
The Health Effects of Real-World Dual Use of Electronic and Conventional Cigarettes versus the Health Effects of Exclusive Smoking of Conventional Cigarettes: A Systematic Review

Abstract
1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Exclusion Criteria
2.3. Information Sources
2.4. Search Strategy
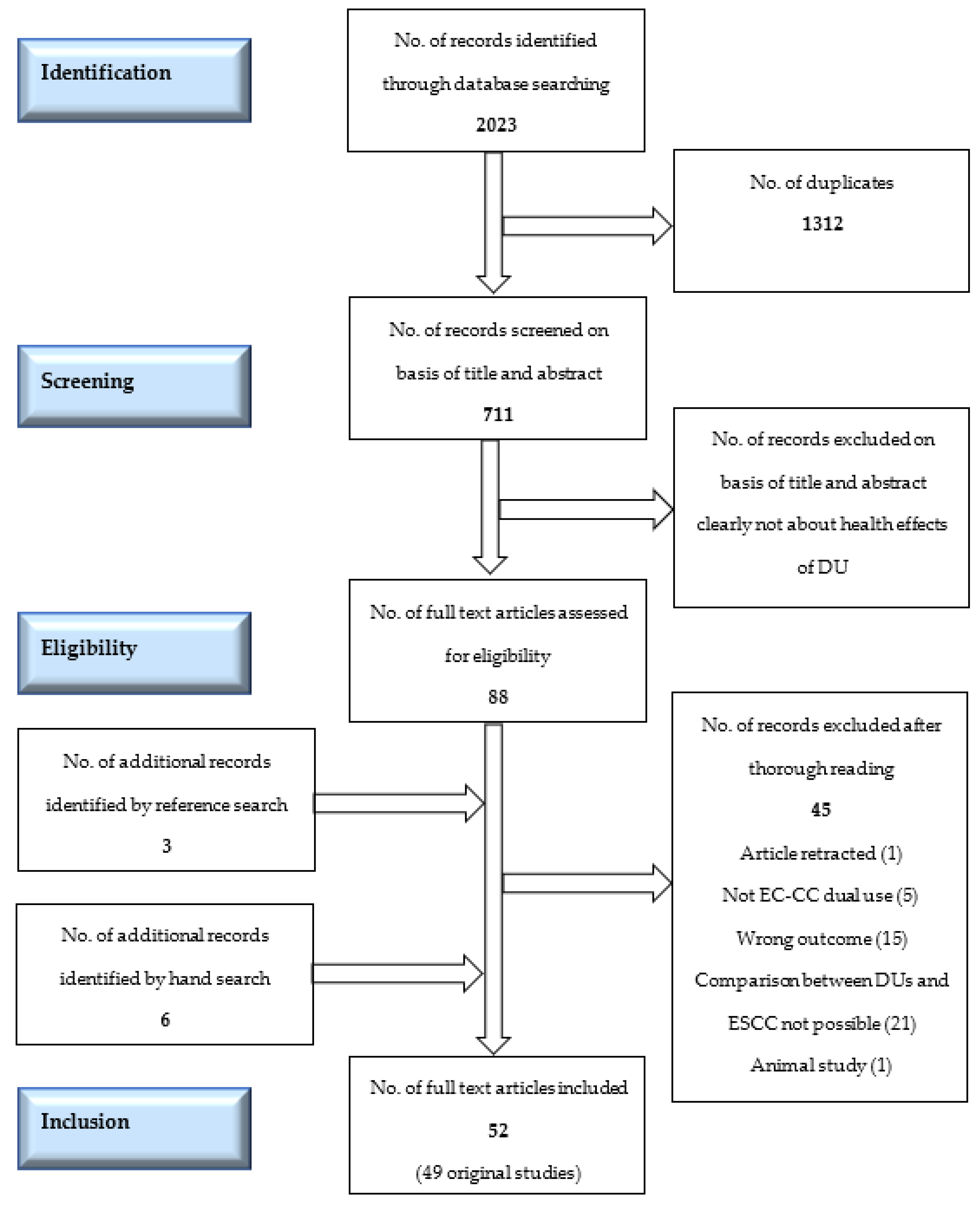
2.5. Selection Process
2.6. Data Collection Process
2.7. Risk of Bias and Quality Assessment
2.8. Effect Measures
2.9. Data Items
2.10. Synthesis Methods
3. Results
3.1. Study Design
3.2. Definitions of Use (Exposure Measurement)
3.3. Conflict of Interest
3.4. Quality Assessment
3.5. Findings from the Prospective Studies (Table 1)
3.6. Cross-Sectional Studies (Table 2)
3.7. Intensity of Smoking or EC use and Impact on Health
3.8. Synthesis of the Results
4. Discussion
4.1. Overall Findings
4.2. Comparison with Other Studies and Considerations about Findings
4.3. Limitations of the Review
4.4. Strengths of the Review
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ESCC | exclusive smokers of conventional cigarettes |
| DU | dual use of conventional cigarettes and e-cigarettes |
| DUs | dual users of conventional cigarettes and e-cigarettes |
| COPD | chronic obstructive pulmonary disease |
| CRP | human c-reactive protein |
| CVD | cardiovascular disease |
| GCF | gingival crevicular fluid |
| 3-HPMA | Urinary 3-hydroxypropyl mercapturic acid, a major metabolite of acrolein |
| TSNA | Tobacco-specific N-nitrosamines |
| PAH | polycyclic aromatic hydrocarbons |
| HDL | high density lipids |
| GTT | glucose tolerance test |
| HbA1c | glycosylated hemoglobin |
| HPMA | N-acetyl-S-3-hydroxypropylcysteine, a metabolite of acrolein (VOC) |
| MHB3 | a metabolite of 1,3-butadiene (VOC) |
| NNAL | 4-(methylnitrosamino)-1-(3-pyridyl)-1-butanol, the principal metabolite of the lung carcinogen NNK (TSNA) |
| PMA | benzene |
