
Clinical and Pathological Manifestation of the Oral Mucosa in Institutionalized Children from Romania

 and
and
Abstract
1. Introduction
2. Materials and Methods
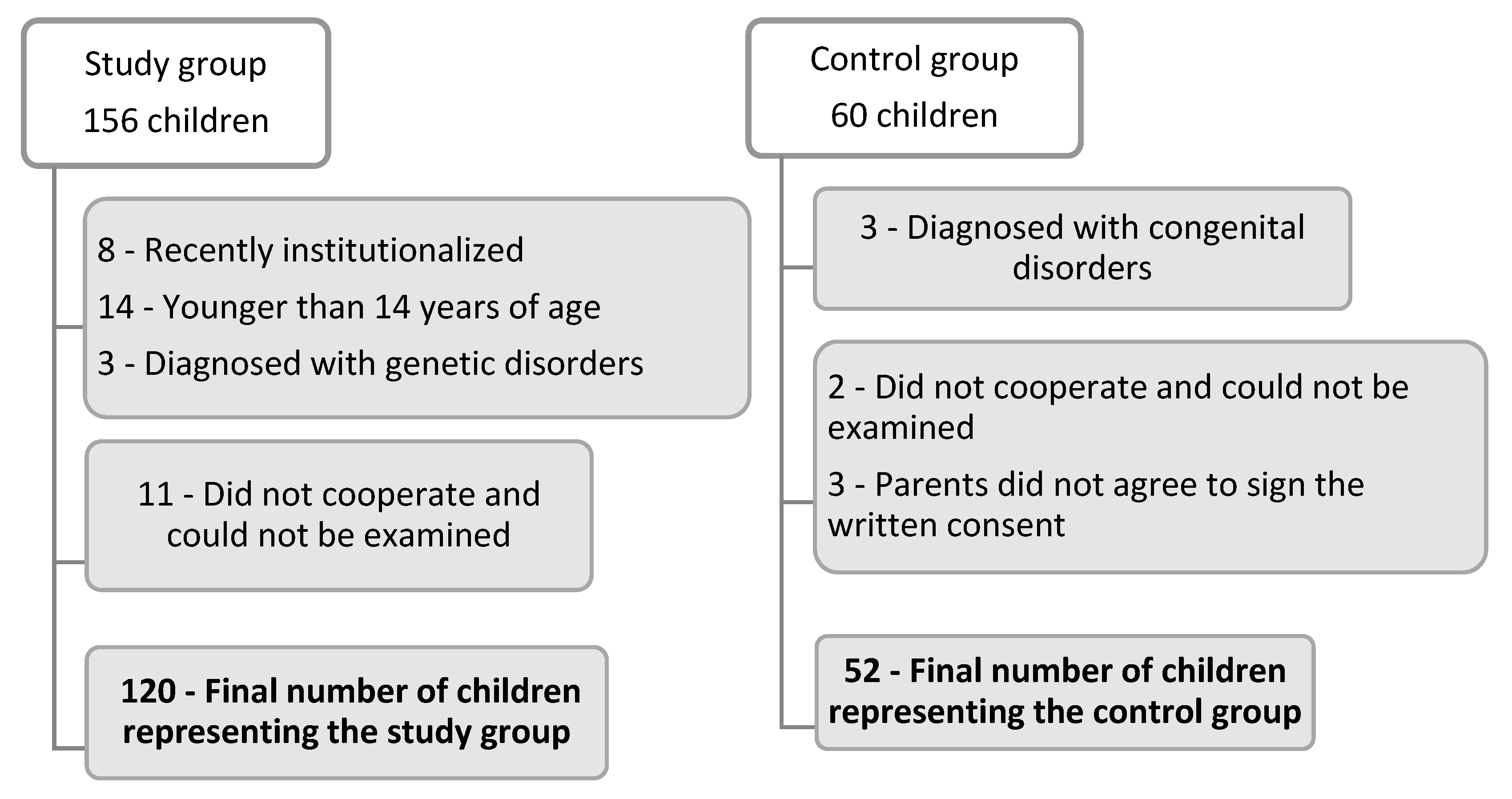
2.1. Study Design
2.2. Clinical Examination and Assessment
2.3. Statistical Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Do, K.Y. Association between Mental Health and Oral Symptoms Experienced in Korean Adolescents; The Ninth Korea Youth Risk Behavior Web-Based Survey. Master’s Thesis, Catholic University of Korea, Seoul, Republic of Korea, 2013. [Google Scholar]
- Little, J.W. Dental implications of mood disorders. Gen. Dent. 2004, 52, 442–450. [Google Scholar]
- Clark, D.B. Dental care for the patient with bipolar disorder. J. Can. Dent. Assoc. 2003, 69, 20–24. [Google Scholar]
- Kim, Y.Y.; Yoo, S.Y. Relationship between health behaviors and factors influencing suicidal ideation in adolescents with asthma by gender differences: Using data from the 10th Korea Youth Risk Behavior Web-based Survey. J. Korean Parent Child Health 2017, 20, 49–57. [Google Scholar]
- Chapple, I.L. The impact of oral disease upon systemic health—Symposium overview. J. Dent. 2009, 37, S568–S571. [Google Scholar] [CrossRef]
- Cormac, I.; Jenkins, P. Understanding the importance of oral health in psychiatric patients. Adv. Psychiatr. Treat. 1999, 5, 53–60. [Google Scholar] [CrossRef]
- George, A.; Lang, G.; Johnson, M.; Ridge, A.; de Silva, A.M.; Ajwani, S. The evaluation of an oral health education program for midwives in Australia. Women Birth 2016, 29, 208–213. [Google Scholar] [CrossRef]
- Cui, T.; Xu, Q.; Wu, Y.; Yang, X.; Sun, H. Longitudinal Follow-up Survey of Effects of Oral Comprehensive Healthcare Measures on Early Childhood Caries. Oral Health Prev. Dent. 2020, 18, 197–203. [Google Scholar] [CrossRef]
- Nsabimana, E.; Rutembesa, E.; Wilhelm, P.; Martin-Soelch, C. Effects of Institutionalization and Parental Living Status on Children’s Self-Esteem, and Externalizing and Internalizing Problems in Rwanda. Front. Psychiatry 2019, 10, 442. [Google Scholar] [CrossRef]
- Stoica, O.; Esian, D.; Bud, A.; Stoica, A.; Beresescu, L.; Bica, C. The Assessment of early server childhood caries status in abandoned Institutionalized Children. Int. J. Environ. Res. Public Health 2022, 19, 8632. [Google Scholar] [CrossRef]
- Vajani, M.; Annest, J.L.; Crosby, A.E.; Alexander, J.D.; Millet, L.M. Nonfatal and fatal self-harm injuries among children aged 10–14 years—United States and Oregon, 2001–2003. Suicide Life Threat. Behav. 2007, 37, 493–506. [Google Scholar] [CrossRef]
- Limeres, J.; Feijoo, J.F.; Baluja, F.; Seoane, J.M.; Diniz, M.; Diz, P. Oral self-injury: An update. Dent. Traumatol. 2013, 29, 8–14. [Google Scholar] [CrossRef]
