
The Incidence of Acute Respiratory Infection Was Higher in the Older Adults with Lower Limb Fracture Who Receive Spinal Anesthesia Than Those Who Receive General Anesthesia

 ,
, 
 ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Donohoe, E.; Roberts, H.J.; Miclau, T.; Kreder, H. Management of Lower Extremity Fractures in the Elderly: A Focus on Post-Operative Rehabilitation. Injury 2020, 51 (Suppl. 2), S118–S122. [Google Scholar] [CrossRef] [PubMed]
- Bohl, D.D.; Idarraga, A.J.P.; Lee, S.; Hamid, K.S.; Lin, J.; Holmes, G.B. Timing of Early Complications Following Open Reduction and Internal Fixation of Closed Ankle Fractures. Foot Ankle Spec. 2021, 14, 140–147. [Google Scholar] [CrossRef] [PubMed]
- Gogna, S.; Latifi, R.; Samson, D.J.; Butler, J. Pelvic fractures in severely injured elderly: A double-adjustment propensity score matched analysis from a level I trauma center. Eur. J. Trauma Emerg. Surg. 2022, 48, 2219–2228. [Google Scholar] [CrossRef] [PubMed]
- Yeh, H.W.; Yeh, L.T.; Chou, Y.H.; Yang, S.F.; Ho, S.W.; Yeh, Y.T.; Yeh, Y.T.; Wang, Y.H.; Chan, C.H.; Yeh, C.B. Risk of Cardiovascular Disease Due to General Anesthesia and Neuraxial Anesthesia in Lower-Limb Fracture Patients: A Retrospective Population-Based Cohort Study. Int. J. Environ. Res. Public Health. 2019, 17, 33. [Google Scholar] [CrossRef] [PubMed]
- Neuman, M.D.; Feng, R.; Carson, J.L.; Gaskins, L.J.; Dillane, D.; Sessler, D.I.; Sieber, F.; Magaziner, J.; Marcantonio, E.R.; Mehta, S.; et al. Spinal Anesthesia or General Anesthesia for Hip Surgery in Older Adults. N. Engl. J. Med. 2021, 385, 2025–2035. [Google Scholar] [CrossRef] [PubMed]
- Smith, G.; D’Cruz, J.R.; Rondeau, B.; Goldman, J. General Anesthesia for Surgeons. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK493199/ (accessed on 7 June 2022).
- Chia, W.T.; Liu, Y.C.; Wong, T.W. Optimize General Anesthesia for a Dystrophic Epidermolysis Bullosa Patient That Cannot Be Intubated. Asian J. Anesthesiol. 2020, 58, 111–114. [Google Scholar]
- Chen, D.X.; Yang, L.; Ding, L.; Li, S.Y.; Qi, Y.N.; Li, Q. Perioperative outcomes in geriatric patients undergoing hip fracture surgery with different anesthesia techniques: A systematic review and meta-analysis. Medicine 2019, 98, e18220. [Google Scholar] [CrossRef] [PubMed]
- Estebsari, F.; Dastoorpoor, M.; Khalifehkandi, Z.R.; Nouri, A.; Mostafaei, D.; Hosseini, M.; Esmaeili, R.; Aghababaeian, H. The Concept of Successful Aging: A Review Article. Curr. Aging Sci. 2020, 13, 4–10. [Google Scholar] [CrossRef]
- Chen, T.; Yasen, Y.; Wu, J.; Cheng, H. Factors influencing lower respiratory tract infection in older patients after general anesthesia. J. Int. Med. Res. 2021, 49, 3000605211043245. [Google Scholar] [CrossRef]
- Guay, J.; Parker, M.J.; Gajendragadkar, P.R.; Kopp, S. Anaesthesia for hip fracture surgery in adults. Cochrane Database Syst. Rev. 2016, 2, CD000521. [Google Scholar] [CrossRef]