| VOC | Volatile organic compounds |
References
- GSTHR. 82 Million Vapers Worldwide in 2021: The GSTHR Estimate. Briefing Papers: 2022. Available online: https://gsthr.org/briefing-papers/82-million-vapers-worldwide-in-2021-the-gsthr-estimate/ (accessed on 10 October 2022).
- McNeill, A.; Brose, L.S.; Calder, R.; Hitchman, S.; Hajek, P.; McRobbie, H. E-Cigarettes: An Evidence Update; England PH, Ed.; Public Health England: London, UK, 2015.
- Hartmann-Boyce, J.; McRobbie, H.; Butler, A.R.; Lindson, N.; Bullen, C.; Begh, R.; Theodoulou, A.; Notley, C.; Rigotti, N.A.; Turner, T.; et al. Electronic cigarettes for smoking cessation. Cochrane Tobacco Addiction Group, editor. Cochrane Database Syst. Rev. 2021, 4, CD010216. [Google Scholar] [CrossRef] [PubMed]
- Tobacco: E-cigarettes. Available online: https://www.who.int/news-room/questions-and-answers/item/tobacco-e-cigarettes (accessed on 10 October 2022).
- Country Laws Regulating E-cigarettes: A Policy Scan. Available online: https://www.globaltobaccocontrol.org/en/policy-scan/e-cigarettes/countries?country=263 (accessed on 10 October 2022).
- Samet, J.M.; Barrington-Trimis, J. E-Cigarettes and Harm Reduction: An Artificial Controversy Instead of Evidence and a Well-Framed Decision Context. Am. J. Public Health 2021, 111, 1572–1574. [Google Scholar] [CrossRef] [PubMed]
- Patel, D.; Davis, K.C.; Cox, S.; Bradfield, B.; King, B.A.; Shafer, P.; Caraballo, R.; Bunnell, R. Reasons for current E -cigarette use among U.S. adults. Prev. Med. 2016, 93, 14–20. [Google Scholar] [CrossRef]
- Calder, R.; Gant, E.; Bauld, L.; McNeill, A.; Robson, D.; Brose, L.S. Vaping in Pregnancy: A Systematic Review. Nicotine Tob. Res. 2021, 23, 1451–1458. [Google Scholar] [CrossRef] [PubMed]
- Using E-Cigarettes to Stop Smoking. NHS. Available online: https://www.nhs.uk/live-well/quit-smoking/using-e-cigarettes-to-stop-smoking/ (accessed on 10 October 2022).
