
Barriers and Facilitators of Hepatitis C Care in Persons Coinfected with Human Immunodeficiency Virus
 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Design and Patient Selection
2.2. Definitions
3. Results
3.1. Baseline Characteristics
3.2. HCV Treatment Protocols and Results
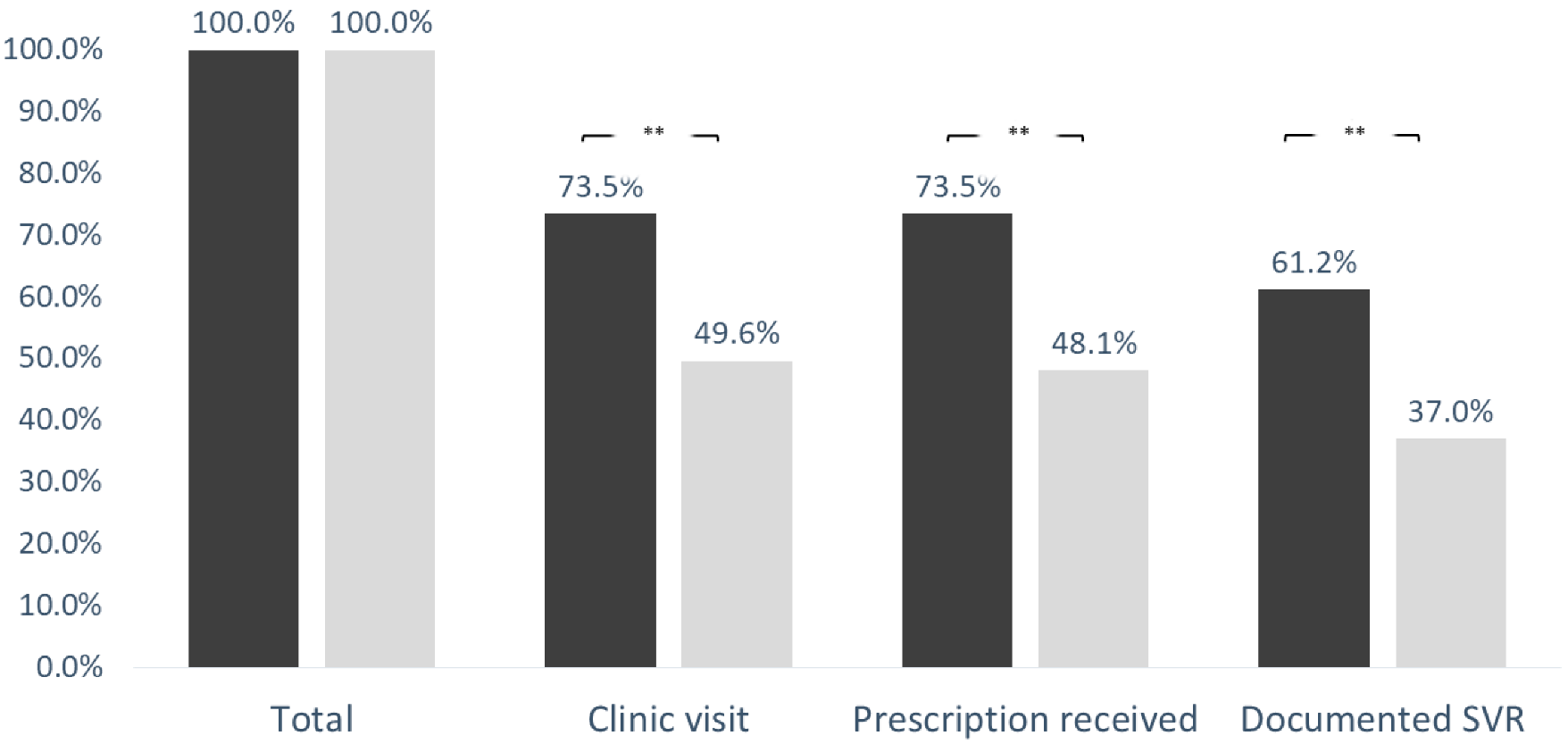
3.3. Linkage to Hepatitis C Care
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Arends, J.E.; Lieveld, F.I.; Boeijen, L.L.; de Kanter, C.T.M.M.; van Erpecum, K.J.; Salmon, D.; Hoepelman, A.I.; Asselah, T.; Ustianowski, A. Natural history and treatment of HCV/HIV coinfection: Is it time to change paradigms? J. Hepatol. 2015, 63, 1254–1262. [Google Scholar] [CrossRef] [PubMed]
- Merican, I.; Sherlock, S.; Mclntyre, N.; Dusheiko, C.M. Clinical, biochemical and histological features in 102 patients with chronic hepatitis C virus infection. QJM Int. J. Med. 1993, 86, 119–125. [Google Scholar]
- Alter, M.J. Epidemiology of viral hepatitis and HIV co-infection. J. Hepatol. 2006, 44 (Suppl. 1), S6–S9. [Google Scholar] [CrossRef] [PubMed]
- Adler, M.W. ABC of AIDS. Development of the epidemic. Br. Med. J. (Clin. Res. Ed.) 1987, 294, 1083–1085. [Google Scholar] [CrossRef][Green Version]
- Lin, W.; Weinberg, E.M.; Chung, R.T. Pathogenesis of accelerated fibrosis in HIV/HCV co-infection. J. Infect. Dis. 2013, 207 (Suppl. 1), S13–S18. [Google Scholar] [CrossRef]
- Simmons, B.; Saleem, J.; Hill, A.; Riley, R.D.; Cooke, G.S. Risk of Late Relapse or Reinfection With Hepatitis C Virus after Achieving a Sustained Virological Response: A Systematic Review and Meta-analysis. Clin. Infect. Dis. 2016, 62, 683–694. [Google Scholar] [CrossRef]
- Nachnani, J.S.; Rao, G.A.; Bulchandani, D.; Pandya, P.K.; Alba, L.M. Predictors of hematological abnormalities in patients with chronic hepatitis C treated with interferon and ribavirin. Ann. Hematol. 2010, 89, 121–125. [Google Scholar] [CrossRef]
- Peters, L.; Laut, K.; Resnati, C.; Del Campo, S.; Leen, C.; Falconer, K.; Trofimova, T.; Paduta, D.; Gatell, J.; Rauch, A.; et al. Uptake of HCV treatment in HIV/HCV coinfected patients across europe in the era of direct-acting antivirals. AIDS 2018, 32, 1995–2004. [Google Scholar] [CrossRef]
- Virlogeux, V.; Zoulim, F.; Pugliese, P.; Poizot-Martin, I.; Valantin, M.-A.; Cuzin, L.; Reynes, J.; Billaud, E.; Huleux, T.; Bani-Sadr, F.; et al. Modeling HIV-HCV coinfection epidemiology in the direct-acting antiviral era: The road to elimination. BMC Med. 2017, 15, 217. [Google Scholar] [CrossRef]
