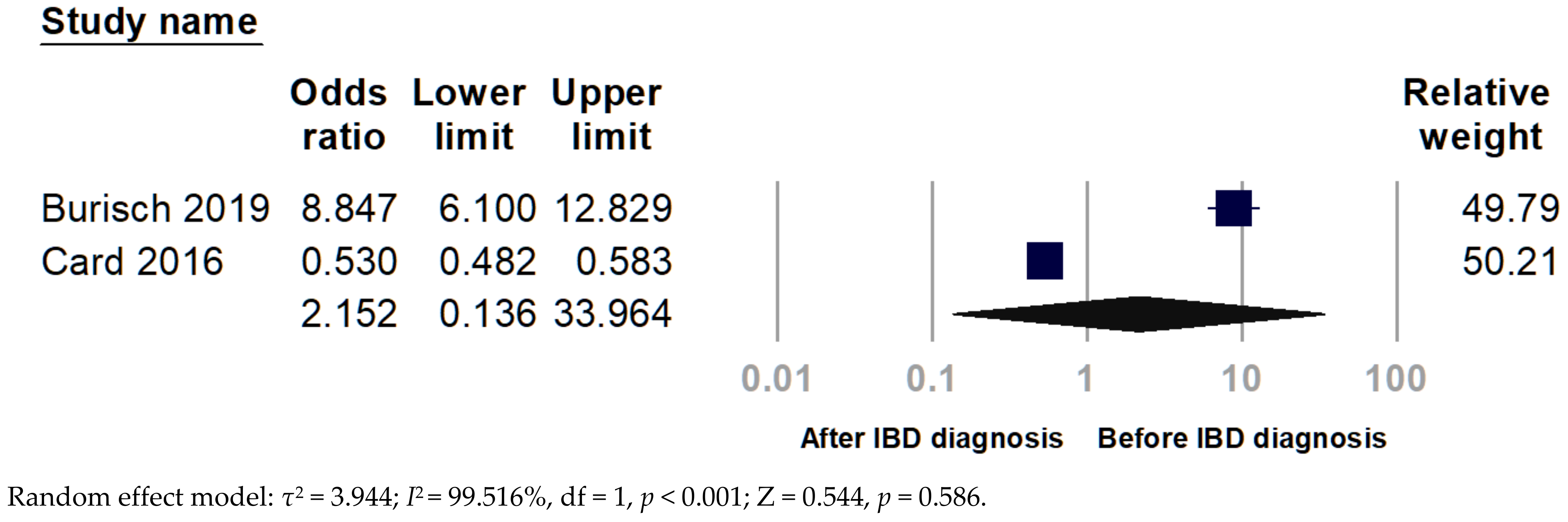
3.5. Chronological Analysis
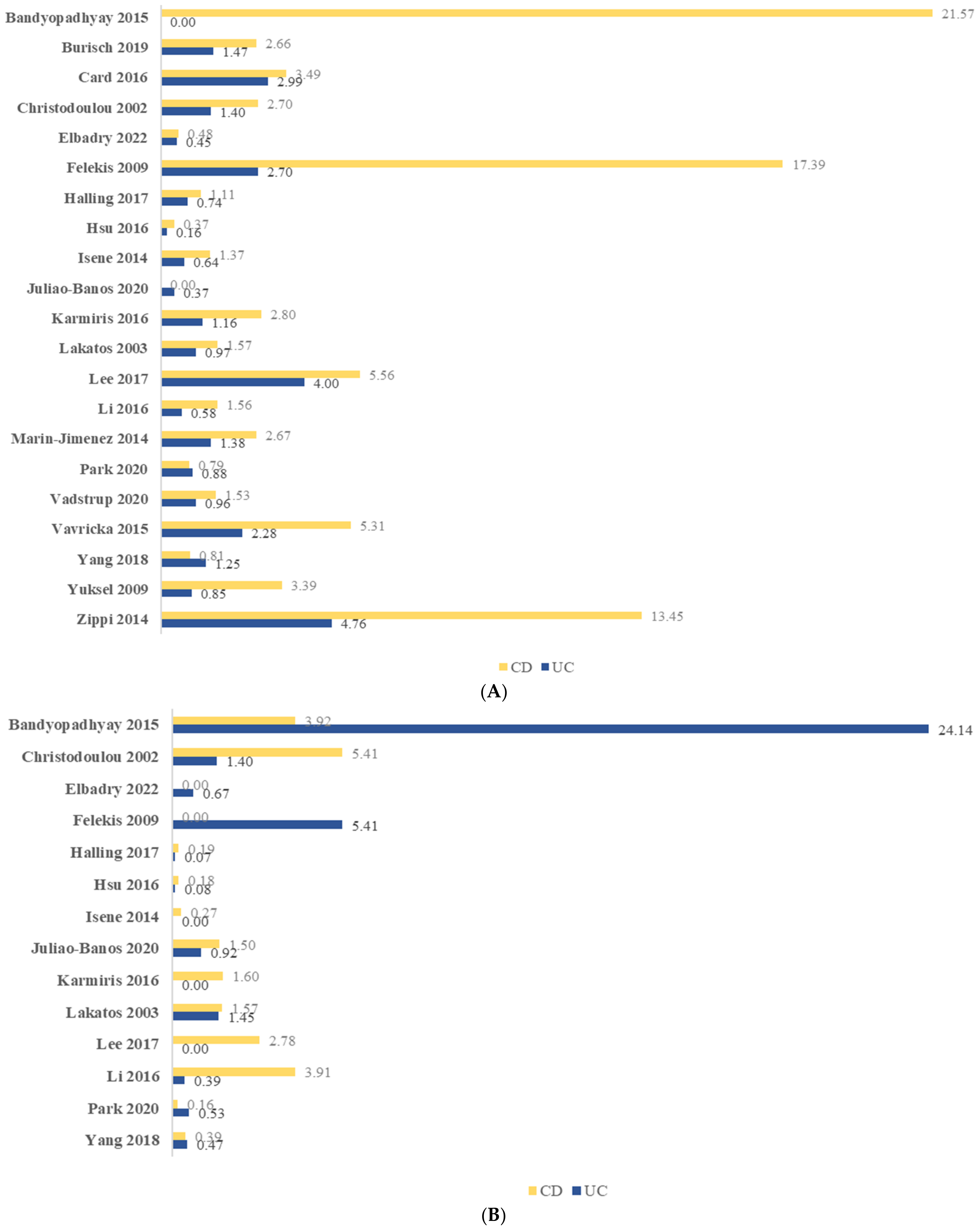
3.6. Period Prevalence of O-EIMs
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Ott, C.; Scholmerich, J. Extraintestinal manifestations and complications in IBD. Nat. Rev. Gastroenterol. Hepatol. 2013, 10, 585–595. [Google Scholar] [CrossRef]
- Greuter, T.; Vavricka, S.R. Extraintestinal manifestations in inflammatory bowel disease-epidemiology, genetics, and pathogenesis. Expert Rev. Gastroenterol. Hepatol. 2019, 13, 307–317. [Google Scholar] [CrossRef] [PubMed]
- Mady, R.; Grover, W.; Butrus, S. Ocular complications of inflammatory bowel disease. Sci. World J. 2015, 2015, 438402. [Google Scholar] [CrossRef] [PubMed]
- Vavricka, S.R.; Rogler, G.; Gantenbein, C.; Spoerri, M.; Prinz Vavricka, M.; Navarini, A.A.; French, L.E.; Safroneeva, E.; Fournier, N.; Straumann, A.; et al. Chronological Order of Appearance of Extraintestinal Manifestations Relative to the Time of IBD Diagnosis in the Swiss Inflammatory Bowel Disease Cohort. Inflamm. Bowel Dis. 2015, 21, 1794–1800. [Google Scholar] [CrossRef] [PubMed]
- Durrani, O.M.; Tehrani, N.N.; Marr, J.E.; Moradi, P.; Stavrou, P.; Murray, P.I. Degree, duration, and causes of visual loss in uveitis. Br. J. Ophthalmol. 2004, 88, 1159–1162. [Google Scholar] [CrossRef]
- Munoz-Fernandez, S.; Martin-Mola, E. Uveitis. Best Pract. Res. Clin. Rheumatol. 2006, 20, 487–505. [Google Scholar] [CrossRef]
- Harbord, M.; Annese, V.; Vavricka, S.R.; Allez, M.; Barreiro-de Acosta, M.; Boberg, K.M.; Burisch, J.; De Vos, M.; De Vries, A.M.; Dick, A.D.; et al. The First European Evidence-based Consensus on Extra-intestinal Manifestations in Inflammatory Bowel Disease. J. Crohns. Colitis. 2016, 10, 239–254. [Google Scholar] [CrossRef]
- Colia, R.; Corrado, A.; Cantatore, F.P. Rheumatologic and extraintestinal manifestations of inflammatory bowel diseases. Ann. Med. 2016, 48, 577–585. [Google Scholar] [CrossRef]
- Katsanos, A.; Asproudis, I.; Katsanos, K.H.; Dastiridou, A.I.; Aspiotis, M.; Tsianos, E.V. Orbital and optic nerve complications of inflammatory bowel disease. J. Crohns. Colitis. 2013, 7, 683–693. [Google Scholar] [CrossRef]
- Bandyopadhyay, D.; Bandyopadhyay, S.; Ghosh, P.; De, A.; Bhattacharya, A.; Dhali, G.K.; Das, K. Extraintestinal manifestations in inflammatory bowel disease: Prevalence and predictors in Indian patients. Indian J. Gastroenterol. 2015, 34, 387–394. [Google Scholar] [CrossRef]
