
Reliable Knowledge about Obesity Risk, Rather Than Personality, Is Associated with Positive Beliefs towards Obese People: Investigating Attitudes and Beliefs about Obesity, and Validating the Polish Versions of ATOP, BAOP and ORK–10 Scales


Abstract
1. Introduction
2. Materials and Methods
2.1. Ethics
2.2. Translation Procedure
2.3. Tools
2.3.1. Metrics and Demographic Data
2.3.2. ATOP
2.3.3. BAOP
2.3.4. ORK–10
2.3.5. Personality
2.4. Data Analysis
3. Results
3.1. Study Sample Characteristics
3.2. The Obesity Risk Knowledge
3.3. PL–ATOP Scale
3.3.1. PL–ATOP Validity and Reliability
3.3.2. PL–ATOP Differences in Groups by Gender and BMI
3.3.3. Correlation and Regression Analysis of the PL–ATOP Scale
3.4. BAOP Scale
3.4.1. PL–BAOP Validity and Reliability
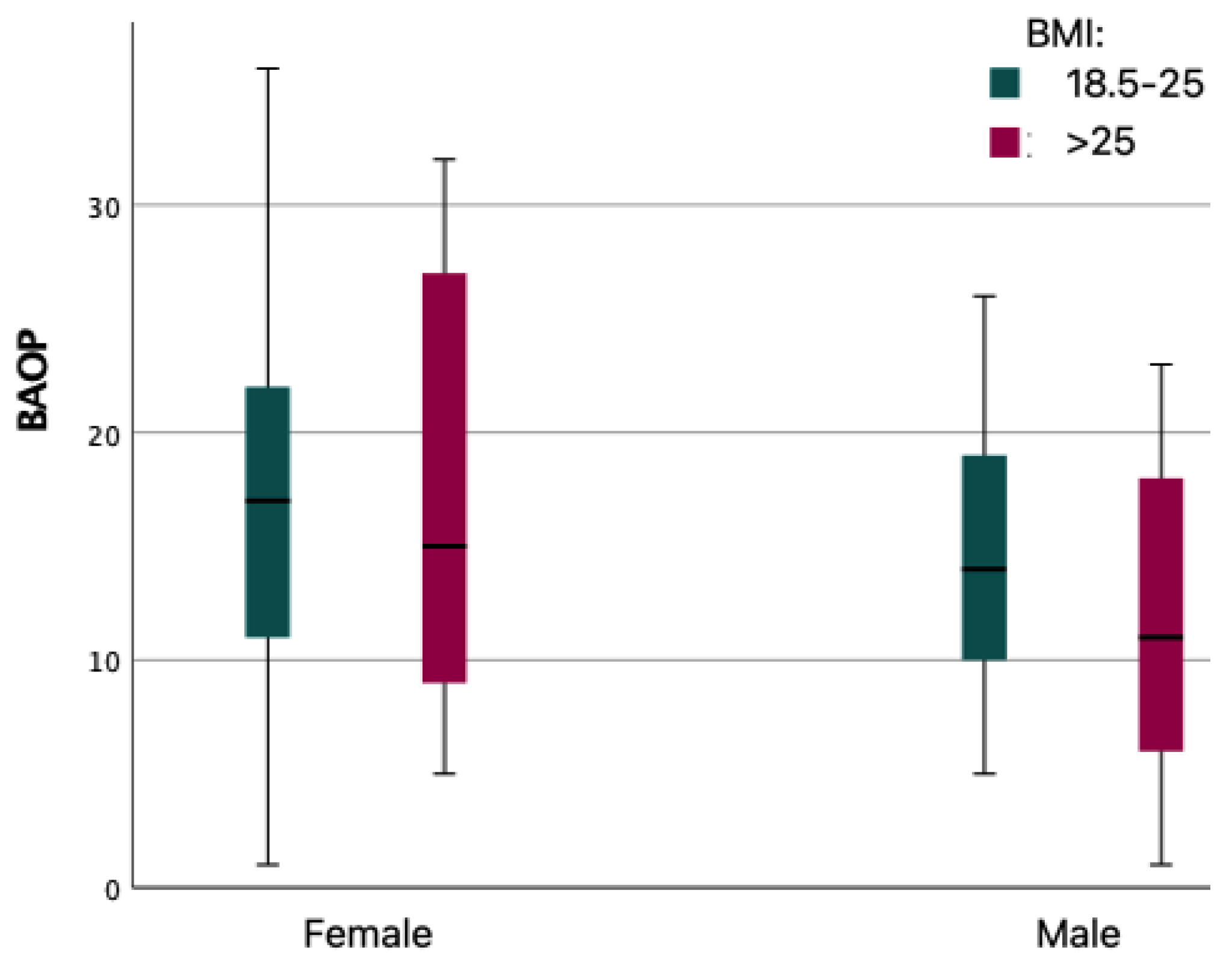
3.4.2. PL–BAOP Differences in Groups by Gender and BMI
3.4.3. Correlation and Regression Analysis of the PL–BAOP Scale
4. Discussion
5. Conclusions
- -
- Obesity risk knowledge predicts positive attitudes and beliefs toward obese people more than personality
- -
- The PL–ATOP and PL–BAOP are fully validated psychometric measurement tools;
- -
- The Polish version of the PL–ORK–10 is a fully useful tool that can also be successfully used with Polish-speaking respondents.
