Abstract
Introduction: One of the most frequent cardiac implantable electronic device (CIED) implantation complications is lead dislodgement, especially in the older adult population. Little evidence is available about the influence of frailty on the risk of lead dislodgment after CIED implantation procedures; thus, the evaluation of frailty could be relevant for the course and safety of the implantation procedure, especially among the elderly with cardiovascular diseases. This study aimed to assess the risks and predictors of early lead dislodgement in the elderly population. Methods: Between 2008 and 2021, 14,293 patients underwent implantations. In 400 elderly patients, lead dislodgement was confirmed, and frailty was retrospectively calculated. Results: The most frequent dislodgement according to the lead position was that of the atrial lead (133; 33.3%). In the logistic regression, frailty (OR: 1.8196, 95% CI:1.4991–2.2086; p < 0.0001) and age (OR: 1.0315, 95% CI:1.0005–1.0634; p < 0.0461) were independent predictors of early dislodgement. In the female group, frailty (OR: 2.1185, 95% CI: 1.5530–2.8899; p < 0.0001) was an independent predictor of early dislodgement. Similarly, in the male group, frailty (OR: 1.6321, 95% CI:1.2725–2.0934; p < 0.0001) was an independent predictor of early dislodgement. Conclusion: Lead dislodgement often occurs in the elderly. Frailty in both men and women is a predictive factor of early lead dislodgment. Evaluating frailty may be an essential element of proper selection, especially in the elderly undergoing CIED procedures, and, consequently, it could help prevent further complications.
1. Introduction
The constantly growing number of cardiac implantable electronic device (CIED) procedures, including the implantation of cardiac pacemakers (PM), implantable cardioverter-defibrillators (ICD), and resynchronization systems (CRT), is related to the aging of the population and the improvement of medical care. Lead technology has recently shown substantial progress, with a reduction in the number of implanted passive leads in favor of leads with active fixation [1,2,3]. Despite the benefits of lead technology, the number of CIED complications is in line with the number of implantation devices [4,5]. One of the most frequent CIED complications is lead dislodgement, which occurs in 2% [6] of cases and is associated with re-operation and following lead fixation [7]. Furthermore, Prutkin et al. [8] showed that lead dislodgement was one of the most substantial risk factors for CIED infection. Early lead dislodgement prolongs hospitalization time and increases patient discomfort [9]. The reasons for lead dislodgement can be spontaneous or related to additional procedures. The data from REPLACE Registry showed that 7.9% of lead dislodgements in patients were in those undergoing device upgrades or pocket revision [10,11]. Another type of lead dislodgement is atrial or ventricular perforation caused by CIED leads. This is rare but potentially life-threatening [2,6,12]. Lead dislodgements can also result in complications, including cardiac tamponade, cardiac arrest, pneumothorax, and pacing failure, leading to hemodynamic instability and sudden death [11,13]. Moreover, there is no clear evidence of how age influences the risk of lead dislodgement in older patients. An essential part of biological age is frailty, which is a predictive factor often used in gerontology and cardiology and which may play a key role in electrotherapy [14]. Little evidence is available about the influence of frailty on the risk of dislocation after CIED implantation procedures, thus the evaluation of frailty could be relevant for the course and safety of the implantation procedure, especially among the elderly with cardiovascular diseases (CVDs) [15]. Therefore, this study aimed to assess the number of lead dislodgements in the elderly population and to analyze the risk factors that might affect early dislodgment occurrence.
2. Materials and Methods
A total of 14,293 patients were hospitalized between 2008 and 2021 in the Electrocardiology Department for de novo CIED implantation, including PM, ICD, and CRT. The data of 480 patients with lead dislodgement were entered into the retrospective registry, and a group of elderly patients aged 60 or older was selected. The study design and patient selection are summarized in a flowchart in Figure 1.
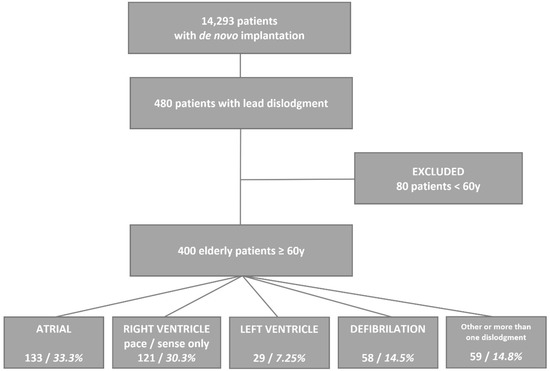
Figure 1.