- Johnson, D.E.; Tang, A.; Almas, A.N.; Degnan, K.A.; McLaughlin, K.A.; Nelson, C.A.; Fox, N.A.; CZeanah, C.H.; Drury, S.S. Caregiving Disruptions Affect Growth and Pubertal Development in Early Adolescence in Institutionalized and Fostered Romanian Children: A Randomized Clinical Trial. J. Pediatr. 2018, 203, 345–353.e3. [Google Scholar] [CrossRef]
- Butera, A.; Maiorani, C.; Morandini, A.; Simonini, M.; Morittu, S.; Trombini, J.; Scribante, A. Evaluation of Children Caries Risk Factors: A Narrative Review of Nutritional Aspects, Oral Hygiene Habits, and Bacterial Alterations. Children 2022, 9, 262. [Google Scholar] [CrossRef]
- Babu, N.C.; Joan Gomes, A. Systemic manifestations of oral diseases. J. Oral Maxillofac. Pathol. 2011, 15, 144–147. [Google Scholar] [CrossRef]
- Dobrova-Krol, N.A.; van Ijzendoorn, M.H.; Bakermans-Kranenburg, M.J.; Cyr, C.; Juffer, F. Physical growth delays and stress dysregulation in stunted and non-stunted Ukrainian institution-reared children. Infant Behav. Dev. 2008, 31, 539–553. [Google Scholar] [CrossRef]
- Yates, T.M.; Carlson, E.A.; Egeland, B. A prospective study of child maltreatment and self-injurious behavior in a community sample. Dev. Psychopathol. 2008, 20, 651–671. [Google Scholar] [CrossRef]
- Brunner, R.; Parzer, P.; Haffner, J. Prevalence and psychological correlates of occasional and deliberate self-harm in adolescents. Arch. Pediatr. Adolesc. Med. 2007, 161, 641–649. [Google Scholar] [CrossRef]
- Portzky, G.; De Wilde, E.J.; van Heeringen, K. Deliberate self-harm in young people: Differences in prevalence and risk factors between the Netherlands and Belgium. Eur. Child Adolesc. Psychiatry 2008, 17, 179–186. [Google Scholar] [CrossRef]
- Tóth, M.D.; Ádám, S.; Zonda, T.; Birkás, E.; Purebl, G. Risk factors for multiple suicide attempts among Roma in Hungary. Transcult. Psychiatry 2018, 55, 55–72. [Google Scholar] [CrossRef]
- Lang, J.; Yao, Y. Prevalence of nonsuicidal self-injury in Chinese middle school and high school students. A meta-analysis. Medicine 2018, 97, e12916. [Google Scholar] [CrossRef]
- AlSadhan, S.A.; Al-Jobair, A.M. Oral habits, dental trauma, and occlusal characteristics among 4- to 12-year-old institutionalized orphan children in Riyadh, Saudi Arabia. Spec. Care Dent. 2017, 37, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Millogo, M.; Ouedraogo, R.W.L.; Ily, V.; Konsem, T.; Ouedraogo, D. Labial lesions by human bite. J. Oral Med. Oral Surg. 2018, 24, 153–156. [Google Scholar] [CrossRef]
- Tortorici, S.; Corrao, S.; Natoli, G.; Difalco, P. Prevalence and distribution of oral mucosal non-malignant lesions in the western Sicilian population. Minerva Stomatol. 2016, 65, 191–206. [Google Scholar]