6. Limitation
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hruby, A.; Hu, F.B. The Epidemiology of Obesity: A Big Picture. PharmacoEconomics 2015, 33, 673–689. [Google Scholar] [CrossRef]
- Spahlholz, J.; Baer, N.; König, H.-H.; Riedel-Heller, S.G.; Luck-Sikorski, C. Obesity and discrimination—A systematic review and meta-analysis of observational studies. Obes. Rev. 2016, 17, 43–55. [Google Scholar] [CrossRef]
- Sikorski, C.; Spahlholz, J.; Hartlev, M.; Riedel-Heller, S.G. Weight-based discrimination: An ubiquitary phenomenon? Int. J. Obes. 2016, 40, 333–337. [Google Scholar] [CrossRef]
- Fikkan, J.L.; Rothblum, E.D. Is Fat a Feminist Issue? Exploring the Gendered Nature of Weight Bias. Sex Roles 2012, 66, 575–592. [Google Scholar] [CrossRef]
- Musher-Eizenman, D.R. Body Size Stigmatization in Preschool Children: The Role of Control Attributions. J. Pediatr. Psychol. 2004, 29, 613–620. [Google Scholar] [CrossRef] [PubMed]
- Zacher, H.; von Hippel, C. Weight-based stereotype threat in the workplace: Consequences for employees with overweight or obesity. Int. J. Obes. 2022, 46, 767–773. [Google Scholar] [CrossRef]
- Argüelles, D.; Pérez-Samaniego, V.; López-Cañada, E. “Do you find it normal to be so fat?” Weight stigma in obese gym users. Int. Rev. Sociol. Sport 2021, 57, 1095–1116. [Google Scholar] [CrossRef]
- Puhl, R.M.; Brownell, K.D. Confronting and coping with weight stigma: An investigation of overweight and obese adults. Obesity 2006, 14, 1802–1815. [Google Scholar] [CrossRef] [PubMed]
- Puhl, R.M.; Heuer, C.A. The Stigma of Obesity: A Review and Update. Obesity 2009, 17, 941–964. [Google Scholar] [CrossRef]
- Puhl, R.M.; Moss-Racusin, C.A.; Schwartz, M.B.; Brownell, K.D. Weight stigmatization and bias reduction: Perspectives of overweight and obese adults. Health Educ. Res. 2008, 23, 347–358. [Google Scholar] [CrossRef]
- Carels, R.A.; Domoff, S.E.; Burmeister, J.M.; Koball, A.M.; Hinman, N.G.; Davis, A.K.; Wagner Oehlhof, M.; Leroy, M.; Bannon, E.; Hoffmann, D.A. Examining perceived stereotype threat among overweight/obese adults using a multi-threat framework. Obes. Facts 2013, 6, 258–268. [Google Scholar] [CrossRef] [PubMed]
- Spencer, S.J.; Logel, C.; Davies, P.G. Stereotype Threat. Annu. Rev. Psychol. 2016, 67, 415–437. [Google Scholar] [CrossRef]
- Schvey, N.A.; Puhl, R.M.; Brownell, K.D. The impact of weight stigma on caloric consumption. Obesity 2011, 19, 1957–1962. [Google Scholar] [CrossRef] [PubMed]
- Schvey, N.A.; Marwitz, S.E.; Mi, S.J.; Galescu, O.A.; Broadney, M.M.; Young-Hyman, D.; Brady, S.M.; Reynolds, J.C.; Tanofsky-Kraff, M.; Yanovski, S.Z.; et al. Weight-based teasing is associated with gain in BMI and fat mass among children and adolescents at-risk for obesity: A longitudinal study. Pediatr. Obes. 2019, 14, e12538. [Google Scholar] [CrossRef]
