
Physical as Well as Psychological Distress and Coping with Situational Dilemmas Experienced by People Infected with COVID-19: A Mixed Method Study


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participant Recruitment
2.2. Sample
2.3. Protocol
2.3.1. Phase 1: Qualitative Study
2.3.2. Phase 2: Building an Instrument
2.3.3. Phase 3: Quantitative Study
2.4. Data Analysis
Rigor and Trustworthiness
2.5. Ethical Aspects
3. Results
3.1. Characterization of the Study Participants
3.2. Mixed Method Study
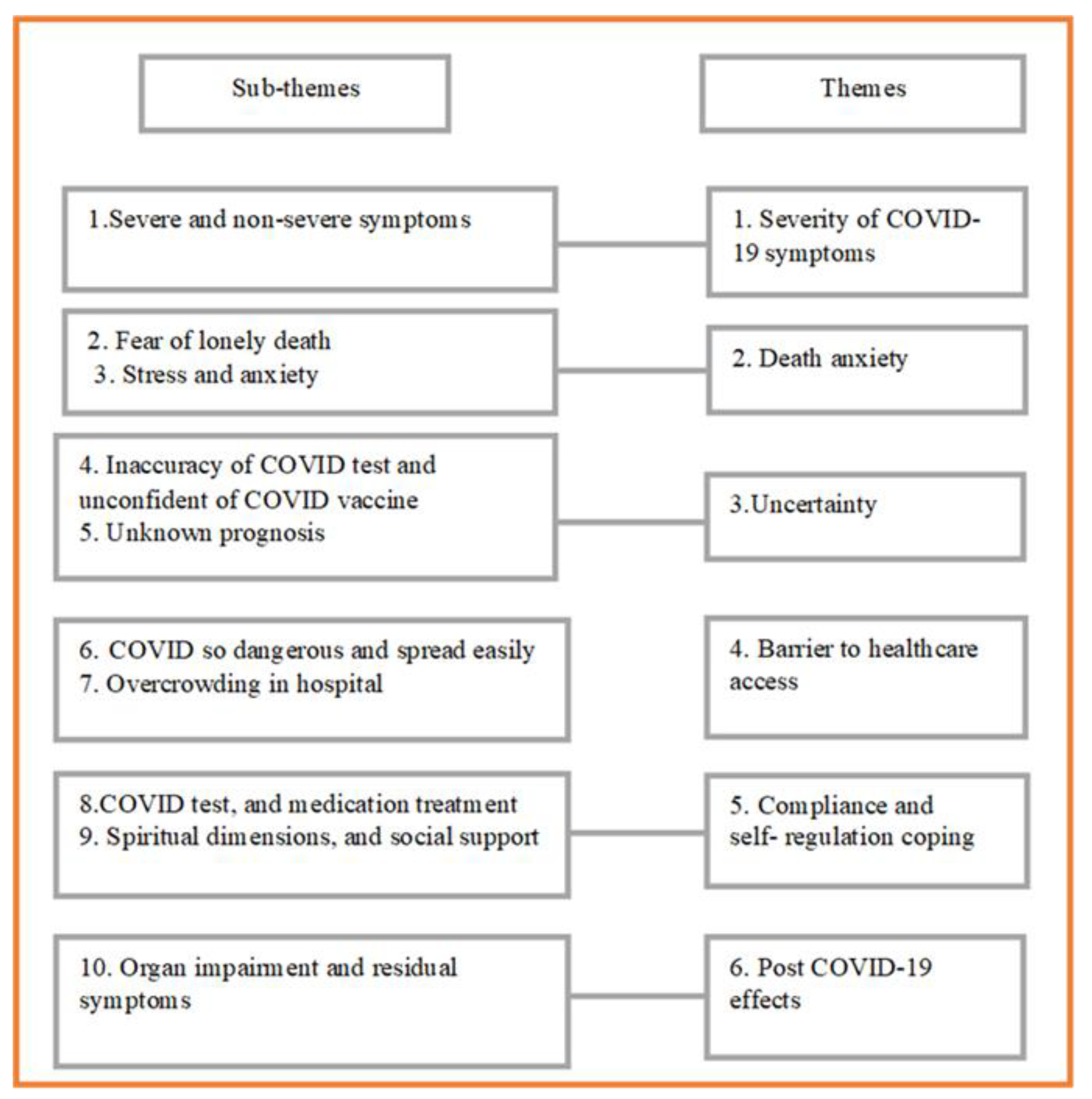
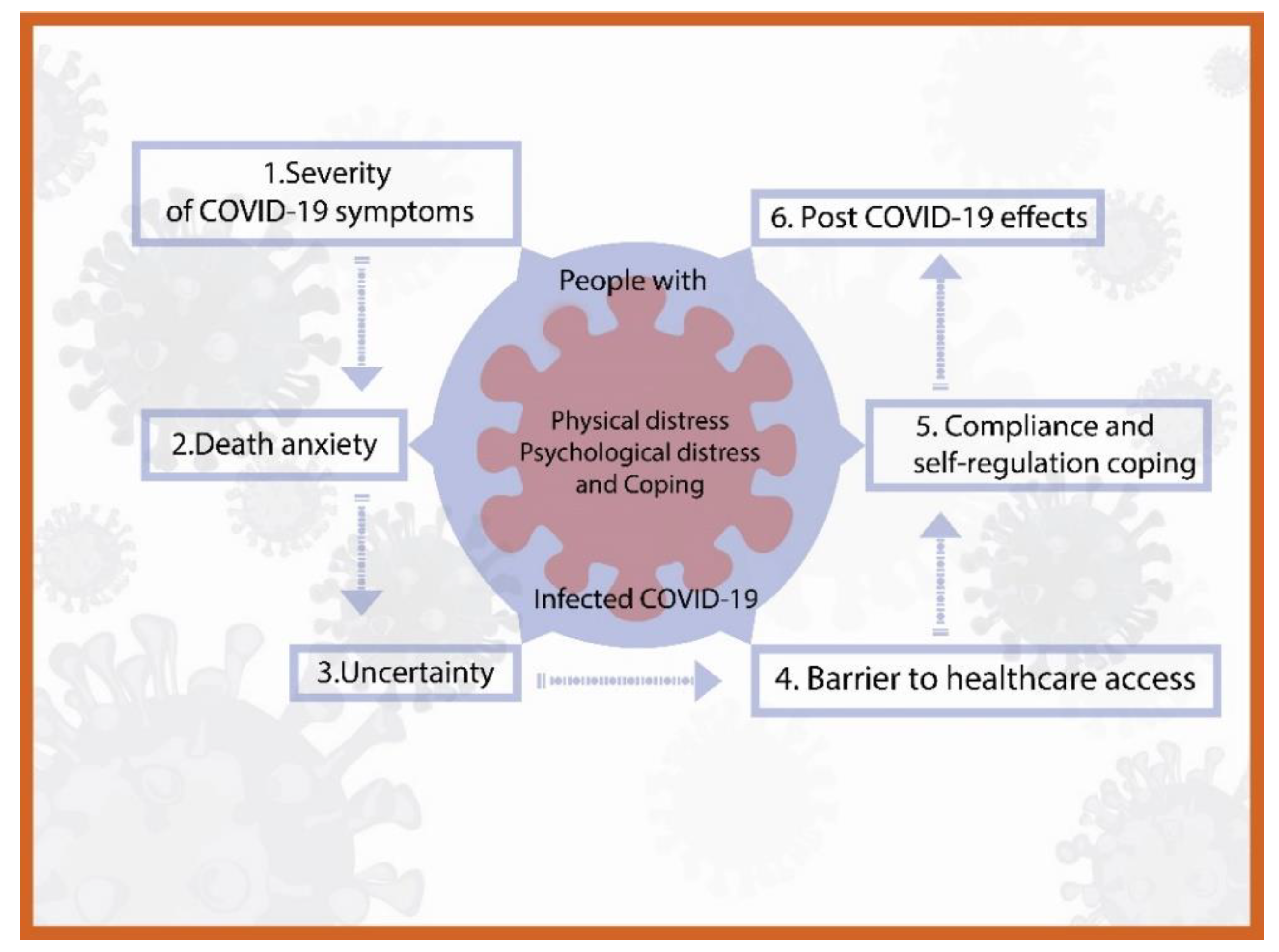
3.2.1. Theme 1: Severity of COVID-19 Symptoms
“I have high fever and chills. I took medication and warm wiped to reduce fever. It helped me a bit. The nurses helped me by giving me some oxygen but it didn’t work well and after that I blacked out. When I was conscious again, a tube was inserted in my throat and connected to the monitor. There were many tubes on me. A few days later the doctor had to make a hole on the outside of my throat to help me breathe better. I was admitted into ICU for 30 days and was transferred to the primary hospital for 10 more days.”(S-female, 47 y)
“I had mild symptoms, having low fever, headache, body aches but, I was in a risk group I have cancer and on chemotherapy. The doctor advised me to be admitted. When I walked to the toilet, I felt very tired. I needed to have oxygen and took Favipiravir after which I felt better. I stayed in the hospital for 4 days and 14 days in home isolation.”(N-S 10- female, 59 y)
3.2.2. Theme 2: Death Anxiety
“At that moment, I was so worried and feared death. I was not ready to die and I hadn’t done anything yet about my assets and will management.”(S- male, 75 y)