- Fukuda, T.; Imai, S.; Shimoda, S.; Maruo, K.; Nakadera, M.; Horiguchi, H. Aspiration pneumonia and anesthesia techniques in hip fracture surgery in elderly patients: A retrospective cohort study using administrative data. J. Orthop. Surg. Hong Kong 2022, 30, 10225536221078622. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, V.A.; Hilsenbeck, S.G.; Noveck, H.; Poses, R.M.; Carson, J.L. Medical complications and outcomes after hip fracture repair. Arch. Intern. Med. 2002, 162, 2053–2057. [Google Scholar] [CrossRef] [PubMed]
- Manku, K.; Bacchetti, P.; Leung, J.M. Prognostic significance of postoperative in-hospital complications in elderly patients. I. Long-term survival. Anesth. Analg. 2003, 96, 583–589. [Google Scholar] [CrossRef] [PubMed]
- Zdravkovic, M.; Podbregar, M.; Kamenik, M. Near-infrared spectroscopy for assessing microcirculation during laparoscopic gynaecological surgery under combined spinal-general anaesthesia or general anaesthesia alone: A randomised controlled trial. J. Clin. Monit. Comput. 2020, 34, 943–953. [Google Scholar] [CrossRef]
- Du, H.; Tong, X.; Sun, X.; Shi, Z.; Liu, B.; Gao, F.; Miao, Z.; Zhang, D. Effect of anesthesia strategy during endovascular therapy on 90-day outcomes in acute basilar artery occlusion: A retrospective observational study. BMC Neurol. 2020, 20, 398. [Google Scholar] [CrossRef]
- Taiping, C.; Jie, Z.; Lingjun, K. The etiological characteristics and risk factors of lower respiratory tract infections after general anesthesia and tracheal intubation in elderly patients. Chin. J. Nosocom. Infect. 2017, 27, 4908–4911. [Google Scholar]
- Urwin, S.C.; Parker, M.J.; Griffiths, R. General versus regional anaesthesia for hip fracture surgery: A meta-analysis of randomized trials. Br. J. Anaesth. 2000, 84, 450–455. [Google Scholar] [CrossRef]
- Tzimas, P.; Samara, E.; Petrou, A.; Korompilias, A.; Chalkias, A.; Papadopoulos, G. The influence of anesthetic techniques on postoperative cognitive function in elderly patients undergoing hip fracture surgery: General vs spinal anesthesia. Injury 2018, 49, 2221–2226. [Google Scholar] [CrossRef]
- Gayat, E.; Lecarpentier, E.; Retout, S.; Bedairia, E.; Batallan, A.; Bonay, M.; Mantz, J.; Montravers, P.; Desmonts, J.M.; Guglielminotti, J. Cough reflex sensitivity after elective Caesarean section under spinal anaesthesia and after vaginal delivery. Br. J. Anaesth. 2007, 99, 694–698. [Google Scholar] [CrossRef]
- Li, T.; Li, J.; Yuan, L.; Wu, J.; Jiang, C.; Daniels, J.; Mehta, R.L.; Wang, M.; Yeung, J.; Jackson, T.; et al. Effect of Regional vs General Anesthesia on Incidence of Postoperative Delirium in Older Patients Undergoing Hip Fracture Surgery: The RAGA Randomized Trial. JAMA 2022, 327, 50–58. [Google Scholar] [CrossRef]