- Tomiyama, A.J. Weight stigma is stressful. A review of evidence for the Cyclic Obesity/Weight-Based Stigma model. Appetite 2014, 82, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Von dem Knesebeck, O.; Lüdecke, D.; Luck-Sikorski, C.; Kim, T.J. Public beliefs about causes of obesity in the USA and in Germany. Int. J. Public Health 2019, 64, 1139–1146. [Google Scholar] [CrossRef]
- Beeken, R.J.; Wardle, J. Public beliefs about the causes of obesity and attitudes towards policy initiatives in Great Britain. Public Health Nutr. 2013, 16, 2132–2137. [Google Scholar] [CrossRef]
- Hebl, M.; Xu, J. Weighing the care: Physicians’ reactions to the size of a patient. Int. J. Obes. 2001, 25, 1246–1252. [Google Scholar] [CrossRef]
- Chambliss, H.O.; Finley, C.E.; Blair, S.N. Attitudes toward Obese Individuals among Exercise Science Students. Med. Sci. Sport. Exerc. 2004, 36, 468–474. [Google Scholar] [CrossRef]
- Fang, V.; Gillespie, C.; Crowe, R.; Popeo, D.; Jay, M. Associations between medical students’ beliefs about obesity and clinical counseling proficiency. BMC Obes. 2019, 6, 5. [Google Scholar] [CrossRef]
- Lynagh, M.; Cliff, K.; Morgan, P.J. Attitudes and Beliefs of Nonspecialist and Specialist Trainee Health and Physical Education Teachers Toward Obese Children: Evidence for “Anti-Fat” Bias. J. Sch. Health 2015, 85, 595–603. [Google Scholar] [CrossRef]
- Davis-Coelho, K.; Waltz, J.; Davis-Coelho, B. Awareness and prevention of bias against fat clients in psychotherapy. Prof. Psychol. Res. Pract. 2000, 31, 682–684. [Google Scholar] [CrossRef]
- Yildiz, M.; Yalcinoz Baysal, H. Prejudice against obesity in university students studying in health-related departments. Perspect. Psychiatr. Care 2019, 55, 170–174. [Google Scholar] [CrossRef]
- Watts, K.; Cranney, J. The Nature and Implications of Implicit Weight Bias. Curr. Psychiatry Rev. 2009, 5, 110–126. [Google Scholar] [CrossRef]
- Ekehammar, B.; Akrami, N. The relation between personality and prejudice: A variable- and a person-centred approach. Eur. J. Personal. 2003, 17, 449–464. [Google Scholar] [CrossRef]
- Hodson, G.; Hogg, S.M.; MacInnis, C.C. The role of “dark personalities” (narcissism, Machiavellianism, psychopathy), Big Five personality factors, and ideology in explaining prejudice. J. Res. Personal. 2009, 43, 686–690. [Google Scholar] [CrossRef]
- Crawford, J.T.; Brandt, M.J. Who Is Prejudiced, and Toward Whom? The Big Five Traits and Generalized Prejudice. Personal. Soc. Psychol. Bull. 2019, 45, 1455–1467. [Google Scholar] [CrossRef]
- Bueno, E.H.; Mendez, R.V. Perceived competence and agreeableness predict positive behaviors toward Mexican immigrants: Less acculturated Hispanics are more welcoming of immigrants. In Proceedings of the 24th Congress of the International Association for Cross-Cultural Psychology, Guelph, ON, Canada, 1–5 July 2018; Available online: https://scholarworks.gvsu.edu/ (accessed on 29 September 2022).
