

Male Victims of Rape: An Observational Study over Four Years in Paris, France


Abstract
1. Introduction
2. Materials and Methods
2.1. Presentation of the Department of Forensic Medicine and of a Forensic Consultation
2.2. Study Methodology
2.3. Statistical Analyses
2.4. Ethical Standards
3. Results
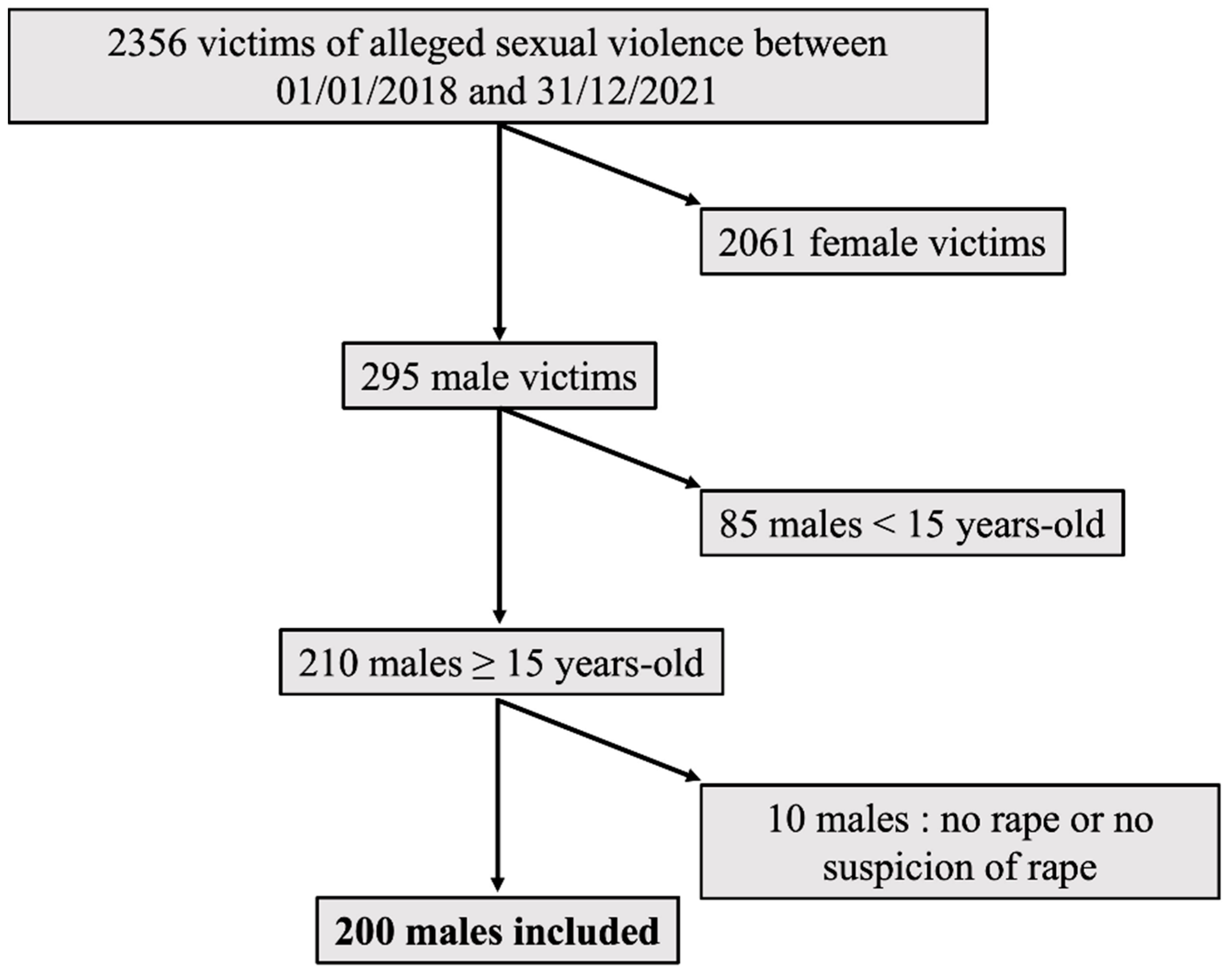
3.1. Study Population
3.2. Characteristics of the Victims
- Age at the time of the assault
- •
- Vulnerabilities
- -
- A social or economic vulnerability linked to the reported living condition for 18 victims (9.0%),
- -
- A psychological vulnerability for 17 victims (8.5%): three victims were hospitalized in a psychiatric department at the time of the assault, four were living in a specialized center due to a mental pathology, and the files of 10 victims mentioned a psychological vulnerability (Down’s syndrome, Alzheimer’s, etc.).