- Harm Reduction and Vaping. Action for Smokefree 2025 (ASH). Available online: https://www.ash.org.nz/vaping-and-harm-reduction (accessed on 10 October 2022).
- Hedman, L.; Galanti, M.R.; Ryk, L.; Gilljam, H.; Adermark, L. Electronic cigarette use and smoking cessation in cohort studies and randomized trials: A systematic review and meta-analysis. Tob. Prev. Cessat. 2021, 7, 62. [Google Scholar] [CrossRef] [PubMed]
- Hedman, L.; Backman, H.; Stridsman, C.; Bosson, J.A.; Lundbäck, M.; Lindberg, A.; Rönmark, E.; Ekerljung, L. Association of Electronic Cigarette Use with Smoking Habits, Demographic Factors, and Respiratory Symptoms. JAMA Netw. Open 2018, 1, e180789. [Google Scholar] [CrossRef] [PubMed]
- Jeon, C.; Jung, K.J.; Kimm, H.; Lee, S.; Barrington-Trimis, J.L.; McConnell, R.; Samet, J.M.; Jee, S.H. E-cigarettes, conventional cigarettes, and dual use in Korean adolescents and university students: Prevalence and risk factors. Drug Alcohol Depend. 2016, 168, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.Y.; Wang, Y.; Yao, T.; Lightwood, J.; Max, W. Polytobacco Use and Nicotine Dependence Symptoms Among US Adults, 2012–2014. Nicotine Tob. Res. 2018, 20 (Suppl. 1), S88–S98. [Google Scholar] [CrossRef] [PubMed]
- Goniewicz, M.L.; Smith, D.M.; Edwards, K.C.; Blount, B.C.; Caldwell, K.L.; Feng, J.; Wang, L.; Christensen, C.; Ambrose, B.; Borek, N.; et al. Comparison of Nicotine and Toxicant Exposure in Users of Electronic Cigarettes and Combustible Cigarettes. JAMA Netw. Open 2018, 1, e185937. [Google Scholar] [CrossRef] [PubMed]
- Grana, R.; Benowitz, N.; Glantz, S.A. E-Cigarettes: A Scientific Review. Circulation 2014, 129, 1972–1986. [Google Scholar] [CrossRef] [PubMed]
- Maglia, M.; Caponnetto, P.; Di Piazza, J.; La Torre, D.; Polosa, R. Dual use of electronic cigarettes and classic cigarettes: A systematic review. Addict. Res. Theory 2018, 26, 330–338. [Google Scholar] [CrossRef]
- Fears of Growth in Children Vaping Disposables Backed up by New National Survey. Action on Smoking and Health (ash). Available online: https://ash.org.uk/media-centre/news/press-releases/fears-of-growth-in-children-vaping-disposables-backed-up-by-new-national-survey (accessed on 10 October 2022).