- Monaghan, L.F.; Rich, E.; Bombak, A.E. Media, ‘Fat Panic’ and Public Pedagogy: Mapping Contested Terrain. Sociol. Compass 2019, 13, e12651. [Google Scholar] [CrossRef]
- Sherf-Dagan, S.; Kessler, Y.; Mardy-Tilbor, L.; Raziel, A.; Sakran, N.; Boaz, M.; Kaufman-Shriqui, V. The Effect of an Education Module to Reduce Weight Bias among Medical Centers Employees: A Randomized Controlled Trial. Obes. Facts 2022, 15, 384–394. [Google Scholar] [CrossRef] [PubMed]
- Wynn, T.; Islam, N.; Thompson, C.; Myint, K.S. The effect of knowledge on healthcare professionals’ perceptions of obesity. Obes. Med. 2018, 11, 20–24. [Google Scholar] [CrossRef]
- Allison, D.B.; Basile, V.C.; Yuker, H.E. The measurement of attitudes toward and beliefs about obese persons. Int. J. Eat. Disord. 1991, 10, 599–607. [Google Scholar] [CrossRef]
- Tsai, M.C.; Strong, C.; Latner, J.D.; Lin, Y.C.; Pakpour, A.H.; Lin, C.Y.; Wang, S.M. Attitudes toward and beliefs about obese persons across Hong Kong and Taiwan: Wording effects and measurement invariance. Health Qual. Life Outcomes 2019, 17, 134. [Google Scholar] [CrossRef] [PubMed]
- Dedeli, O.; Bursalioglu, S.A.; Deveci, A. Validity and reliability of the Turkish version of the attitudes toward obese persons scale and the beliefs about obese persons scale. Clin. Nurs. Stud. 2014, 2, 105–117. [Google Scholar] [CrossRef][Green Version]
- Lillis, J.; Luoma, J.B.; Levin, M.E.; Hayes, S.C. Measuring weight self-stigma: The weight self-stigma questionnaire. Obesity 2010, 18, 971–976. [Google Scholar] [CrossRef]
- Latner, J.D.; Stunkard, A.J.; Wilson, G.T. Stigmatized students: Age, sex, and ethnicity effects in the stigmatization of obesity. Obes. Res. 2005, 13, 1226–1231. [Google Scholar] [CrossRef] [PubMed]
- Swift, J.A.; Glazebrook, C.; Macdonald, I. Validation of a brief, reliable scale to measure knowledge about the health risks associated with obesity. Int. J. Obes. 2006, 30, 661–668. [Google Scholar] [CrossRef] [PubMed]
- Costa, P.T.; McCrae, R.R. The revised NEO personality inventory (NEO-PI-R). In The SAGE Handbook of Personality Theory and Assessment: Volume 2—Personality Measurement and Testing; SAGE Publications Ltd.: Thousand Oaks, CA, USA, 2008; pp. 179–198. [Google Scholar] [CrossRef]
- Jarmuż, S.; Wyższa, S.; Społecznej, P.; Zamiejscowy, W.; Lach, W.Ł. Metacecha a struktura czynnikowa kwestionariusza NEO-FFI. Prz. Psychol. 2007, 50, 303–317. [Google Scholar]
- Klinkosz, W.; Iskra, J. Examination of the Relations of the Myers-Briggs Type Indicator and the Neo–4 Personality Inventory in a Polish Sample. Psychol. Rep. 2010, 107, 578–586. [Google Scholar] [CrossRef]
- Ambwani, S.; Thomas, K.M.; Hopwood, C.J.; Moss, S.A.; Grilo, C.M. Obesity stigmatization as the status quo: Structural considerations and prevalence among young adults in the U.S. Eat. Behav. 2014, 15, 366–370. [Google Scholar] [CrossRef]
- Zagaria, A.; Mocini, E.; Cerolini, S.; Donini, L.M.; Castelnuovo, G.; Manzoni, G.M.; Pietrabissa, G.; Lombardo, C. A validation study of the Italian version of the Attitudes Toward Obese Persons (I-ATOP) questionnaire. Obes. Res. Clin. Pract. 2022, 16, 262–268. [Google Scholar] [CrossRef]