- •
- Usual treatments
- -
- Psychiatric medications were reported by 43 patients (21.5%). Psychiatric medication intake was not associated with a suspected DFSA (p = 0.1568) or with alcohol or illicit substance consumption before the assault (p = 0.1193 and p = 0.2217, respectively).
- -
- Endocrine medications linked to sexual reassignment were reported by 8 patients (4.0%).
- -
- Anti-retroviral treatment not related to the assault was reported by 29 patients (14.5%), 15 in connection with positive HIV status (7.5%) and 14 with HIV pre-exposure prophylaxis (PREP, 7.0%).
- •
- Opportunistic DFSA
- -
- Alcohol use was reported by 107 patients (53.5%). The quantity was specified in 89 files. The average reported consumption was 61.8 g of pure alcohol (median 60 g [40–80]).
- -
- Illicit substance use was reported by 49 patients (24.5%). These patients reported a median of one illicit substance (excluding alcohol) [1;1]. These were mainly cannabis (16.5%), cocaine (3.0%), 3-methylmethcathinone (3MMC) (2.5%), gamma-hydroxybutyric acid (GHB) or gamma-butyrolactone (GBL) (1.5%), 3,4-methylenedioxymethamphetamine (MDMA) (1.5%), poppers (1.0%), and diverted psychoactive drugs (pregabalin 1.0%, clonazepam 0.5%). One patient reported taking methamphetamines (0.5%) and another reported alpha-pyrrolidinopentiophenone (alpha-PVP, known as “flakka”, 0.5%). Illicit substances other than cannabis were reported to have been voluntarily consumed in the context of chem-sex or slam-sex by 14 patients (7.0%).
3.3. Characteristics of the Assault
- Location
- Type
- -
- Of the 126 patients who reported a rape, 73 (57.9%) reported a single act and 53 (42.1%) reported several acts. The acts reported were most often anal penetrations committed on the victim (108/126; 85.7%). They were most frequently penile (77/126; 65.9%) or digital (25/126; 19.8%). Six victims reported a rape with objects (6/126; 4.7%). Penile oral penetration of the victim was reported in more than one-third of cases (46/126; 36.5%). Victims less frequently reported being forced to perform penile penetration on the assailant (oral 10/126—7.9% or anal 3/126—2.4%).
- -
- For the 74 patients suspecting a rape, amnesia was mostly related to a proactive or opportunistic DFSA (62/74; 83%). Rape was suspected upon awakening, with several interrelated elements of concern: report of theft of valuables (29/74; 39%), physical injuries (24/74; 32%), patient awakening in an unusual place (22/74; 30%), or patient awakening naked in the company of another person (30/74; 41%). In ten cases, a possible assault could not be specified because of a state of psychological vulnerability of the patient (10/74; 14%; autism, psychiatric pathologies, mental retardation, etc.). For these cases, the circumstances were reported by the family or care takers. Finally, in two cases, the circumstances could not be specified because of a head injury resulting in loss of consciousness (2/74; 3%).
- Associated theft
- Associated physical violence
- Threat or use of a weapon
- Suspicion of proactive DFSA
3.4. Characteristics of the Assailant
3.5. Characteristics of the Forensic Examination
- Time between the assault and the forensic examination
- Extragenital findings
- Anogenital findings
- Samples for judicial purposes
- Management of the infectious risk
3.6. Aggravating Circumstances
3.7. Characteristics of the Victims and the Assaults According to the Victim’s Vulnerability
3.8. Characteristics of the Victims and the Assaults According to the Victim’s Memory of the Assault
3.9. Characteristics of the Victims and the Assaults According to the Assailant’s Status
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Krug, E.G.; Dahlberg, L.L.; Mercy, J.A.; Zwi, A.B.; Lozano, R.; World Health Organization. World Report on Violence and Health. Rapp Mond Sur Violence Santé. 2002. Available online: https://apps.who.int/iris/handle/10665/42495 (accessed on 4 February 2022).