- Hailegiorgis, M.T.; Berheto, T.M.; Sibamo, E.L.; Asseffa, N.A.; Tesfa, G.; Birhanu, F. Psychological wellbeing of children at public primary schools in Jimma town: An orphan and non-orphan comparative study. PLoS ONE 2018, 13, e0195377. [Google Scholar] [CrossRef]
- Majorana, A.; Bardellini, E.; Flocchini, P.; Amadori, F.; Conti, G.; Campus, G. Oral mucosal lesions in children from 0 to 12 years old: Ten years’ experience. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2010, 110, 13–18. [Google Scholar] [CrossRef]
- Heaton, B.; Cherng, S.T.; Sohn, W. Complex Systems Model of Dynamic Mechanisms of Early Childhood Caries Development. J. Dent. Res. 2020, 99, 537–543. [Google Scholar] [CrossRef]
- Stoica, A.M.; Stoica, O.E.; Vlad, R.E.; Pop, A.M.; Monea, M. Correlation between Oral Self-Harm and Ethnicity in Institutionalized Children. Children 2021, 8, 2. [Google Scholar] [CrossRef] [PubMed]
- Khayamzadeh, M.; Najafi, S.; Sadrolodabaei, P.; Vakili, F.; Kharrazi Fard, M. Determining salivary and serum levels of iron, zinc and vitamin B12 in patients with geographic tongue. J. Dent. Res. Dent. Clin. Dent. Prospect. 2019, 13, 221–226. [Google Scholar] [CrossRef]
- Macpherson, L.M.D.; McCann, M.F.; Gibson, J.; Binnie, V.I.; Stephen, K.W. The role of primary healthcare professionals in oral cancer prevention and detection. Br. Dent. J. 2003, 195, 277–281. [Google Scholar] [CrossRef]
- Hassona, Y.; Scully, C.; Shahin, A.; Maayta, W.; Sawair, F. Factors Influencing Early Detection of Oral Cancer by Primary Health-Care Professionals. J. Cancer Educ. 2016, 31, 285–291. [Google Scholar] [CrossRef]
- Raittio, E.; Farmer, J. Methodological Gaps in Studying the Oral-Systemic Disease Connection. J. Dent. Res. 2021, 100, 445–447. [Google Scholar] [CrossRef] [PubMed]
- Sabbah, W.; Tsakos, G.; Chandola, T.; Sheiham, A.; Watt, R. Social gradients in oral and general health. J. Dent. Res. 2007, 86, 992–996. [Google Scholar] [CrossRef] [PubMed]
- Watt, R.G.; Sheiham, A. Integrating the common risk factor approach into a social determinants framework. Community Dent. Oral Epidemiol. 2012, 40, 289–296. [Google Scholar] [CrossRef] [PubMed]
- Müller, S. Frictional Keratosis, Contact Keratosis and Smokeless Tobacco Keratosis: Features of Reactive White Lesions of the Oral Mucosa. Head Neck Pathol. 2019, 13, 16–24. [Google Scholar] [CrossRef]
- Monea, M.; Olah, P.; Comaneanu, R.M.; Hancu, V.; Ormenisan, A. The Role of Toluidine Blue as a Visual Diagnostic Method in Oral Premalignant Lesions. Rev. Chim. 2016, 67, 1370–1372. [Google Scholar]
- Gilbert, S.; Corey, L.; Cunningham, A.; Malkin, J.E.; Stanberry, L.; Whitley, R.; Spruance, S. An update on short-course intermittent and prevention therapies for herpes labialis. Herpesviridae 2007, 14 (Suppl. S1), 14–18. [Google Scholar]
