
Acute Effects of Percussive Massage Treatment on Drop Jump Performance and Achilles Tendon Stiffness


 ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
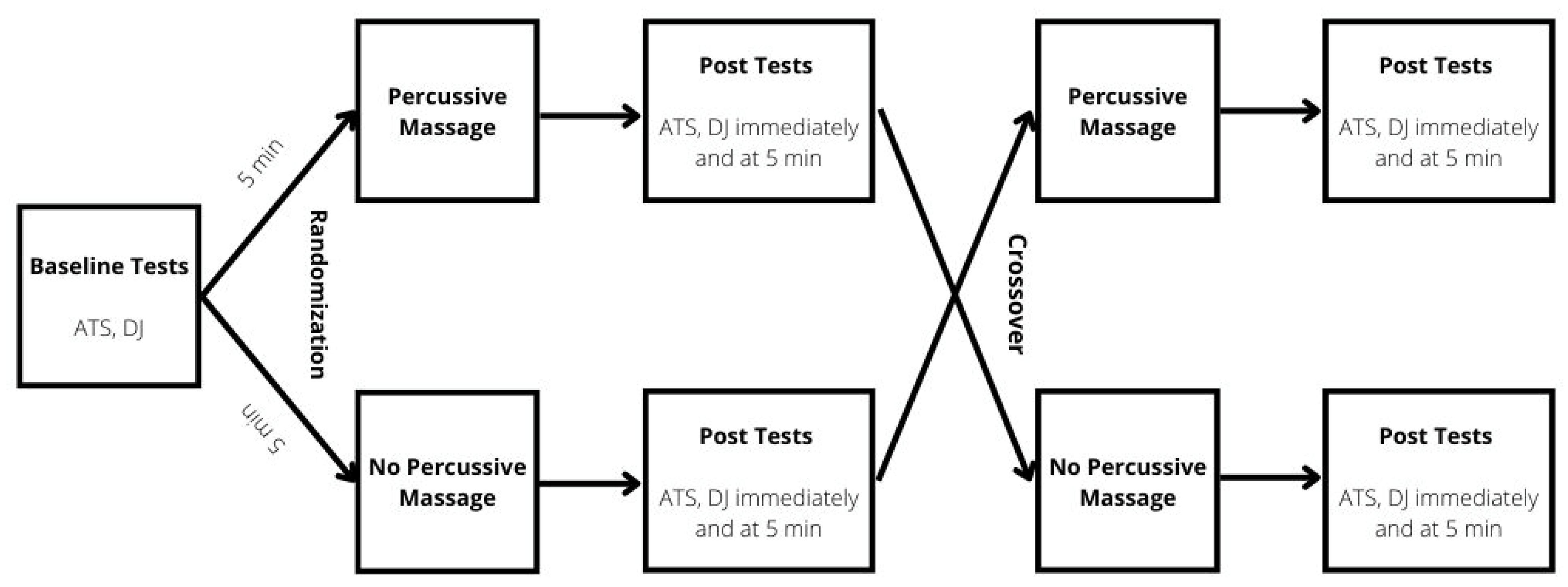
2.1. Experimental Approach to the Problem
2.2. Subjects
2.3. Familiarization Session
2.4. Achilles Tendon Percussive Massage
2.5. Measurement of Drop Jump Performance
2.6. Measurement of Achilles Tendon Stiffness
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cheatham, S.W.; Baker, R.T.; Behm, D.G.; Stull, K.; Kolber, M.J. Mechanical Percussion Devices: A Survey of Practice Patterns Among Healthcare Professionals. Int. J. Sports Phys. Ther. 2021, 16, 766–777. [Google Scholar] [CrossRef] [PubMed]
- Behm, D.G.; Peach, A.; Maddigan, M.; Aboodarda, S.J.; DiSanto, M.C.; Button, D.C.; Maffiuletti, N.A. Massage and Stretching Reduce Spinal Reflex Excitability without Affecting Twitch Contractile Properties. J. Electromyogr. Kinesiol. 2013, 23, 1215–1221. [Google Scholar] [CrossRef]
- Poppendieck, W.; Wegmann, M.; Ferrauti, A.; Kellmann, M.; Pfeiffer, M.; Meyer, T. Massage and Performance Recovery: A Meta-Analytical Review. Sports Med. 2016, 46, 183–204. [Google Scholar] [CrossRef] [PubMed]
- García-Sillero, M.; Benítez-Porres, J.; García-Romero, J.; Bonilla, D.A.; Petro, J.L.; Vargas-Molina, S. Comparison of Interventional Strategies to Improve Recovery after Eccentric Exercise-Induced Muscle Fatigue. Int. J. Environ. Res. Public Health 2021, 18, 647. [Google Scholar] [CrossRef] [PubMed]
- Martínez Rodríguez, R.; Galán del Río, F. Mechanistic Basis of Manual Therapy in Myofascial Injuries. Sonoelastographic Evolution Control. J. Bodyw. Mov. Ther. 2013, 17, 221–234. [Google Scholar] [CrossRef]
- Schleip, R.; Müller, D.G. Training Principles for Fascial Connective Tissues: Scientific Foundation and Suggested Practical Applications. J. Bodyw. Mov. Ther. 2013, 17, 103–115. [Google Scholar] [CrossRef]
- García-Sillero, M.; Jurado-Castro, J.M.; Benítez-Porres, J.; Vargas-Molina, S. Acute Effects of a Percussive Massage Treatment on Movement Velocity during Resistance Training. Int. J. Environ. Res. Public Health 2021, 18, 7726. [Google Scholar] [CrossRef]
- Kablan, N.; Alaca, N.; Tatar, Y. Comparison of the Immediate Effect of Petrissage Massage and Manual Lymph Drainage Following Exercise on Biomechanical and Viscoelastic Properties of the Rectus Femoris Muscle in Women. J. Sport Rehabil. 2021, 30, 725–730. [Google Scholar] [CrossRef]