- Bajos, N.; Bozon, M. Enquête sur la Sexualité en France. Pratiques, Genre et Santé; La Découverte: Paris, France, 2008; 612p, (Hors Collection Social); Available online: https://www.cairn.info/enquete-sur-la-sexualite-en-france--9782707154293.htm (accessed on 6 February 2022).
- Bajos, N.; Rahib, D.; Lydié, N. Baromètre Santé 2016. In Genre et Sexualité; Santé Publique France: Saint Maurice, France, 2018. [Google Scholar]
- Institut National de la Statistique et des Etudes Economiques (Insee). Observatoire National de la Délinquance et de la Réponse Pénale (ONDRP). Rapport D’enquête « Cadre de vie et Sécurité » 2019. Service Statistique Ministériel de la Sécurité Intérieure (SSMSI). 2019. Available online: https://www.interieur.gouv.fr/Interstats/Actualites/Rapport-d-enquete-Cadre-de-vie-et-securite-2019 (accessed on 9 February 2022).
- Murdoch, M.; Polusny, M.A.; Street, A.; Noorbaloochi, S.; Simon, A.B.; Bangerter, A.; Grill, J.; Voller, E. Sexual Assault During the Time of Gulf War I: A Cross-Sectional Survey of U.S. Service Men Who Later Applied for Department of Veterans Affairs PTSD Disability Benefits. Mil. Med. Mars 2014, 179, 285–293. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Oosterhoff, P.; Zwanikken, P.; Ketting, E. Sexual Torture of Men in Croatia and Other Conflict Situations: An Open Secret. Reprod. Health Matters 2004, 12, 68–77. [Google Scholar] [CrossRef]
- Anderson, L.J.; Flynn, A.; Pilgrim, J.L. A global epidemiological perspective on the toxicology of drug-facilitated sexual assault: A systematic review. J. Forensic Leg Med. Avr. 2017, 47, 46–54. [Google Scholar] [CrossRef] [PubMed]
- Finnerty, F.; Fitzpatrick, C.; Stockwell, S.; Richardson, D. The changing face of male sexual assault: Recreational drug use and multiple assailants. Sex Transm. Infect. 2019, 95, 550. [Google Scholar] [CrossRef] [PubMed]
- Expert Opinion on the Evolution of Public Discourse on Alcohol Consumption in France Organized by Public Health France and the National Cancer Institute. Santé Publique France, 2017. Available online: https://www.santepubliquefrance.fr/les-actualites/2017/avis-d-experts-relatif-a-l-evolution-du-discours-public-en-matiere-de-consommation-d-alcool-en-france-organise-par-sante-publique-france-et-l-insti (accessed on 9 February 2022).
- Article 222-23 du Code Pénal, Modifié par LOI n°2021-478 du 21 Avril 2021—Art. 9. Available online: https://www.legifrance.gouv.fr/jorf/id/JORFTEXT000043403203#:~:text=%2DHors%20le%20cas%20pr%C3%A9vu%20%C3%A0,majeur%20et%20le%20mineur%20est (accessed on 6 August 2022).
- Article 222-22 du Code Pénal, Modifié par LOI n°2021-478 du 21 Avril 2021—Art. 1. Available online: https://www.legifrance.gouv.fr/jorf/id/JORFTEXT000043403203#:~:text=euros%20d’amende.-,%C2%AB%20Les%20peines%20sont%20port%C3%A9es%20%C3%A0%20dix%20ans%20d’emprisonnement%20et,%C3%A9t%C3%A9%20commis%20en%20bande%20organis%C3%A9e.%20%C2%BB (accessed on 6 August 2022).
