
Lifestyle, Type of Work, and Temporary Disability: An Incidence Study of the Working Population

 , ,
, ,  , , ,
, , ,
Abstract
1. Introduction
2. Material and Methods
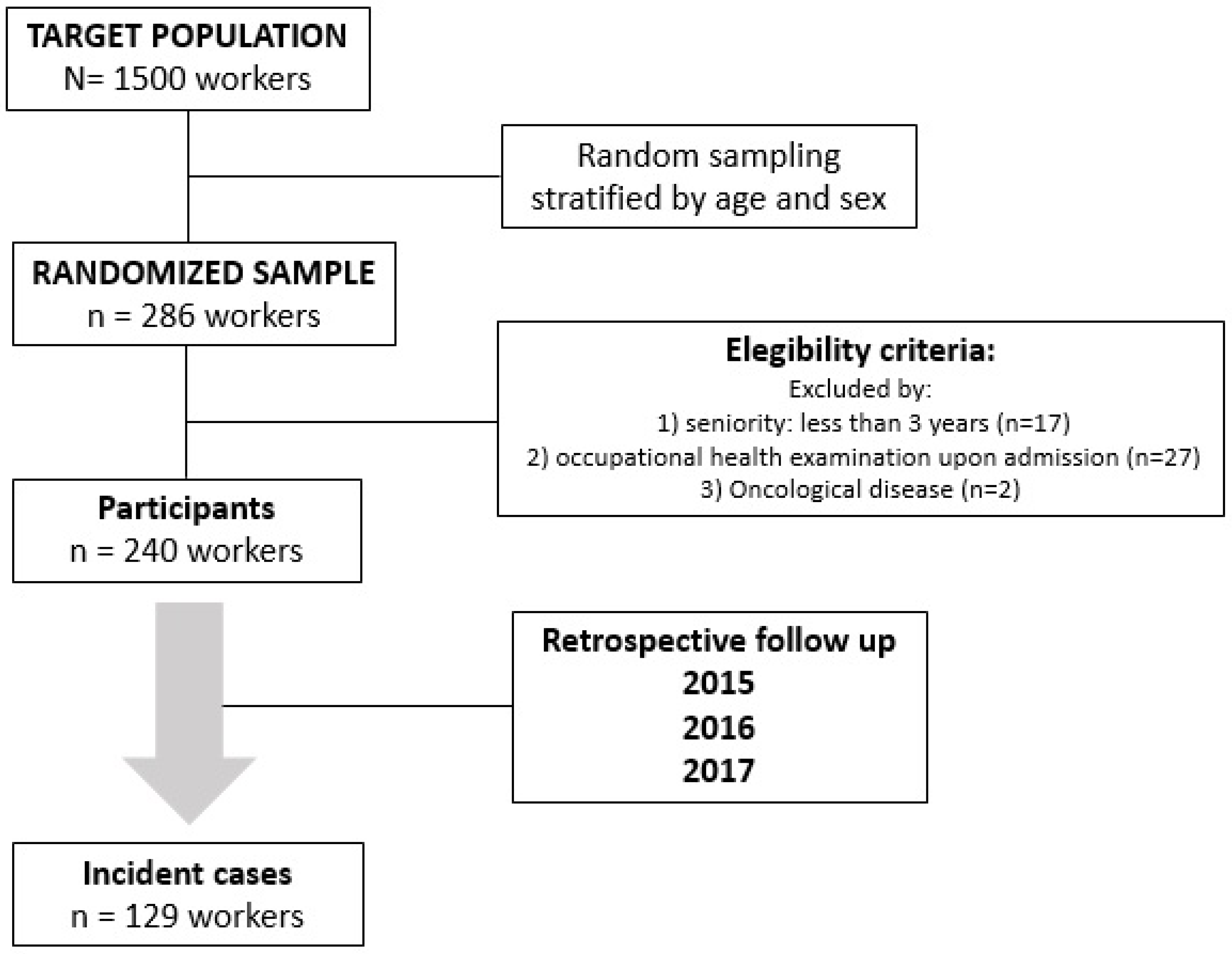
2.1. Study Design
2.2. Population and Sample
2.3. Eligibility Criteria
2.4. Study Variables and Measurement
2.5. Ethical and Legal Aspects
2.6. Data Analysis
3. Results
3.1. Temporary Disability
3.2. Adherence to the Mediterranean Diet and Physical Activity
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hill, P.W. mHealth: A cost-effective solution to chronic problems? J. Med. Therap. 2018, 2, 2–4. [Google Scholar] [CrossRef]
- World Health Organisation. Preventing Chronic Disease: Vital Investment. Available online: https://apps.who.int/iris/handle/10665/43314 (accessed on 3 March 2022).
