



Assessment of Health-Related Quality of Life, Medication Adherence, and Prevalence of Depression in Kidney Failure Patients
 , , ,
, , ,  ,
,  , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Inclusion and Exclusion Criteria
2.3. Tools
2.4. Sociodemographic Data Sheet
2.5. Laboratory Investigation Assessment Datasheet
2.6. Assessment of Depression, HRQOL, and Medication Adherence
2.7. Kidney Disease Quality of Life-Short Form (KDQOL-SF-36)
2.8. Hamilton Depression Rating Scale Urdu Version (HAM-D-U)
- No depression at all: <8
- Mild (subthreshold): 8–13
- Moderate (mild): 14–18
- Severe (moderate): 19–22
- Very severe (severe): >23
2.9. Morisky Levine Greens Adherence Scales (MLGS)
2.10. Study Flow
2.11. Ethical Approval and Consent to Participate
2.12. Statistical Analysis
3. Result
3.1. Patient Characteristics
3.2. Laboratory Parameters
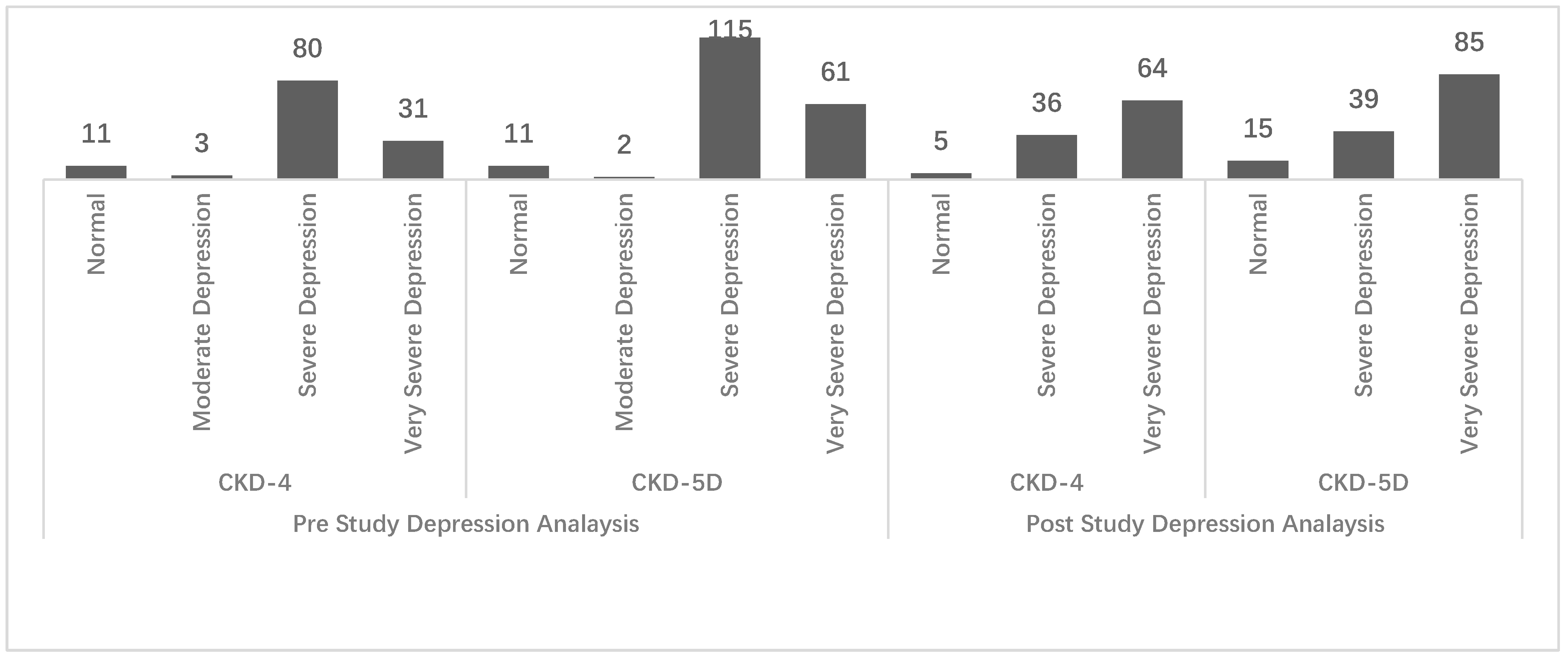
3.3. Depression
3.4. Medication Adherence
3.5. HRQOL
3.6. Medication Adherence and HRQOL
3.7. Depression and HRQOL
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jankowski, J.; Floege, J.; Fliser, D.; Böhm, M.; Marx, N. Cardiovascular disease in chronic kidney disease: Pathophysiological insights and therapeutic options. Circulation 2021, 143, 1157–1172. [Google Scholar] [CrossRef] [PubMed]
- Naicker, S. Burden of end-stage renal disease in sub-Saharan Africa. Clin. Nephrol. 2010, 74, S13–S16. [Google Scholar] [CrossRef] [PubMed]
- Carney, E.F. The impact of chronic kidney disease on global health. Nat. Rev. Nephrol. 2020, 16, 251. [Google Scholar] [CrossRef] [PubMed]
- Nataatmadja, M.; Evangelidis, N.; Manera, K.E.; Cho, Y.; Johnson, D.W.; Craig, J.C.; Baumgart, A.; Hanson, C.S.; Shen, J.; Guha, C. Perspectives on mental health among patients receiving dialysis. Nephrol. Dial. Transplant. 2021, 36, 1317–1325. [Google Scholar] [CrossRef] [PubMed]
- Rota-Musoll, L.; Subirana-Casacuberta, M.; Oriol-Vila, E.; Homs-Del Valle, M.; Molina-Robles, E.; Brigidi, S. The experience of donating and receiving a kidney: A systematic review of qualitative studies. J. Ren. Care 2020, 46, 169–184. [Google Scholar] [CrossRef]
- Okoro, R.N.; Adibe, M.O.; Okonta, M.J.; Ummate, I.; Ohieku, J.D.; Yakubu, S.I. Assessment of health-related quality of life and its determinants in the pre-dialysis patients with chronic kidney disease. Int. Urol. Nephrol. 2021, 54, 165–172. [Google Scholar] [CrossRef] [PubMed]
- Tao, X.; Zhang, H.; Huang, J.; Gu, A.; Jin, Y.; He, Y.; Li, N.; Yang, Y. Physical performance and health-related quality of life among older adults on peritoneal dialysis: A cross-sectional study. Int. Urol. Nephrol. 2021, 53, 1033–1042. [Google Scholar] [CrossRef]