“For me, I had mild symptoms, took anti-viral drugs for 2–3 days. I felt much better, but my 2-year-old daughter had a fever and her ATK test was positive. Her fever wasn’t that high but she developed a seizure. I’m so sorry for her, I felt so sad and worried about her. I didn’t want to lose her and I cried a lot, couldn’t sleep. I had no time to rest. I started to have chest pain, shortness of breath and was coughing a lot. I couldn’t stand how I felt at that time. Then I thought that I had to be stronger in order to look after my daughter. Two months have passed and I’m still scared for her.”(NS- male, 43 y)
3.2.3. Theme 3 Uncertainty
“I was not expected to be infected. There were problems with both the ATK and PCR test results. I had done the test 4 times and the results were negative until the fifth time when mine was positive. In spite of the onset of the symptoms became apparent and getting worse.”(NS- male, 43 y)
“I was admitted for oxygen therapy at all time. I received the bad news during my admission that my son who had cirrhosis of the liver with COVID infection died after 5 days admission to hospital.”
“I was so sad, I did not expect him to die so soon. It was reality uncertainty.”(S- female 75 y)
“I protected myself strictly because my work was related to COVID infection patients. I wore N 95 double masks and face shield all time including washing my hands frequently. The first COVID infection was on 24 August 2021. I had got it from my workplace and Delta virus was found. On 5 March 2022, I was infected again with Omicron virus…I could not believe it.”(NS- male, 30 y)
3.2.4. Theme 4: Barrier to Healthcare Access
“I was certain that the Delta virus was very dangerous, even though I protected myself really well but I still got it.”(NS- male, 43 y)
“In 2021, while I was infected, the situation was so scary. There were many infected people taken by ambulances to the hospitals but there were not enough health services, not even COVID screening.”(S- male, 75 y)