- Rivers, A.M.; Sherman, J.W.; Rees, H.R.; Reichardt, R.; Klauer, K.C. On the Roles of Stereotype Activation and Application in Diminishing Implicit Bias. Personal. Soc. Psychol. Bull. 2020, 46, 349–364. [Google Scholar] [CrossRef] [PubMed]
- Plant, E.A.; Devine, P.G. Internal and external motivation to respond without prejudice. J. Personal. Soc. Psychol. 1998, 75, 811–832. [Google Scholar] [CrossRef]
- Kruglanski, A.W.; Webster, D.M. Motivated closing of the mind: “Seizing” and “freezing”. Psychol. Rev. 1996, 103, 263–283. [Google Scholar] [CrossRef] [PubMed]
- Fiske, S.; Taylor, S. Social Cognition; McGraw-Hill: New York, NY, USA, 1991. [Google Scholar]
- Fiske, S.; Lin, M.; Neuberg, S. The continuum model: Ten years later. In Dual Process Theories in Social Psychology; Chaiken, S., Trope, Y., Eds.; Guilford: New York, NY, USA, 1999; pp. 231–254. [Google Scholar]



{kind=link}
{kind=link}
| Items | True/False | ||
|---|---|---|---|
| 1 | EN | A person with a ‘beer-belly’ shaped stomach has an increased risk of getting diabetes | T |
| PL | Osoba z brzuchem w kształcie “piwnego brzucha” ma zwiększone ryzyko zachorowania na cukrzycę | ||
| 2 | EN | Obesity increases the risk of getting bowel cancer | T |
| PL | Otyłość zwiększa ryzyko zachorowania na raka jelita grubego | ||
| 3 | EN | An obese person who gets diabetes needs to lose at least 40% of their body weight for clear health benefits | F |
| PL | Osoba otyła, która choruje na cukrzycę, musi stracić co najmniej 40% masy ciała, aby uzyskać wyraźne korzyści zdrowotne | ||
| 4 | EN | Obese people can expect to live as long as nonobese people | F |
| PL | Osoby otyłe mogą spodziewać się, że będą żyły tak długo jak osoby nieotyłe | ||
| 5 | EN | Obesity increases the risk of getting breast cancer after the menopause | T |
| PL | Otyłość zwiększa ryzyko zachorowania na raka piersi po menopauzie | ||
| 6 | EN | Obesity is more of a risk to health for people from South Asia (e.g., India and Pakistan) than it is for White Europeans | T |
| PL | Otyłość jest większym zagrożeniem dla zdrowia dla osób z Azji Południowej (np. Indii i Pakistanu) niż dla białych Europejczyków | ||
| 7 | EN | There is no major health benefit if an obese person who gets diabetes, loses weight | F |
| PL | Nie stanowi istotnych korzyści zdrowotnych, jeśli osoba otyła, która zachoruje na cukrzycę, straci na wadze | ||
| 8 | EN | Obesity does not increase the risk of developing high blood pressure | F |
| PL | Otyłość nie zwiększa ryzyka rozwoju wysokiego ciśnienia krwi | ||
| 9 | EN | It is better for a person’s health to have fat around the hips and thighs than around the stomach and waist | T |
| PL | Lepiej dla zdrowia człowieka jest mieć tłuszcz wokół bioder i ud niż wokół brzucha i talii | ||
| 10 | EN | Obesity increases the risk of getting a food allergy | F |
| PL | Otyłość zwiększa ryzyko zachorowania na alergię pokarmową | ||
| Factors | ATOP Items | Factor Loading | % of the Variance (Cronbach’s Alpha) | |||
|---|---|---|---|---|---|---|
| Different personality | 4 | EN | Obese workers cannot be as successful as other workers. | 0.53 | 15.56% (0.68) | 36.62% (0.73) |