- Unruh, M.; Miskulin, D.; Yan, G.; Hays, R.D.; Benz, R.; Kusek, J.W.; Meyer, K.B.; Group, H.S. Racial differences in health-related quality of life among hemodialysis patients. Kidney Int. 2004, 65, 1482–1491. [Google Scholar] [CrossRef]
- Mapes, D.L.; Lopes, A.A.; Satayathum, S.; McCullough, K.P.; Goodkin, D.A.; Locatelli, F.; Fukuhara, S.; Young, E.W.; Kurokawa, K.; Saito, A. Health-related quality of life as a predictor of mortality and hospitalization: The Dialysis Outcomes and Practice Patterns Study (DOPPS). Kidney Int. 2003, 64, 339–349. [Google Scholar] [CrossRef]
- Lowrie, E.G.; Curtin, R.B.; LePain, N.; Schatell, D. Medical outcomes study short form-36: A consistent and powerful predictor of morbidity and mortality in dialysis patients. Am. J. Kidney Dis. 2003, 41, 1286–1292. [Google Scholar] [CrossRef]
- DeOreo, P.B. Hemodialysis patient-assessed functional health status predicts continued survival, hospitalization, and dialysis-attendance compliance. Am. J. Kidney Dis. 1997, 30, 204–212. [Google Scholar] [CrossRef]
- Knight, E.L.; Ofsthun, N.; Teng, M.; Lazarus, J.M.; Curhan, G.C. The association between mental health, physical function, and hemodialysis mortality. Kidney Int. 2003, 63, 1843–1851. [Google Scholar] [CrossRef] [PubMed]
- Jenkinson, C.; Jenkinson, D.; Shepperd, S.; Richard, L.; Petersen, S. Evaluation of treatment for congestive heart failure in patients aged 60 years and older using generic measures of health status (SF-36 and COOP charts). Age Ageing 1997, 26, 7–13. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Walters, B.A.; Hays, R.D.; Spritzer, K.L.; Fridman, M.; Carter, W.B. Health-related quality of life, depressive symptoms, anemia, and malnutrition at hemodialysis initiation. Am. J. Kidney Dis. 2002, 40, 1185–1194. [Google Scholar] [CrossRef] [PubMed]
- Kefale, B.; Alebachew, M.; Tadesse, Y.; Engidawork, E. Quality of life and its predictors among patients with chronic kidney disease: A hospital-based cross sectional study. PLoS ONE 2019, 14, e0212184. [Google Scholar] [CrossRef]
- Ware, J.E.; Richardson, M.M.; Meyer, K.B.; Gandek, B. Improving CKD-specific patient-reported measures of health-related quality of life. J. Am. Soc. Nephrol. 2019, 30, 664–677. [Google Scholar] [CrossRef]
- Imtiaz, S.; Alam, A. Is haemodialysis the most feasible dialysis modality for Pakistan? J. Pak. Med. Assoc. 2020, 71, 1–8. [Google Scholar] [CrossRef]
- Senanayake, S.; Gunawardena, N.; Palihawadana, P.; Senanayake, S.; Karunarathna, R.; Kumara, P.; Kularatna, S. Health related quality of life in chronic kidney disease; a descriptive study in a rural Sri Lankan community affected by chronic kidney disease. Health Qual. Life Outcomes 2020, 18, 108. [Google Scholar] [CrossRef]
