
Burden and Risk Factors of Melioidosis in Southeast Asia: A Scoping Review


 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Selection of Studies
2.3. Data Extraction
3. Results
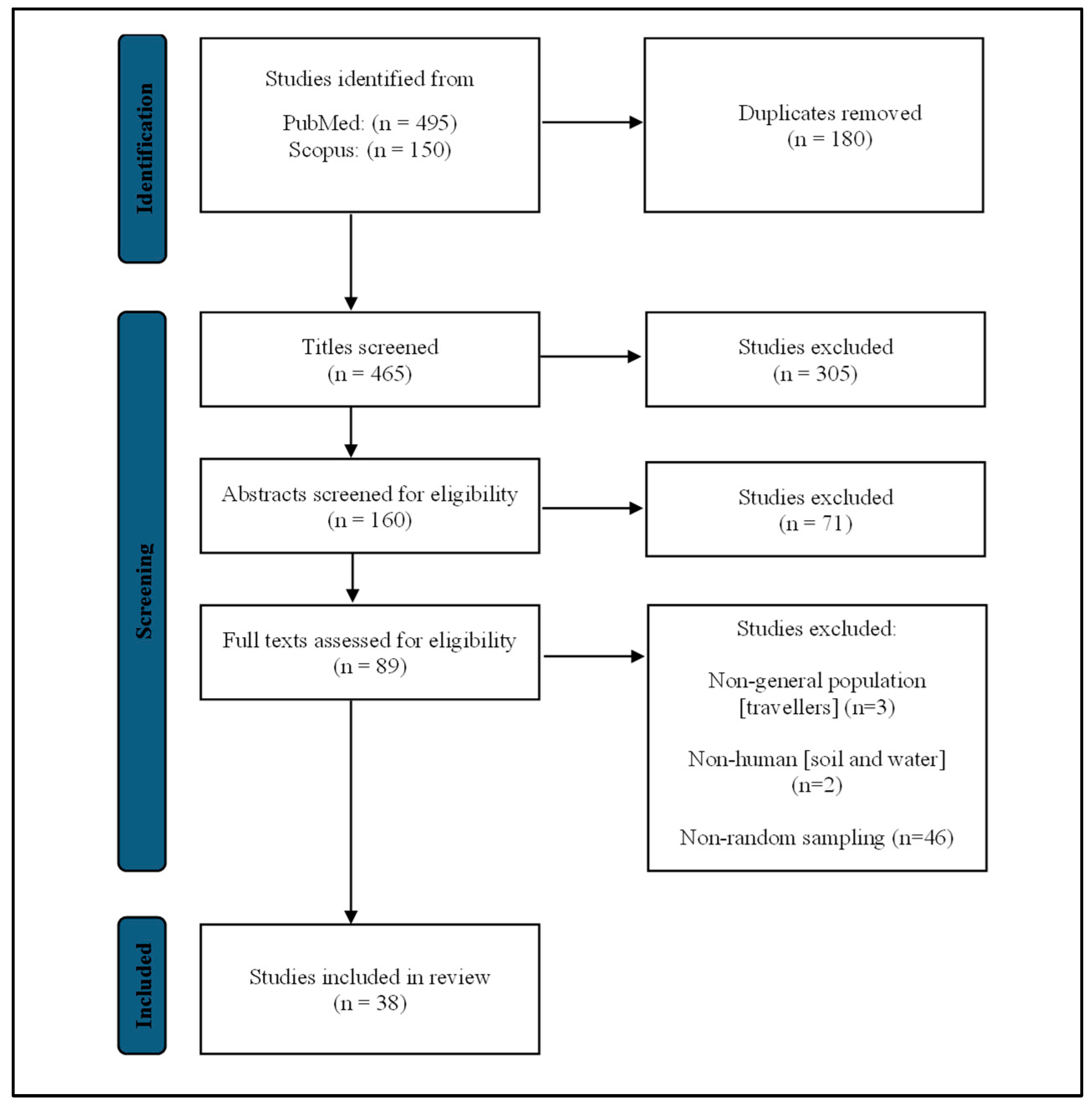
3.1. Search Results
3.2. Prevalence of Melioidosis
3.2.1. Disease Prevalence of Melioidosis
3.2.2. Seroprevalence of Melioidosis
3.3. Risk Factors of Melioidosis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Whitmore, A.; Krishnaswami, C.S. A Hitherto Undescribed Infective Disease in Rangoon. Indian Med. Gaz. 1912, 47, 262–267. [Google Scholar]
- Kaestli, M.; Schmid, M.; Mayo, M.; Rothballer, M.; Harrington, G.; Richardson, L.; Hill, A.; Hill, J.; Tuanyok, A.; Keim, P.; et al. Out of the ground: Aerial and exotic habitats of the melioidosis bacterium Burkholderia pseudomallei in grasses in Australia. Environ. Microbiol. 2012, 14, 2058–2070. [Google Scholar] [CrossRef] [PubMed]
- Wiersinga, W.J.; Virk, H.S.; Torres, A.G.; Currie, B.J.; Peacock, S.J.; Dance, D.A.B.; Limmathurotsakul, D. Melioidosis. Nat. Rev. Dis. Primers 2018, 4, 17107. [Google Scholar] [CrossRef] [PubMed]
- Karunanayake, P. Melioidosis: Clinical aspects. Clin. Med. 2022, 22, 6–8. [Google Scholar] [CrossRef] [PubMed]
- Currie, B.J.; Fisher, D.A.; Anstey, N.M.; Jacups, S.P. Melioidosis: Acute and chronic disease, relapse and re-activation. Trans. R. Soc. Trop. Med. Hyg. 2000, 94, 301–304. [Google Scholar] [CrossRef]
- Veluthat, C.; Venkatnarayan, K.; Padaki, P.; Krishnaswamy, U.M. Case of melioidosis misdiagnosed as pulmonary tuberculosis. BMJ Case Rep. 2021, 14, e242499. [Google Scholar] [CrossRef] [PubMed]
- Jamani, N.A.; Mohd Nor, F.H.; Yatim, Y. It is tuberculosis or melioidosis? A clinical diagnostic dilemma. Med. J. Malays. 2021, 76, 734–736. [Google Scholar]
- Vidyalakshmi, K.; Chakrapani, M.; Shrikala, B.; Damodar, S.; Lipika, S.; Vishal, S. Tuberculosis mimicked by melioidosis. Int. J. Tuberc. Lung Dis. Off. J. Int. Union Against Tuberc. Lung Dis. 2008, 12, 1209–1215. [Google Scholar]
- Vidyalakshmi, K.; Lipika, S.; Vishal, S.; Damodar, S.; Chakrapani, M. Emerging clinico-epidemiological trends in melioidosis: Analysis of 95 cases from western coastal India. Int. J. Infect. Dis. 2012, 16, e491–e497. [Google Scholar] [CrossRef]
- White, N.J. Melioidosis. Lancet 2003, 361, 1715–1722. [Google Scholar] [CrossRef]
- Limmathurotsakul, D.; Golding, N.; Dance, D.A.; Messina, J.P.; Pigott, D.M.; Moyes, C.L.; Rolim, D.B.; Bertherat, E.; Day, N.P.; Peacock, S.J.; et al. Predicted global distribution of Burkholderia pseudomallei and burden of melioidosis. Nat. Microbiol. 2016, 1, 15008. [Google Scholar] [CrossRef] [PubMed]
- Limmathurotsakul, D.; Wongratanacheewin, S.; Teerawattanasook, N.; Wongsuvan, G.; Chaisuksant, S.; Chetchotisakd, P.; Chaowagul, W.; Day, N.P.J.; Peacock, S.J. Increasing incidence of human melioidosis in Northeast Thailand. Am. J. Trop. Med. Hyg. 2010, 82, 1113–1117. [Google Scholar] [CrossRef] [PubMed]
- Hinjoy, S.; Hantrakun, V.; Kongyu, S.; Kaewrakmuk, J.; Wangrangsimakul, T.; Jitsuronk, S.; Saengchun, W.; Bhengsri, S.; Akarachotpong, T.; Thamthitiwat, S.; et al. Melioidosis in Thailand: Present and Future. Trop. Med. Infect. Dis. 2018, 3, 38. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Pang, L.; Sim, S.H.; Goh, K.T.; Ravikumar, S.; Win, M.S.; Tan, G.; Cook, A.R.; Fisher, D.; Chai, L.Y.A. Association of melioidosis incidence with rainfall and humidity, Singapore, 2003–2012. Emerg. Infect. Dis. 2015, 21, 159–162. [Google Scholar] [CrossRef] [PubMed]
- Leelarasamee, A. Melioidosis in Southeast Asia. Acta Trop. 2000, 74, 129–132. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Chaowagul, W.; White, N.J.; Dance, D.A.B.; Wattanagoon, Y.; Naigowit, P.; Davis, T.M.E.; Looareesuwan, S.; Pitakwatchara, N. Melioidosis: A Major Cause of Community-Acquired Septicemia in Northeastern Thailand. J. Infect. Dis. 1989, 159, 890–899. [Google Scholar] [CrossRef]