| PL | Otyli pracownicy nie mogą odnosić takich sukcesów jak inni pracownicy. | |||||
| 6 | EN | Severely obese people are usually untidy | 0.54 | |||
| PL | Poważnie otyli ludzie są zwykle niechlujni. | |||||
| 11 | EN | Obese people are often less aggressive than nonobese people. | 0.45 | |||
| PL | Osoby otyłe są często mniej agresywne niż osoby nieotyłe. | |||||
| 12 | EN | Most obese people have different personalities than nonobese people | 0.59 | |||
| PL | Większość osób otyłych ma inną osobowość niż osoby nieotyłe. | |||||
| 14 | EN | Most obese people resent normal weight people. | 0.65 | |||
| PL | Większość osób otyłych nie lubi ludzi o prawidłowej masie ciała. | |||||
| 15 | EN | Obese people are more emotional than nonobese people. | 0.61 | |||
| PL | Osoby otyłe są bardziej emocjonalne niż osoby nieotyłe. | |||||
| 17 | EN | Obese people are just as healthy as nonobese people | 0.63 | |||
| PL | Osoby otyłe są tak samo zdrowe jak osoby nieotyłe. | |||||
| 20 | EN | One of the worst things that could happen to a person would be for him to become obese. | 0.64 | |||
| PL | Jedną z najgorszych rzeczy, jaka może się przydarzyć w życiu jest otyłość. | |||||
| Social difficulties | 5 | EN | Most nonobese people would not want to marry anyone who is obese. | 0.72 | 11.92% (0.64) | |
| PL | Większość osób nieotyłych nie chciałaby poślubić nikogo, kto jest otyły. | |||||
| 7 | EN | Obese people are usually sociable. | 0.40 | |||
| PL | Osoby otyłe są zazwyczaj towarzyskie. | |||||
| 10 | EN | Most people feel uncomfortable when they associate with obese people. | 0.62 | |||
| PL | Większość ludzi czuje się nieswojo, gdy ma kontakt z osobami otyłymi. | |||||
| 16 | EN | Obese people should not expect to lead normal lives. | 0.41 | |||
| PL | Osoby otyłe nie powinny oczekiwać, że będą prowadziły normalne życie. | |||||
| 18 | EN | Obese people are just as sexually attractive as nonobese people. | 0.63 | |||
| PL | Osoby otyłe są tak samo atrakcyjne seksualnie jak osoby nieotyłe. | |||||
| 19 | EN | Obese people tend to have family problems. | 0.49 | |||
| PL | Osoby otyłe mają zwykle problemy rodzinne. | |||||
| Self-esteem | 1 | EN | Obese people are as happy as nonobese people. | 0.70 | 9.13% (0.61) | |
| PL | Osoby otyłe są tak samo szczęśliwe jak osoby nieotyłe. | |||||
| 2 | EN | Most obese people feel that they are not as good as other people. | 0.42 | |||
| PL | Większość osób otyłych uważa, że nie są oni tak dobrzy jak inni. | |||||
| 3 | EN | Most obese people are more self-conscious than other people. | 0.48 | |||
| PL | Większość osób otyłych jest bardziej świadomymi siebie niż inne osoby. | |||||
| 8 | EN | Most obese people are not dissatisfied with themselves. | 0.71 | |||
| PL | Większość osób otyłych nie jest z siebie niezadowolona. | |||||
| 9 | EN | Obese people are just as self-confident as other people. | 0.76 | |||
| PL | Osoby otyłe są tak samo pewne siebie jak inne osoby. | |||||
| 13 | EN | Very few obese people are ashamed of their weight. | 0.43 | |||
| PL | Bardzo niewiele osób otyłych wstydzi się swojej wagi. | |||||
| Variables | GENDER | BMI | ALL | |||
|---|---|---|---|---|---|---|