- Yapa, H.E.; Purtell, L.; Chambers, S.; Bonner, A. Alterations in symptoms and health-related quality of life as kidney function deteriorates: A cross-sectional study. J. Clin. Nurs. 2021, 30, 1787–1796. [Google Scholar] [CrossRef]
- Gorke, A. Dialysis Outcomes and Practice Patterns Study (DOPPS). Dial. Aktuell 2016, 20, 274–275. [Google Scholar] [CrossRef][Green Version]
- Banerjee, T.; Kim, S.J.; Astor, B.; Shafi, T.; Coresh, J.; Powe, N.R. Vascular access type, inflammatory markers, and mortality in incident hemodialysis patients: The Choices for Healthy Outcomes in Caring for End-Stage Renal Disease (CHOICE) Study. Am. J. Kidney Dis. 2014, 64, 954–961. [Google Scholar] [CrossRef] [PubMed]
- Wirkner, J.; Scheuch, M.; Dabers, T.; Freiin von Rheinbaben, S.; Fiene, B.; Aymanns, S.; Endlich, K.; Endlich, N.; Lendeckel, U.; Rettig, R. Comorbid Depression and Diabetes Are Associated with Impaired Health-Related Quality of Life in Chronic Kidney Disease Patients. J. Clin. Med. 2022, 11, 4671. [Google Scholar] [CrossRef]
- Boulware, L.E.; Liu, Y.; Fink, N.E.; Coresh, J.; Ford, D.E.; Klag, M.J.; Powe, N.R. Temporal relation among depression symptoms, cardiovascular disease events, and mortality in end-stage renal disease: Contribution of reverse causality. Clin. J. Am. Soc. Nephrol. 2006, 1, 496–504. [Google Scholar] [CrossRef] [PubMed]
- Hedayati, S.S.; Bosworth, H.B.; Briley, L.P.; Sloane, R.J.; Pieper, C.F.; Kimmel, P.L.; Szczech, L.A. Death or hospitalization of patients on chronic hemodialysis is associated with a physician-based diagnosis of depression. Kidney Int. 2008, 74, 930–936. [Google Scholar] [CrossRef] [PubMed]
- Kimmel, P.L.; Peterson, R.A.; Weihs, K.L.; Simmens, S.J.; Alleyne, S.; Cruz, I.; Veis, J.H. Multiple measurements of depression predict mortality in a longitudinal study of chronic hemodialysis outpatients. Kidney Int. 2000, 57, 2093–2098. [Google Scholar] [CrossRef] [PubMed]
- Lopes, A.A.; Bragg, J.; Young, E.; Goodkin, D.; Mapes, D.; Combe, C.; Piera, L.; Held, P.; Gillespie, B.; Port, F.K. Depression as a predictor of mortality and hospitalization among hemodialysis patients in the United States and Europe. Kidney Int. 2002, 62, 199–207. [Google Scholar] [CrossRef]
- Wyld, M.L.; Morton, R.L.; Clayton, P.; Wong, M.G.; Jardine, M.; Polkinghorne, K.; Chadban, S. The impact of progressive chronic kidney disease on health-related quality-of-life: A 12-year community cohort study. Qual. Life Res. 2019, 28, 2081–2090. [Google Scholar] [CrossRef]
- Wee, H.-L.; Seng, B.J.J.; Lee, J.J.; Chong, K.J.; Tyagi, P.; Vathsala, A.; How, P. Association of anemia and mineral and bone disorder with health-related quality of life in Asian pre-dialysis patients. Health Qual. Life Outcomes 2016, 14, 94. [Google Scholar] [CrossRef]