- Christensen, T.; Welsh, E.; Faseru, B. Profile of e-cigarette use and its relationship with cigarette quit attempts and abstinence in Kansas adults. Prev. Med. 2014, 69, 90–94. [Google Scholar] [CrossRef] [PubMed]
- Xiao, L.; Yin, X.; Di, X.; Nan, Y.; Lyu, T.; Wu, Y.; Li, X. Awareness and prevalence of e-cigarette use among Chinese adults: Policy implications. Tob. Control 2021, 31, 498–504. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.Y.; Paek, Y.J.; Seo, H.G.; Cheong, Y.S.; Lee, C.M.; Park, S.M.; Park, D.W.; Lee, K. Dual use of electronic and conventional cigarettes is associated with higher cardiovascular risk factors in Korean men. Sci. Rep. 2020, 10, 5612. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.; Choi, H.; Kang, J.; Kim, J. Association between electronic cigarette use and metabolic syndrome in the Korean general population: A nationwide population-based study. PLoS ONE 2020, 15, e0237983. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.; Kim, Y.; Kang, J. Association of electronic cigarette exposure with serum uric acid level and hyperuricemia: 2016-2017 Korea National Health and Nutritional Examination Survey. PLoS ONE 2021, 16, e0247868. [Google Scholar] [CrossRef] [PubMed]
- Xie, Z.; Ossip, D.J.; Rahman, I.; Li, D. Use of Electronic Cigarettes and Self-Reported Chronic Obstructive Pulmonary Disease Diagnosis in Adults. Nicotine Tob. Res. 2020, 22, 1155–1161. [Google Scholar] [CrossRef]
- Chen, D.T.H.; Kyriakos, C.N. Cigarette and E-Cigarettes Dual Users, Exclusive Users and COVID-19: Findings from Four UK Birth Cohort Studies. Int. J. Environ. Res. Public Health 2021, 18, 3935. [Google Scholar] [CrossRef]
- Osei, A.D.; Mirbolouk, M.; Orimoloye, O.A.; Dzaye, O.; Uddin, S.I.; Benjamin, E.J.; Hall, M.E.; DeFilippis, A.P.; Stokes, A.; Bhatnagar, A.; et al. Association Between E-Cigarette Use and Cardiovascular Disease Among Never and Current Combustible-Cigarette Smokers. Am. J. Med. 2019, 132, 949–954.e2. [Google Scholar] [CrossRef] [PubMed]
- Miller, C.R.; Shi, H.; Li, D.; Goniewicz, M.L. Cross-Sectional Associations of Smoking and E-cigarette Use with Self-Reported Diagnosed Hypertension: Findings from Wave 3 of the Population Assessment of Tobacco and Health Study. Toxics 2021, 9, 52. [Google Scholar] [CrossRef]
- Manzoli, L.; Flacco, M.E.; Ferrante, M.; La Vecchia, C.; Siliquini, R.; Ricciardi, W.; Marzuillo, C.; Villari, P.; Fiore, M. Cohort study of electronic cigarette use: Effectiveness and safety at 24 months. Tob. Control 2017, 26, 284–292. [Google Scholar] [CrossRef] [PubMed]
- Flacco, M.E.; Fiore, M.; Acuti Martellucci, C.; Ferrante, M.; Gualano, M.R.; Liguori, G.; Bravi, F.; Pirone, G.M.; Marzuillo, C.; Manzoli, L. Tobacco vs. electronic cigarettes: Absence of harm reduction after six years of follow-up. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 3923–3934. [Google Scholar] [PubMed]
- Sweet, L.; Brasky, T.M.; Cooper, S.; Doogan, N.; Hinton, A.; Klein, E.G.; Nagaraja, H.; Quisenberry, A.; Xi, W.; Wewers, M.E. Quitting Behaviors Among Dual Cigarette and E-Cigarette Users and Cigarette Smokers Enrolled in the Tobacco User Adult Cohort. Nicotine Tob. Res. 2019, 21, 278–284. [Google Scholar] [CrossRef] [PubMed]