| Female | Male | <25 | >25 | |||
| PL–ATOP | Age | −0.05 | 0.33 ** | 0.01 | 0.265 ** | 0.06 |
| BMI | −0.06 | 0.02 | −0.01 | −0.33 ** | −0.11 | |
| Neuroticism | −0.07 | −0.18 | 0.05 | 0.15 | 0.06 | |
| Extraversion | 0.27 ** | 0.22 | 0.032 ** | −0.11 | 0.21 * | |
| Openness | 0.15 | 0.14 | 0.13 | 0.01 | 0.06 | |
| Agreeableness | 0.36 ** | 0.27 | 0.44 ** | 0.38 | 0.38 ** | |
| Conscientiousness | 0.09 | 0.06 | 0.19 | −0.16 | 0.10 | |
| Obesity Risk Knowledge | 0.75 ** | 0.81 ** | 0.75 ** | 0.79 ** | 0.77 ** | |
| BAOP | 0.27 ** | 0.55 ** | 0.35 ** | 0.45 ** | 0.34 * | |
| PL–ATOP-Different Personality | Age | −0.01 | 0.49 ** | 0.09 | 0.19 | 0.11 |
| BMI | −0.07 | 0.21 | −0.03 | −0.31 ** | −0.05 | |
| Neuroticism | −0.12 | −0.07 | 0.01 | 0.31 | 0.03 | |
| Extraversion | 0.37 ** | 0.20 | 0.38 ** | −0.42 * | 0.27 * | |
| Openness | 0.14 | 0.02 | 0.15 | −0.36 | 0.03 | |
| Agreeableness | 0.29 ** | 0.20 | 0.38 ** | 0.24 | 0.31 ** | |
| Conscientiousness | 0.08 | −0.09 | 0.13 | −0.30 | 0.05 | |
| Obesity Risk Knowledge | 0.72 ** | 0.73 ** | 0.74 ** | 0.69 ** | 0.72 ** | |
| BAOP | 0.26 ** | 0.29 ** | 0.35 ** | 0.25 * | 0.32 * | |
| PL–ATOP-Social Difficulties | Age | −0.07 | 0.13 | −0.01 | 0.08 | −0.01 |
| BMI | −0.04 | 0.11 | 0.08 | −0.31 ** | −0.06 | |
| Neuroticism | 0.13 | −0.22 | 0.17 | 0.02 | 0.16 | |
| Extraversion | −0.05 | 0.04 | 0.04 | −0.02 | −0.04 | |
| Openness | 0.18 | 0.45 * | 0.17 | 0.42 ** | 0.20 * | |
| Agreeableness | 0.25 * | 0.35 * | 0.35 ** | 0.52 * | 0.33 * | |
| Conscientiousness | 0.03 | 0.19 | 0.09 | −0.02 | 0.09 | |
| Obesity Risk Knowledge | 0.70 ** | 0.54 ** | 0.65 ** | 0.74 ** | 0.68 ** | |
| BAOP | 0.28 ** | 0.34 ** | 0.29 ** | 0.44 ** | 0.29 * | |
| PL–ATOP-Self-Esteem | Age | −0.03 | −0.08 | −0.1 | 0.33 ** | −0.01 |
| BMI | −0.02 | −0.39 ** | −0.08 | −0.04 | −0.16 * | |
| Neuroticism | −0.16 | −0.04 | −0.08 | −0.03 | −0.02 | |
| Extraversion | 0.27 ** | 0.18 | 0.29 ** | 0.22 | 0.21 * | |
| Openness | 0.01 | −0.24 | −0.07 | −0.17 | −0.13 | |
| Agreeableness | 0.32 ** | −0.01 | 0.30 ** | −0.07 | 0.21 * | |
| Conscientiousness | 0.13 | 0.06 | 0.26 ** | −0.02 | 0.116 | |
| Obesity Risk Knowledge | 0.16 | 0.59 ** | 0.27 ** | 0.19 | 0.24 ** | |
| BAOP | 0.04 | 0.50 ** | 0.13 | 0.25 * | 0.12 * | |
| BAOP Items | Factor Loading | % of the Variance (Cronbach’s Alpha) | ||
|---|---|---|---|---|
| 1 | EN | Obesity often occurs when eating is used as a form of compensation for lack of love or attention. | 0.59 | 42.61% (0.76) |
| PL | Otyłość często pojawia się, gdy jedzenie jest wykorzystywane jako forma rekompensaty za brak miłości lub uwagi. | |||
| 2 | EN | In many cases, obesity is the result of a biological disorder. | 0.40 | |
| PL | W wielu przypadkach otyłość jest wynikiem zaburzeń o podłożu medycznym. | |||
| 3 | EN | Obesity is usually caused by overeating. | 0.76 | |
| PL | Otyłość jest zwykle spowodowana przejadaniem się. | |||
| 4 | EN | Most obese people cause their problem by not getting enough exercise. | 0.82 | |
| PL | U większości osób otyłych problem z otyłością jest powodowany przez brak wystarczającej ilości ruchu. | |||
| 5 | EN | Most obese people eat more than nonobese people. | 0.80 | |