- Charrier, L.; Berchialla, P.; Galeone, D.; Spizzichino, L.; Boraccino, A.; Lemma, P. Smoking habits among Italian adolescents: What has changed in the last decade? Biomed. Res. Int. 2014, 2014, 287139. [Google Scholar] [CrossRef] [PubMed]
- Maroso, F.B.; Gaio, E.J.; Rösing-Cassiano, K.; Fernandes, M.I. Correlation between gingival thickness and gingival recession in humans. Acta Odontol. Latinoam. 2015, 28, 162–166. [Google Scholar]
- Brannon, R.B.; Anand, P.M. Oral granular cell tumors: An analysis of 10 new pediatric and adolescent case and a review of the literature. J. Clin. Pediatr. Dent. 2004, 29, 69–74. [Google Scholar] [CrossRef]
- Krishnamurthy, A.; George, R.; Majhi, U. Malignant granular cell tumor of the tongue: A clinico-pathological challenge. Indian J. Surg. Oncol. 2014, 5, 71–74. [Google Scholar] [CrossRef] [PubMed]
- Luis-Montoya, P.; Domínguez-Soto, L.; Vega-Memije, E. Lichen Planus in 24 children with review of the literature. Pediatr. Dermatol. 2005, 22, 295–298. [Google Scholar] [CrossRef] [PubMed]
- Regezi, J.; Sciubba, J.; Jordan, R. Oral Pathology, 7th ed.; Elsevier-Saunders: New York, NY, USA, 2016; pp. 15–19. [Google Scholar]
- Lo Giudice, R.; Militi, A.; Nicita, F.; Bruno, G.; Tamà, C.; Lo Giudice, F.; Puleio, F.; Calapai, F.; Mannucci, C. Correlation between Oral Hygiene and IL-6 in Children. Dent. J. 2020, 8, 91. [Google Scholar] [CrossRef] [PubMed]
- Bossù, M.; Trottini, M.; Corridore, D.; Di Giorgio, G.; Sfasciotti, G.L.; Palaia, G.; Ottolenghi, L.; Polimeni, A.; Di Carlo, S. Oral Health Status of Children with Autism in Central Italy. Appl. Sci. 2020, 10, 2247. [Google Scholar] [CrossRef]
- Paszynska, E.; Dmitrzak-Weglarz, M.; Ostalska-Nowicka, D.; Nowicki, M.; Gawriolek, M.; Zachwieja, J. Association of Oral Status and Early Primary Hypertension Biomarkers among Children and Adolescents. Int. J. Environ. Res. Public Health 2020, 17, 7981. [Google Scholar] [CrossRef] [PubMed]
- Bianco, A.; Mazzea, S.; Fortunato, L.; Giudice, A.; Papadopoli, R.; Nobile, C.G.A.; Pavia, M. Oral Health Status and the Impact on Oral Health-Related Quality of Life among the Institutionalized Elderly Population: A Cross-Sectional Study in an Area of Southern Italy. Int. J. Environ. Res. Public Health 2021, 18, 2175. [Google Scholar] [CrossRef] [PubMed]
- Lupi, M.; Pascadopoli, M.; Maiorani, C.; Preda, C.; Trapani, B.; Chiesa, A.; Esposito, F.; Scribante, A.; Butera, A. Oral Hygiene Practice among Hospitalized Patients: An Assessment by Dental Hygiene Students. Healthcare 2022, 10, 115. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gender | Study Group | Control Group |
|---|---|---|
| Boys | 54 (45%) | 25 (48.1%) |
| Girls | 66 (55%) | 27 (51.9%) |