“I contacted many hospitals in Bangkok but there was not a place offering a COVID test and the admission wait was 3 days. I began to feel worse, so my husband with my child took me in our car up country, more than 400 km away. Luckily, I was admitted to a hospital; if not, I would have died.”(S- female, 47 y)
3.2.5. Theme 5: Compliance and Self-Regulation Coping
“I prayed with a little Buddha image which I brought with me to the ICU that made me mindful, distractions, lay on lateral side and on oxygen therapy all the time as the nurse advised and I felt better.”(S- pregnant woman, 31 y)
“The nurses advised me to lay on my stomach and I did as they advised. I could do only 5–7 min in the daytime, but the night time I was so afraid that no one could come to help me in case the oxygen tube was missing.”(S- female, 75 y)
“My daughter who looked after me, called the ambulance which took me to the hospital. She had talked to the doctor via phone every day and let me know all that.”(S- male, 75 y)
3.2.6. Theme 6: Post-COVID-19 Effects
“I was discharged 6 months ago. At the moment, I am not the same. I am easily tired. My sugar level has increased and the doctor prescribed me more medication for my DM.”(S- female, 47 y)
“After my baby was born by cesarean surgery his weight was 3000 g and being easy baby. The doctor told me that he had abnormal heart valves. There were both of leakage on the right side and stenosis on the tip of lung. I believed it was caused by the COVID infection but the doctor stated that the baby might have had it as a congenital disease.”(S- pregnant female, 29 y)
4. Discussion
5. Limitation
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- The Bureau of Registration Administration. Population Statistics, Civil Registration (Monthly). 2022. Available online: https://stat.bora.dopa.go.th/stat/statnew/statMONTH/statmonth/#/mainpage (accessed on 25 April 2022). (In Thai).