- Kanerva, N.; Pietiläinen, O.; Lallukka, T.; Rahkonen, O.; Lahti, J. Unhealthy lifestyle and sleep problems as risk factors for increased direct employers’ cost of short-term sickness absence. Scand. J. Work Environ. Health 2018, 44, 192–201. [Google Scholar] [CrossRef] [PubMed]
- Tamers, S.L.; Streit, J.; Pana-Cryan, R.; Ray, T.; Syron, L.; Flynn, M.A.; Castillo, D.; Roth, G.; Geraci, C.; Guerin, R.; et al. Envisioning the future of work to safeguard the safety, health, and well-being of the workforce: A perspective from the CDC’s National Institute for Occupational Safety and Health. Am. J. Ind. Med. 2020, 63, 1065–1084. [Google Scholar] [CrossRef] [PubMed]
- Syed, I.U.B. Diet, physical activity, and emotional health: What works, what doesn’t, and why we need integrated solutions for total worker health. BMC Public Health 2020, 20, 152. [Google Scholar] [CrossRef] [PubMed]
- Nathan, N.; Murawski, B.; Hope, K.; Young, S.; Sutherland, R.; Hodder, R.; Booth, D.; Toomey, E.; Yoong, S.L.; Reilly, K.; et al. The Efficacy of Workplace Interventions on Improving the Dietary, Physical Activity and Sleep Behaviours of School and Childcare Staff: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 4998. [Google Scholar] [CrossRef]
- Holtermann, A.; Mathiassen, S.E.; Straker, L. Promoting health and physical capacity during productive work: The Goldilocks Principle. Scand. J. Work Environ. Health 2019, 45, 90–97. [Google Scholar] [CrossRef]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. PREDIMED Study Investigators. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts. N. Engl. J. Med. 2018, 378, 34. [Google Scholar] [CrossRef]
- Martínez-González, M.A.; Gea, A.; Ruiz-Canela, M. The Mediterranean Diet and Cardiovascular Health. Circ Res. 2019, 124, 779–798. [Google Scholar] [CrossRef]
- Di Daniele, N.; Noce, A.; Vidiri, M.F.; Moriconi, E.; Marrone, G.; Annicchiarico-Petruzzelli, M.; D’Urso, G.; Tesauro, M.; Rovella, V.; De Lorenzo, A. Impact of Mediterranean diet on metabolic syndrome, cancer and longevity. Oncotarget 2017, 8, 8947–8979. [Google Scholar] [CrossRef]
- D’Innocenzo, S.; Biagi, C.; Lanari, M. Obesity and the Mediterranean Diet: A Review of Evidence of the Role and Sustainability of the Mediterranean Diet. Nutrients 2019, 11, 1306. [Google Scholar] [CrossRef]
- Mentella, M.C.; Scaldaferri, F.; Ricci, C.; Gasbarrini, A.; Miggiano, G.A.D. Cancer and Mediterranean Diet: A Review. Nutrients 2019, 11, 2059. [Google Scholar] [CrossRef] [PubMed]