- Article 222-24 du Code Pénal, Modifié par LOI n°2021-478 du 21 Avril 2021—Art. 8. Available online: https://www.legifrance.gouv.fr/jorf/id/JORFTEXT000043403203 (accessed on 6 August 2022).
- Prise en Charge du VIH—Recommandations du Groupe D’experts. 2017. Available online: https://cns.sante.fr/actualites/prise-en-charge-du-vih-recommandations-du-groupe-dexperts/ (accessed on 8 August 2022).
- Bullock, C.M.; Beckson, M. Male victims of sexual assault: Phenomenology, psychology, physiology. J. Am. Acad. Psychiatry Law. 2011, 39, 197–205. [Google Scholar]
- Duchesne, S.; Seyller, M.; Chariot, P. Male sexual assaults in the Paris, France area: An observational study over 8 years. Forensic. Sci. Int. 2018, 290, 16–28. [Google Scholar] [CrossRef] [PubMed]
- Hiquet, J.; Groleron Gros, N.; Gromb, S. L’homme face aux violences sexuelles. Onze ans d’expérience au centre d’accueil en urgence des victimes d’agression (CAUVA) du CHU de Bordeaux. Rev. Méd. Légale 2012, 3, 64–71. [Google Scholar] [CrossRef]
- Loi n° 2018-703 du 3 Août 2018 Renforçant la Lutte Contre les Violences Sexuelles et Sexistes. Available online: https://www.legifrance.gouv.fr/jorf/id/JORFTEXT000037284450#:~:text=%2DLe%20fait%20d’administrer%20%C3%A0,75%20000%20%E2%82%AC%20d’amende. (accessed on 8 August 2022).
- McCann, J.; Voris, J. Perianal injuries resulting from sexual abuse: A longitudinal study. Pediatrics. Pediatrics 1993, 91, 390–397. [Google Scholar] [CrossRef] [PubMed]
- Casali, M.B.; Palazzo, E.; Blandino, A.; Battistini, A.; Motta, F.; Kustermann, A.; Cattaneo, C. The Adult Male Rape Victim: Forensic Description of a Series of 57 Cases. Am. J. Forensic Med. Pathol. 2017, 38, 175–179. [Google Scholar] [CrossRef] [PubMed]
- Jewkes, R.; Christofides, N.; Vetten, L.; Jina, R.; Sigsworth, R.; Loots, L. Medico-Legal Findings, Legal Case Progression, and Outcomes in South African Rape Cases: Retrospective Review. Beyrer C, éditeur. PLoS Med. 2009, 6, e1000164. [Google Scholar] [CrossRef] [PubMed]
- Muccigrosso, L. Sexual Abuse Prevention Strategies and Programs for persons with Developmental Disabilities. Sex Disabil. 1991, 9, 261–271. [Google Scholar] [CrossRef]
- Rajan, G.; Ljunggren, G.; Wändell, P.; Wahlström, L.; Svedin, C.G.; Carlsson, A.C. Diagnoses of sexual abuse and their common registered comorbidities in the total population of Stockholm. J. Epidemiol. Community Health. 2017, 71, 592–598. [Google Scholar] [CrossRef] [PubMed]
- État des Lieux de la Consommation des Benzodiazépines en France; Agence Nationale de Sécurité du Médicament et des Produits de Santé: Saint-Denis, France, 2017.
- Usage des Médicaments de Ville en France Durant L’Epidémie de la COVID-19; Agence Nationale de Sécurité du Médicament et des Produits de Santé: Saint-Denis, France, 2021.
- Fisher, B.; Hovell, M.; Hofstetter, C.R.; Hough, R. Risks Associated with Long-Term Homelessness among Women: Battery, Rape, and HIV Infection. Int. J. Health Serv. 1995, 25, 351–369. [Google Scholar] [CrossRef] [PubMed]
- Wenzel, S.L.; Koegel, P.; Gelberg, L. Antecedents of Physical and Sexual Victimization Among Homeless Women: A Comparison to Homeless Men. Am. J. Community Psychol. 2000, 28, 367–390. [Google Scholar] [CrossRef] [PubMed]
- Girard, V.; Bonin, J.P.; Tinland, A.; Farnarier, C.; Pelletier, J.F.; Delphin, M.; Rowe, M.; Simeoni, M.C. Mental health outreach and street policing in the downtown of a large French city. Int. J. Law Psychiatry 2014, 37, 376–382. [Google Scholar] [CrossRef] [PubMed]
- Addictovigilance Française, CEIP-A, Soumission et Vulnérabilité Chimique. Available online: https://addictovigilance.fr/projets-scientifiques/soumission-chimique/ (accessed on 8 August 2022).