Study design and patient selection.
Arterial hypertension was the most common comorbid disease (84.1%) in the enrolled patients. The next most common comorbidities were ischemic heart disease (56.9%), atrial fibrillation (41.6%), heart failure (36.6%) and diabetes (30.4%). Most patients received ACE blockers (83.4%), B-blockers (74.8%), calcium blockers (70.3%) and statins (67.1%).
Episodes of lead dislodgement data were divided into two categories: early (up to 30 days from implantation) and late (more than 30 days from implantation). The existence and intensity of frailty in the analyzed patients were calculated retrospectively.
2.1. Frailty Evaluation
Frailty was retrospectively based on data before CIED implantation evaluated using the 7-point Canadian Study of Health and Aging Clinical Frailty Scale (CSHA-CFS). This scale has good predictive validity (regarding death and the need for institutional care), and its predictive power relies on clinical judgment. Values = 4 described patients who might be in danger of developing frailty. Patients with values ≥ 5 were recognized with as having frailty. The detailed description of the individual points is follows, according to The Canadian Study of Health and Aging Clinical Frailty Scale [16]:
- Very fit—Robust active, energetic, well-motivated, and fit; these people commonly exercise regularly and are in the fittest group for their age.
- Well—Without any active disease, but less fit than people in category 1.
- Well, with treated comorbid disease—Disease symptoms are well controlled compared to those in category 4.
- Apparently vulnerable—Although not clinically dependent, these people commonly complain of being “slowed down” or having disease symptoms.
- Mildly frail—With limited dependence on others for the instrumental activities of daily living.
- Moderately frail—Help is needed with both the instrumental and non-instrumental activities of daily living.
- Severely frail—Completely dependent on others for the activities of daily living or terminally ill.
2.2. Statistical Analysis
In order to check the normality of the data distribution, the Shapiro–Wilk test was used. Logistic regression analysis was used to predict factors responsible for lead dislodgement. The ROC curve analysis was performed to assess the value of frailty to predict a higher risk of dislodgement.
The results were considered significant at p-values < 0.05. All the presented analyses were performed using MedCalc® Statistical Software version 20.114 (MedCalc Software Ltd., Ostend, Belgium).
2.3. Bioethical Consideration
Participation in this study was anonymous and voluntary. The Local Bioethics Committee of the Medical University of Silesia approved the study protocol (PCN/CBN/0022/KB/8/22). When the study was designed, the protocol complied with the current version of the Helsinki Convention.
3. Results
In 400 elderly patients (187 women; aged 74. 0 ± 7.9 for a fourteen-year follow-up), one or more lead dislodgements were noted, and a lead correction procedure was also performed. The exact annual number of dislodgements is presented in Figure 2. In 361 patients, one lead dislodgement was found (90.3%); in 37 patients, two leads were dislodged (9.3%), and three leads were dislodged in two patients (0.5%). A total of 67.5% of devices with dislodgment of the lead(s) were cardiac pacemakers, 12% were implanted cardioverter defibrillators (ICD), 18% were cardiac resynchronization with implanted cardioverter defibrillators (CRT-D) and 2.5% were cardiac resynchronization devices (CRT-P).
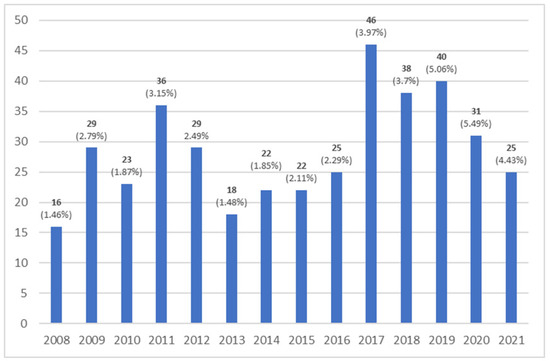
Figure 2.
Annual number of dislodgements.
The frequency of dislodgement according to the lead position was as follows: atrial lead (133; 33.3%), right ventricle pace/sense only (121; 30.3%), and left ventricle (29; 7.25%). Defibrillation lead dislodgement was found in 58 (14.5%) cases. Additionally, the His pacing lead was dislocated in 13 patients (3.3%). In five patients (1.3%), the temporary pacing lead was dislodged, and in one case (0.3%), the left bundle branch pacing lead was dislodged. In all other cases, two or more leads were dislodged.