- Osibogun, O.; Bursac, Z.; Mckee, M.; Li, T.; Maziak, W. Cessation outcomes in adult dual users of e-cigarettes and cigarettes: The Population Assessment of Tobacco and Health cohort study, USA, 2013–2016. Int. J. Public Health 2020, 65, 923–936. [Google Scholar] [CrossRef] [PubMed]
- Hinton, A.; Nagaraja, H.N.; Cooper, S.; Wewers, M.E. Tobacco product transition patterns in rural and urban cohorts: Where do dual users go? Prev. Med. Rep. 2018, 12, 241–244. [Google Scholar] [CrossRef] [PubMed]
- Wei, L.; Muhammad-Kah, R.S.; Hannel, T.; Pithawalla, Y.B.; Gogova, M.; Chow, S.; Black, R.A. The impact of cigarette and e-cigarette use history on transition patterns: A longitudinal analysis of the population assessment of tobacco and health (PATH) study, 2013–2015. Harm Reduct. J. 2020, 17, 45. [Google Scholar] [CrossRef]
- Piper, M.E.; Baker, T.B.; Benowitz, N.L.; Jorenby, D.E. Changes in Use Patterns Over 1 Year Among Smokers and Dual Users of Combustible and Electronic Cigarettes. Nicotine Tob. Res. 2020, 22, 672–680. [Google Scholar] [CrossRef]
- Manzoli, L.; Flacco, M.E.; Fiore, M.; La Vecchia, C.; Marzuillo, C.; Gualano, M.R.; Liguori, G.; Cicolini, G.; Capasso, L.; D’Amario, C.; et al. Electronic Cigarettes Efficacy and Safety at 12 Months: Cohort Study. PLoS ONE 2015, 10, e0129443. [Google Scholar] [CrossRef] [PubMed]
- Etter, J.F. A longitudinal study of cotinine in long-term daily users of e-cigarettes. Drug Alcohol Depend. 2016, 160, 218–221. [Google Scholar] [CrossRef] [PubMed]
- Huh, J.; Leventhal, A.M. Intraindividual covariation between e-cigarette and combustible cigarette use in Korean American emerging adults. Psychol. Addict. Behav. 2016, 30, 246–251. [Google Scholar] [CrossRef] [PubMed]
- Goniewicz, M.L.; Leigh, N.J.; Gawron, M.; Nadolska, J.; Balwicki, L.; McGuire, C.; Sobczak, A. Dual use of electronic and tobacco cigarettes among adolescents: A cross-sectional study in Poland. Int. J. Public Health 2016, 61, 189–197. [Google Scholar] [CrossRef] [PubMed]
- DeVito, E.E.; Fagle, T.; Allen, A.M.; Pang, R.D.; Petersen, N.; Smith, P.H.; Weinberger, A.H. Electronic Nicotine Delivery Systems (ENDS) Use and Pregnancy I: ENDS Use Behavior During Pregnancy. Curr. Addict. Rep. 2021, 8, 347–365. [Google Scholar] [CrossRef] [PubMed]
- E-Cigarette, or Vaping, Product Visual Dictionary. U.S. Department of Health and Human Services. Center for Disease Control and Prevention. Available online: https://www.cdc.gov/tobacco/basic_information/e-cigarettes/pdfs/ecigarette-or-vaping-products-visual-dictionary-508.pdf (accessed on 10 October 2022).
- Rankin, G.D.; Wingfors, H.; Uski, O.; Hedman, L.; Ekstrand-Hammarström, B.; Bosson, J.; Lundbäck, M. The toxic potential of a fourth-generation E-cigarette on human lung cell lines and tissue explants. J. Appl. Toxicol. 2019, 39, 1143–1154. [Google Scholar] [CrossRef]
- Cardenas, V.M.; Cen, R.; Clemens, M.M.; Moody, H.L.; Ekanem, U.S.; Policherla, A.; Fischbach, L.A.; Eswaran, H.; Magann, E.F.; Delongchamp, R.R.; et al. Use of Electronic Nicotine Delivery Systems (ENDS) by pregnant women I: Risk of small-for-gestational-age birth. Tob. Induc. Dis. 2019, 17, 44. Available online: http://www.journalssystem.com/tid/Use-of-Electronic-Nicotine-Delivery-Systems-by-Pregnant-Women-I-Risk-of-Small-for,106089,0,2.html (accessed on 10 October 2022). [CrossRef] [PubMed]