- Rattanaumpawan, P.; Ussavasodhi, P.; Kiratisin, P.; Aswapokee, N. Epidemiology of bacteremia caused by uncommon non-fermentative gram-negative bacteria. BMC Infect. Dis 2013, 13, 167. [Google Scholar] [CrossRef]
- Supatjaree, C.; Alan, G.; Kamolwish, L. Hepatic/splenic abscess and/or skin and soft tissue infection as predictors of melioidosis in children. J. Infect. Dev. Ctries. 2019, 13, 149–153. [Google Scholar] [CrossRef]
- Jatapai, A.; Gregory, C.J.; Thamthitiwat, S.; Tanwisaid, K.; Bhengsri, S.; Baggett, H.C.; Sangwichian, O.; Jorakate, P.; MacArthur, J.R. Hospitalized Bacteremic Melioidosis in Rural Thailand: 2009–2013. Am. J. Trop. Med. Hyg. 2018, 98, 1585–1591. [Google Scholar] [CrossRef]
- Suntornsut, P.; Kasemsupat, K.; Silairatana, S.; Wongsuvan, G.; Jutrakul, Y.; Wuthiekanun, V.; Day, N.P.J.; Peacock, S.J.; Limmathurotsakul, D. Prevalence of melioidosis in patients with suspected pulmonary tuberculosis and sputum smear negative for acid-fast bacilli in northeast Thailand. Am. J. Trop Med. Hyg 2013, 89, 983–985. [Google Scholar] [CrossRef] [PubMed]
- Teparrukkul, P.; Nilsakul, J.; Dunachie, S.; Limmathurotsakul, D. Clinical Epidemiology of Septic Arthritis Caused by Burkholderia pseudomallei and Other Bacterial Pathogens in Northeast Thailand. Am. J. Trop. Med. Hyg. 2017, 97, 1695–1701. [Google Scholar] [CrossRef]
- Hinjoy, S.; Wacharapluesadee, S.; Iamsirithaworn, S.; Smithsuwan, P.; Padungtod, P. Zoonotic and vector borne agents causing disease in adult patients hospitalized due to fever of unknown origin in Thailand. Asian Pac. J. Trop. Dis. 2017, 7, 577–581. [Google Scholar] [CrossRef]
- Hantrakun, V.; Somayaji, R.; Teparrukkul, P.; Boonsri, C.; Rudd, K.; Day, N.P.J.; West, T.E.; Limmathurotsakul, D. Clinical epidemiology and outcomes of community acquired infection and sepsis among hospitalized patients in a resource limited setting in Northeast Thailand: A prospective observational study (Ubon-sepsis). PLoS ONE 2018, 13, e0204509. [Google Scholar] [CrossRef]
- Srivanitchapoom, C.; Yata, K. Suppurative cervical lymphadenitis in adult: An analysis of predictors for surgical drainage. Auris Nasus Larynx 2020, 47, 887–894. [Google Scholar] [CrossRef]
- Teawtrakul, N.; Jetsrisuparb, A.; Sirijerachai, C.; Chansung, K.; Wanitpongpun, C. Severe bacterial infections in patients with non-transfusion-dependent thalassemia: Prevalence and clinical risk factors. Int. J. Infect. Dis. 2015, 39, 53–56. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Kasper, M.R.; Blair, P.J.; Touch, S.; Sokhal, B.; Yasuda, C.Y.; Williams, M.; Richards, A.L.; Burgess, T.H.; Wierzba, T.F.; Putnam, S.D. Infectious etiologies of acute febrile illness among patients seeking health care in south-central Cambodia. Am. J. Trop. Med. Hyg. 2012, 86, 246–253. [Google Scholar] [CrossRef]
- Rammaert, B.; Beauté, J.; Borand, L.; Hem, S.; Buchy, P.; Goyet, S.; Overtoom, R.; Angebault, C.; Te, V.; Try, P.L.; et al. Pulmonary melioidosis in Cambodia: A prospective study. BMC Infect. Dis. 2011, 11, 126. [Google Scholar] [CrossRef] [PubMed]
- Stoesser, N.; Pocock, J.; Moore, C.E.; Soeng, S.; Chhat, H.P.; Sar, P.; Limmathurotsakul, D.; Day, N.; Thy, V.; Sar, V.; et al. Pediatric suppurative parotitis in Cambodia between 2007 and 2011. Pediatr. Infect. Dis. J. 2012, 31, 865–868. [Google Scholar] [CrossRef]
- Chheng, K.; Carter, M.J.; Emary, K.; Chanpheaktra, N.; Moore, C.E.; Stoesser, N.; Putchhat, H.; Sona, S.; Reaksmey, S.; Kitsutani, P.; et al. A prospective study of the causes of febrile illness requiring hospitalization in children in Cambodia. PLoS ONE 2013, 8, e60634. [Google Scholar] [CrossRef]