- Nápoles, T.M.; Batchelder, A.W.; Lin, A.; Moran, L.; Johnson, M.O.; Shumway, M.; Luetkemeyer, A.F.; Peters, M.G.; Eagen, K.V.; Riley, E.D. HCV treatment barriers among HIV/HCV co-infected patients in the US: A qualitative study to understand low uptake among marginalized populations in the DAA era. J. Public Health 2019, 41, e283–e289. [Google Scholar] [CrossRef]
- Grebely, J.; Oser, M.; Taylor, L.E.; Dore, G.J. Breaking down the barriers to hepatitis C virus (HCV) treatment among individuals with HCV/HIV coinfection: Action required at the system, provider, and patient levels. J. Infect. Dis. 2013, 207 (Suppl. 1), S19–S25. [Google Scholar] [CrossRef] [PubMed]
- Moussalli, J.; Delaquaize, H.; Boubilley, D.; Lhomme, J.P.; Merleau Ponty, J.; Sabot, D.; Kerever, A.; Valleur, M.; Poynard, T. Factors to improve the management of hepatitis C in drug users: An observational study in an addiction centre. Gastroenterol. Res. Pract. 2010, 2010, 261472. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Broers, B.; Helbling, B.; François, A.; Schmid, P.; Chuard, C.; Hadengue, A.; Negro, F.; Swiss Association for the Study of the Liver (SASL 18). Barriers to interferon-alpha therapy are higher in intravenous drug users than in other patients with acute hepatitis C. J. Hepatol. 2005, 42, 323–328. [Google Scholar] [CrossRef] [PubMed]
- Bruggmann, P.; Falcato, L.; Dober, S.; Helbling, B.; Keiser, O.; Negro, F.; Meili, D.; Swiss Hepatitis C Cohort Study. Active intravenous drug use during chronic hepatitis C therapy does not reduce sustained virological response rates in adherent patients. J. Viral Hepat. 2008, 15, 747–752. [Google Scholar] [CrossRef]
- Liao, P.-Y.; Choi, Y.S.; Lee, K.H. FSscan: A mechanism-based program to identify +1 ribosomal frameshift hotspots. Nucleic Acids Res. 2009, 37, 7302–7311. [Google Scholar] [CrossRef][Green Version]
- WHO Releases First-Ever Global Guidance for Country Validation of Viral Hepatitis B and C Elimination [Internet]. Available online: https://www.who.int/news/item/25-06-2021-who-releases-first-ever-global-guidance-for-country-validation-of-viral-hepatitis-b-and-c-elimination (accessed on 30 March 2022).
- Toyoda, H.; Atsukawa, M.; Watanabe, T. Real-world experience of 12-week direct-acting antiviral regimen of glecaprevir and pibrentasvir in patients with chronic hepatitis C virus infection. J. Gastroenterol. Hepatol. 2020, 35, 855–861. [Google Scholar] [CrossRef]
- Phillips, C.; Schulkind, J.; O’Sullivan, M.; Edelman, N.; Smith, H.E.; Verma, S.; Jones, C.J. Improving access to care for people who inject drugs: Qualitative evaluation of project ITTREAT-An integrated community hepatitis C service. J. Viral Hepat. 2020, 27, 176–187. [Google Scholar] [CrossRef]