- Seng, J.J.B.; Tan, J.Y.; Yeam, C.T.; Htay, H.; Foo, W.Y.M. Factors affecting medication adherence among pre-dialysis chronic kidney disease patients: A systematic review and meta-analysis of literature. Int. Urol. Nephrol. 2020, 52, 903–916. [Google Scholar] [CrossRef]
- Schmid, H.; Hartmann, B.; Schiffl, H. Adherence to prescribed oral medication in adult patients undergoing chronic hemodialysis: A critical review of the literature. Eur. J. Med. Res. 2009, 14, 185–190. [Google Scholar] [CrossRef]
- Rehman, I.U.; Chan, K.G.; Munib, S.; Lee, L.H.; Khan, T.M. The association between CKD-associated pruritus and quality of life in patients undergoing hemodialysis in Pakistan: A STROBE complaint cross-sectional study. Medicine 2019, 98, e16812. [Google Scholar] [CrossRef] [PubMed]
- Rizvi, S.A.H.; Manzoor, K. Causes of chronic renal failure in Pakistan: A single large center experience. Saudi J. Kidney Dis. Transplant. 2002, 13, 376. [Google Scholar]
- Imtiaz, S.; Alam, A. Is haemodialysis the most feasible dialysis modality for Pakistan? JPMA J. Pak. Med. Assoc. 2021, 71, 528–530. [Google Scholar]
- Neuen, B.L.; Chadban, S.J.; Demaio, A.R.; Johnson, D.W.; Perkovic, V. Chronic kidney disease and the global NCDs agenda. BMJ Spec. J. 2017, 2, e000380. [Google Scholar] [CrossRef] [PubMed]
- Barra, S.; Providência, R.; Faustino, C.; Paiva, L.; Fernandes, A.; Marques, A.L. Performance of the cockcroft-gault, MDRD and CKD-EPI formulae in non-valvular atrial fibrillation: Which one should be used for risk stratification? J. Atr. Fibrillation 2013, 6, 896. [Google Scholar] [PubMed]
- Anees, M.; Ibrahim, M.; Imtiaz, M.; Batool, S.; Elahi, I.; Malik, M.R. Translation, validation and reliability of the kidney diseases quality of life-short form (KDQOL-SF Form) tool in Urdu. J. Coll. Physicians Surg. Pak. 2016, 26, 651–654. [Google Scholar] [PubMed]
- Hashmi, A.M.; Naz, S.; Asif, A.; Khawaja, I.S. Urdu translation of the Hamilton Rating Scale for Depression: Results of a validation study. Pak. J. Med. Sci. 2016, 32, 1479. [Google Scholar] [CrossRef]
- Morisky, D.E.; Green, L.W.; Levine, D.M. Concurrent and predictive validity of a self-reported measure of medication adherence. Med. Care 1986, 67–74. [Google Scholar] [CrossRef]
- Taber, K.S. The use of Cronbach’s alpha when developing and reporting research instruments in science education. Res. Sci. Educ. 2018, 48, 1273–1296. [Google Scholar] [CrossRef]
- Pagels, A.A.; Söderkvist, B.K.; Medin, C.; Hylander, B.; Heiwe, S. Health-related quality of life in different stages of chronic kidney disease and at initiation of dialysis treatment. Health Qual. Life Outcomes 2012, 10, 1–11. [Google Scholar] [CrossRef]