- Ruscic, K.J.; Grabitz, S.D.; Rudolph, M.I.; Eikermann, M. Prevention of respiratory complications of the surgical patient: Actionable plan for continued process improvement. Curr. Opin Anaesthesiol. 2017, 30, 399–408. [Google Scholar] [CrossRef] [PubMed]
- Attaallah, A.F.; Vallejo, M.C.; Elzamzamy, O.M.; Mueller, M.G.; Eller, W.S. Perioperative risk factors for postoperative respiratory failure. J. Perioper. Pract. 2019, 29, 49–53. [Google Scholar] [CrossRef] [PubMed]
- Yoon, S.H.; Kim, B.R.; Lee, S.Y.; Beom, J.; Choi, J.H.; Lim, J.Y. Influence of comorbidities on functional outcomes in patients with surgically treated fragility hip fractures: A retrospective cohort study. BMC Geriatr. 2021, 21, 283. [Google Scholar] [CrossRef] [PubMed]
- Aveyard, P.; Gao, M.; Lindson, N.; Hartmann-Boyce, J.; Watkinson, P.; Young, D.; Coupland, C.A.C.; Tan, P.S.; Clift, A.K.; Harrison, D.; et al. Association between pre-existing respiratory disease and its treatment, and severe COVID-19: A population cohort study. Lancet Respir. Med. 2021, 9, 909–923. [Google Scholar] [CrossRef]


{kind=link}
| Demographics | GA | RA | Total | p Value | SMD |
|---|---|---|---|---|---|
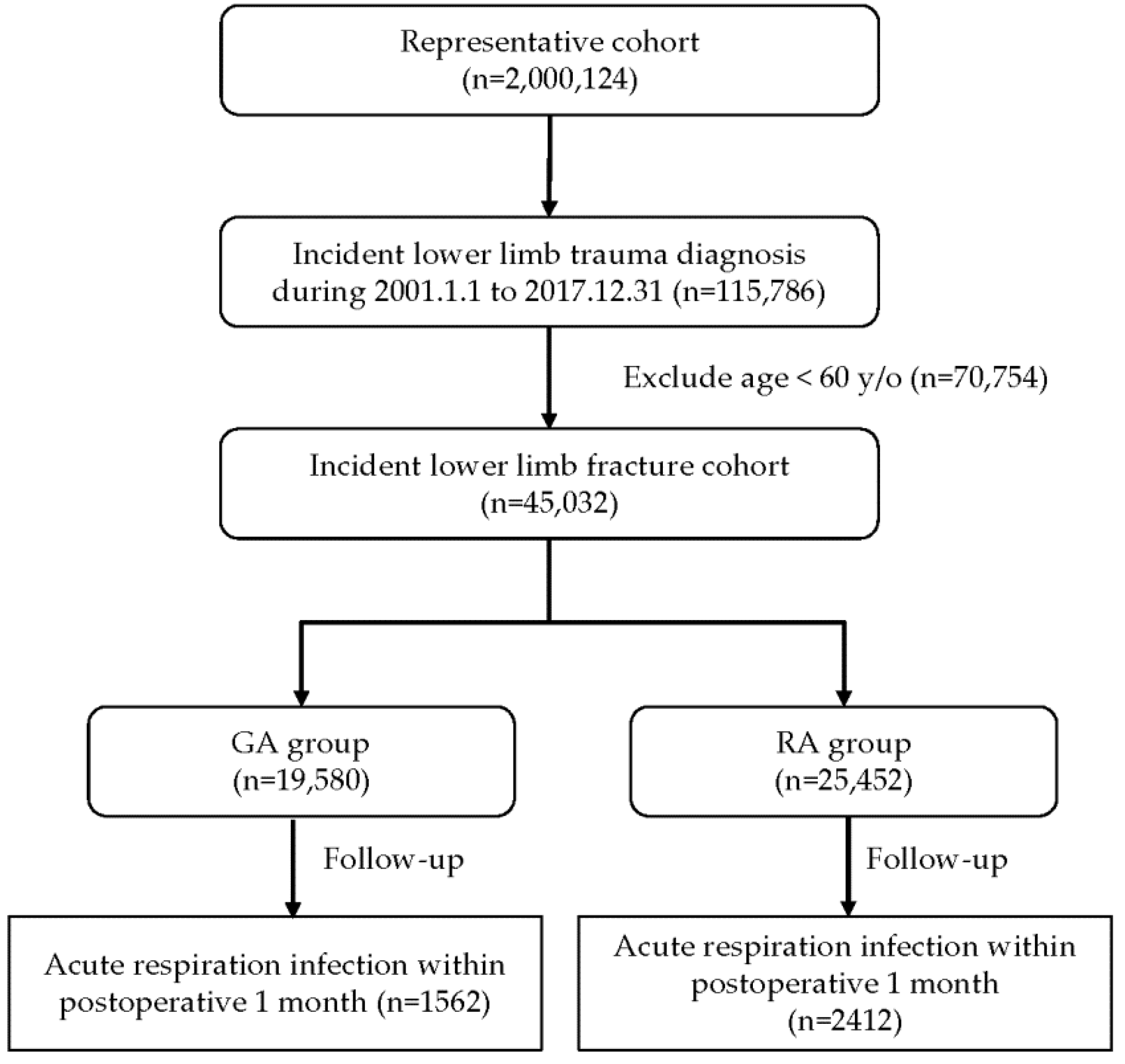
| N | 19,580 | 25,452 | 45,032 | ||
| Age | 73.8 ± 8.7 | 75.9 ± 8.9 | 75.0 ± 8.9 | <0.001 * | 0.24 |
| Age group | - | - | - | <0.001 * | 0.24 |
| 60–80 y/o | 14,101(72.0%) | 15,960(62.7%) | 30,061(66.8%) | ||
| ≥80 y/o | 5479(28.0%) | 9492(37.3%) | 14,971(33.2%) | ||
| Gender | - | - | - | <0.001 * | 0.08 |
| Male | 7845(40.1%) | 10,661(41.9%) | 18,506(41.1%) | ||
| Female | 11,735(59.9%) | 14,791(58.1%) | 26,526(58.9%) | ||
| Comorbidities | |||||
| Hypertension (%) | 9733(49.7%) | 13,245(52.0%) | 22,978(51.0%) | <0.001 * | 0.05 |
| Diabetes (%) | 5073(25.9%) | 6727(26.4%) | 11,800(26.2%) | 0.214 | 0.01 |
| Dyslipidemia (%) | 3616(18.5%) | 4219(16.6%) | 7835(17.4%) | <0.001 * | −0.05 |
| Liver disease (%) | 1287(6.6%) | 1436(5.6%) | 2723(6.1%) | <0.001 * | −0.04 |
| Chronic renal faliure (%) | 1102(5.6%) | 1355(5.3%) | 2457(5.5%) | 0.161 | −0.01 |
| Chronic obstructive pulmonary disease (%) | 1593(8.1%) | 2740(10.8%) | 4333(9.6%) | <0.001 * | 0.09 |
| Acute respiratory infection in postoperative 1 month (%) | 1562(8.0%) | 2412(9.5%) | 3974(8.8%) | <0.001 * | 0.05 |
| Risk Factors Associated with Acute Respiratory Infection | Crude | Adjusted | ||
|---|---|---|---|---|
| OR (95% CI) | p Value | OR (95% CI) | p Value | |
| Age group (≥80 y/o vs. 60–80 y/o) | 1.24(1.16, 1.33) | <0.001 * | 1.16(1.08, 1.24) | <0.001 * |
| Gender (Male vs. Female) | 1.04(0.97, 1.11) | 0.253 | 0.99(0.93, 1.06) | 0.848 |
| Anesthesia (RA vs. GA) | 1.21(1.13, 1.29) | <0.001 * | 1.17(1.09, 1.25) | <0.001 * |
| Hypertension vs. None | 1.18(1.11, 1.26) | <0.001 * | 1.16(1.08, 1.24) | <0.001 * |
| Diabetes vs. None | 0.97(0.90, 1.05) | 0.465 | 0.96(0.89, 1.05) | 0.380 |