| Age | Study Group Total 120 | Control Group Total 52 |
|---|---|---|
| 14 years old | 33 (27.5%) | 12 (23.1%) |
| 15 years old | 27 (22.5%) | 17 (32.7%) |
| 16 years old | 40 (33.3%) | 13 (25%) |
| 17 years old | 20 (16.6%) | 10 (19.1%) |
| Oral Mucosa Pathology | Study Group | Total | |
|---|---|---|---|
| Girls | Boys | ||
| Geographic tongue | 8 (6.6%) | 6 (5%) | 11.6% |
| Herpes simplex lesions | 4 (3.3%) | 5 (4.2%) | 7.5% |
| Oral ulceration | 15 (12.5%) | 13 (10.8%) | 23.3% |
| Plaque-induced gingivitis | 32 (26.6%) | 43 (35.8%) | 62.4% |
| Chronic keratosis (Morsicatio buccarul) significant difference p < 0.01 | 28 (23.3%) | 4 (3.3%) | 26.6% |
| Oral Mucosa Pathology | Control Group | Total % | |
|---|---|---|---|
| Girls | Boys | ||
| Geographic tongue | 14 (26.9%) | 9 (17.3%) | 44.2% |
| Plaque-induced gingivitis | 10 (19.2%) | 16 (30.8%) | 50% |
| Oral Mucosa Pathology | Study Group Pain/Sensibility |
|---|---|
| Geographic tongue | Present 7 girls (10.6%) 5 boys (9.2%) |
| Herpes simplex lesions | Present 1 girl (1.5%) 2 boys (3.7%) |
| Oral ulceration | Present 2 girls (3%) 3 boys (5.5%) |
| Plaque-induced gingivitis | Present 16 girls (24.24%) 19 boys (35.2%) |
| Chronic keratosis (Morsicatio buccarul) | Present 9 girls (13.6%) 1 boy (1.9%) |
| Oral mucosa pathology | Control Group Pain/Sensibility |
| Geographic tongue | Present 8 girls (29.6%) 7 boys (28%) |
| Plaque-induced gingivitis | Present 5 girls (18.5%) 11 boys (44%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stoica, A.M.; Kovacs-Ivacson, C.A.; Stoica, O.E.; Beresescu, L.; Monea, M. Clinical and Pathological Manifestation of the Oral Mucosa in Institutionalized Children from Romania. Int. J. Environ. Res. Public Health 2022, 19, 15564. https://doi.org/10.3390/ijerph192315564
Stoica AM, Kovacs-Ivacson CA, Stoica OE, Beresescu L, Monea M. Clinical and Pathological Manifestation of the Oral Mucosa in Institutionalized Children from Romania. International Journal of Environmental Research and Public Health. 2022; 19(23):15564. https://doi.org/10.3390/ijerph192315564
Chicago/Turabian StyleStoica, Alexandra Mihaela, Csinszka Andrea Kovacs-Ivacson, Oana Elena Stoica, Liana Beresescu, and Monica Monea. 2022. "Clinical and Pathological Manifestation of the Oral Mucosa in Institutionalized Children from Romania" International Journal of Environmental Research and Public Health 19, no. 23: 15564. https://doi.org/10.3390/ijerph192315564
APA StyleStoica, A. M., Kovacs-Ivacson, C. A., Stoica, O. E., Beresescu, L., & Monea, M. (2022). Clinical and Pathological Manifestation of the Oral Mucosa in Institutionalized Children from Romania. International Journal of Environmental Research and Public Health, 19(23), 15564. https://doi.org/10.3390/ijerph192315564