- Tesfaye, W.H.; McKercher, C.; Peterson, G.M.; Castelino, R.L.; Jose, M.; Zaidi, S.T.R.; Wimmer, B.C. Medication adherence, burden and health-related quality of life in adults with predialysis chronic kidney disease: A prospective cohort study. Int. J. Environ. Res. Public Health 2020, 17, 371. [Google Scholar] [CrossRef] [PubMed]
- Ajeebi, A.; Saeed, A.; Aljamaan, A.; Alshehri, M.; Nasradeen, M.; Alharbi, N.; Omair, A.; Al-Sayyari, A.A. A study of quality of life among hemodialysis patients and its associated factors using kidney disease quality of life instrument-SF36 in Riyadh, Saudi Arabia. Saudi J. Kidney Dis. Transplant. 2020, 31, 1225. [Google Scholar] [CrossRef] [PubMed]
- Mok, E.; Tam, B. Stressors and coping methods among chronic haemodialysis patients in Hong Kong. J. Clin. Nurs. 2001, 10, 503–511. [Google Scholar] [CrossRef]
- Jordakieva, G.; Grabovac, I.; Steiner, M.; Winnicki, W.; Zitta, S.; Stefanac, S.; Brooks, M.; Sunder-Plaßmann, G.; Rosenkranz, A.R.; Godnic-Cvar, J. Employment status and associations with workability, quality of life and mental health after kidney transplantation in Austria. Int. J. Environ. Res. Public Health 2020, 17, 1254. [Google Scholar] [CrossRef] [PubMed]
- Zemestani, M.; Mozaffari, S. Acceptance and commitment therapy for the treatment of depression in persons with physical disability: A randomized controlled trial. Clin. Rehabil. 2020, 34, 938–947. [Google Scholar] [CrossRef]
- Farrokhi, F.; Abedi, N.; Beyene, J.; Kurdyak, P.; Jassal, S.V. Association between depression and mortality in patients receiving long-term dialysis: A systematic review and meta-analysis. Am. J. Kidney Dis. 2014, 63, 623–635. [Google Scholar] [CrossRef]
- Tsai, Y.-C.; Chiu, Y.-W.; Hung, C.-C.; Hwang, S.-J.; Tsai, J.-C.; Wang, S.-L.; Lin, M.-Y.; Chen, H.-C. Association of symptoms of depression with progression of CKD. Am. J. Kidney Dis. 2012, 60, 54–61. [Google Scholar] [CrossRef]
- Khan, A.; Khan, A.H.; Adnan, A.S.; Sulaiman, S.A.S.; Mushtaq, S. Prevalence and predictors of depression among hemodialysis patients: A prospective follow-up study. BMC Public Health 2019, 19, 1–13. [Google Scholar] [CrossRef]
- Hirst, J.A.; Hill, N.; O’Callaghan, C.A.; Lasserson, D.; McManus, R.J.; Ogburn, E.; Mena, J.M.O.; Shine, B.; Taylor, C.J.; Vazquez-Montes, M.D. Prevalence of chronic kidney disease in the community using data from OxRen: A UK population-based cohort study. Br. J. Gen. Pract. 2020, 70, e285–e293. [Google Scholar] [CrossRef]
- Amaral, T.L.M.; Amaral, C.d.A.; Vasconcellos, M.T.L.d.; Monteiro, G.T.R. Prevalence and factors associated to chronic kidney disease in older adults. Rev. De Saude Publica 2019, 53, 44. [Google Scholar] [CrossRef]
- Lv, J.-C.; Zhang, L.-X. Prevalence and disease burden of chronic kidney disease. Ren. Fibros. Mech. Ther. 2019, 1165, 3–15. [Google Scholar]