- Lanna, C.C.; Ferrari Mde, L.; Rocha, S.L.; Nascimento, E.; De Carvalho, M.A.; Da Cunha, A.S. A cross-sectional study of 130 Brazilian patients with Crohn’s disease and ulcerative colitis: Analysis of articular and ophthalmologic manifestations. Clin. Rheumatol. 2008, 27, 503–509. [Google Scholar] [CrossRef]
- Ananthakrishnan, A.N. Environmental risk factors for inflammatory bowel disease. Gastroenterol. Hepatol. 2013, 9, 367–374. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef]
- Burisch, J.; Jess, T.; Egeberg, A. Incidence of Immune-Mediated Inflammatory Diseases Among Patients With Inflammatory Bowel Diseases in Denmark. Clin. Gastroenterol. Hepatol. 2019, 17, 2704–2712.e3. [Google Scholar] [CrossRef]
- Card, T.R.; Langan, S.M.; Chu, T.P. Extra-Gastrointestinal Manifestations of Inflammatory Bowel Disease May Be Less Common Than Previously Reported. Dig. Dis. Sci. 2016, 61, 2619–2626. [Google Scholar] [CrossRef]
- Christodoulou, D.K.; Katsanos, K.H.; Kitsanou, M.; Stergiopoulou, C.; Hatzis, J.; Tsianos, E.V. Frequency of extraintestinal manifestations in patients with inflammatory bowel disease in Northwest Greece and review of the literature. Dig. Liver Dis. 2002, 34, 781–786. [Google Scholar] [CrossRef]
- Elbadry, M.; Nour, M.O.; Hussien, M.; Ghoneem, E.A.; Medhat, M.A.; Shehab, H.; Galal, S.; Eltabbakh, M.; El-Raey, F.; Negm, M.; et al. Clinico-Epidemiological Characteristics of Patients With Inflammatory Bowel Disease in Egypt: A Nationwide Multicenter Study. Front. Med. 2022, 9, 867293. [Google Scholar] [CrossRef]
- Felekis, T.; Katsanos, K.; Kitsanou, M.; Trakos, N.; Theopistos, V.; Christodoulou, D.; Asproudis, I.; Tsianos, E.V. Spectrum and frequency of ophthalmologic manifestations in patients with inflammatory bowel disease: A prospective single-center study. Inflamm. Bowel Dis. 2009, 15, 29–34. [Google Scholar] [CrossRef]
- Halling, M.L.; Kjeldsen, J.; Knudsen, T.; Nielsen, J.; Hansen, L.K. Patients with inflammatory bowel disease have increased risk of autoimmune and inflammatory diseases. World J. Gastroenterol. 2017, 23, 6137–6146. [Google Scholar] [CrossRef]