- Du Mont, J.; Macdonald, S.; Rotbard, N.; Bainbridge, D.; Asllani, E.; Smith, N.; Cohen, M.M. Drug-facilitated sexual assault in Ontario, Canada: Toxicological and DNA findings. J. Forensic Leg. Med. 2010, 17, 333–338. [Google Scholar] [CrossRef] [PubMed]
- Hurley, M.; Parker, H.; Wells, D.L. The epidemiology of drug facilitated sexual assault. J. Clin. Forensic. Med. 2006, 13, 181–185. [Google Scholar] [CrossRef]
- Caballero, C.G.; Jorge, Ó.Q.; Landeira, A.C. Alleged drug-facilitated sexual assault in a Spanish population sample. Forensic Chem. 2017, 4, 61–66. [Google Scholar] [CrossRef]
- Hagemann, C.T.; Helland, A.; Spigset, O.; Espnes, K.A.; Ormstad, K.; Schei, B. Ethanol and drug findings in women consulting a Sexual Assault Center—Associations with clinical characteristics and suspicions of drug-facilitated sexual assault. J. Forensic Leg. Med. 2013, 20, 777–784. [Google Scholar] [CrossRef]
- Tiemensma, M.; Davies, B. Investigating drug-facilitated sexual assault at a dedicated forensic centre in Cape Town, South Africa. Forensic Sci. Int. 2018, 288, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Dos Massaro, L.T.S.; Adesse, L.; Laranjeira, R.; Caetano, R.; Madruga, C.S. Estupros no Brasil e relações com o consumo de álcool: Estimativas baseadas em autorrelato sigiloso. Cad Saúde Pública 2019, 35, e00022118. [Google Scholar] [CrossRef] [PubMed]
- Rapport Européen sur les Drogues: Tendances et Evolutions. 100. Available online: https://www.emcdda.europa.eu/system/files/publications/13838/2021.2256_FR_02_.pdf (accessed on 10 September 2022).
- Baud, F.; Garnier, R. Toxicologie Clinique, 6th ed; Lavoisier: Paris, France, 2017. [Google Scholar]
- Sida Info Services, Tout Savoir sur le Chem-Sex. Available online: https://www.sida-info-service.org/questions-chemsex/#:~:text=Le%20chemsex%20c’est%20quoi,bien%20ins%C3%A9r%C3%A9s%20dans%20l’anus (accessed on 10 September 2022).
- Jänisch, S.; Meyer, H.; Germerott, T.; Albrecht, U.V.; Schulz, Y.; Debertin, A.S. Analysis of clinical forensic examination reports on sexual assault. Int. J. Legal Med. 2010, 124, 227–235. [Google Scholar] [CrossRef] [PubMed]
- Saint-Martin, P.; Bouyssy, M.; O’Byrne, P. Analysis of 756 cases of sexual assault in Tours (France): Medico-legal findings and judicial outcomes. Med. Sci. Law 2007, 47, 315–324. [Google Scholar] [CrossRef]
- Sugar, N.F.; Fine, D.N.; Eckert, L.O. Physical injury after sexual assault: Findings of a large case series. Am. J. Obstet. Gynecol. 2004, 190, 71–76. [Google Scholar] [CrossRef]
- Vanier, C.; Langlade, A. Comprendre le dépôt de plainte des victimes de viol: Facteurs individuels et circonstanciels. Déviance Soc. 2018, 42, 501–533. [Google Scholar] [CrossRef]
- Loi n° 2016-444 du 13 Avril 2016. Available online: https://juridique.defenseurdesdroits.fr/index.php?lvl=notice_display&id=18317&opac_view=-1#:~:text=R%C3%A9sum%C3%A9%20%3A,non%20plus%20comme%20des%20d%C3%A9linquantes. (accessed on 10 September 2022).