- Schully, K.L.; Berjohn, C.M.; Prouty, A.M.; Fitkariwala, A.; Som, T.; Sieng, D.; Gregory, M.J.; Vaughn, A.; Kheng, S.; Te, V.; et al. Melioidosis in lower provincial Cambodia: A case series from a prospective study of sepsis in Takeo Province. PLoS Negl. Trop. Dis. 2017, 11, e0005923. [Google Scholar] [CrossRef]
- Pho, Y.; Nhem, S.; Sok, C.; By, B.; Phann, D.; Nob, H.; Thann, S.; Yin, S.; Kim, C.; Letchford, J.; et al. Melioidosis in patients with suspected tuberculosis in Cambodia: A single-center cross-sectional study. Int. J. Tuberc. Lung Dis. Off. J. Int. Union Against Tuberc. Lung Dis. 2018, 22, 1481–1485. [Google Scholar] [CrossRef]
- Aung, M.K.; Mar, T.T. Re-emergence of melioidosis in Myanmar. Trans. R. Soc. Trop. Med. Hyg. 2008, 102, S10–S11. [Google Scholar] [CrossRef]
- Myat, T.O.; Oo, K.M.; Mone, H.K.; Htike, W.W.; Biswas, A.; Hannaway, R.F.; Murdoch, D.R.; Ussher, J.E.; Crump, J.A. A prospective study of bloodstream infections among febrile adolescents and adults attending Yangon General Hospital, Yangon, Myanmar. PLoS Negl. Trop. Dis. 2020, 14, e0008268. [Google Scholar] [CrossRef]
- Ye Lynn, K.L.; Hanson, J.; Mon, N.C.N.; Yin, K.N.; Nyein, M.L.; Thant, K.Z.; Kyi, M.M.; Oo, T.Z.C.; Aung, N.M. The clinical characteristics of patients with sepsis in a tertiary referral hospital in Yangon, Myanmar. Trans. R. Soc. Trop. Med. Hyg. 2019, 113, 81–90. [Google Scholar] [CrossRef]
- Win, M.M.; Win, K.K.N.; Wah, T.T.; Aye, S.N.; Htwe, T.T.; Zin, K.N.; Aung, M.T.; Aung, W.W.; Ashley, E.A.; Smithuis, F.; et al. Enhanced melioidosis surveillance in patients attending four tertiary hospitals in Yangon, Myanmar. Epidemiol. Infect. 2021, 149, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Warrell, C.E.; Phyo, A.P.; Win, M.M.; McLean, A.R.D.; Watthanaworawit, W.; Swe, M.M.M.; Soe, K.; Lin, H.N.; Aung, Y.Y.; Ko, C.K.; et al. Observational study of adult respiratory infections in primary care clinics in Myanmar: Understanding the burden of melioidosis, tuberculosis and other infections not covered by empirical treatment regimes. Trans. R. Soc. Trop. Med. Hyg. 2021, 115, 914–921. [Google Scholar] [CrossRef] [PubMed]
- Thabit, A.; Mutalip, M.; Kamil, W.M.; Din, M.; Arumugam, M.; Azman, S.; Jaafar, R.; Singh, S.; Abdullah, R.; Muhammad, E.; et al. Etiologies of tropical acute febrile illness in West Pahang, Malaysia: A prospective observational study. Asian Pac. J. Trop. Med. 2020, 13, 115–122. [Google Scholar] [CrossRef]
- Parry, C.M.; Wuthiekanun, V.; Hoa, N.T.T.; Diep, T.S.; Thao, L.T.T.; Loc, P.V.; Wills, B.A.; Wain, J.; Hien, T.T.; White, N.J.; et al. Melioidosis in Southern Vietnam: Clinical Surveillance and Environmental Sampling. Clin. Infect. Dis. 1999, 29, 1323–1326. [Google Scholar] [CrossRef] [PubMed]
- Takeshita, N.; Anh, N.Q.; Phuong, D.M.; Thanh, D.V.; Thuy, P.P.; Huong, M.T.L.; Takahashi, M.; Ohmagari, N. Assessment of Bacteremia in a Large Tertiary Care Hospital in Northern Vietnam: A Single-Center Retrospective Surveillance Study. Jpn. J. Infect. Dis. 2019, 72, 118–120. [Google Scholar] [CrossRef]
- Dat, V.Q.; Vu, H.N.; Nguyen The, H.; Nguyen, H.T.; Hoang, L.B.; Vu Tien Viet, D.; Bui, C.L.; Van Nguyen, K.; Nguyen, T.V.; Trinh, D.T.; et al. Bacterial bloodstream infections in a tertiary infectious diseases hospital in Northern Vietnam: Aetiology, drug resistance, and treatment outcome. BMC Infect. Dis. 2017, 17, 493. [Google Scholar] [CrossRef]
- Poulose, V. Severe community-acquired pneumonia requiring intensive care: A study of 80 cases from Singapore. Singap. Med. J. 2008, 49, 458–461. [Google Scholar]
- Kanai, K.; Kurata, T.; Akksilp, S.; Auwanit, W.; Chaowagul, V.; Naigowit, P. A preliminary survey for human immunodeficient virus (HIV) infections in tuberculosis and melioidosis patients in Ubon Ratchathani, Thailand. Jpn. J. Med. Sci. Biol. 1992, 45, 247–253. [Google Scholar] [CrossRef][Green Version]