- Hsu, Y.C.; Wu, T.C.; Lo, Y.C.; Wang, L.S. Gastrointestinal complications and extraintestinal manifestations of inflammatory bowel disease in Taiwan: A population-based study. J. Chin. Med. Assoc. 2017, 80, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Isene, R.; Bernklev, T.; Hoie, O.; Munkholm, P.; Tsianos, E.; Stockbrugger, R.; Odes, S.; Palm, O.; Smastuen, M.; Moum, B.; et al. Extraintestinal manifestations in Crohn’s disease and ulcerative colitis: Results from a prospective, population-based European inception cohort. Scand. J. Gastroenterol. 2015, 50, 300–305. [Google Scholar] [CrossRef] [PubMed]
- Juliao-Banos, F.; Arrubla, M.; Osorio, L.; Camargo, J.; Londono, J.; Caceres, C.; Carvajal, J.; Mosquera-Klinger, G.; Donado, J. Characterization and prevalence of extraintestinal manifestations in a cohort of patients with inflammatory intestinal disease in Medellin, Colombia. Gastroenterol. Hepatol. 2021, 44, 398–404. [Google Scholar] [CrossRef] [PubMed]
- Karmiris, K.; Avgerinos, A.; Tavernaraki, A.; Zeglinas, C.; Karatzas, P.; Koukouratos, T.; Oikonomou, K.A.; Kostas, A.; Zampeli, E.; Papadopoulos, V.; et al. Prevalence and Characteristics of Extra-intestinal Manifestations in a Large Cohort of Greek Patients with Inflammatory Bowel Disease. J. Crohns. Colitis. 2016, 10, 429–436. [Google Scholar] [CrossRef]
- Lakatos, L. Extraintestinal manifestations in inflammatory bowel diseases. Lege Artis Med. 2003, 13, 186–193. [Google Scholar] [CrossRef]
- Lee, H.J.; Song, H.J.; Jeong, J.H.; Kim, H.U.; Boo, S.J.; Na, S.Y. Ophthalmologic manifestations in patients with inflammatory bowel disease. Intest. Res. 2017, 15, 380–387. [Google Scholar] [CrossRef]
- Li, Y.C.; Li, W.Z.; Wu, C.R.; Feng, Y.; Ren, L.; Mi, C.; Li, Y. Prevalence and characteristics of ophthalmological extra-intestinal manifestations in Chinese patients with inflammatory bowel disease. Int. J. Ophthalmol. 2016, 9, 1476–1479. [Google Scholar] [CrossRef]
- Marin-Jimenez, I.; Garcia Sanchez, V.; Gisbert, J.P.; Lazaro Perez Calle, J.; Lujan, M.; Gordillo Abalos, J.; Tabernero, S.; Julia, B.; Romero, C.; Cea-Calvo, L.; et al. Immune-mediated inflammatory diseases in patients with inflammatory bowel disease. Baseline data from the Aquiles study. Gastroenterol. Hepatol. 2014, 37, 495–502. [Google Scholar] [CrossRef]
- Park, S.K.; Wong, Z.; Park, S.H.; Vu, K.V.; Bang, K.B.; Piyachaturawat, P.; Myint, T.; Hilmi, I.; Park, D.I. Extraintestinal manifestation of inflammatory bowel disease in Asian patients: A multinational study. Dig. Liver Dis. 2021, 53, 196–201. [Google Scholar] [CrossRef]