In the logistic regression, frailty (OR: 1.8196, 95% CI:1.4991–2.2086; p < 0.0001; Nagelkerke R2 = 0.1635) and age (OR: 1.0315, 95% CI:1.0005–1.0634; p < 0.0461; Nagelkerke R2 = 0.1635) were independent predictors of early dislodgement. Detailed regression results are presented in Table 1.

Table 1.
Detailed results of logistic regression.
The ROC curves for frailty and early dislodgement are presented in Figure 3. The area under the curve was 0.714 (95% CI:0.667–0.758). The cutoff value for recognizing frailty was > 4 (p < 0.0001).
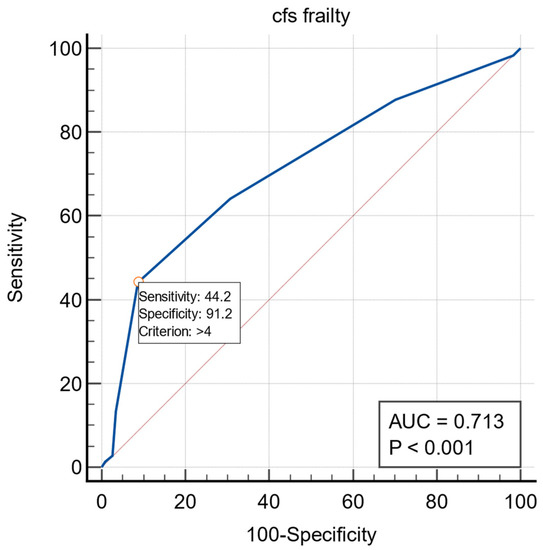
Figure 3.
The ROC curves for frailty and dislodgement.
In the logistic regression in the female group, frailty (OR: 2.1185, 95% CI: 1.5530–2.8899; p < 0.0001; Nagelkerke R2 = 0.2214) was an independent predictor of early dislodgement. Detailed regression results are presented in Table 2.
Table 2.
Detailed results of logistic regression—female subgroup.
The ROC curves for frailty and early dislodgement are presented in Figure 4. The area under the curve was 0.737 (95% CI: 0.668–0.799). The cutoff value for recognizing frailty was >4 (p < 0.0001).
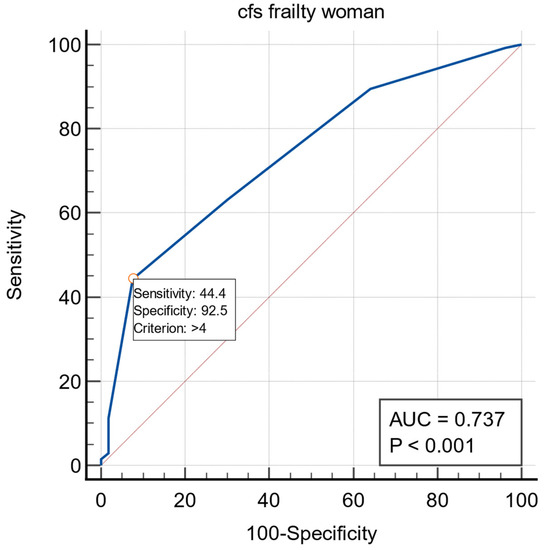
Figure 4.
The ROC curves for frailty in the dislodgement in female subgroup.
The same observation in the male group was performed. In the logistic regression, frailty (OR: 1.6321, 95% CI: 1.2725–2.0934; p < 0.0001; Nagelkerke R2 = 0.1218) was an independent predictor of early dislodgement. Detailed regression results are presented in Table 3.
Table 3.
Detailed results of logistic regression—male subgroup.
The ROC curves for frailty and early dislodgement are presented in Figure 5. The area under the curve was 0.695 (95% CI: 0.629–0.756). The cutoff value for recognizing frailty was 4 (p < 0.0001).