- Wuthiekanun, V.; Chierakul, W.; Rattanalertnavee, J.; Langa, S.; Sirodom, D.; Wattanawaitunechai, C.; Winothai, W.; White, N.J.; Day, N.; Peacock, S.J. Serological evidence for increased human exposure to Burkholderia pseudomallei following the tsunami in southern Thailand. J. Clin. Microbiol. 2006, 44, 239–240. [Google Scholar] [CrossRef] [PubMed]
- Suttisunhakul, V.; Hip, P.; Ouch, P.; Ly, P.; Supaprom, C.; Rachmat, A.; Prouty, M.; Vaughn, A.; Eltayeb, A.; Kheng, S.; et al. Retrospective Analysis of Fever and Sepsis Patients from Cambodia Reveals Serological Evidence of Melioidosis. Am. J. Trop. Med. Hyg. 2018, 98, 1039–1045. [Google Scholar] [CrossRef]
- Win, Z.Z.; Phokrai, P.; Aung, Z.; Zaw, T.; Burtnick, M.N.; Chantratita, N.; Brett, P.J.; Hlaing, T.M. Use of Rapid Enzyme-Linked Immunosorbent Assays for Serological Screening of Melioidosis in Myanmar. Am. J. Trop. Med. Hyg. 2018, 98, 1300–1302. [Google Scholar] [CrossRef]
- Sapian, M.; Khair, M.T.; How, S.H.; Rajalingam, R.; Sahhir, K.; Norazah, A.; Khebir, V.; Jamalludin, A.R. Outbreak of melioidosis and leptospirosis co-infection following a rescue operation. Med. J. Malays. 2012, 67, 293–297. [Google Scholar]
- Hii, S.F.F.; Kee, C.C.; Ahmad, N. Melioidosis: Overview of seropositivity in Malaysia. Trop. Biomed. 2016, 33, 697–701. [Google Scholar] [PubMed]
- Hadi, F.S.; Ghazali, S.; Ahmad, N.; Ramli, S.R. Trend and pattern of melioidosis seropositivity among suspected patients in Malaysia 2015—2019. Trop. Biomed. 2021, 38, 561–567. [Google Scholar] [CrossRef] [PubMed]
- Embi, N.; Suhaimi, A.; Mohamed, R.; Ismail, G. Prevalence of Antibodies to Pseudomonas pseudomallei Exotoxin and Whole Cell Antigens in Military Personnel in Sabah and Sarawak, Malaysia. Microbiol. Immunol. 1992, 36, 899–904. [Google Scholar] [CrossRef] [PubMed]
- Ng, C.Y.; Leong, E.C.; Chng, H.C. Ten-year series of splenic abscesses in a general hospital in Singapore. Ann. Acad. Med. Singap. 2008, 37, 749–752. [Google Scholar] [PubMed]
- Suputtamongkol, Y.; Chaowagul, W.; Chetchotisakd, P.; Lertpatanasuwun, N.; Intaranongpai, S.; Ruchutrakool, T.; Budhsarawong, D.; Mootsikapun, P.; Wuthiekanun, V.; Teerawatasook, N.; et al. Risk Factors for Melioidosis and Bacteremic Melioidosis. Clin. Infect. Dis. 1999, 29, 408–413. [Google Scholar] [CrossRef]
- Limmathurotsakul, D.; Kanoksil, M.; Wuthiekanun, V.; Kitphati, R.; de Stavola, B.; Day, N.P.J.; Peacock, S.J. Activities of daily living associated with acquisition of melioidosis in northeast Thailand: A matched case-control study. PLoS Negl. Trop. Dis. 2013, 7, e2072. [Google Scholar] [CrossRef]
- Abu Hassan, M.R.; Aziz, N.; Ismail, N.; Shafie, Z.; Mayala, B.; Donohue, R.E.; Pani, S.P.; Michael, E. Socio-epidemiological and land cover risk factors for melioidosis in Kedah, Northern Malaysia. PLoS Negl. Trop. Dis. 2019, 13, e0007243. [Google Scholar] [CrossRef]
- Birnie, E.; Virk, H.S.; Savelkoel, J.; Spijker, R.; Bertherat, E.; Dance, D.A.B.; Limmathurotsakul, D.; Devleesschauwer, B.; Haagsma, J.A.; Wiersinga, W.J. Global burden of melioidosis in 2015: A systematic review and data synthesis. Lancet Infect. Dis. 2019, 19, 892–902. [Google Scholar] [CrossRef]
- Savelkoel, J.; Dance, D.A.B.; Currie, B.J.; Limmathurotsakul, D.; Wiersinga, W.J. A call to action: Time to recognise melioidosis as a neglected tropical disease. Lancet Infect. Dis. 2022, 22, e176–e182. [Google Scholar] [CrossRef]
- Marshall, S.W. Prevalence and Incidence. In Encyclopedia of Social Measurement; Kempf-Leonard, K., Ed.; Elsevier: New York, NY, USA, 2005; pp. 141–147. [Google Scholar] [CrossRef]
- Win, M.M.; Ashley, E.A.; Zin, K.N.; Aung, M.T.; Swe, M.M.M.; Ling, C.L.; Nosten, F.; Thein, W.M.; Zaw, N.N.; Aung, M.Y.; et al. Melioidosis in Myanmar. Trop. Med. Infect. Dis. 2018, 3, 28. [Google Scholar] [CrossRef]