- Vadstrup, K.; Alulis, S.; Borsi, A.; Jørgensen, T.R.; Nielsen, A.; Munkholm, P.; Qvist, N. Extraintestinal Manifestations and Other Comorbidities in Ulcerative Colitis and Crohn Disease: A Danish Nationwide Registry Study 2003–2016. Crohn’s Colitis 360 2020, 2, 1–10. [Google Scholar] [CrossRef]
- Yang, B.R.; Choi, N.K.; Kim, M.S.; Chun, J.; Joo, S.H.; Kim, H.; Lee, J. Prevalence of extraintestinal manifestations in Korean inflammatory bowel disease patients. PLoS ONE 2018, 13, e0200363. [Google Scholar] [CrossRef]
- Yuksel, I.; Basar, O.; Ataseven, H.; Ertugrul, I.; Arhan, M.; Ibis, M.; Dagli, U.; Demirel, B.T.; Ulker, A.; Secilmis, S.; et al. Mucocutaneous manifestations in inflammatory bowel disease. Inflamm. Bowel Dis. 2009, 15, 546–550. [Google Scholar] [CrossRef]
- Zippi, M.; Corrado, C.; Pica, R.; Avallone, E.V.; Cassieri, C.; De Nitto, D.; Paoluzi, P.; Vernia, P. Extraintestinal manifestations in a large series of Italian inflammatory bowel disease patients. World J. Gastroenterol. 2014, 20, 17463–17467. [Google Scholar] [CrossRef]
- Bernstein, C.N.; Blanchard, J.F.; Rawsthorne, P.; Yu, N. The prevalence of extraintestinal diseases in inflammatory bowel disease: A population-based study. Am. J. Gastroenterol. 2001, 96, 1116–1122. [Google Scholar] [CrossRef]
- Biedermann, L.; Renz, L.; Fournier, N.; Rossel, J.B.; Butter, M.; Bluemel, S.; Vavricka, S.R.; Rogler, G.; Scharl, M. Uveitis manifestations in patients of the Swiss Inflammatory Bowel Disease Cohort Study. Therap. Adv. Gastroenterol. 2019, 12, 1756284819865142. [Google Scholar] [CrossRef]
- Jose, F.A.; Garnett, E.A.; Vittinghoff, E.; Ferry, G.D.; Winter, H.S.; Baldassano, R.N.; Kirschner, B.S.; Cohen, S.A.; Gold, B.D.; Abramson, O.; et al. Development of extraintestinal manifestations in pediatric patients with inflammatory bowel disease. Inflamm. Bowel Dis. 2009, 15, 63–68. [Google Scholar] [CrossRef]
- Greuter, T.; Bertoldo, F.; Rechner, R.; Straumann, A.; Biedermann, L.; Zeitz, J.; Misselwitz, B.; Scharl, M.; Rogler, G.; Safroneeva, E.; et al. Extraintestinal Manifestations of Pediatric Inflammatory Bowel Disease: Prevalence, Presentation, and Anti-TNF Treatment. J. Pediatr. Gastroenterol. Nutr. 2017, 65, 200–206. [Google Scholar] [CrossRef]
- Ottaviano, G.; Salvatore, S.; Salvatoni, A.; Martelossi, S.; Ventura, A.; Naviglio, S. Ocular Manifestations of Paediatric Inflammatory Bowel Disease: A Systematic Review and Meta-analysis. J. Crohns. Colitis. 2018, 12, 870–879. [Google Scholar] [CrossRef]