- World Health Organization Thailand. COVID-19 Situation, Thailand 25 May 2022. Available online: https://cdn.who.int/media/docs/default-source/searo/thailand/2022_05_25_tha-sitrep-237-covid-19.pdf?sfvrsn=42e15724_1 (accessed on 25 May 2022). (In Thai).
- Ministry of Public Health of Thailand. Report about COVID-19 in Thailand, 30 May 2022. Available online: https://media.thaigov.go.th/uploads/public_img/source/300565.pdf (accessed on 30 May 2022).
- Li, C.; He, Q.; Qian, H.; Liu, J. Overview of the pathogenesis of COVID-19 (Review). Exp. Ther. Med. 2021, 22, 1011. [Google Scholar] [CrossRef]
- Lotfi, M.; Hamblin, M.R.; Rezaei, N. COVID-19: Transmission, prevention, and potential therapeutic opportunities. Clin. Chim. Acta 2020, 508, 254–266. [Google Scholar] [CrossRef]
- Talukder, A.; Razu, S.R.; Alif, S.M.; Rahman, M.A.; Islam, S.M.S. Association Between Symptoms and Severity of Disease in Hospitalised Novel Coronavirus (COVID-19) Patients: A Systematic Review and Meta-Analysis. J. Multidiscip. Health 2022, 15, 1101–1110. [Google Scholar] [CrossRef]
- Amin, T.; Hasan, M.; Alam Bhuiya, N.M.M. Prevalence of COVID-19 Associated Symptoms, Their Onset and Duration, and Variations Among Different Groups of Patients in Bangladesh. Front. Public Health 2021, 9, 738352. [Google Scholar] [CrossRef]
- Rahman, M.A.; Islam, S.M.S.; Tungpunkom, P.; Sultana, F.; Alif, S.M.; Banik, B.; Salehin, M.; Joseph, B.; Lam, L.; Watts, M.C.; et al. COVID-19: Factors associated with psychological distress, fear, and coping strategies among community members across 17 countries. Glob. Health 2021, 17, 117. [Google Scholar] [CrossRef]
- Ruksakulpiwat, S.; Zhou, W.; Chiaranai, C.; Saengchut, P.; Vonck, J.E. Age, Sex, Population Density and COVID-19 Pandemic in Thailand: A Nationwide Descriptive Correlational Study. J. Health Sci. Med. Res. 2021, 40, 281–291. [Google Scholar] [CrossRef]
- Li, J.; Wang, A.; Liu, L.; Chen, X.; Bai, X. Caring for Psychological Distress of Patients With COVID-19: A Mixed-Method Cross-Sectional Study. Front. Psychol. 2022, 13, 766036. [Google Scholar] [CrossRef]
- Nochaiwong, S.; Ruengorn, C.; Thavorn, K.; Hutton, B.; Awiphan, R.; Phosuya, C.; Ruanta, Y.; Wongpakaran, N.; Wongpakaran, T. Global prevalence of mental health issues among the general population during the coronavirus disease-2019 pandemic: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 10173. [Google Scholar] [CrossRef]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef]
- Wipatayotin, A. Bed Shortage Prompts New Treatment Strategy. 2021. Available online: https://www.bangkokpost.com/thailand/general/2138707/ (accessed on 20 July 2022).