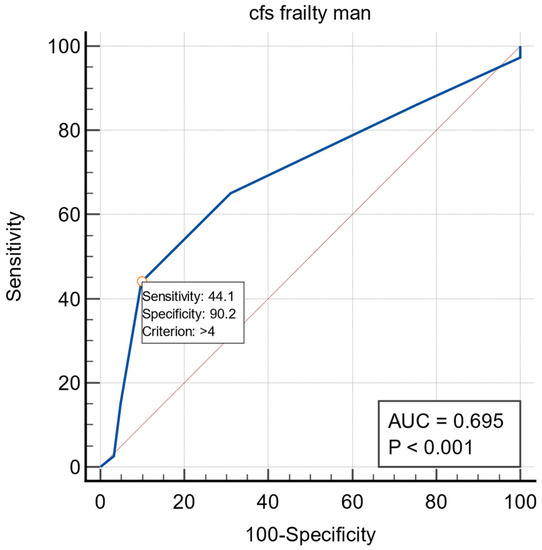
Figure 5.
The ROC curves for frailty in the dislodgement in male subgroup.
4. Discussion
Increasing use of CIEDs is associated with increased complications, including lead dislodgements. Recently, numerous studies have evaluated the risk factors of lead dislodgements [6,13,17,18]. For instance, Dębski et al. [17] showed that atrial lead position is an independent risk factor of lead dislodgement. Moreover, the authors indicate that the younger the age at implantation, the higher the probability of lead failure (odds ratio: 0.985; p < 0.001) [17]. Furthermore, Ghani et al. [6] presented an analysis of 3909 implantation leads and showed that right atrial and ICD lead dislodgements are more frequent than right ventricular lead dislodgements. Moreover, they report that lead dislodgements were more often observed in resynchronization systems with ICD and dual-chamber cardioverter-defibrillators than single-chamber PMs. The MOST trial [18] showed that the most common complication is dislodgement of the right atrial lead (1.7%) in the first 30 days after implantation.
In a subgroup analysis of the MIRACLE ICD study, Cheng et al. reported that older age, female sex, atrial fibrillation, and left ventricular leads are linked to a higher rate of acute lead dislodgement [13]. Furthermore, the authors showed that females had higher complication rates (95% CI: 0.98 to 1.99, p = 0.06) but without specifying dislodgements. It is known from the literature that the implantation of CIEDs in advanced age is an independent risk factor for in-hospital mortality [19,20]. Thus, the indication and need for intervention should be determined carefully, particularly in elderly patients. In this report, sex, age, and frailty were independent predictors of early lead dislodgement. However, data on the effect of the frailty syndrome on the occurrence of lead dislodgement are scarce. Frailty is a health condition associated with the aging of the population [21].
Moreover, frailty is frequently overlooked and identified with comorbidities. It is a state of limited capacity reserve of essential systems and their homeostasis. Frailty is caused when chronic inflammation leads to kinesiophobia and further progression of cardiovascular, immune, musculoskeletal, and hematopoietic failure; it results in increased morbidity and mortality [22]. A study by Mlynarska et al. demonstrated that frailty syndrome has a negative impact on the quality of life of patients who qualify for the implantation of CIEDs [23]. Frailty has also been identified as a predictor of poor CRT therapy outcomes [24] and predicts the maintenance of sinus rhythm in the elderly after cardioversion [25].
Furthermore, it has recently been shown that a higher frailty syndrome score is observed in the elderly with accompanying cardiac arrhythmias [26]. Therefore, our results showed the risk of early lead dislodgement by calculating the severity of frailty. Evaluating the occurrence of frailty may be an essential element of the proper selection of elderly patients to undergo CIED procedures. This could help prevent further complications and improve clinical outcomes. In addition, results noted in our study provide insight into carrying out better and faster follow-ups after CIED implantation, especially among patients with high frailty rates. Moreover, studies show that it is necessary to avoid the inadequate lead position during CIED implantation due to the high risk of perforation, especially in the right ventricle’s apex and the right atrium’s lateral wall [6]. In earlier studies, attempts have been made to establish [27] the benefits of implanting single-lead atrioventricular pacemakers performed without fluoroscopy. This report showed that using single-lead VDD pacemakers with electroanatomic navigation systems (The NavX system) would allow dependable visualization of the implantation site. Thus, our study provides the framework for future studies to assess another implantation techniques and choose the most satisfactory option for the elderly. Recently, Pagan et al. [28] presented evidence suggesting that leadless pacemakers are safe alternatives with low rates of procedure-related complications for old, frail patients. In this context, further investigations of appropriate implantation techniques, lead construction technology, and diagnosis of frailty may ensure a high success rate in all patients, especially among the elderly.