- Trinh, T.T.; Nguyen, L.D.N.; Nguyen, T.V.; Tran, C.X.; Le, A.V.; Nguyen, H.V.; Assig, K.; Lichtenegger, S.; Wagner, G.E.; Do, C.D.; et al. Melioidosis in Vietnam: Recently Improved Recognition but still an Uncertain Disease Burden after Almost a Century of Reporting. Trop. Med. Infect. Dis. 2018, 3, 39. [Google Scholar] [CrossRef] [PubMed]
- Trinh, T.T.; Hoang, T.S.; Tran, D.A.; Trinh, V.T.; Göhler, A.; Nguyen, T.T.; Hoang, S.N.; Krumkamp, R.; Nguyen, L.T.N.; May, J.; et al. A simple laboratory algorithm for diagnosis of melioidosis in resource-constrained areas: A study from north-central Vietnam. Clin. Microbiol. Infect. 2018, 24, 84.e81–84.e84. [Google Scholar] [CrossRef] [PubMed]
- Cheng, A.C.; Currie, B.J. Melioidosis: Epidemiology, pathophysiology, and management. Clin. Microbiol. Rev. 2005, 18, 383–416. [Google Scholar] [CrossRef] [PubMed]
- Sim, S.H.; Ong, C.E.; Gan, Y.H.; Wang, D.; Koh, V.W.; Tan, Y.K.; Wong, M.S.; Chew, J.S.; Ling, S.F.; Tan, B.Z.; et al. Melioidosis in Singapore: Clinical, Veterinary, and Environmental Perspectives. Trop. Med. Infect. Dis. 2018, 3, 31. [Google Scholar] [CrossRef] [PubMed]
- Limmathurotsakul, D.; Dance, D.A.B.; Wuthiekanun, V.; Kaestli, M.; Mayo, M.; Warner, J.; Wagner, D.M.; Tuanyok, A.; Wertheim, H.; Yoke Cheng, T.; et al. Systematic review and consensus guidelines for environmental sampling of Burkholderia pseudomallei. PLoS Negl. Trop. Dis. 2013, 7, e2105. [Google Scholar] [CrossRef] [PubMed]
- Wiersinga, W.J.; van der Poll, T.; White, N.J.; Day, N.P.; Peacock, S.J. Melioidosis: Insights into the pathogenicity of Burkholderia pseudomallei. Nat. Rev. Microbiol. 2006, 4, 272–282. [Google Scholar] [CrossRef] [PubMed]
- Zueter, A.; Yean, C.Y.; Abumarzouq, M.; Rahman, Z.A.; Deris, Z.Z.; Harun, A. The epidemiology and clinical spectrum of melioidosis in a teaching hospital in a North-Eastern state of Malaysia: A fifteen-year review. BMC Infect. Dis. 2016, 16, 333. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.-S.; Chen, Y.-S.; Lin, H.-H.; Liu, P.-J.; Ni, W.-F.; Hsueh, P.-T.; Liang, S.-H.; Chen, C.; Chen, Y.-L. Airborne Transmission of Melioidosis to Humans from Environmental Aerosols Contaminated with B. pseudomallei. PLoS Negl. Trop. Dis. 2015, 9, e0003834. [Google Scholar] [CrossRef] [PubMed]
- Tang, R.Y.; Lim, S.H.; Lam, J.E.; Nurasykin, S.; Eileen, T.; Chan, Y.W. A 5-year retrospective study of melioidosis cases treated in a district specialist hospital. Med. J. Malays. 2019, 74, 472–476. [Google Scholar]
- Chowdhury, S.; Barai, L.; Afroze, S.R.; Ghosh, P.K.; Afroz, F.; Rahman, H.; Ghosh, S.; Hossain, M.B.; Rahman, M.Z.; Das, P.; et al. The Epidemiology of Melioidosis and Its Association with Diabetes Mellitus: A Systematic Review and Meta-Analysis. Pathogens 2022, 11, 149. [Google Scholar] [CrossRef]
- Chanchamroen, S.; Kewcharoenwong, C.; Susaengrat, W.; Ato, M.; Lertmemongkolchai, G. Human polymorphonuclear neutrophil responses to Burkholderia pseudomallei in healthy and diabetic subjects. Infect. Immun. 2009, 77, 456–463. [Google Scholar] [CrossRef] [PubMed]
- Jabbar, Z.; Currie, B.J. Melioidosis and the kidney. Nephrology 2013, 18, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Fong, S.M.; Wong, K.J.; Fukushima, M.; Yeo, T.W. Thalassemia Major Is a Major Risk Factor for Pediatric Melioidosis in Kota Kinabalu, Sabah, Malaysia. Clin. Infect. Dis. 2015, 60, 1802–1807. [Google Scholar] [CrossRef]
- Limmathurotsakul, D.; Wongsuvan, G.; Aanensen, D.; Ngamwilai, S.; Saiprom, N.; Rongkard, P.; Thaipadungpanit, J.; Kanoksil, M.; Chantratita, N.; Day, N.P.J.; et al. Melioidosis caused by Burkholderia pseudomallei in drinking water, Thailand, 2012. Emerg. Infect. Dis. 2014, 20, 265–268. [Google Scholar] [CrossRef]
- Hackshaw, A. Small studies: Strengths and limitations. Eur. Respir. J. 2008, 32, 1141. [Google Scholar] [CrossRef]