- Hernández-Díaz, Y.; Genis-Mendoza, A.D.; Ramos-Méndez, M.; Juárez-Rojop, I.E.; Tovilla-Zárate, C.A.; González-Castro, T.B.; López-Narváez, M.L.; Nicolini, H. Mental Health Impact of the COVID-19 Pandemic on Mexican Population: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 6953. [Google Scholar] [CrossRef]
- World Bank. Monitoring the Impact of COVID-19 in Thailand. 2021. Available online: https://www.worldbank.org/en/country/thailand/publication/monitoring-the-impact-of-covid-19-in-thailand (accessed on 20 October 2022).
- Gaesawahong, R.; Peasui, N.; Warapapong, O.; Yongprawat, T.; Dawudom, N. A Survey of Stress and Impacts in Registered Nurses During the COVID-19 Pandemic. Bangk. Med. J. 2022, 18, 106–112. [Google Scholar] [CrossRef]
- Creswell, J.W. Research Design: Quantitative, Qualitative, and Mixed Method Approaches, 3rd ed.; Sage: Los Angeles, CA, USA, 2009. [Google Scholar]
- Harley, A.E.; Buckworth, J.; Katz, M.L.; Willis, S.K.; Odoms-Young, A.; Heaney, C.A. Developing long-term physical activity participation: A grounded theory study with african american women. In Qualitative Inquiry & Research Design: Choosing among Five Approaches; Creswell, J.W., Ed.; Sage: Los Angeles, CA, USA, 2013; pp. 347–367. [Google Scholar]
- Creswell, J.W.; Creswell, D.J. Research Design: Qualitative, Quantitative, and Mixed Methods Approaches, 5th ed.; Sage: Los Angeles, CA, USA, 2018. [Google Scholar]
- Department of Psychology. G*Power. 2020. Available online: https://www.psychologie.hhu.de/arbeitsgruppen/allgemeine-psychologie-und-arbeitspsychologie/gpower (accessed on 3 May 2022).
- Creswell, J.W. Qualitative Inquiry & Research Design: Choosing among Five Approaches; Sage: Los Angeles, CA, USA, 2013. [Google Scholar]
- Lincoln, Y.S.; Guba, E.G.; Pilotta, J.J. Naturalistic Inquiry; SAGE: Beverly Hills, CA, USA, 1985. [Google Scholar] [CrossRef]
- Jarou, Z.J.; Beiser, D.G.; Sharp, W.W.; Chacko, R.R.; Goode, D.; Rubin, D.S.; Kurian, D.; Dalton, A.; Estime, S.R.; O’Connor, M.; et al. Emergency Department-initiated High-flow Nasal Cannula for COVID-19 Respiratory Distress. West. J. Emerg. Med. 2021, 22, 979–987. [Google Scholar] [CrossRef] [PubMed]
- Goyal, P.; Choi, J.J.; Pinheiro, L.C.; Schenck, E.J.; Chen, R.; Jabri, A.; Satlin, M.J.; Campion, T.R., Jr.; Nahid, M.; Ringel, J.B.; et al. Clinical Characteristics of Covid-19 in New York City. N. Engl. J. Med. 2020, 382, 2372–2374. [Google Scholar] [CrossRef] [PubMed]
- Vegivinti, C.T.R.; Evanson, K.W.; Lyons, H.; Akosman, I.; Barrett, A.; Hardy, N.; Kane, B.; Keesari, P.R.; Pulakurthi, Y.S.; Sheffels, E.; et al. Efficacy of antiviral therapies for COVID-19: A systematic review of randomized controlled trials. BMC Infect Dis. 2022, 22, 107. [Google Scholar] [CrossRef] [PubMed]
- Firouzkouhi, M.; Abdollahimohammad, A.; Alimohammadi, N.; Naderifar, M.; Akbarizadeh, M. Lived Experiences of Critically Ill COVID-19 Patients About Death and Dying: A Descriptive Phenomenology. Omega J. Death Dying 2022, 1–14. [Google Scholar] [CrossRef]
- Özgüç, S.; Serin, E.K.; Tanriverdi, D. Death Anxiety Associated with Coronavirus (COVID-19) Disease: A Systematic Review and Meta-Analysis. Omega J. Death Dying 2021, 1–34. [Google Scholar] [CrossRef]