- Khamis, S.S.A.; El Edel, R.H.; Zahran, A.M.; Ibrahim, M.A.; El Zorkany, K.M.A. Prevalence of Chronic Kidney Disease in Relatives of Chronic Hemodialysis Patients. Open J. Nephrol. 2020, 10, 274. [Google Scholar] [CrossRef]
- Duan, J.; Wang, C.; Liu, D.; Qiao, Y.; Pan, S.; Jiang, D.; Zhao, Z.; Liang, L.; Tian, F.; Yu, P. Prevalence and risk factors of chronic kidney disease and diabetic kidney disease in Chinese rural residents: A cross-sectional survey. Sci. Rep. 2019, 9, 10408. [Google Scholar] [CrossRef]
- Jitraknatee, J.; Ruengorn, C.; Nochaiwong, S. Prevalence and risk factors of chronic kidney disease among type 2 diabetes patients: A cross-sectional study in primary care practice. Sci. Rep. 2020, 10, 6205. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.-H.; Hsu, Y.-J.; Tzeng, W.-C. Physical Activity and Health-Related Quality of Life of Patients on Hemodialysis with Comorbidities: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 811. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | n (%) | |
|---|---|---|
| Gender | Female | 164 (52.4) |
| Male | 150 (47.6) | |
| Age mean (±SD) | 54.64 (±15.33) | |
| Age group (years) | ||
| <40 | 57 (18.2) | |
| 41–60 | 145 (46.2) | |
| >60 | 112 (35.7) | |
| BMI mean (±SD) | 20.08 (±3.65) | |
| BMI * Classification | ||
| Underweight | 102 (32.4) | |
| Normal | 167 (53.0) | |
| Overweight | 32 (10.2) | |
| Obese | 12 (3.8) | |
| Socioeconomic status ** | ||
| Low | 94 (29.9) | |
| Middle | 197 (62.8) | |
| High | 23 (7.3) | |
| Education Level | ||
| Uneducated | 185 (59.9) | |
| Educated | 129 (41.08) | |
| Marital Status | ||
| Single | 32 (10.1) | |
| Married | 282 (89.9) | |
| Smoking Status | ||
| Current Smoker | 73 (23.2) | |
| Non-Smoker | 241 (76.8) | |
| Employment | ||
| Unemployed | 120 (54.5) | |
| Employed | 100 (45.5) | |
| Grade of kidney failure | ||
| Chronic kidney disease grade 4 | 125 (39.8) | |
| Kidney failure grade 5 (Non-Dialysis) | 29 (9.2) | |
| Kidney failure grade 5 (Hemodialysis) | 160 (50.9) | |
| Kidney failure Duration | ||
| 1 year | 91 (29) | |
| 2–4 years | 153 (48.7) | |
| >5 years | 70 (22.3) |
| Biochemical Parameters ** | Normal Range | Grade 4 Pre Laboratory Parameters | Grade 4 Post Laboratory Parameters | PCS p-Value | MCS p-Value | Grade 5 Pre Laboratory Parameters | Grade 5 Post Laboratory Parameters | PCS p-Value | MCS p-Value |
|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | ||||||
| Hematology | Hemoglobin (11–18 g/dL) | 8.9 ± 1.61 | 8.8 ± 1.7 | <0.05 * | 0.471 | 9.95 ± 1.69 | 8.85 ± 1.62 | <0.05 * | 0.412 |
| Serum Iron Studies | Ferritin (250–450 µg/dL) | 147.60 ± 81.52 | 136.59 ± 82.0 | <0.05 * | <0.05 * | 147.60 ± 81.52 | 136.59 ± 82.0 | <0.05 * | <0.05 * |