- Lo, T.C.; Chen, Y.Y.; Chen, H.H. Risk of inflammatory bowel disease in uveitis patients: A population-based cohort study. Eye 2022, 36, 1288–1293. [Google Scholar] [CrossRef]
- King, D.; Chandan, J.S.; Thomas, T.; Denniston, A.K.; Braithwaite, T.; Niranthrankumar, K.; Reulen, R.; Adderley, N.; Trudgill, N.J. Risk of a subsequent diagnosis of inflammatory bowel disease in subjects with ophthalmic disorders associated with inflammatory bowel disease: A retrospective cohort analysis of UK primary care data. BMJ Open 2022, 12, e052833. [Google Scholar] [CrossRef] [PubMed]
- Vavricka, S.R.; Brun, L.; Ballabeni, P.; Pittet, V.; Prinz Vavricka, B.M.; Zeitz, J.; Rogler, G.; Schoepfer, A.M. Frequency and risk factors for extraintestinal manifestations in the Swiss inflammatory bowel disease cohort. Am. J. Gastroenterol. 2011, 106, 110–119. [Google Scholar] [CrossRef] [PubMed]
- Taleban, S.; Li, D.; Targan, S.R.; Ippoliti, A.; Brant, S.R.; Cho, J.H.; Duerr, R.H.; Rioux, J.D.; Silverberg, M.S.; Vasiliauskas, E.A.; et al. Ocular Manifestations in Inflammatory Bowel Disease Are Associated with Other Extra-intestinal Manifestations, Gender, and Genes Implicated in Other Immune-related Traits. J. Crohns. Colitis. 2016, 10, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Peyrin-Biroulet, L.; Van Assche, G.; Gomez-Ulloa, D.; Garcia-Alvarez, L.; Lara, N.; Black, C.M.; Kachroo, S. Systematic Review of Tumor Necrosis Factor Antagonists in Extraintestinal Manifestations in Inflammatory Bowel Disease. Clin. Gastroenterol. Hepatol. 2017, 15, 25–36.e27. [Google Scholar] [CrossRef] [PubMed]
- Veloso, F.T.; Carvalho, J.; Magro, F. Immune-related systemic manifestations of inflammatory bowel disease. A prospective study of 792 patients. J. Clin. Gastroenterol. 1996, 23, 29–34. [Google Scholar] [CrossRef]
- Ricart, E.; Panaccione, R.; Loftus, E.V., Jr.; Tremaine, W.J.; Harmsen, W.S.; Zinsmeister, A.R.; Sandborn, W.J. Autoimmune disorders and extraintestinal manifestations in first-degree familial and sporadic inflammatory bowel disease: A case-control study. Inflamm. Bowel Dis. 2004, 10, 207–214. [Google Scholar] [CrossRef]
- Troncoso, L.L.; Biancardi, A.L.; De Moraes, H.V., Jr.; Zaltman, C. Ophthalmic manifestations in patients with inflammatory bowel disease: A review. World J. Gastroenterol. 2017, 23, 5836–5848. [Google Scholar] [CrossRef]