- Yammine, A.; Namsi, A.; Vervandier-Fasseur, D.; Mackrill, J.J.; Lizard, G.; Latruffe, N. Polyphenols of the Mediterranean diet and their metabolites in the prevention of colorectal cancer. Molecules 2021, 26, 3483. [Google Scholar] [CrossRef] [PubMed]
- Farràs, M.; Almanza-Aguilera, E.; Hernáez, Á.; Agustí, N.; Julve, J.; Fitó, M.; Castañer, O. Beneficial effects of olive oil and Mediterranean diet on cancer physio-pathology and incidence. Semin. Cancer Biol. 2021, 73, 178–195. [Google Scholar] [CrossRef] [PubMed]
- Tsai, S.Y. Effect of Yoga Exercise on Premenstrual Symptoms among Female Employees in Taiwan. Int. J. Environ. Res. Public Health 2016, 13, 721. [Google Scholar] [CrossRef]
- Ivandic, I.; Freeman, A.; Birner, U.; Nowak, D.; Sabariego, C. A systematic review of brief mental health and well-being interventions in organizational settings. Scand. J. Work Environ. Health 2017, 43, 99–108. [Google Scholar] [CrossRef]
- Albulescu, P.; Macsinga, I.; Rusu, A.; Sulea, C.; Bodnaru, A.; Tulbure, B.T. “Give me a break!” A systematic review and meta-analysis on the efficacy of micro-breaks for increasing well-being and performance. PLoS ONE 2022, 17, e0272460. [Google Scholar] [CrossRef]
- Barene, S.; Holtermann, A.; Oseland, H.; Brekke, O.L.; Krustrup, P. Effects on muscle strength, maximal jump height, flexibility and postural sway after soccer and Zumba exercise among female hospital employees: A 9-month randomised controlled trial. J. Sports Sci. 2016, 34, 1849–1858. [Google Scholar] [CrossRef]
- Ginoux, C.; Isoard-Gautheur, S.; Sarrazin, P. “Workplace Physical Activity Program” (WOPAP) study protocol: A four-arm. BMC Public Health 2019, 19, 289. [Google Scholar] [CrossRef]
- Mailey, E.L.; Rosenkranz, S.K.; Ablah, E.; Swank, A.; Casey, K. Effects of an Intervention to Reduce Sitting at Work on Arousal, Fatigue, and Mood Among Sedentary Female Employees: A Parallel-Group Randomized Trial. J. Occup. Environ. Med. 2017, 59, 1166–1171. [Google Scholar] [CrossRef]
- Pronk, N.P. Implementing movement at the workplace: Approaches to increase physical activity and reduce sedentary behavior in the context of work. Prog. Cardiovasc. Dis. 2021, 64, 17–21. [Google Scholar] [CrossRef]
- World Health Organization. International Guide for Monitoring Alcohol Consumption and Related Harm. Department of Mental Health and Substance Dependence. Available online: http://apps.who.int/iris/bitstream/handle/10665/66529/WHO_MSD_MSB_00.4.pdf;jsessionid=3704F27F9D5CCADC524C301D84CEB6CC?sequence=1 (accessed on 25 February 2022).