| Dyslipidemia vs. None | 0.92(0.84, 1.01) | 0.052 | 0.92(0.84, 1.01) | 0.091 |
| Liver disease vs. None | 1.19(1.05, 1.36) | 0.007 * | 1.20(1.05, 1.36) | 0.006 * |
| Chronic renal failure vs. None | 0.98(0.85, 1.14) | 0.836 | 0.95(0.82, 1.10) | 0.472 |
| Chronic obstructive pulmonary disease vs. None | 1.82(1.66, 1.99) | <0.001 * | 1.73(1.57, 1.90) | <0.001 * |
| Subgroup Comparative Analysis | Crude OR (95% CI) (RA vs. GA) | p Value | Adjusted OR (95% CI) (RA vs. GA) | p Value | p for Interaction |
|---|---|---|---|---|---|
| Main Model | 1.21(1.13, 1.29) | <0.001 * | 1.17(1.09, 1.25) | <0.001 * | |
| Age group | 0.082 | ||||
| 60–80 y/o | 1.24(1.14, 1.34) | <0.001 * | 1.22(1.12, 1.32) | <0.001 * | |
| ≥80 y/o | 1.10(0.98, 1.23) | 0.102 | 1.08(0.96, 1.21) | 0.195 | |
| Gender | 0.020 * | ||||
| Male | 1.35(1.21, 1.50) | <0.001 * | 1.27(1.14, 1.41) | <0.001 * | |
| Female | 1.12(1.03, 1.22) | 0.012 * | 1.10(1.01, 1.20) | 0.036 * | |
| With any of comorbidity # | 0.767 | ||||
| No | 1.16(1.03, 1.32) | 0.015 * | 1.14(1.01, 1.29) | 0.037 * | |
| Yes | 1.22(1.12, 1.32) | <0.001 * | 1.18(1.08, 1.28) | <0.001 * | |
| Chronic obstructive pulmonary disease | 0.879 | ||||
| No | 1.19(1.10, 1.28) | <0.001 * | 1.17(1.09, 1.25) | <0.001 * | |
| Yes | 1.18(0.98, 1.41) | 0.076 | 1.17(0.97, 1.40) | 0.091 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yeh, K.-T.; Wu, W.-T.; Lee, R.-P.; Wang, J.-H.; Chen, T.-Y. The Incidence of Acute Respiratory Infection Was Higher in the Older Adults with Lower Limb Fracture Who Receive Spinal Anesthesia Than Those Who Receive General Anesthesia. Int. J. Environ. Res. Public Health 2022, 19, 14260. https://doi.org/10.3390/ijerph192114260
Yeh K-T, Wu W-T, Lee R-P, Wang J-H, Chen T-Y. The Incidence of Acute Respiratory Infection Was Higher in the Older Adults with Lower Limb Fracture Who Receive Spinal Anesthesia Than Those Who Receive General Anesthesia. International Journal of Environmental Research and Public Health. 2022; 19(21):14260. https://doi.org/10.3390/ijerph192114260
Chicago/Turabian StyleYeh, Kuang-Ting, Wen-Tien Wu, Ru-Ping Lee, Jen-Hung Wang, and Tsung-Ying Chen. 2022. "The Incidence of Acute Respiratory Infection Was Higher in the Older Adults with Lower Limb Fracture Who Receive Spinal Anesthesia Than Those Who Receive General Anesthesia" International Journal of Environmental Research and Public Health 19, no. 21: 14260. https://doi.org/10.3390/ijerph192114260
APA StyleYeh, K.-T., Wu, W.-T., Lee, R.-P., Wang, J.-H., & Chen, T.-Y. (2022). The Incidence of Acute Respiratory Infection Was Higher in the Older Adults with Lower Limb Fracture Who Receive Spinal Anesthesia Than Those Who Receive General Anesthesia. International Journal of Environmental Research and Public Health, 19(21), 14260. https://doi.org/10.3390/ijerph192114260