- Toulabi, T.; Pour, F.J.; Veiskramian, A.; Heydari, H. Exploring COVID-19 patients’ experiences of psychological distress during the disease course: A qualitative study. BMC Psychiatry 2021, 21, 625. [Google Scholar] [CrossRef]
- Galehdar, N.; Toulabi, T.; Kamran, A.; Heydari, H. Exploring nurses’ perception about the care needs of patients with COVID-19: A qualitative study. BMC Nurs. 2020, 19, 119. [Google Scholar] [CrossRef]
- Thomas, D.; Lawton, R.; Brown, T.; Kranton, R. Prevalence, severity and distribution of depression and anxiety symptoms using observational data collected before and nine months into the COVID-19 pandemic. Lancet Reg. Health Am. 2021, 1, 100009. [Google Scholar] [CrossRef]
- Tandoc, J.E.C.; Lee, J.C.B. When viruses and misinformation spread: How young Singaporeans navigated uncertainty in the early stages of the COVID-19 outbreak. New Media Soc. 2020, 24, 778–796. [Google Scholar] [CrossRef]
- Koffman, J.; Gross, J.; Etkind, S.N.; Selman, L. Uncertainty and COVID-19: How are we to respond? J. R. Soc. Med. 2020, 113, 211–216. [Google Scholar] [CrossRef] [PubMed]
- Sugg, H.V.R.; Russell, A.-M.; Morgan, L.M.; Iles-Smith, H.; Richards, D.A.; Morley, N.; Burnett, S.; Cockcroft, E.J.; Coon, J.T.; Cruickshank, S.; et al. Fundamental nursing care in patients with the SARS-CoV-2 virus: Results from the ‘COVID-NURSE’ mixed methods survey into nurses’ experiences of missed care and barriers to care. BMC Nurs. 2021, 20, 215. [Google Scholar] [CrossRef] [PubMed]
- Hu, K.; Lin, L.; Liang, Y.; Shao, X.; Hu, Z.; Luo, H.; Lei, M. COVID-19: Risk factors for severe cases of the Delta variant. Aging 2021, 13, 23459–23470. [Google Scholar] [CrossRef] [PubMed]
- Fisman, D.N.; Tuite, A.R. Evaluation of the relative virulence of novel SARS-CoV-2 variants: A retrospective cohort study in Ontario, Canada. Can. Med. Assoc. J. 2021, 193, E1619–E1625. [Google Scholar] [CrossRef]
- Ratcliffe, R.; Siradapuvadol, N. Thailand’s Hospitals under Pressure as COVID Crisis Deepen. Available online: https://www.theguardian.com/world/2021/jul/27/thailands-hospitals-under-pressure-as-covid-crisis-deepens (accessed on 25 April 2022).
- Kumprasit, U. Development of nursing model during the COVID-19 outbreaks: In-patient department, Nonthai hospital. RHPC.9 J. 2022, 16, 30–44. (In Thai) [Google Scholar]
- Sousa, S.S.; Ferreira, M.M.; Cruz, S.; Sampaio, A.; Silva-Fernandes, A. A Structural Equation Model of Self-Regulation and Healthy Habits as an Individual Protective Tool in the Context of Epidemics–Evidence From COVID-19. Front. Psychol. 2021, 12, 3819. [Google Scholar] [CrossRef]
- Schnell, T.; Krampe, H. Meaning in Life and Self-Control Buffer Stress in Times of COVID-19: Moderating and Mediating Effects with Regard to Mental Distress. Front. Psychiatry 2020, 11, 582352. [Google Scholar] [CrossRef]
- Liu, C.; Huang, N.; Fu, M.; Zhang, H.; Feng, X.L.; Guo, J. Relationship Between Risk Perception, Social Support, and Mental Health Among General Chinese Population During the COVID-19 Pandemic. Risk Manag. Health Policy 2021, 14, 1843–1853. [Google Scholar] [CrossRef]