- Lam, J.O.; Hurley, L.B.; Chamberland, S.; Champsi, J.H.; Gittleman, L.C.; Korn, D.G.; Lai, J.B.; Quesenberry, C.P., Jr.; Ready, J.; Saxena, V.; et al. Hepatitis C treatment uptake and response among human immunodeficiency virus/hepatitis C virus-coinfected patients in a large integrated healthcare system. Int. J. STD AIDS 2019, 30, 689–695. [Google Scholar] [CrossRef]
- Ma, J.; Non, L.; Amornsawadwattana, S.; Olsen, M.A.; Garavaglia Wilson, A.; Presti, R.M. Hepatitis C care cascade in HIV patients at an urban clinic in the early direct-acting antiviral era. Int. J. STD AIDS 2019, 30, 834–842. [Google Scholar] [CrossRef]
- Jatt, L.P.; Gandhi, M.M.; Guo, R. Barriers to hepatitis C direct-acting antiviral therapy among HIV/hepatitis C virus-coinfected persons. J. Gastroenterol. Hepatol. 2021, 36, 1095–1102. [Google Scholar] [CrossRef]
- Patel, S.V.; Jayaweera, D.T.; Althoff, K.N.; Eron, J.J.; Radtchenko, J.; Mills, A.; Moyle, G.; Santiago, S.; Sax, P.E.; Gillman, J.; et al. Real-world efficacy of direct acting antiviral therapies in patients with HIV/HCV. PLoS ONE 2020, 15, e0228847. [Google Scholar] [CrossRef] [PubMed]
- Ho, S.B.; Bräu, N.; Cheung, R.; Liu, L.; Sanchez, C.; Sklar, M.; Phelps, T.E.; Marcus, S.G.; Wasil, M.M.; Tisi, A.; et al. Integrated care increases treatment and improves outcomes of patients with chronic hepatitis C virus infection and psychiatric illness or substance abuse. Clin. Gastroenterol. Hepatol. 2015, 13, 2005–2014.e1. [Google Scholar] [CrossRef] [PubMed]
- Busschots, D.; Bielen, R.; Koc, Ö.M.; Heyens, L.; Dercon, E.; Verrando, R.; Janssens, F.; Van den Bergh, L.; Van Lint, P.; Bruckers, L.; et al. On-site testing and case management to improve hepatitis C care in drug users: A prospective, longitudinal, multicenter study in the DAA era. BMC Public Health 2021, 21, 1574. [Google Scholar] [CrossRef] [PubMed]
- Saab, S.; Challita, Y.P.; Najarian, L.M.; Guo, R.; Saggi, S.S.; Choi, G. Hepatitis C screening: Barriers to linkage to care. J. Clin. Transl. Hepatol. 2019, 7, 226–231. [Google Scholar] [CrossRef]
- Abadie, R.; Goldenberg, S.; Welch-Lazoritz, M.; Fisher, C.B. Establishing trust in HIV/HCV research among people who inject drugs (PWID): Insights from empirical research. PLoS ONE 2018, 13, e0208410. [Google Scholar] [CrossRef]
- Akiyama, M.J.; Lipsey, D.; Heo, M.; Agyemang, L.; Norton, B.L.; Hidalgo, J.; Lora, K.; Litwin, A.H. Low Hepatitis C Reinfection Following Direct-acting Antiviral Therapy Among People Who Inject Drugs on Opioid Agonist Therapy. Clin. Infect. Dis. 2020, 70, 2695–2702. [Google Scholar] [CrossRef]