- Hoffmaster, A.R.; AuCoin, D.; Baccam, P.; Baggett, H.C.; Baird, R.; Bhengsri, S.; Blaney, D.D.; Brett, P.J.; Brooks, T.J.G.; Brown, K.A.; et al. Melioidosis diagnostic workshop, 2013. Emerg. Infect. Dis. 2015, 21, e141045. [Google Scholar] [CrossRef]
- Limmathurotsakul, D.; Jamsen, K.; Arayawichanont, A.; Simpson, J.A.; White, L.J.; Lee, S.J.; Wuthiekanun, V.; Chantratita, N.; Cheng, A.; Day, N.P.J.; et al. Defining the true sensitivity of culture for the diagnosis of melioidosis using Bayesian latent class models. PLoS ONE 2010, 5, e12485. [Google Scholar] [CrossRef] [PubMed]
- Wongsuvan, G.; Hantrakun, V.; Teparrukkul, P.; Imwong, M.; West, T.E.; Wuthiekanun, V.; Day, N.P.; AuCoin, D.; Limmathurotsakul, D. Sensitivity and specificity of a lateral flow immunoassay (LFI) in serum samples for diagnosis of melioidosis. Trans. R. Soc. Trop. Med. Hyg. 2018, 112, 568–570. [Google Scholar] [CrossRef] [PubMed]
- Jayakumar, E. Molecular detection of Burkholderia pseudomallei in patients with suspected pulmonary and extra pulmonary tuberculosis. J. Microbiol. Infect. Dis. 2017, 7, 21–28. [Google Scholar] [CrossRef][Green Version]
- Patel, T.S.; Kaakeh, R.; Nagel, J.L.; Newton, D.W.; Stevenson, J.G. Cost analysis of implementing matrix-assisted laser desorption ionization–time of flight mass spectrometry plus real-time antimicrobial stewardship intervention for bloodstream infections. J. Clin. Microbiol. 2017, 55, 60–67. [Google Scholar] [CrossRef] [PubMed]
- Gilmore, G.; Barnes, J.; Ketheesan, N.; Norton, R. Use of antigens derived from Burkholderia pseudomallei, B. thailandensis, and B. cepacia in the indirect hemagglutination assay for melioidosis. Clin. Vaccine Immunol. 2007, 14, 1529–1531. [Google Scholar] [CrossRef] [PubMed]
- Cheng, A.C.; O’Brien, M.; Freeman, K.; Lum, G.; Currie, B.J. Indirect hemagglutination assay in patients with melioidosis in northern Australia. Am. J. Trop. Med. Hyg. 2006, 74, 330–334. [Google Scholar] [CrossRef]
- van Crevel, R.; van de Vijver, S.; Moore, D.A.J. The global diabetes epidemic: What does it mean for infectious diseases in tropical countries? Lancet Diabetes Endocrinol. 2017, 5, 457–468. [Google Scholar] [CrossRef]
- Dunachie, S.; Chamnan, P. The double burden of diabetes and global infection in low and middle-income countries. Trans. R. Soc. Trop. Med. Hyg. 2019, 113, 56–64. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Year of Study | Study Area | Study Design | Sample Size (n) | Prevalence (%) | Diagnostic Assay | Target Population | Reference |
|---|---|---|---|---|---|---|---|---|
| 1. | 1986–1987 | Thailand (Northeast) | CS | 225 | 24.7 | Blood culture | Patients with CAS | [17] |
| 2. | 2007–2008 | Thailand (Central) | CS | 221 | 2.7 | Blood culture | Patients infected with NFGNB | [18] |
| 3. | 2002–2014 | Thailand (South) | CS | 145 | 11.0 | Culture | Patients with suspected melioidosis | [19] |
| 4. | 2009–2013 | Thailand (Northeast) | CS | 2031 | 28.3 | Blood culture | Patients had a presumed pathogen isolated | [20] |
| 5. | 2012–2013 | Thailand (Northeast) | CS | 118 | 2.5 | Sputum culture | Patients with suspected pulmonary tuberculosis | [21] |
| 6. | 2012–2014 | Thailand (Northeast) | CS | 154 | 48.0 | Blood and synovial fluid culture | Culture-confirmed bacterial septic arthritis patients | [22] |
| 7. | 2013–2015 | Thailand | CS | 463 | 0.5 | Multiplex real-time PCR (whole blood) | Patients with a fever (agricultural communities) | [23] |
| 8. | 2013–2017 | Thailand (Northeast) | CS | 4989 | 3.0 | Blood culture | Patients with community-acquired infection | [24] |
| 9. | 2014–2019 | Thailand | CS | 41 | 2.4 | Pus culture | Patients with SCL | [25] |
| 10. | NR | Thailand (Northeast) | CS | 211 | 1.4 | Blood and pus culture | Patients with NTDT | [26] |
| 11. | 2006–2009 | Cambodia | CS | 9821 | 0.02 | Blood culture | Patients with AFI | [27] |