- Clemens, M.M.; Cardenas, V.M.; Fischbach, L.A.; Cen, R.; Siegel, E.R.; Eswaran, H.; Ekanem, U.S.; Policherla, A.; Moody, H.L.; Magann, E.F.; et al. Use of electronic nicotine delivery systems by pregnantwomen II: Hair biomarkers for exposures to nicotine andtobacco-specific nitrosamines. Tob. Induc. Dis. 2019, 17, 50. Available online: http://www.journalssystem.com/tid/Use-of-Electronic-Nicotine-Delivery-Systems-by-Pregnant-Women-II-Hair-Biomarkers,105387,0,2.html (accessed on 10 October 2022). [CrossRef]
- Harlow, A.F.; Hatch, E.E.; Wesselink, A.K.; Rothman, K.J.; Wise, L.A. Electronic Cigarettes and Fecundability: Results From a Prospective Preconception Cohort Study. Am. J. Epidemiol. 2021, 190, 353–361. [Google Scholar] [CrossRef]
- McDonnell, B.; Dicker, P.; Regan, C. Electronic cigarettes and obstetric outcomes: A prospective observational study. BJOG Int. J. Obstet. Gy. 2020, 127, 750–756. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Lee, N.L.; Burstyn, I. Smoking and use of electronic cigarettes (vaping) in relation to preterm birth and small-for-gestational-age in a 2016 U.S. national sample. Prev. Med. 2020, 134, 106041. [Google Scholar] [CrossRef]
- McRobbie, H.; Phillips, A.; Goniewicz, M.L.; Smith, K.M.; Knight-West, O.; Przulj, D.; Hajek, P. Effects of Switching to Electronic Cigarettes with and without Concurrent Smoking on Exposure to Nicotine, Carbon Monoxide, and Acrolein. Cancer Prev. Res. 2015, 8, 873–878. [Google Scholar] [CrossRef]
- Bhatta, D.N.; Glantz, S.A. Association of E-Cigarette Use with Respiratory Disease Among Adults: A Longitudinal Analysis. Am. J. Prev. Med. 2020, 58, 182–190. [Google Scholar] [CrossRef]
- Sanou, A.Z.; Ziadeh, C.; Stahlman, S.; Clausen, S.S. Acute Respiratory Infections Among Active Component Service Members Who Use Combustible Tobacco Products and/or E-cigarette/Vaping Products, U.S. Armed Forces, 2018–2019. MSMR 2020, 27, 2–7. [Google Scholar] [PubMed]
- Flacco, M.E.; Ferrante, M.; Flore, M.; Marzuillo, C.; La Vecchia, C.; Gualano, M.R.; Liguori, G.; Fragassi, G.; Carradori, T.; Bravi, F.; et al. Cohort study of electronic cigarette use: Safety and effectiveness after 4 years of follow-up. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 402–412. [Google Scholar] [PubMed]
- Riehm, K.E.; Rojo-Wissar, D.M.; Feder, K.A.; Mojtabai, R.; Spira, A.P.; Thrul, J.; Crum, R.M. E-cigarette use and sleep-related complaints among youth. J. Adolesc. 2019, 76, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Prokopowicz, A.; Sobczak, A.; Szuła-Chraplewska, M.; Ochota, P.; Kośmider, L. Exposure to Cadmium and Lead in Cigarette Smokers Who Switched to Electronic Cigarettes. Nicotine Tob. Res. 2019, 21, 1198–1205. [Google Scholar] [CrossRef]
- Carroll, D.M.; Wagener, T.L.; Peck, J.D.; Brame, L.S.; Thompson, D.M.; Stephens, L.D.; Campbell, J.E.; Beebe, L.A. Biomarkers of Exposure in ENDS Users, Smokers, and Dual Users of American Indian Descent. Tob. Regul. Sci. 2018, 4, 3–15. [Google Scholar] [CrossRef]
- Jain, R.B. Concentrations of cadmium, lead, and mercury in blood among US cigarettes, cigars, electronic cigarettes, and dual cigarette-e-cigarette users. Environ. Pollut. 2019, 251, 970–974. [Google Scholar] [CrossRef]