- Cancela, J.M.; Ayán, C.; Vila, H.; Gutierrez, J.M.; Gutierrez-Santiago, A. Validez de constructo del cuestionario internacional de actividad física en universitarios españoles. Rev. Iberoam. Diagnóstico Evaluación-E Avaliação Psicológica 2019, 52, 5–14. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean diet and survival in a Greek population. N. Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef]
- Høgsbro, C.; Davidsen, M.; Sørensen, J. Long-term sickness absence from work due to physical inactivity: A registry-based study. Scand. J. Public Health 2018, 46, 306–313. [Google Scholar] [CrossRef] [PubMed]
- López-Bueno, R.; Casajús-Mallén, J.A.; Garatachea-Vallejo, N. Physical activity as a tool to reduce disease-related work absenteeism in sedentary employees: A systematic review. Rev. Esp. Salud Publica 2018, 92, e201810071. [Google Scholar] [PubMed]
- Lahti, J.; Laaksonen, M.; Lahelma, E.; Rahkonen, O. The impact of physical activity on sickness absence. Scand. J. Med. Sci. Sports 2010, 20, 191–199. [Google Scholar] [CrossRef]
- Herruzo, B.; Martín, J.J.; Molina, G.; Romero, M.; Sanz, J.J.; Moreno, R. Promoción de la salud en el lugar de trabajo. Hábitos de vida saludable y factores de riesgo cardiovascular en trabajadores de ámbito sanitario en atención primaria. Rev. Asoc. Esp. Espec. Med. Trab. 2017, 26, 9–21. [Google Scholar]
- Proper, K.I.; van den Heuvel, S.G.; De Vroome, E.M.; Hildebrandt, V.H.; Van der Beek, A.J. Dose-response relation between physical activity and sick leave. Br. J. Sports Med. 2006, 40, 173–178. [Google Scholar] [CrossRef]
- Ball, K.; Carver, A.; Downing, K.; Jackson, M.; O’Rourke, K. Addressing the social determinants of inequities in physical activity and sedentary behaviours. Health Promot. Int. 2005, 30, ii8–ii19. [Google Scholar] [CrossRef]
- Laddu, D.; Paluch, A.E.; LaMonte, M.J. The role of the built environment in promoting movement and physical activity across the lifespan: Implications for public health. Prog. Cardiovasc. Dis. 2021, 64, 33–40. [Google Scholar] [CrossRef]
- Lobczowska, K.; Banik, A.; Forberger, S.; Kaczmarek, K.; Kubiak, T.; Neumann-Podczaska, A.; Romaniuk, P.; Scheidmeir, M.; Scheller, D.A.; Steinacker, J.M.; et al. Policy Evaluation Network (PEN) Consortium. Social, economic, political, and geographical context that counts: Meta-review of implementation determinants for policies promoting healthy diet and physical activity. BMC Public Health 2022, 22, 1055. [Google Scholar] [CrossRef]
- World Health Organization. Global Strategy on Diet, Physical Activity and Health. Available online: https://www.who.int/publications/i/item/9241592222 (accessed on 2 November 2022).
- Bantham, A.; Taverno Ross, S.E.; Sebastião, E.; Hall, G. Overcoming barriers to physical activity in underserved populations. Prog. Cardiovasc. Dis. 2021, 64, 64–71. [Google Scholar] [CrossRef] [PubMed]
- Tuttolomondo, A.; Simonetta, I.; Daidone, M.; Mogavero, A.; Ortello, A.; Pinto, A. Metabolic and Vascular Effect of the Mediterranean Diet. Int. J. Mol. Sci. 2019, 20, 4716. [Google Scholar] [CrossRef] [PubMed]