| Iron (50–170 µg/dL) | 175.1 ± 31.38 | 164.26 ± 31.56 | <0.05 * | <0.05 * | 176.4 ± 31.38 | 174.16 ± 32.8 | 0.163 | <0.05 * | |
| Renal Function Test | Creatinine (0.5–1.1 mg/dL) | 10.9 ± 3.2 | 14.6 ± 2.71 | <0.05 * | 0.241 | 14.46 ± 9.1 | 10.66 ± 3.01 | N/A | N/A |
| Urea (13–43 mg/dL) | 174.03 ± 57.78 | 163.68 ± 72.13 | <0.05 * | <0.05 * | 160.3 ± 67.8 | 154.3 ± 62.7 | N/A | N/A | |
| Liver Function Test | Bilirubin (0.3–1.2 mg/dL) | 1.11 ± 0.31 | 1.10 ± 0.32 | 0.277 | 0.432 | 1.31 ± 0.41 | 1.10 ± 0.22 | 0.289 | 0.093 |
| Serum Electrolytes | Calcium (8.4–10.2 mg/dL) | 6.6 ± 1.2 | 6.7 ± 1.31 | 0.240 | 0.331 | 8.77 ± 1.19 | 8.70 ± 1.28 | 0.683 | 0.569 |
| Sodium (136–146 mEq/L) | 137.1 ± 13.9 | 137.0 ± 13.0 | 0.760 | 0.491 | 138.26 ± 13.05 | 139.5 ± 13.27 | 0.852 | 0.311 | |
| Potassium (3.5–5.1 mEq/L) | 4.49 ± 0.52 | 4.15 ± 0.33 | 0.778 | 0.922 | 4.59 ± 0.42 | 4.65 ± 0.43 | 0.201 | 0.542 | |
| Phosphate (35–105 U/L) | 76.2 ± 14.73 | 73.04 ± 16.6 | 0.807 | 0.547 | 81.2 ± 12.11 | 79.04 ± 15.1 | 0.838 | 0.368 |
| KDQOL Domains | No. of Items in a Scale | Mean | Mean | KDQOL Scale | No. of Items in Scale | Mean | Mean | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre-Study | p-value | Post-Study | p-Value | Pre-Study | p-Value | Post Study | p-Value | ||||||||
| Grade 4 | Grade 5 | Grade 4 | Grade 5 | Grade 4 | Grade 5 | Grade 4 | Grade 5 | ||||||||
| Symptom/problem list | 12 | 57.70 ± 11.44 | 63.70 ± 12.39 | 0.08 | 58.70 ± 16.63 | 68.70 ± 11.13 | 0.002 * | Physical functioning | 10 | 41.68 ± 27.17 | 61.24 ± 8.72 | 0.008 * | 40.12 ± 24.66 | 57.44 ± 9.12 | 0.03 * |
| Role limitations--physical | 4 | 33.31 ± 17.85 | 41.02 ± 11.12 | 0.02 * | 33.12 ± 19.05 | 40.82 ± 10.72 | 0.28 | ||||||||
| Effects of kidney disease | 8 | 56.45 ± 11.23 | 55.85 ± 10.80 | 0.1 | 57.45 ± 13.41 | 49.25 ± 9.10 | 0.35 | Pain | 2 | 13.60 ± 6.57 | 12.67 ± 3.41 | 0.41 | 14.11 ± 5.07 | 17.07 ± 4.88 | 0.41 |
| General Health | 5 | 31.84 ± 10.35 | 31.11 ± 8.43 | 0.88 | 30.04 ± 11.75 | 34.31 ± 8.69 | 0.68 | ||||||||
| Burden of kidney disease | 4 | 29.06 ± 11.59 | 34.06 ± 9.83 | 0.24 | 26.06 ± 11.59 | 34.86 ± 10.11 | 0.04 * | Emotional well-being | 5 | 39.30 ± 9.07 | 51.44 ± 7.32 | 0.009 * | 31.03 ± 12.17 | 48.42 ± 6.12 | 0.000 * |
| Physical Health Composite | 12 | 31.28 ± 7.91 | 36.28 ± 8.41 | 0.68 | 33.81 ± 7.14 | 37.22 ± 8.11 | 0.68 | Role limitations-- emotional | 3 | 28.42 ± 11.59 | 28.22 ± 8.47 | 0.78 | 28.11 ± 9.11 | 29.62 ± 7.97 | 0.78 |
| Social function | 2 | 18.13 ± 5.39 | 21.85 ± 7.77 | 0.45 | 19.03 ± 5.11 | 20.65 ± 7.01 | 0.61 | ||||||||