- Tavarela Veloso, F. Review article: Skin complications associated with inflammatory bowel disease. Aliment. Pharmacol. Ther. 2004, 20 (Suppl. S4), 50–53. [Google Scholar] [CrossRef]
- Greuter, T.; Navarini, A.; Vavricka, S.R. Skin Manifestations of Inflammatory Bowel Disease. Clin. Rev. Allergy Immunol. 2017, 53, 413–427. [Google Scholar] [CrossRef]
- Pardi, D.S.; Tremaine, W.J.; Sandborn, W.J.; McCarthy, J.T. Renal and urologic complications of inflammatory bowel disease. Am. J. Gastroenterol. 1998, 93, 504–514. [Google Scholar] [CrossRef]
- Santeford, A.; Wiley, L.A.; Park, S.; Bamba, S.; Nakamura, R.; Gdoura, A.; Ferguson, T.A.; Rao, P.K.; Guan, J.L.; Saitoh, T.; et al. Impaired autophagy in macrophages promotes inflammatory eye disease. Autophagy 2016, 12, 1876–1885. [Google Scholar] [CrossRef]
- Lin, P.; Tessler, H.H.; Goldstein, D.A. Family history of inflammatory bowel disease in patients with idiopathic ocular inflammation. Am. J. Ophthalmol. 2006, 141, 1097–1104. [Google Scholar] [CrossRef]
- Algaba, A.; Guerra, I.; Ricart, E.; Iglesias, E.; Manosa, M.; Gisbert, J.P.; Guardiola, J.; Minguez, M.; Castro, B.; De Francisco, R.; et al. Extraintestinal Manifestations in Patients with Inflammatory Bowel Disease: Study Based on the ENEIDA Registry. Dig. Dis. Sci. 2021, 66, 2014–2023. [Google Scholar] [CrossRef]
- Petagna, L.; Antonelli, A.; Ganini, C.; Bellato, V.; Campanelli, M.; Divizia, A.; Efrati, C.; Franceschilli, M.; Guida, A.M.; Ingallinella, S.; et al. Pathophysiology of Crohn’s disease inflammation and recurrence. Biol. Direct. 2020, 15, 23. [Google Scholar] [CrossRef]
- Kaur, A.; Goggolidou, P. Ulcerative colitis: Understanding its cellular pathology could provide insights into novel therapies. J. Inflamm. 2020, 17, 15. [Google Scholar] [CrossRef]
- Torres, J.; Mehandru, S.; Colombel, J.F.; Peyrin-Biroulet, L. Crohn’s disease. Lancet 2017, 389, 1741–1755. [Google Scholar] [CrossRef]
- Ordas, I.; Eckmann, L.; Talamini, M.; Baumgart, D.C.; Sandborn, W.J. Ulcerative colitis. Lancet 2012, 380, 1606–1619. [Google Scholar] [CrossRef]
- Beaugerie, L.; Langholz, E.; Nyboe-Andersen, N.; Pigneur, B.; Sokol, H.; Epicom, E. Differences in epidemiological features between ulcerative colitis and Crohn’s disease: The early life-programmed versus late dysbiosis hypothesis. Med. Hypotheses 2018, 115, 19–21. [Google Scholar] [CrossRef]