| 12. | 2007–2010 | Cambodia (Takeo and Kampong Cham) | CS | 2407 | 1.6 | Blood and sputum culture | Patients with ALRI | [28] |
| 13. | 2007–2011 | Cambodia (Siem Reap) | CS | 39 | 74.4 | Parotid culture | Children with suppurative parotitis | [29] |
| 14. | 2009–2010 | Cambodia (Siem Reap) | CS | 1180 | 0.5 | Blood culture | Febrile children | [30] |
| 15. | 2014–2015 | Cambodia (Takeo) | CS | 139 | 5.0 | Blood and sputum culture | Patients with SIRS | [31] |
| 16. | 2015 | Cambodia (Kampong Cham) | CS | 404 | 1.0 | Sputum culture | Patients with suspected tuberculosis | [32] |
| 17. | 2004–2006 | Myanmar (Yangon) | CS | 133 | 2.3 | Pus culture | Patients with abscess | [33] |
| 18. | 2015–2016 | Myanmar (Yangon) | CS | 90 | 1.1 | Blood culture, VITEK2, and LA | Patients with BSI | [34] |
| 19. | 2016–2017 | Myanmar (Yangon) | CS | 120 | 0.83 | Blood culture | Patients with fever and dysfunction of at least two organ systems | [35] |
| 20. | 2017–2019 | Myanmar (Yangon) | CS | 364 | 5.7 | Culture, LA, API 20 NE, antibiotic susceptibility testing and molecular confirmation | Patients infected with oxidase-positive Gram-negative rods | [36] |
| 21. | 2018–2019 | Myanmar (Yangon) | CS | 299 | 0.33 | Sputum culture and antigen detection (AMD-LFA) | Patients presenting with fever and productive cough | [37] |
| 22. | 2016 | Malaysia (Pahang) | CS | 336 | 6.0 | Blood, sputum, tissue, pus aspirate, and body fluid aspirate culture | Patients with AFI | [38] |
| 23. | 1992–1998 | Vietnam (South) | CS | 3653 | 0.25 | Blood culture | Hospitalized patients | [39] |
| 24. | 2005–2009 | Vietnam (North) | CS | 7428 | 0.7 | Blood culture | Patients with bacteraemia | [40] |
| 25. | 2011–2013 | Vietnam (North) | CS | 738 | 2.0 | Blood culture | Patients with BSI | [41] |
| 26. | 2003–2005 | Singapore | CS | 80 | 5.0 | Respiratory specimen culture | Patients admitted to the medical ICU with CAP | [42] |
| No. | Year of Study | Study Area | Study Design | Sample Size (n) | Prevalence (%) | Diagnostic Assay | Target Population | Reference |
|---|---|---|---|---|---|---|---|---|
| 1. | 1992 | Thailand (Northeast) | CS | 439 | 5.0 | Antibody detection (IHA 1:160; IFA-IgM 1:8 and IFA-IgG 1:32) | Culture-positive tuberculous patients | [43] |
| 2. | 2005 | Thailand (South) | CS | 52 | 63.5 (≥1:10) and 13.5 (≥1:160) | Antibody detection (IHA ≥1:10 and ≥ 1:160) | Tsunami survivors | [44] |
| 3. | 2002–2014 | Thailand (South) | CS | 145 | 11.0 | Antibody detection (IFA-IgM ≥ 1:20 and IHA ≥ 1:160) | Patients with suspected melioidosis | [19] |
| 4. | 2005 and 2014–2015 | Cambodia | CS | 1316 | 12.0 | Antibody detection (ELISA-IgG using OPS 1: 2000) | Patients with fever or sepsis of unknown origin | [45] |
| 5. | 2016 | Myanmar (delta region during the rainy season) | CS | 124 | 3.2 | Antibody detection (ELISA using OPS and Hcp1 1: 2000) | Febrile patients | [46] |
| 6. | 2010 | Malaysia (Pahang) | CS | 153 | 7.2 | Antibody detection (IFA-IgM ≥ 1:80 or four-fold rise in IgM) | People involved in the search and rescue operation for a drowned victim with a fever | [47] |
| 7. | 2013–2014 | Malaysia | CS | 17,234 | 10.5 | Antibody detection (IFA-IgM using the whole-cell antigen ≥ 1:160) | Patients with suspected melioidosis | [48] |
| 8. | 2015–2019 | Malaysia | CS | 26,665 | 16.4 | Antibody detection (IFA-IgM ≥ 1:160 and ELISA-IgM ≥ 1:320) | Patients with suspected melioidosis | [49] |
| 9. | NR | Malaysia (Sabah and Sarawak) | CS | 420 | 54.4 (exotoxin) and 65.7 (whole-cell antigens) | Antibody detection (ELISA using exotoxin and whole-cell antigens) | Military personnel | [50] |
| 10. | 1996–2005 | Singapore | CS | 21 | 71.4 | Antibody detection | Patients with radiological evidence of splenic abscess | [51] |
| No. | Year of Study | Study Area | Study Design | Sample Size (n) | Risk Factor (OR) | Diagnostic Assay | Target Population | Reference |