- Konrad, A.; Glashüttner, C.; Reiner, M.M.; Bernsteiner, D.; Tilp, M. The Acute Effects of a Percussive Massage Treatment with a Hypervolt Device on Plantar Flexor Muscles’ Range of Motion and Performance. J. Sports Sci. Med. 2020, 19, 690–694. [Google Scholar]
- Cochrane, D.J.; Stannard, S.R.; Firth, E.C.; Rittweger, J. Acute Whole-Body Vibration Elicits Post-Activation Potentiation. Eur. J. Appl. Physiol. 2010, 108, 311–319. [Google Scholar] [CrossRef]
- Dallas, G.; Colson, S.; Pappas, P.; Dallas, C.; Paradisis, G. Whole Body Vibration and Drop Jumps Induces Post-Activation Performance Enhancement. Hum. Mov. 2022, 24. [Google Scholar] [CrossRef]
- Cochrane, D.J.; Stannard, S.R.; Firth, E.C.; Rittweger, J. Comparing Muscle Temperature during Static and Dynamic Squatting with and without Whole-Body Vibration: Squatting, Muscle Temperature & Vibration. Clin. Physiol. Funct. Imaging 2010, 30, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Blazevich, A.J.; Babault, N. Post-Activation Potentiation Versus Post-Activation Performance Enhancement in Humans: Historical Perspective, Underlying Mechanisms, and Current Issues. Front. Physiol. 2019, 10, 1359. [Google Scholar] [CrossRef]
- Lythgo, N.; Eser, P.; de Groot, P.; Galea, M. Whole-Body Vibration Dosage Alters Leg Blood Flow. Clin. Physiol. Funct. Imaging 2009, 29, 53–59. [Google Scholar] [CrossRef]
- Eriksson Crommert, M.; Lacourpaille, L.; Heales, L.J.; Tucker, K.; Hug, F. Massage Induces an Immediate, Albeit Short-Term, Reduction in Muscle Stiffness: Effect of Massage on Muscle Stiffness. Scand. J. Med. Sci. Sports 2015, 25, e490–e496. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.-S. Therapeutic Effects of Massage and Electrotherapy on Muscle Tone, Stiffness and Muscle Contraction Following Gastrocnemius Muscle Fatigue. J. Phys. Ther. Sci. 2017, 29, 144–147. [Google Scholar] [CrossRef]
- Goebel, R.T.; Kleinöder, H.; Yue, Z.; Gosh, R.; Mester, J. Effect of Segment-Body Vibration on Strength Parameters. Sports Med. Open 2015, 1, 14. [Google Scholar] [CrossRef]
- Tankisheva, E.; Bogaerts, A.; Boonen, S.; Delecluse, C.; Jansen, P.; Verschueren, S.M.P. Effects of a Six-Month Local Vibration Training on Bone Density, Muscle Strength, Muscle Mass, and Physical Performance in Postmenopausal Women. J. Strength Cond. Res. 2015, 29, 2613–2622. [Google Scholar] [CrossRef]