| Mental Health Composite | 12 | 36.66 ± 6.57 | 48.66 ± 5.44 | 0.009 * | 37.99 ± 6.57 | 47.16 ± 7.44 | 0.01 * | Energy/fatigue | 4 | 48.50 ± 9.11 | 59.21 ± 5.51 | 0.046 * | 47.11 ± 8.61 | 51.59 ± 7.91 | 0.046 * |
| Outcome | Depression Defined Using MGLS as a Categorical Variable | ||
|---|---|---|---|
| Unadjusted Association | Adjusted Association | ||
| Grade 4 | PCS | −3.99 (−8.29, 0.31) ** | −4.64 (−9.10, −0.17) ** |
| MCS | 1.82 (−3.12, 6.78) ** | 2.03 (−2.99, 7.05) * | |
| Grade 5 | PCS | −3.0(−9.9, 3.9) ** | −3.4(−9.1, 0.90) ** |
| MCS | 1.43 (−4.99, 7.85) * | 1.15(−5.3,7.6) * | |
| Outcome | Depression Defined Using HAM-D as a Continuous Variable | Depression Defined Using HAM-D as a Categorical Variable | |||
|---|---|---|---|---|---|
| Unadjusted Association | Adjusted Association | Unadjusted Association | Adjusted Association | ||
| Grade 4 | PCS | −1.62 (−2.38, −0.86) | −1.29 (−1.87, −0.72) | −2.13 (−3.66, −0.60) * | −1.73 (−3.09, −0.37) ** |
| MCS | −5.32 (−6.11, −4.53) | −4.52 (−5.15, −3.89) | −9.24 (−11.27, −7.21) | −8.13 (−9.83, −6.44) * | |
| Grade 5 | PCS | −1.96 (−3.01, −0.91) | −1.68 (−2.41, −0.96) | −2.01 (−3.06, −0.97) | −1.71 (−2.87, −0.55) * |
| MCS | −5.30 (−6.84, −3.77) | −4.71 (−5.98, −3.44) | −9.06 (−10.51, −7.61) ** | −7.81 (−9.30, −6.33) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Butt, M.D.; Ong, S.C.; Butt, F.Z.; Sajjad, A.; Rasool, M.F.; Imran, I.; Ahmad, T.; Alqahtani, F.; Babar, Z.-U.-D. Assessment of Health-Related Quality of Life, Medication Adherence, and Prevalence of Depression in Kidney Failure Patients. Int. J. Environ. Res. Public Health 2022, 19, 15266. https://doi.org/10.3390/ijerph192215266
Butt MD, Ong SC, Butt FZ, Sajjad A, Rasool MF, Imran I, Ahmad T, Alqahtani F, Babar Z-U-D. Assessment of Health-Related Quality of Life, Medication Adherence, and Prevalence of Depression in Kidney Failure Patients. International Journal of Environmental Research and Public Health. 2022; 19(22):15266. https://doi.org/10.3390/ijerph192215266
Chicago/Turabian StyleButt, Muhammad Daoud, Siew Chin Ong, Fatima Zahid Butt, Ahsan Sajjad, Muhammad Fawad Rasool, Imran Imran, Tanveer Ahmad, Faleh Alqahtani, and Zaheer-Ud-Din Babar. 2022. "Assessment of Health-Related Quality of Life, Medication Adherence, and Prevalence of Depression in Kidney Failure Patients" International Journal of Environmental Research and Public Health 19, no. 22: 15266. https://doi.org/10.3390/ijerph192215266
APA StyleButt, M. D., Ong, S. C., Butt, F. Z., Sajjad, A., Rasool, M. F., Imran, I., Ahmad, T., Alqahtani, F., & Babar, Z.-U.-D. (2022). Assessment of Health-Related Quality of Life, Medication Adherence, and Prevalence of Depression in Kidney Failure Patients. International Journal of Environmental Research and Public Health, 19(22), 15266. https://doi.org/10.3390/ijerph192215266