- Kerzman, H.; Green, M.S.; Shinar, E. Risk factors for hepatitis C virus infection among blood donors in Israel: A case-control study between native Israelis and immigrants from the former Soviet Union. Transfusion 2007, 47, 1189–1196. [Google Scholar] [CrossRef]
- Greenaway, C.; Makarenko, I.; Tanveer, F.; Janjua, N.Z. Addressing hepatitis C in the foreign-born population: A key to hepatitis C virus elimination in Canada. Can. Liver J. 2018, 1, 34–50. [Google Scholar] [CrossRef]
- Corcorran, M.A.; Tsui, J.I.; Scott, J.D.; Dombrowski, J.C.; Glick, S.N. Age and gender-specific hepatitis C continuum of care and predictors of direct acting antiviral treatment among persons who inject drugs in Seattle, Washington. Drug Alcohol Depend. 2021, 220, 108525. [Google Scholar] [CrossRef]
- Morris, M.D.; Mirzazadeh, A.; Evans, J.L.; Briceno, A.; Coffin, P.; Hahn, J.A.; Page, K.A. Treatment cascade for hepatitis C virus in young adult people who inject drugs in San Francisco: Low number treated. Drug Alcohol Depend. 2019, 198, 133–135. [Google Scholar] [CrossRef]
- Tempalski, B.; Pouget, E.R.; Cleland, C.M.; Brady, J.E.; Cooper, H.L.F.; Hall, H.I.; Lansky, A.; West, B.S.; Friedman, S.R. Trends in the population prevalence of people who inject drugs in US metropolitan areas 1992–2007. PLoS ONE 2013, 8, e64789. [Google Scholar] [CrossRef] [PubMed]
- Zibbell, J.E.; Iqbal, K.; Patel, R.C.; Suryaprasad, A.; Sanders, K.J.; Moore-Moravian, L.; Serrecchia, J.; Blankenship, S.; Ward, J.W.; Holtzman, D. Increases in hepatitis C virus infection related to injection drug use among persons aged ≤30 years—Kentucky, Tennessee, Virginia, and West Virginia, 2006–2012. MMWR Morb. Mortal. Wkly. Rep. 2015, 64, 453–458. [Google Scholar] [PubMed]
- Mateu-Gelabert, P.; Guarino, H.; Quinn, K.; Meylakhs, P.; Campos, S.; Meylakhs, A.; Berbesi, D.; Toro-Tobón, D.; Goodbody, E.; Ompad, D.C.; et al. Young drug users: A vulnerable population and an underutilized resource in HIV/HCV prevention. Curr. HIV/AIDS Rep. 2018, 15, 324–335. [Google Scholar] [CrossRef] [PubMed]
- Falade-Nwulia, O.; Ward, K.M.; McCormick, S.; Mehta, S.H.; Pitts, S.R.; Katz, S.; Chander, G.; Thomas, D.L.; Sulkowski, M.; Latkin, C.A. Network-based recruitment of people who inject drugs for hepatitis C testing and linkage to care. J. Viral Hepat. 2020, 27, 663–670. [Google Scholar] [CrossRef]


{kind=link}
| Total (n = 274) | |
|---|---|
| Age (years) | 37.2 ± 8.6 |