- Heishman, A.D.; Daub, B.D.; Miller, R.M.; Freitas, E.D.S.; Frantz, B.A.; Bemben, M.G. Countermovement Jump Reliability Performed With and Without an Arm Swing in NCAA Division 1 Intercollegiate Basketball Players. J. Strength Cond. Res. 2020, 34, 546–558. [Google Scholar] [CrossRef]
- Haen, T.X.; Roux, A.; Soubeyrand, M.; Laporte, S. Shear Waves Elastography for Assessment of Human Achilles Tendon’s Biomechanical Properties: An Experimental Study. J. Mech. Behav. Biomed. Mater. 2017, 69, 178–184. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Campbell, M.J.; Walters, S.J.K.; Machin, D. Medical Statistics: A Textbook for the Health Sciences, 5th ed.; John Wiley Blackwell: Hoboken, NJ, USA, 2021; ISBN 978-1-119-42364-5. [Google Scholar]
- McKechnie, G.J.B.; Young, W.B.; Behm, D.G. Acute Effects of Two Massage Techniques on Ankle Joint Flexibility and Power of the Plantar Flexors. J. Sports Sci. Med. 2007, 6, 498–504. [Google Scholar] [PubMed]
- Krzysztofik, M.; Wilk, M.; Stastny, P.; Golas, A. Post-Activation Performance Enhancement in the Bench Press Throw: A Systematic Review and Meta-Analysis. Front. Physiol. 2021, 11, 598628. [Google Scholar] [CrossRef] [PubMed]
- Kagaya, A.; Ohmori, F.; Okuyama, S.; Muraoka, Y.; Sato, K. Blood Flow and Arterial Vessel Diameter Change During Graded Handgrip Exercise in Dominant and Non-Dominant Forearms of Tennis Players. In Oxygen Transport to Tissue XXXI; Takahashi, E., Bruley, D.F., Eds.; Advances in Experimental Medicine and Biology; Springer: Boston, MA, USA, 2010; Volume 662, pp. 365–370. ISBN 978-1-4419-1239-8. [Google Scholar]



{kind=link}
{kind=link}
| Variables | ICC [95% CI] | CV [%] |
|---|---|---|
| Jump Height | 0.91 (0.68 to 0.98) | 11% |
| Contact Time | 0.92 (0.70 to 0.98) | 4% |
| Reactive Strength Index | 0.85 (0.62 to 0.9) | 10% |
| Relative Peak Power | 0.84 (0.66 to 0.91) | 7% |
| Peak Velocity | 0.92 (0.69 to 0.98) | 2% |
| Dominant Achilles Tendon Stiffness | 0.96 (0.88 to 0.99) | 3% |
| Non-dominant Achilles Tendon Stiffness | 0.92 (0.71 to 0.98) | 4% |
| Variable | EXP | CTRL | ||||
|---|---|---|---|---|---|---|
| Pre | Post | 5 min. Post | Pre | Post | 5 min. Post | |