{kind=link}
| Aggravating Circumstance | Number of Victims (%) |
|---|---|
| Act resulting in permanent mutilation or disability | 2 (1.0) |
| Act committed on a minor of 15 years old | not included in the study |
| Physical/psychological vulnerability of the victim | 17 (8.5) |
| Economic/social vulnerability of the victim | 18 (9.0) |
| Act committed by an ascendant/person in authority | 1 (0.5) |
| Act committed by a person who abuses authority * | 6 (3.0) |
| Act committed by several persons | 28 (14.0) |
| Act committed with the use or threat of a weapon | 4 (2.0) |
| Contact with the perpetrator through (…) an electronic communication network | not included in the study |
| Act committed in conjunction with one or more other rapes committed on other victims | 0 (0.0) |
| Act committed by a spouse | 4 (2.0) |
| Act committed by a person acting in a state of obvious intoxication or under the influence of drugs | not included in the study |
| Act committed on a person engaged in prostitution | 14 (7.0) |
| Minor present at time of offence | 0 (0.0) |
| Proactive DFSA | Suspicion: 82 (41.0) ** |
| Vulnerable n = 32 Number (%) | Non Vulnerable n = 168 Number (%) | p | |
|---|---|---|---|
| Victim | |||
| Median age (years) | 25.93 | 26.98 | 0.5280 |
| Psychiatric medication | 17 (55) | 35 (20.8) | 0.0001 |
| Alcohol use before the assault | 9 (29) | 70 (41.7) | 0.1509 |
| Psychoactive substance use before the assault | 12 (38) | 37 (22.0) | 0.0621 |
| Initial medical examination | 13 (41) | 65 (38.7) | 0.9371 |
| Median delay between the assault and the forensic examination (days) | 1 day | 1 day | 0.9110 |
| Extragenital lesions | 9 (28) | 71 (42.3) | 0.1346 |
| Anogenital lesions | 3 (9) | 41 (24.4) | 0.0381 |
| Assault | |||
| Number of assailants (mean) | 1 (3) | 1 (0.6) | 0.3199 |
| Previously known assailant | 13 (41) | 18 (10.7) | 0.0001 |
| Place of assault | |||
| Assailant’s home | 3 (9) | 28 (16.7) | 0.3242 |
| Victim’s home/place of living | 15 (47) | 30 (17.9) | 0.0002 |
| Public place | 4 (13) | 38 (22.6) | 0.2232 |
| Type of assault | |||
| Cannot recall any assault | 13 (41) | 61 (36.3) | 0.6431 |
| Anal penetration of the victim | 16 (50) | 82 (48.8) | 0.9017 |
| Oral penetration of the victim | 8 (25) | 39 (23.2) | 0.8272 |
| Penetration of the assailant | 22 (69) | 11 (6.5) | 0.9501 |
| Physical violence | 6 (19) | 58 (34.5) | 0.0796 |
| Theft | 1 (3) | 35 (20.8) | 0.0169 |
| Suspicion of proactive DFSA | 5 (16) | 77 (45.8) | 0.0015 |
| Patient Reporting a Rape n = 126 Number (%) | Total Amnesia n = 74 Number (%) | p | ||
|---|---|---|---|---|
| Victim | ||||
| Median age (years) | 24.67 | 28.52 | 0.0045 | |
| Psychiatric medication | 33 (26.2) | 19 (26) | 0.9361 | |
| Vulnerability | 19 (15.1) | 13 (18) | 0.6431 | |
| Alcohol use before the assault | 49 (38.9) | 58 (78) | <0.0001 | |
| Psychoactive substance use before the assault | 17 (13.5) | 32 (43) | <0.0001 | |
| Initial medical examination | 50 (39.7) | 28 (38) | 0.7962 | |
| Median delay between the assault and the forensic examination (days) | 1 day | 1 day | 0.8205 | |