Important problems which should be answered is to distinguish between micro and macro dislodgments. Chest radiography allows us to find true, massive dislocations (visible in the radiological assessment), but there is no definition of micro-dislocation, which is often difficult to find. This lack of explicit criteria resulted in the lack of such analyses in the presented paper.
Significant problems related to the implanted cardiological leads are, e.g., too early patient agitation after implantation with psychomotor agitation and inappropriate movements of the limbs and chest, traumatic events, and manipulations in the area of the CIED which can cause possible Twiddler’s syndrome. All of these can potentially be responsible for lead(s) dislodgment. In older adults with frailty syndrome, early autonomous mobilization by the patient or alterations of CIED due to weight loss should also be analyzed. This is especially important in the case of patients at risk of lead dislodgment. Based on the presented analysis, it seems that older adults qualifying for CIED implantation should be especially cared for to prevent lead dislocation.
5. Conclusions
In just over 14,000 CIED procedures performed in the past 14 years, the most frequent dislodgement observed was atrial lead dislodgement. Additionally, we report that the incidence of lead dislodgement is high in the elderly. Frailty in both men and women is predictive of early lead dislodgment. Thus, our findings show that the estimation of the prevalence of frailty could be included in routine CIED management to enable high clinical and procedural success.
6. Limitations
The main limitations of the study were the single center and the study’s observational nature. No data were collected on implantation techniques leading to lead dislodgements. In addition, the regression models do not include adjustments for other factors beyond sex and age.
Author Contributions
Conceptualization, R.M., A.M., M.J., S.G.-W. and K.S.G.; methodology, R.M., A.M., M.J., S.G.-W. and K.S.G.; software, R.M., M.J. and K.S.G.; validation, R.M., A.M., M.J., S.G.-W. and K.S.G.; formal analysis, R.M., A.M., M.J., S.G.-W. and K.S.G.; investigation, R.M., A.M., M.J., S.G.-W., M.H., J.S. and K.S.G.; resources, R.M., A.M., M.J., S.G.-W. and K.S.G.; data curation, R.M., A.M., M.J., S.G.-W. and K.S.G.; writing—original draft preparation, R.M., A.M., M.J. and S.G.-W.; writing—review and editing, K.S.G.; visualization, R.M., A.M., M.J., S.G.-W. and K.S.G.; supervision, R.M. and K.S.G.; project administration, R.M., A.M., M.J., S.G.-W., M.H., J.S. and K.S.G.; funding acquisition, R.M., A.M., M.J., S.G.-W. and K.S.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research was founded by the Medical University of Silesia in Katowice, grant number PCN-1-109/N/1/K.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Local Bioethics Committee of Medical University of Silesia (protocol code PCN/CBN/0022/KB/8/22).
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Sterliński, M.; Przybylski, A.; Maciąg, A.; Syska, P.; Pytkowski, M.; Lewandowski, M.; Kowalik, I.; Firek, B.; Kołsut, P.; Religa, G.; et al. Subacute cardiac perforations associated with active fixation leads. Europace 2008, 11, 206–212. [Google Scholar] [CrossRef] [PubMed]
- Mahapatra, S.; Bybee, K.A.; Bunch, T.J.; Espinosa, R.E.; Sinak, L.J.; McGoon, M.D.; Hayes, D.L. Incidence and predictors of cardiac perforation after permanent pacemaker placement. Heart Rhythm 2005, 2, 907–911. [Google Scholar] [CrossRef] [PubMed]