| Jump Height [cm] | 36.9 ± 5.5 (33.2 to 40.6) | 37.3 ± 5.1 (33.8 to 40.7) | 35.6 ± 4.6 (32.5 to 38.7) | 36.1 ± 4.4 (33.1 to 39.0) | 36.2 ± 4.8 (33.0 to 39.4) | 36.6 ± 4.3 (33.6 to 39.5) |
| Contact Time [ms] | 0.383 ± 0.128 (0.297 to 0.469) | 0.385 ± 0.118 (0.306 to 0.464) | 0.374 ± 0.118 (0.295 to 0.454) | 0.366 ± 0.132 (0.278 to 0.455) | 0.380 ± 0.127 (0.295 to 0.465) | 0.373 ± 0.113 (0.297 to 0.449) |
| Reactive Strength Index | 1.05 ± 0.29 (0.86 to 1.24) | 1.04 ± 0.27 (0.85 to 1.22) | 1.03 ± 0.28 (0.84 to 1.22) | 1.09 ± 0.31 (0.88 to 1.29) | 1.04 ± 0.33 (0.82 to 1.27) | 1.05 ± 0.28 (0.86 to 1.25) |
| Relative Peak Power [W/kg] | 113.6 ± 16.0 (102.9 to 124.3) | 111.2 ± 13.9 (101.8 to 120.5) | 109.2 ± 14.5 (99.4 to 118.9) | 114.7 ± 18.1 (102.6 to 126.9) | 111.1 ± 19.4 (98.1 to 124.2) | 111.7 ± 15.6 (101.2 to 122.2) |
| Peak Velocity [m/s] | 2.81 ± 0.20 (2.68 to 2.95) | 2.82 ± 0.19 (2.70 to 2.95) | 2.76 ± 0.17 (2.65 to 2.88) | 2.78 ± 0.17 (2.67 to 2.90) | 2.79 ± 0.18 (2.66 to 2.91) | 2.80 ± 0.17 (2.68 to 2.91) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szymczyk, P.; Węgrzynowicz, K.; Trybulski, R.; Spieszny, M.; Ewertowska, P.; Wilk, M.; Krzysztofik, M. Acute Effects of Percussive Massage Treatment on Drop Jump Performance and Achilles Tendon Stiffness. Int. J. Environ. Res. Public Health 2022, 19, 15187. https://doi.org/10.3390/ijerph192215187
Szymczyk P, Węgrzynowicz K, Trybulski R, Spieszny M, Ewertowska P, Wilk M, Krzysztofik M. Acute Effects of Percussive Massage Treatment on Drop Jump Performance and Achilles Tendon Stiffness. International Journal of Environmental Research and Public Health. 2022; 19(22):15187. https://doi.org/10.3390/ijerph192215187
Chicago/Turabian StyleSzymczyk, Patryk, Kamil Węgrzynowicz, Robert Trybulski, Michał Spieszny, Paulina Ewertowska, Michał Wilk, and Michał Krzysztofik. 2022. "Acute Effects of Percussive Massage Treatment on Drop Jump Performance and Achilles Tendon Stiffness" International Journal of Environmental Research and Public Health 19, no. 22: 15187. https://doi.org/10.3390/ijerph192215187
APA StyleSzymczyk, P., Węgrzynowicz, K., Trybulski, R., Spieszny, M., Ewertowska, P., Wilk, M., & Krzysztofik, M. (2022). Acute Effects of Percussive Massage Treatment on Drop Jump Performance and Achilles Tendon Stiffness. International Journal of Environmental Research and Public Health, 19(22), 15187. https://doi.org/10.3390/ijerph192215187