| Extragenital lesions | 54 (42.9) | 26 (35) | 0.2818 | |
| Anogenital lesions | 34 (27.0) | 6 (8) | 0.0001 | |
| Chem-sex | 6 (4.8) | 8 (11) | 0.1055 | |
| Assault | ||||
| Number of assailants (mean) | 1.25 | 1.8 | 0.0049 | |
| Previously known assailant | 23 (18.3) | 8 (11) | 0.1602 | |
| Place of the assault | ||||
| Assailant’s home | 22 (17.5) | 9 (12) | 0.3175 | |
| Victim’s home/place of living | 31 (24.6) | 14 (19) | 0.3527 | |
| Public place | 36 (28.6) | 6 (8) | 0.0006 | |
| Unknown place | 0 (0.0) | 35 (47) | <0.0001 | |
| Physical violence | 64 (50.8) | 0 (0) | <0.0001 | |
| Theft | 7 (5.6) | 29 (39) | <0.0001 | |
| Suspicion of proactive DFSA | 20 (15.9) | 62 (84) | <0.0001 | |
| Known Assailant n = 31 Number (%) | Previously Unknown Assailant n = 96 Number (%) | p | ||
|---|---|---|---|---|
| Victim | ||||
| Median age (years) | 26.7 | 25.5 | 0.8699 | |
| Psychiatric medication | 21 (68) | 12 (13) | <0.0001 | |
| Vulnerability | 13 (42) | 11 (11) | 0.0002 | |
| Alcohol use before the assault | 12 (39) | 45 (47) | 0.4268 | |
| Psychoactive substance use before the assault | 11 (35) | 21 (22) | 0.1292 | |
| Initial medical examination | 9 (29) | 43 (45) | 0.0411 | |
| Median delay between the assault and the forensic examination (days) | 1 day | 1 day | 0.2945 | |
| Extragenital lesions | 7 (23) | 42 (44) | 0.0055 | |
| Anogenital lesions | 1 (3) | 35 (36) | 0.0004 | |
| Chem-sex | 0 (0) | 9 (9) | 0.0770 | |
| Assault | ||||
| Number of assailants (mean) | 1.2 | 1.4 | 0.7958 | |
| Place of the assault | ||||
| Assailant’s home | 5 (16) | 24 (25) | 0.3063 | |
| Victim’s home/place of living | 20 (65) | 17 (18) | <0.0001 | |
| Public place | 1 (3) | 30 (31) | 0.0016 | |
| Physical violence | 7 (23) | 47 (49) | 0.0098 | |
| Theft | 0 (0) | 13 (14) | 0.0306 | |
| Suspicion of proactive DFSA | 6 (19) | 32 (33) | 0.1395 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liautard, M.; Deguette, C.; Alcaraz, E.; Diot, H.; Vasseur, P.; Gorgiard, C.; Dufayet, L. Male Victims of Rape: An Observational Study over Four Years in Paris, France. Int. J. Environ. Res. Public Health 2022, 19, 13909. https://doi.org/10.3390/ijerph192113909
Liautard M, Deguette C, Alcaraz E, Diot H, Vasseur P, Gorgiard C, Dufayet L. Male Victims of Rape: An Observational Study over Four Years in Paris, France. International Journal of Environmental Research and Public Health. 2022; 19(21):13909. https://doi.org/10.3390/ijerph192113909
Chicago/Turabian StyleLiautard, Marc, Céline Deguette, Elizabeth Alcaraz, Hélène Diot, Patricia Vasseur, Charlotte Gorgiard, and Laurène Dufayet. 2022. "Male Victims of Rape: An Observational Study over Four Years in Paris, France" International Journal of Environmental Research and Public Health 19, no. 21: 13909. https://doi.org/10.3390/ijerph192113909
APA StyleLiautard, M., Deguette, C., Alcaraz, E., Diot, H., Vasseur, P., Gorgiard, C., & Dufayet, L. (2022). Male Victims of Rape: An Observational Study over Four Years in Paris, France. International Journal of Environmental Research and Public Health, 19(21), 13909. https://doi.org/10.3390/ijerph192113909