- Qin, X. Food additives: Possible cause for recent remarkable increase of inflammatory bowel disease in children. J. Pediatr. Gastroenterol. Nutr. 2012, 54, 564. [Google Scholar] [CrossRef]
- Lowe, A.M.; Roy, P.O.; Poulin, M.B.; Michel, P.; Bitton, A.; St-Onge, L.; Brassard, P. Epidemiology of Crohn’s disease in Quebec, Canada. Inflamm. Bowel Dis. 2009, 15, 429–435. [Google Scholar] [CrossRef]
- Bernstein, C.N.; Wajda, A.; Svenson, L.W.; MacKenzie, A.; Koehoorn, M.; Jackson, M.; Fedorak, R.; Israel, D.; Blanchard, J.F. The epidemiology of inflammatory bowel disease in Canada: A population-based study. Am. J. Gastroenterol. 2006, 101, 1559–1568. [Google Scholar] [CrossRef] [PubMed]
- Abramson, O.; Durant, M.; Mow, W.; Finley, A.; Kodali, P.; Wong, A.; Tavares, V.; McCroskey, E.; Liu, L.; Lewis, J.D.; et al. Incidence, prevalence, and time trends of pediatric inflammatory bowel disease in Northern California, 1996 to 2006. J. Pediatr. 2010, 157, 233–239.e1. [Google Scholar] [CrossRef] [PubMed]
- Perminow, G.; Brackmann, S.; Lyckander, L.G.; Franke, A.; Borthne, A.; Rydning, A.; Aamodt, G.; Schreiber, S.; Vatn, M.H.; Group, I.-I. A characterization in childhood inflammatory bowel disease, a new population-based inception cohort from South-Eastern Norway, 2005–2007, showing increased incidence in Crohn’s disease. Scand. J. Gastroenterol. 2009, 44, 446–456. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Number | Country | Duration (years) | Definition of Uveitis | Uveitis | Episcleritis | Conjunctivitis | IBD | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CD | UC | CD | UC | CD | UC | CD | UC | |||||
| Bandyopadhyay 2015 [10] | 109 | India | 1.5 | uveitis | 11 | 0 | 2 | 14 | - | - | 51 | 58 |
| Burisch 2019 [16] | 14,377 | Denmark | 15 | iridocyclitis | 103 | 154 | - | - | - | - | 3879 | 10,498 |
| Card 2016 [17] | 45,312 | UK | 24 | uveitis | 636 | 811 | - | - | - | - | 18,204 | 27,108 |
| Christodoulou 2002 [18] | 252 | Greece | 14 | iridocyclitis | 1 | 3 | 2 | 3 | - | - | 37 | 215 |
| Elbadry 2022 [19] | 2001 | Egypt | 3 | uveitis | 1 | 4 | 0 | 6 | - | - | 207 | 897 |
| Felekis 2009 [20] | 60 | Greece | N/M | uveitis | 4 | 1 | 0 | 2 | 1 | 0 | 23 | 37 |
| Halling 2017 [21] | 44,409 | Denmark | 36 | iridocyclitis | 148 | 230 | 25 | 23 | - | - | 13,343 | 31,066 |
| Hsu 2016 [22] | 3153 | Taiwan | 13 | iritis, uveitis | 2 | 4 | 1 | 2 | - | - | 547 | 2490 |