- Ohlow, M.A.; Lauer, B.; Brunelli, M.; Geller, J.C. Incidence and predictors of pericardial effusion after permanent heart rhythm device implantation: Prospective evaluation of 968 consecutive patients. Circ. J. 2013, 77, 975–981. [Google Scholar] [CrossRef] [PubMed]
- Tracy, C.M.; Epstein, A.E.; Darbar, D.; Dimarco, J.P.; Dunbar, S.B.; Estes, N.A.M.; Ferguson, T.B.; Hammill, S.C.; Karasik, P.E.; Link, M.S.; et al. 2012 ACCF/AHA/HRS Focused Update of the 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Heart Rhythm 2012, 9, 1737–1753. [Google Scholar] [CrossRef] [PubMed]
- van Rees, J.B.; de Bie, M.K.; Thijssen, J.; Borleffs, C.J.W.; Schalij, M.J.; van Erven, L. Implantation-related complications of implantable cardioverter-defibrillators and cardiac resynchronization therapy devices: A systematic review of randomized clinical trials. J. Am. Coll Cardiol. 2011, 58, 995–1000. [Google Scholar] [CrossRef]
- Ghani, A.; Delnoy, P.P.H.M.; Misier, A.R.R.; Smit, J.J.J.; Adiyaman, A.; Ottervanger, J.P.; Elvan, A. Incidence of lead dislodgement, malfunction and perforation during the first year following device implantation. Neth. Heart J. 2014, 22, 286–291. [Google Scholar] [CrossRef] [PubMed]
- Polyzos, K.; Konstantelias, A.A.; Falagas, M.E. Risk factors for cardiac implantable electronic device infection: A systematic review and meta-analysis. Europace 2015, 17, 767–777. [Google Scholar] [CrossRef]
- Prutkin, J.M.; Reynolds, M.R.; Bao, H.; Curtis, J.P.; Al-Khatib, S.M.; Aggarwal, S.; Uslan, D.Z. Response to Letter Regarding Article, “Rates of and Factors Associated With Infection in 200 909 Medicare Implantable Cardioverter-Defibrillator Implants: Results From the National Cardiovascular Data Registry”. Circulation 2015, 131, e518. [Google Scholar] [CrossRef][Green Version]
- Traykov, V.; Bongiorni, M.G.; Boriani, G.; Burri, H.; Costa, R.; Dagres, N.; Deharo, J.-C.; Epstein, L.; Erba, P.A.; Snygg-Martin, U.; et al. Clinical practice and implementation of guidelines for the prevention, diagnosis and management of cardiac implantable electronic device infections: Results of a worldwide survey under the auspices of the European Heart Rhythm Association. Europace 2019, 21, 1270–1279. [Google Scholar] [CrossRef]
- Poole, J.E.; Gleva, M.J.; Mela, T.; Chung, M.K.; Uslan, D.Z.; Borge, R.; Gottipaty, V.; Shinn, T.; Dan, D.; Feldman, L.A.; et al. Complication rates associated with pacemaker or implantable cardioverter-defibrillator generator replacements and upgrade procedures: Results from the REPLACE registry. Circulation 2010, 122, 1553–1561. [Google Scholar] [CrossRef]
- Afzal, M.R.; Horner, S.; Matre, N.B.; Blake, P.; Dunham, K.; Pinkhas, D.; Okabe, T.; Tyler, J.; Houmsse, M.; Kalbfleisch, S.J.; et al. Comprehensive strategy to reduce the incidence of lead dislodgement for cardiac implantable electronic devices. Pacing Clin. Electrophysiol. 2018, 42, 58–62. [Google Scholar] [CrossRef] [PubMed]
- Migliore, F.; Zorzi, A.; Bertaglia, E.; Leoni, L.; Siciliano, M.; de Lazzari, M.; Ignatiuk, B.; Veronese, M.; Verlato, R.; Tarantini, G.; et al. Incidence, Management, and Prevention of Right Ventricular Perforation by Pacemaker and Implantable Cardioverter Defibrillator Leads. Pacing Clin. Electrophysiol. 2014, 37, 1602–1609. [Google Scholar] [CrossRef] [PubMed]
- Cheng, A.; Wang, Y.; Curtis, J.P.; Varosy, P.D. Acute Lead Dislodgements and In-Hospital Mortality in Patients Enrolled in the National Cardiovascular Data Registry Implantable Cardioverter Defibrillator Registry. J. Am. Coll. Cardiol. 2010, 56, 1651–1656. [Google Scholar] [CrossRef] [PubMed]