- Ho, Y.-C.L.; Chew, M.S.-L.; Mahirah, D.; Thumboo, J. Family Resilience and Psychological Responses to COVID-19: A Study of Concordance and Dyadic Effects in Singapore Households. Front. Psychol. 2022, 13, 770927. [Google Scholar] [CrossRef]
- Ruiz-Frutos, C.; Arias-Ulloa, C.A.; Ortega-Moreno, M.; Romero-Martín, M.; Escobar-Segovia, K.F.; Adanaque-Bravo, I.; Gómez-Salgado, J. Factors Associated to Psychological Distress During the COVID-19 Pandemic Among Healthcare Workers in Ecuador. Int. J. Public Health 2022, 67, 36. [Google Scholar] [CrossRef]
- Li, F.; Luo, S.; Mu, W.; Li, Y.; Ye, L.; Zheng, X.; Xu, B.; Ding, Y.; Ling, P.; Zhou, M.; et al. Effects of sources of social support and resilience on the mental health of different age groups during the COVID-19 pandemic. BMC Psychiatry 2021, 21, 16. [Google Scholar] [CrossRef]
- Wu, L.; Wu, Y.; Xiong, H.; Mei, B.; You, T. Persistence of Symptoms After Discharge of Patients Hospitalized Due to COVID-19. Front. Med. 2021, 8, 2314. [Google Scholar] [CrossRef] [PubMed]
- Han, Q.; Zheng, B.; Daines, L.; Sheikh, A. Long-Term Sequelae of COVID-19: A Systematic Review and Meta-Analysis of One-Year Follow-Up Studies on Post-COVID Symptoms. Pathogens 2022, 11, 269. [Google Scholar] [CrossRef] [PubMed]
- Montenegro, P.; Moral, I.; Puy, A.; Cordero, E.; Chantada, N.; Cuixart, L.; Brotons, C. Prevalence of Post COVID-19 Condition in Primary Care: A Cross Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 1836. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Leon, S.; Wegman-Ostrosky, T.; Perelman, C.; Sepulveda, R.; Rebolledo, P.A.; Cuapio, A.; Villapol, S. More than 50 long-term effects of COVID-19: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 16144. [Google Scholar] [CrossRef] [PubMed]
- Esteves, C.S.; de Oliveira, C.R.; Argimon, I.I.D.L. Social Distancing: Prevalence of Depressive, Anxiety, and Stress Symptoms Among Brazilian Students During the COVID-19 Pandemic. Front. Public Health 2021, 8, 589966. [Google Scholar] [CrossRef]
- Fernández-De-Las-Peñas, C.; Martín-Guerrero, J.D.; Pellicer-Valero, J.; Navarro-Pardo, E.; Gómez-Mayordomo, V.; Cuadrado, M.L.; Arias-Navalón, J.A.; Cigarán-Méndez, M.; Hernández-Barrera, V.; Arendt-Nielsen, L. Female Sex Is a Risk Factor Associated with Long-Term Post-COVID Related-Symptoms but Not with COVID-19 Symptoms: The LONG-COVID-EXP-CM Multicenter Study. J. Clin. Med. 2022, 11, 413. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Participants Demographic Characteristics | Frequency | Percent |
|---|---|---|
| Non-aged (≤60 year) | 133 | 73.9 |
| Aging/older adult (≥61 year) | 47 | 26.1 |
| Severity | ||
| Severe | 45 | 25 |
| Non-severe | 135 | 75 |
| Gender | ||
| Male | 56 | 31.1 |
| Female | 124 | 68.9 |
| Educational | ||
| Elementary school | 89 | 49.4 |
| High school or vocational school | 30 | 16.7 |
| Bachelor degree, and higher degree | 61 | 33.9 |
| Employment Status | ||
| Retirement | 34 | 18.9 |
| Employed | 84 | 46.7 |
| Unemployed | 31 | 17.2 |
| Student | 20 | 11.1 |
| Housewife | 11 | 6.1 |
| Vulnerability/Comorbidity | ||
| No | 87 | 48.3 |
| Yes | 93 | 51.7 |
| Comorbidity | 87 | 63.5 |
| Pregnant | 3 | 2.2 |
| Older adult | 47 | 34.3 |
| Hospitalization | ||