| Isene 2014 [23] | 1145 | Multi-national * | 2 | iridocyclitis, uveitis | 5 | 5 | 1 | 0 | - | - | 364 | 781 |
| Juliao-Banos 2020 [24] | 744 | Colombia | N/M | uveitis | 0 | 2 | 3 | 5 | - | - | 200 | 544 |
| Karmiris 2016 [25] | 1860 | Greece | N/M | iridocyclitis, vitritis, choroiditis, retinitis | 28 | 10 | 16 | 0 | - | - | 1001 | 859 |
| Lakatos 2003 [26] | 873 | Hungary | 25 | anterior uveitis | 4 | 6 | 4 | 9 | 1 | 4 | 254 | 619 |
| Lee 2017 [27] | 61 | Korea | 1 | iritis | 2 | 1 | 1 | 0 | - | - | 36 | 25 |
| Li 2016 [28] | 645 | China | 20 | uveitis | 2 | 3 | 5 | 2 | - | - | 128 | 517 |
| Marin-Jimenez 2014 [29] | 518 | Spain | 2 | uveitis | 8 | 3 | - | - | - | - | 300 | 218 |
| Park 2020 [30] | 1764 | Multi-national # | 16 | iritis, uveitis | 5 | 10 | 1 | 6 | - | - | 634 | 1130 |
| Vadstrup 2020 [31] | 32,446 | Denmark | 13 | iritis, uveitis | 134 | 199 | - | - | - | - | 8769 | 20,722 |
| Vavricka 2015 [4] | 1218 | Switzerland | 4 | uveitis | 39 | 11 | - | - | - | - | 735 | 483 |
| Yang 2018 [32] | 43,281 | Korea | 1 | iridocyclitis | 113 | 368 | 55 | 139 | - | - | 13,925 | 29,356 |
| Yuksel 2009 [33] | 352 | Turkey | 4.5 | uveitis | 4 | 2 | - | - | - | - | 118 | 234 |
| Zippi 2014 [34] | 329 | Italy | 12 | uveitis | 16 | 10 | - | - | - | - | 119 | 210 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, J.-X.; Chiang, C.-C.; Chen, S.-N.; Lin, J.-M.; Tsai, Y.-Y. The Prevalence of Ocular Extra-Intestinal Manifestations in Adults Inflammatory Bowel Disease: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 15683. https://doi.org/10.3390/ijerph192315683
Li J-X, Chiang C-C, Chen S-N, Lin J-M, Tsai Y-Y. The Prevalence of Ocular Extra-Intestinal Manifestations in Adults Inflammatory Bowel Disease: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2022; 19(23):15683. https://doi.org/10.3390/ijerph192315683
Chicago/Turabian StyleLi, Jing-Xing, Chun-Chi Chiang, San-Ni Chen, Jane-Ming Lin, and Yi-Yu Tsai. 2022. "The Prevalence of Ocular Extra-Intestinal Manifestations in Adults Inflammatory Bowel Disease: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 19, no. 23: 15683. https://doi.org/10.3390/ijerph192315683
APA StyleLi, J.-X., Chiang, C.-C., Chen, S.-N., Lin, J.-M., & Tsai, Y.-Y. (2022). The Prevalence of Ocular Extra-Intestinal Manifestations in Adults Inflammatory Bowel Disease: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 19(23), 15683. https://doi.org/10.3390/ijerph192315683