- Ramón-Arbués, E.; Martínez-Abadía, B.; Granada-López, J.M.; Echániz-Serrano, E.; Huércanos-Esparza, I.; Antón-Solanas, I. Association between adherence to the Mediterranean diet and the prevalence of cardiovascular risk factors. Rev. Lat.-Am. Enferm. 2020, 28, e3295. [Google Scholar] [CrossRef] [PubMed]
- Ruilope, L.M.; Catalina-Romero, C.; Sanchez-Chaparro, M.A.; Valdivielso, P.; Quevedo-Aguado, L.; Moral, I.; Brotons, C.; Calvo-Bonacho, E. Dietary habits and sick leave. Eur. Heart J. 2018, 39, 566–576. [Google Scholar] [CrossRef]
- Lemke, M.K. Is the Total Worker Health Program Missing Its Mark?: Integrating Complex Systems Approaches to Unify Vision and Epistemology. J. Occup. Environ. Med. 2021, 63, e304–e307. [Google Scholar] [CrossRef] [PubMed]
- Sorensen, G.; Dennerlein, J.T.; Peters, S.E.; Sabbath, E.L.; Kelly, E.L.; Wagner, G.R. The future of research on work, safety, health and wellbeing: A guiding conceptual framework. Soc. Sci. Med. 2021, 269, 113593. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Study Sample n = 240 | Reference Population N = 1500 | p |
|---|---|---|---|
| Men | 177 (73.8%) | 1039 (69.3%) | 0.18 |
| Women | 63 (26.2%) | 461 (30.4%) | 0.18 |
| Age (men) | 50.2 (8.3) | 49.5 (7.9) | 0.28 |
| Age (women) | 50.5 (6.3) | 50 (7.2) | 0.6 |
| Age (total) | 50.2 (7.9) | 49.7 (7.7) | 0.35 |
| Administrative professions | 109 (45.4%) | 565 (37.7%) | 0.02 |
| Trade professions | 59 (24.6%) | 419 (27.9%) | 0.33 |
| Security professions | 72 (30%) | 474 (31.6%) | 0.79 |
| Variable | n (%) | Duration Mean ± SD | Median Duration (IQR) | Range (Max-min) | p |
|---|---|---|---|---|---|
| Gender | 0.4 | ||||
| Men | 177 (73.8%) | 49.3 ± 97.8 | 7 (57.5) | 0–741 | |
| Women | 63 (26.2%) | 37.1 ± 103.8 | 0 (23) | 0–608 | |
| Alcohol consumption | 0.08 a | ||||
| None/Low | 192 (80%) | 40.4 ± 85.9 | 2 (45) | 0–608 | |
| Moderate/High | 48 (20%) | 68.7 ± 139.6 | 11 (75.8) | 0–741 | |
| Tobacco use | 0.37 a | ||||
| Non-smoker | 123 (51.25%) | 38.7 ± 72.8 | 4 (48) | 0–432 | |
| Smoker | 44 (18.3%) | 72.3 ± 143.6 | 6 (87.5) | 0–741 | |
| Ex-smoker | 73 (30.4%) | 42.6 ± 104.3 | 0 (37 | 0–608 | |
| Type of work | 0.001 a | ||||
| Administrative professions | 109 (45.4%) | 29.5 ± 75.1 | 0 (20.5) | 0–441 | |
| Trade professions | 59 (24.6%) | 74.5 ± 149 | 8 (78) | 0–741 | |
| Security professions | 72 (30%) | 47.8 ± 73.9 | 15.5 (77.8) | 0–417 |
| Components and Portions | n (%) | Duration Mean ± SD | p | |
|---|---|---|---|---|
| Olive oil (teaspoons per day) | <2 | 17 (7.1%) | 37.2 ± 57.4 | |
| ≥2 | 223 (92.9%) | 46.7 ± 101.8 | 0.7 | |
| Vegetables (servings per day) | <2 | 149 (62.1%) | 51.1 ± 106.3 | |
| ≥2 | 91 (37.9%) | 37.7 ± 86.6 | 0.3 | |
| Fruit (servings per day) | <3 | 146 (66.8%) | 45.2 ± 104.6 | |
| ≥3 | 94 (33.2%) | 47.4 ± 90.9 | 0.87 | |
| Red meat (servings per day) | <1 | 102 (42.5%) | 32.4 ± 59.9 | |
| ≥1 | 138 (57.5%) | 56.2 ± 119.6 | 0.067 | |
| Butter (servings per day) | <1 | 214 (89.2%) | 45.3 ± 98 | |
| ≥1 | 26 (10.8%) | 51.9 ± 111.4 | 0.75 | |
| Sugary drinks (per day) | <1 | 183 (76.25%) | 47.5 ± 107.6 | |
| ≥1 | 57 (23.75%) | 41.6 ± 66.4 | 0.7 | |
| Wine (glasses per week) | <3 | 175 (72.9%) | 41.6 ± 91.4 | |
| ≥3 | 64 (27.1%) | 59 ± 118.5 | 0.23 | |