| Male sex | 202 (73.7) |
| Immigrant from endemic country | 219 (79) |
| Excessive Alcohol use | 35 (12.7) |
| Active substance use | 40 (14.6) |
| Opiate substitution treatment | 24 (9) |
| Presumed mode of transmission (n = 184), some coexist. | |
| PWID | 135 (73.4) |
| MSM | 28 (15.2) |
| Unprotected intercourse (non MSM) | 18 (9.7) |
| Blood product transmission | 8 (4.3) |
| Iatrogenic transmission | 1 (0.5) |
| HCV characteristics (n = 142) | |
| 1a | 20 (14.1) |
| 1b | 64 (45.1) |
| 2 | 5 (3.5) |
| 3 | 38 (26.7) |
| 4 | 15 (10.6) |
| Liver fibrosis level (n = 109) | |
| F0-1 | 66 (60.5) |
| F2 | 16 (14.7) |
| F3 | 11 (10.1) |
| F4 | 16 (14.7) |
| Triple infection (HBsAg positive) | 14 (5.1) |
| Resolved HBV infection (HBsAg negative, HB-core positive) | 156 (56.9%) |
| Non-PWID (n = 49) | PWID (n = 135) | p Value | |
|---|---|---|---|
| Age (years) | 37.8 + 8.2 | 36.1 + 13.3 | NS |
| Age at HIV diagnosis | 33.8 ± (8.6) | 33.9 ± (8.8) | NS |
| Male sex | 37 (75.5) | 101 (74.8) | NS |
| Marital status | NS | ||
| Single | 26 (53.1) | 63 (46.7) | |
| Married | 11 (22.4) | 43 (31.9) | |
| Divorced/widowed | 12 (24.5) | 29 (21.5) | |
| Has children | 20 (40.8) | 73 (54.1) | NS |
| Active drug use | Not applicable | 40 (29.6) | NA |
| Excessive Alcohol use | 8 (28.6) | 27 (38.6) | NS |
| Immigrant from endemic country | 29 (59.2) | 119 (88.1) | p < 0.001 |
| Presumed viral transmission way | NA | ||
| MSM | 26 (53.1) | 2 (1.5) | |
| Non MSM unprotected sex (see text) | 14 (28.6) | 4 (3.0) | |
| Blood product transmission | 8 (16.3) | 0 (0) | |
| Iatrogenic transmission | 1 (2) | 0 (0) | |
| HCV genotype (n = 118) | <0.001 | ||
| 1a | 9 (23.7) | 10 (12.5) | |
| 1b | 14 (36.8) | 37 (46.3) | |
| 2 | 0 (0) | 4 (5) | |
| 3 | 4 (10.5) | 27 (33.8) | |
| 4 | 11 (28.9) | 2 (2.5) | |
| CD4 count | 620 (365–818) | 594 (436–831) | |
| Fibrosis level (n = 109) | NS | ||
| F0-1 | 22 (61.1) | 44 (60.3) | |
| F2 | 5 (13.9) | 11 (15.1) | |
| F3 | 4 (11.1) | 7 (9.6) | |
| F4 | 5 (13.9) | 11 (15.1) | |
| Serologic data | |||
| HBs Ag (+): triple infection (data available in 174) | 3 (6.8) | 7 (5.4) | NS |
| Anti-HB core (+) (data available in 173) | 25 (56.8) | 92 (71.3) | NS |
| VDRL (data available in = 154) | 10 (25.6) | 9 (7.8) | 0.001 |
| TPHA (data available in = 154) | 16 (41) | 18 (15.7) | 0.009 |
| Clinic Visit | Prescription Received | SVR Documentation | |
|---|---|---|---|
| Age (for every 5y) | 1.17 (1.01–1.34), p = 0.031 | 1.16 (1.01–1.33), p = 0.036 | 1.18 (1.02–1.36), p = 0.025 |