| No | 95 | 69.3 |
| Yes | 75 | 54.7 |
| Vaccination | ||
| No | 32 | 18 |
| Yes | 148 | 82 |
| Variables | 1. Physical Distress | 2. Psychological Distress | 3. Coping |
|---|---|---|---|
| 1. Physical distress | 1 | 0.62 ** | 0.18 * |
| 2. Psychological distress | 0.62 ** | - | 0.33 ** |
| 3. Coping | 0.18 | 0.33 ** | 1 |
| Variables | Non-Severe Group n = 45 | Severe Group n = 45 | t-Test | p-Value | ||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||
| Physical distress | 48.06 | 13.98 | 71.02 | 7.16 | −14.66 | <0.001 |
| Psychological distress | 38.71 | 16.31 | 66.15 | 19.09 | −7.33 | <0.001 |
| Coping | 34.46 | 13.17 | 40.68 | 12.88 | −2.26 | <0.05 |
| Effect of COVID-19 | Frequency | Percent | 95% CI (Lower–Upper) |
|---|---|---|---|
| Non-effects | 54 | 30 | 23.6–36.7 |
| Effects | 126 | 70 | 63.3–76.4 |
| 1. Decreased activity tolerance | 72 | 40 | 32.8–47.2 |
| 2. Fatigue | 60 | 33.3 | 25.3–39.4 |
| 3. Anxiety/fear of abnormal lungs | 60 | 33.3 | 25.3–39.4 |
| 4. Dyspnea | 50 | 27.8 | 21.4–31.4 |
| 5. Allergy and asthma | 44 | 24.4 | 18.9–31.1 |
| 6. Lung impairment | 40 | 22.2 | 16.1–28.8 |
| 7. Cough/sore throat | 23 | 12.8 | 7.8–18.0 |
| 8. Muscle pain/back pain/and neck pain | 23 | 12.8 | 7.8–18.0 |
| 9. Drowsiness | 23 | 12.8 | 8.3–19.1 |
| 10. Sleep disturbance | 22 | 12.2 | 6.7–16.9 |
| 11. Loss of appetite | 22 | 12.2 | 7.5–17.5 |
| 12.Headache | 13 | 7.2 | 3.9–11.1 |
| 13.Hypertension (HT) | 12 | 6.7 | 3.6–11.1 |
| 14. High blood-sugar level | 12 | 6.7 | 3.3–10.3 |
| 15. Memory impairment | 10 | 5.6 | 2.5–9.4 |
| 16. Palpitation/chest pain | 8 | 4.4 | 1.7–7.5 |
| 17. Hair loss/fragile nail | 6 | 3.3 | 1.1–5.6 |
| 18. Hyper platelet and stroke | 3 | 1.7 | 0.0–3.3 |
| 19. Eyes impairment | 2 | 1.1 | 0.0–2.8 |
| 20. Effect more than 2 symptoms | 98 | 54 | 47.2–61.7 |
| 21.The others: liver, kidney impairment, gout, and neuritis | 12 | 6.7 | 3.3–10.6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hengyotmark, A.; Kusoom, W. Physical as Well as Psychological Distress and Coping with Situational Dilemmas Experienced by People Infected with COVID-19: A Mixed Method Study. Int. J. Environ. Res. Public Health 2022, 19, 14657. https://doi.org/10.3390/ijerph192214657
Hengyotmark A, Kusoom W. Physical as Well as Psychological Distress and Coping with Situational Dilemmas Experienced by People Infected with COVID-19: A Mixed Method Study. International Journal of Environmental Research and Public Health. 2022; 19(22):14657. https://doi.org/10.3390/ijerph192214657
Chicago/Turabian StyleHengyotmark, Arunee, and Wichitra Kusoom. 2022. "Physical as Well as Psychological Distress and Coping with Situational Dilemmas Experienced by People Infected with COVID-19: A Mixed Method Study" International Journal of Environmental Research and Public Health 19, no. 22: 14657. https://doi.org/10.3390/ijerph192214657
APA StyleHengyotmark, A., & Kusoom, W. (2022). Physical as Well as Psychological Distress and Coping with Situational Dilemmas Experienced by People Infected with COVID-19: A Mixed Method Study. International Journal of Environmental Research and Public Health, 19(22), 14657. https://doi.org/10.3390/ijerph192214657