- Manzano, L.; Babalis, D.; Roughton, M.; Shibata, M.; Anker, S.D.; Ghio, S.; van Veldhuisen, D.J.; Cohen-Solal, A.; Coats, A.J.; Poole-Wilson, P.P.; et al. Predictors of clinical outcomes in elderly patients with heart failure. Eur. J. Heart Fail. 2011, 13, 528–536. [Google Scholar] [CrossRef]
- Singh, M.; Stewart, R.; White, H. Importance of frailty in patients with cardiovascular disease. Eur. Heart J. 2014, 35, 1726–1731. [Google Scholar] [CrossRef]
- Rockwood, K.; Song, X.; MacKnight, C.; Bergman, H.; Hogan, D.B.; McDowell, I.; Mitnitski, A. A global clinical measure of fitness and frailty in elderly people. CMAJ 2005, 173, 489–495. [Google Scholar] [CrossRef]
- Dębski, M.; Ulman, M.; Ząbek, A.; Boczar, K.; Haberka, K.; Kuniewicz, M.; Lelakowski, J.; Małecka, B. Lead-related complications after DDD pacemaker implantation. Kardiol. Polska 2018, 76, 1224–1231. [Google Scholar] [CrossRef]
- Ellenbogen, K.A.; Hellkamp, A.S.; Wilkoff, B.; Camunãs, J.L.; Love, J.C.; Hadjis, T.A.; Lee, K.L.; Lamas, G.A. Complications arising after implantation of DDD pacemakers: The MOST experience. Am. J. Cardiol. 2003, 92, 740–741. [Google Scholar] [CrossRef]
- Swindle, J.P.; Rich, M.W.; McCann, P.; Burroughs, T.E.; Hauptman, P.J. Implantable cardiac device procedures in older pa-tients: Use and in-hospital outcomes. Arch. Intern. Med. 2010, 170, 631–637. [Google Scholar] [CrossRef][Green Version]
- Huang, D.T.; Sesselberg, H.W.; McNitt, S.; Noyes, K.; Andrews, M.L.; Hall, W.J.; Dick, A.; Daubert, J.P.; Zareba, W.; Moss, A.J.; et al. Improved Survival Associated with Prophylactic Implantable Defibrillators in Elderly Patients with Prior Myocardial Infarction and Depressed Ventricular Function: A MADIT-II Substudy. J. Cardiovasc. Electrophysiol. 2007, 18, 833–838. [Google Scholar] [CrossRef]
- Buckinx, F.; Rolland, Y.; Reginster, J.Y.; Ricour, C.; Petermans, J.; Bruyère, O. Burden of frailty in the elderly population: Per-spectives for a public health challenge. Arch Public Health 2015, 73, 19. [Google Scholar] [CrossRef] [PubMed]
- Kluszczyńska, M.; Młynarska, A.; Mikulakova, W. Influence of Frailty Syndrome on Kinesiophobia According to the Gender of Patients after Coronary Artery Bypass Surgery. Healthcare 2021, 9, 730. [Google Scholar] [CrossRef] [PubMed]
- Mlynarska, A.; Mlynarski, R.; Golba, K.S. Influence of frailty on the quality of life patients qualified for pacemaker implantation. J. Clin. Nurs. 2017, 27, 555–560. [Google Scholar] [CrossRef] [PubMed]
- Mlynarska, A.; Mlynarski, R.; Golba, K. Frailty as a predictor of negative outcomes after cardiac resynchronization therapy. Pacing Clin. Electrophysiol. 2018, 41, 572–577. [Google Scholar] [CrossRef] [PubMed]
- Mlynarska, A.; Mlynarski, R.; Marcisz, C.; Golba, K.S. Modified frailty as a novel factor in predicting the response to cardiac resynchronization in the elderly population. Clin. Interv. Aging 2019, 14, 437–443. [Google Scholar] [CrossRef]
- Mlynarska, A.; Mlynarski, R.; Golba, K.S. Frailty syndrome in patients with heart rhythm disorders. Geriatr. Gerontol. Int. 2016, 17, 1313–1318. [Google Scholar] [CrossRef]
- Ruiz-Granell, R.; Ferrero, A.; Morell-Cabedo, S.; Martinez-Brotons, A.; Bertomeu, V.; Llacer, A.; García-Civera, R. Implantation of sin-gle-lead atrioventricular permanent pacemakers guided by electroanatomic navigation without the use of fluoroscopy. Europace 2008, 10, 1048–1051. [Google Scholar] [CrossRef]
- Pagan, E.; Gabriels, J.; Khodak, A.; Chang, D.; Beldner, S.; Epstein, L.M.; Willner, J. Safety of leadless pacemaker implantation in the very elderly. Heart Rhythm 2020, 17, 2023–2028. [Google Scholar] [CrossRef]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).