| Male sex | 1.36 (0.79–2.33), NS | 1.3 (0.76–2.24), NS | 1.45 (0.81–2.57), NS |
| Being married | 1.03 (0.71–1.48), p NS | 1.08 (0.75–1.56). NS | 1.18 (0.82–1.7), NS |
| Having children | 1 (0.56–1.78), NS | 1.09 (0.61–1.94), NS | 1.26 (0.7–2.3), NS |
| Being an Immigrant from endemic countries | 0.54 (0.3–1), p = 0.051 | 0.58 (0.32–1.06), p = 0.077 | 0.63 (0.34–1.16), p = 0.135 |
| Excessive Alcohol use | 0.81 (0.37–1.74), NS | 0.81 (0.37–1.74), NS | 1.11 (0.52–2.39), NS |
| Being a PWID | 0.36 (0.17–0.73), p = 0.005 | 0.34 (0.16–0.69), p = 0.003 | 0.37 (0.19–0.73), p = 0.004 |
| Active drug use | 0.1 (0.04–0.26), p < 0.001 | 0.08 (0.03–0.23), p < 0.001 | 0.08 (0.02–0.29), p < 0.001 |
| Clinic Visit | Prescription Received | SVR Documentation | |
|---|---|---|---|
| Age (for every 5y) | 1.36 (1.11–1.68) p = 0.003 | 1.35 (1.1–1.66) p = 0.004 | 1.25 (1.04–1.52) p = 0.021 |
| PWID | 0.44 (0.2–0.98), p = 0.043 | 0.41 (0.18–0.91) p = 0.028 | 0.45 (0.22–0.94) p = 0.034 |
| Active drug use | 0.1 (0.42–0.24), p < 0.001 | 0.09 (0.04–0.22) p < 0.001 | 0.1 (0.04–0.27) p < 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bar, N.; Bensoussan, N.; Rabinowich, L.; Levi, S.; Houri, I.; Ben-Ami Shor, D.; Shibolet, O.; Mor, O.; Weitzman, E.; Turner, D.; et al. Barriers and Facilitators of Hepatitis C Care in Persons Coinfected with Human Immunodeficiency Virus. Int. J. Environ. Res. Public Health 2022, 19, 15237. https://doi.org/10.3390/ijerph192215237
Bar N, Bensoussan N, Rabinowich L, Levi S, Houri I, Ben-Ami Shor D, Shibolet O, Mor O, Weitzman E, Turner D, et al. Barriers and Facilitators of Hepatitis C Care in Persons Coinfected with Human Immunodeficiency Virus. International Journal of Environmental Research and Public Health. 2022; 19(22):15237. https://doi.org/10.3390/ijerph192215237
Chicago/Turabian StyleBar, Nir, Noa Bensoussan, Liane Rabinowich, Sharon Levi, Inbal Houri, Dana Ben-Ami Shor, Oren Shibolet, Orna Mor, Ella Weitzman, Dan Turner, and et al. 2022. "Barriers and Facilitators of Hepatitis C Care in Persons Coinfected with Human Immunodeficiency Virus" International Journal of Environmental Research and Public Health 19, no. 22: 15237. https://doi.org/10.3390/ijerph192215237
APA StyleBar, N., Bensoussan, N., Rabinowich, L., Levi, S., Houri, I., Ben-Ami Shor, D., Shibolet, O., Mor, O., Weitzman, E., Turner, D., & Katchman, H. (2022). Barriers and Facilitators of Hepatitis C Care in Persons Coinfected with Human Immunodeficiency Virus. International Journal of Environmental Research and Public Health, 19(22), 15237. https://doi.org/10.3390/ijerph192215237