| Pulses (servings per week) | <3 | 141 (58.75%) | 44.9 ± 88.4 | |
| ≥3 | 99 (41.25%) | 47.7 ± 113.5 | 0.8 | |
| Fish (servings per week) | <3 | 162 (67.5%) | 45.6 ± 97.7 | |
| ≥3 | 78 (32.5%) | 47 ± 103.2 | 0.9 | |
| Baked goods (servings per week) | <3 | 188 (78.3%) | 49.8 ± 97.7 | 0.27 |
| ≥3 | 52 (21.7%) | 47.7 ± 113.5 | ||
| Nuts (servings per week) | <1 | 38 (15.8%) | 70.3 ± 114.7 | |
| ≥1 | 202 (84.2%) | 41.5 ± 95.7 | 0.1 | |
| Fried food (servings per week) | <2 | 32 (13.3%) | 51 ± 130.1 | |
| ≥2 | 208 (86.7%) | 45.3 ± 94 | 0.34 |
| Level of Physical Activity | n (%) | Duration Mean ± SD | Duration Median (IQR) | Range (Max–Min) | p | |
|---|---|---|---|---|---|---|
| 3 categories | Sedentary–light Moderate High | 11 (4.6%) | 40.7 ± 59 | 3 (114) | 0–145 | 0.67 * |
| 72 (30%) | 68 ± 146.4 | 0 (78.8) | 0–741 | |||
| 157 (65.4%) | 36.3 ± 69.4 | 4 834.5) | 0–417 | |||
| 2 categories | Sedentary–light–moderate High | 83 (34.6%) | 64.4 ± 138.1 | 0 (80) | 0–744 | 0.085 |
| 157 (65.4%) | 36.3 ± 69.4 | 7 (45) | 0–444 | |||
| Quartiles (METs) | Q1 (<2455) | 60 (25%) | 84 ± 157.36 | 1.5 (96.5) | 0–741 | 0.002 |
| Q2 (2455–4000) | 60 (25%) | 19.4 ± 39.1 | 0 (18.5) | 0–212 | ||
| Q3 (4001–5700) | 60 (25%) | 32.2 ± 65.2 | 3.5 (39) | 0–417 | ||
| Q4 (>5700) | 60 (25%) | 48.6 ± 84 | 13 (60.3) | 0–444 | ||
| Variable | Coefficient | Standard Error | 95% CI | p |
|---|---|---|---|---|
| Trade professions | 51.5 | 15.8 | 20.2 to 82.7 | <0.01 |
| Security professions | 24 | 14.9 | −5.3 to 53.3 | 0.11 |
| High level of PA | −35.4 | 13.4 | −61.7 to −9 | <0.01 |
| Constant | 49.3 | 11.9 | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiménez-Mérida, R.; Romero-Saldaña, M.; de-Pedro-Jiménez, D.; Alcaide-Leyva, J.M.; Cantón-Habas, V.; Álvarez-Fernández, C.; Vaquero-Abellán, M. Lifestyle, Type of Work, and Temporary Disability: An Incidence Study of the Working Population. Int. J. Environ. Res. Public Health 2022, 19, 14932. https://doi.org/10.3390/ijerph192214932
Jiménez-Mérida R, Romero-Saldaña M, de-Pedro-Jiménez D, Alcaide-Leyva JM, Cantón-Habas V, Álvarez-Fernández C, Vaquero-Abellán M. Lifestyle, Type of Work, and Temporary Disability: An Incidence Study of the Working Population. International Journal of Environmental Research and Public Health. 2022; 19(22):14932. https://doi.org/10.3390/ijerph192214932
Chicago/Turabian StyleJiménez-Mérida, Rocío, Manuel Romero-Saldaña, Domingo de-Pedro-Jiménez, José Manuel Alcaide-Leyva, Vanesa Cantón-Habas, Carlos Álvarez-Fernández, and Manuel Vaquero-Abellán. 2022. "Lifestyle, Type of Work, and Temporary Disability: An Incidence Study of the Working Population" International Journal of Environmental Research and Public Health 19, no. 22: 14932. https://doi.org/10.3390/ijerph192214932
APA StyleJiménez-Mérida, R., Romero-Saldaña, M., de-Pedro-Jiménez, D., Alcaide-Leyva, J. M., Cantón-Habas, V., Álvarez-Fernández, C., & Vaquero-Abellán, M. (2022). Lifestyle, Type of Work, and Temporary Disability: An Incidence Study of the Working Population. International Journal of Environmental Research and Public Health, 19(22), 14932. https://doi.org/10.3390/ijerph192214932