|---|---|---|---|---|---|---|---|---|
| 1 | 1997 | Thailand (Northeast) | CC | 580 | High soil and water exposure (3.3) Moderate soil and water exposure (2.1) Diabetes mellitus (5.9) Hematologic or solid tumour (0.4) Pre-existing renal disease (2.9) Thalassaemic disease (10.2) Diabetes and occupation involving high (8.5) and moderate soil and water exposure (5.6) | Blood, urine, sputum, pus, and throat swab culture | Patients with suspected bacteraemia | [52] |
| 2 | 2010–2011 | Thailand (Northeast) | CC | 800 | Working in a rice field (2.1) Other activities involving exposure to soil or water (1.4) Open wound (2.0) Eating food contaminated with soil or dust (1.5) Drinking untreated water (1.7) Outdoor exposure to dust clouds (1.3) Outdoor exposure to rain (2.1) Water inhalation (2.4) Current smoking (1.5) Steroid intake (3.1) | Blood culture | Hospitalized patients | [53] |
| 3 | 2005–2011 | Malaysia (Kedah) | CC | 484 | Diabetes mellitus (3.46) Chronic renal failure (4.04) Other diseases (chronic lung failure, HIV, and immunocompromised states) (1.2) | Blood and other body fluids culture | Hospitalized patients | [54] |
| 4 | 2013–2014 | Malaysia | CS | 17,234 | Gender: female (1.12) | Antibody (IgM) detection (IFA ≥ 1:160) | Patients with suspected melioidosis | [48] |
| Age group: <15 (4.71); 15–24 (2.82); 25–34 (2.21); 35–4; (2.05); and 45–54 (1.62) | ||||||||
| Ethnicity: Malay (0.92); Indians (1.20); Orang Asli (1.17); Sabah native (1.61); Sarawak native (1.27); and non-Malaysian (1.37) | ||||||||
| Region: northern (1.32); southern (1.28); eastern coast (1.47); Sabah (0.90); and Sarawak (1.46) | ||||||||
| 5 | 2015–2019 | Malaysia | CS | 26,665 | Gender: female (1.05) | Antibody (IgM) detection (IFA ≥ 1:160 and ELISA ≥ 1:320) | Patients with suspected melioidosis | [49] |
| Age group: <15 (3.04); 15–24 (2.99); 25–34 (2.59); 35–44 (1.98); and 45–54 (1.32) | ||||||||
| Region: northern (1.17); southern (0.91); eastern (1.17); Sabah (1.61); and Sarawak (1.75) | ||||||||
| Race: Malay (1.27); Indian (1.23); Orang Asli (1.78); Bumiputera Sarawak (2.04); Bumiputera Sabah (1.90); and others (1.52) | ||||||||
| Previous exposure: history of swimming in the river (4.39) and history of soil contact (1.02) | ||||||||
| Underlying diseases: diabetes mellitus (0.73); hypertension (0.60); chronic kidney disease (0.56); thalassemia (1.34); chronic lung disease (3.60); hepatitis (4.43); retroviral disease (1.31); and malignancy (1.27) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Selvam, K.; Ganapathy, T.; Najib, M.A.; Khalid, M.F.; Abdullah, N.A.; Harun, A.; Wan Mohammad, W.M.Z.; Aziah, I. Burden and Risk Factors of Melioidosis in Southeast Asia: A Scoping Review. Int. J. Environ. Res. Public Health 2022, 19, 15475. https://doi.org/10.3390/ijerph192315475
Selvam K, Ganapathy T, Najib MA, Khalid MF, Abdullah NA, Harun A, Wan Mohammad WMZ, Aziah I. Burden and Risk Factors of Melioidosis in Southeast Asia: A Scoping Review. International Journal of Environmental Research and Public Health. 2022; 19(23):15475. https://doi.org/10.3390/ijerph192315475
Chicago/Turabian StyleSelvam, Kasturi, Thanasree Ganapathy, Mohamad Ahmad Najib, Muhammad Fazli Khalid, Nor Azlina Abdullah, Azian Harun, Wan Mohd Zahiruddin Wan Mohammad, and Ismail Aziah. 2022. "Burden and Risk Factors of Melioidosis in Southeast Asia: A Scoping Review" International Journal of Environmental Research and Public Health 19, no. 23: 15475. https://doi.org/10.3390/ijerph192315475
APA StyleSelvam, K., Ganapathy, T., Najib, M. A., Khalid, M. F., Abdullah, N. A., Harun, A., Wan Mohammad, W. M. Z., & Aziah, I. (2022). Burden and Risk Factors of Melioidosis in Southeast Asia: A Scoping Review. International Journal of Environmental Research and Public Health, 19(23), 15475. https://doi.org/10.3390/ijerph192315475