| PL | Większość osób otyłych je więcej niż osoby zdrowe. | |||
| 6 | EN | The majority of obese people have poor eating habits that lead to their obesity. | 0.81 | |
| PL | Większość osób otyłych ma złe nawyki żywieniowe, które prowadzą do otyłości. | |||
| 7 | EN | Obesity is rarely caused by a lack of willpower. | 0.60 | |
| PL | Otyłość rzadko kiedy jest spowodowana brakiem siły woli. | |||
| 8 | EN | People can be addicted to food, just as others are addicted to drugs, and these people usually become obese. | 0.58 | |
| PL | Ludzie mogą być uzależnieni od jedzenia, tak jak inni są uzależnieni od narkotyków. Takie uzależnienie jest zwykle przyczyną otyłości. | |||
| Variables | GENDER | BMI | ALL Individuals | ||
|---|---|---|---|---|---|
| Female | Male | <25 | >25 | ||
| Age | 0.01 | 0.08 | −0.07 | 0.38 ** | 0.05 |
| BMI | 0.09 | −0.13 | 0.11 | 0.03 | −0.03 |
| Neuroticism | 0.01 | 0.10 | 0.09 | 0.38 | 0.14 |
| Extraversion | 0.07 | −0.04 | 0.07 | 0.01 | 0.01 |
| Openness | 0.07 | −0.13 | 0.01 | −0.09 | −0.06 |
| Agreeableness | 0.22 * | 0.13 | 0.22 | 0.29 | 0.24 ** |
| Conscientiousness | 0.01 | −0.02 | 0.11 | −0.08 | 0.02 |
| Obesity Risk Knowledge | 0.73 ** | 0.83 ** | 0.74 ** | 0.76 ** | 0.75 ** |
| ATOP | 0.27 ** | 0.55 ** | 0.35 ** | 0.45 ** | 0.34 ** |
| ATOP–DP | 0.26 ** | 0.29 ** | 0.35 ** | 0.25 * | 0.32 ** |
| ATOP–SD | 0.28 *** | 0.34 ** | 0.29 ** | 0.44 ** | 0.29 ** |
| ATOP–SE | 0.04 | 0.50 * | 0.13 | 0.25 * | 0.12 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Styk, W.; Wojtowicz, E.; Zmorzynski, S. Reliable Knowledge about Obesity Risk, Rather Than Personality, Is Associated with Positive Beliefs towards Obese People: Investigating Attitudes and Beliefs about Obesity, and Validating the Polish Versions of ATOP, BAOP and ORK–10 Scales. Int. J. Environ. Res. Public Health 2022, 19, 14977. https://doi.org/10.3390/ijerph192214977
Styk W, Wojtowicz E, Zmorzynski S. Reliable Knowledge about Obesity Risk, Rather Than Personality, Is Associated with Positive Beliefs towards Obese People: Investigating Attitudes and Beliefs about Obesity, and Validating the Polish Versions of ATOP, BAOP and ORK–10 Scales. International Journal of Environmental Research and Public Health. 2022; 19(22):14977. https://doi.org/10.3390/ijerph192214977
Chicago/Turabian StyleStyk, Wojciech, Ewa Wojtowicz, and Szymon Zmorzynski. 2022. "Reliable Knowledge about Obesity Risk, Rather Than Personality, Is Associated with Positive Beliefs towards Obese People: Investigating Attitudes and Beliefs about Obesity, and Validating the Polish Versions of ATOP, BAOP and ORK–10 Scales" International Journal of Environmental Research and Public Health 19, no. 22: 14977. https://doi.org/10.3390/ijerph192214977
APA StyleStyk, W., Wojtowicz, E., & Zmorzynski, S. (2022). Reliable Knowledge about Obesity Risk, Rather Than Personality, Is Associated with Positive Beliefs towards Obese People: Investigating Attitudes and Beliefs about Obesity, and Validating the Polish Versions of ATOP, BAOP and ORK–10 Scales. International Journal of Environmental Research and Public Health, 19(22), 14977. https://doi.org/10.3390/ijerph192214977