- Keith, R.J.; Fetterman, J.L.; Orimoloye, O.A.; Dardari, Z.; Lorkiewicz, P.K.; Hamburg, N.M.; DeFilippis, A.P.; Blaha, M.J.; Bhatnagar, A. Characterization of Volatile Organic Compound Metabolites in Cigarette Smokers, Electronic Nicotine Device Users, Dual Users, and Nonusers of Tobacco. Nicotine Tob. Res. 2020, 22, 264–272. [Google Scholar] [CrossRef]
- Prokopowicz, A.; Sobczak, A.; Szdzuj, J.; Grygoyć, K.; Kośmider, L. Metal Concentration Assessment in the Urine of Cigarette Smokers Who Switched to Electronic Cigarettes: A Pilot Study. Int. J. Environ. Res. Public Health 2020, 17, 1877. [Google Scholar] [CrossRef]
- Rostron, B.L.; Corey, C.G.; Chang, J.T.; van Bemmel, D.M.; Miller, M.E.; Chang, C.M. Associations of Cigarettes Smoked Per Day with Biomarkers of Exposure Among U.S. Adult Cigarette Smokers in the Population Assessment of Tobacco and Health (PATH) Study Wave 1 (2013–2014). Cancer Epidemiol. Biomark. Prev. 2019, 28, 1443–1453. [Google Scholar] [CrossRef]
- Shahab, L.; Goniewicz, M.L.; Blount, B.C.; Brown, J.; McNeill, A.; Alwis, K.U.; Feng, J.; Wang, L.; West, R. Nicotine, Carcinogen, and Toxin Exposure in Long-Term E-Cigarette and Nicotine Replacement Therapy Users: A Cross-sectional Study. Ann. Intern. Med. 2017, 166, 390. [Google Scholar] [CrossRef]
- Smith, D.M.; Shahab, L.; Blount, B.C.; Gawron, M.; Kosminder, L.; Sobczak, A.; Xia, B.; Sosnoff, C.S.; Goniewicz, M.L. Differences in Exposure to Nicotine, Tobacco-Specific Nitrosamines, and Volatile Organic Compounds among Electronic Cigarette Users, Tobacco Smokers, and Dual Users from Three Countries. Toxics 2020, 8, 88. [Google Scholar] [CrossRef] [PubMed]
- Cho, J.H.; Paik, S.Y. Association between Electronic Cigarette Use and Asthma among High School Students in South Korea. Fehrenbach H, editor. PLoS ONE 2016, 11, e0151022. [Google Scholar]
- Chung, S.J.; Kim, B.K.; Oh, J.H.; Shim, J.S.; Chang, Y.S.; Cho, S.H.; Yang, M.S. Novel tobacco products including electronic cigarette and heated tobacco products increase risk of allergic rhinitis and asthma in adolescents: Analysis of Korean youth survey. Allergy 2020, 75, 1640–1648. [Google Scholar] [CrossRef]
- Lee, A.; Lee, S.Y.; Lee, K.S. The Use of Heated Tobacco Products is Associated with Asthma, Allergic Rhinitis, and Atopic Dermatitis in Korean Adolescents. Sci. Rep. 2019, 9, 17699. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Sundar, I.K.; McIntosh, S.; Ossip, D.J.; Goniewicz, M.L.; O’Connor, R.J.; Rahman, I. Association of smoking and electronic cigarette use with wheezing and related respiratory symptoms in adults: Cross-sectional results from the Population Assessment of Tobacco and Health (PATH) study, wave 2. Tob. Control 2019, 29, 140–147. [Google Scholar] [CrossRef] [PubMed]
- Osei, A.D.; Mirbolouk, M.; Orimoloye, O.A.; Dzaye, O.; Uddin, S.I.; Benjamin, E.J.; Hall, M.E.; DeFilippis, A.P.; Bhatnagar, A.; Biswal, S.S.; et al. Association Between E-Cigarette Use and Chronic Obstructive Pulmonary Disease by Smoking Status: Behavioral Risk Factor Surveillance System 2016 and 2017. Am. J. Prev. Med. 2020, 58, 336–342. [Google Scholar] [CrossRef]
- Parekh, T.; Owens, C.; Fay, K.; Phillips, J.; Kitsantas, P. Use of e-Cigarettes and Development of Respiratory Conditions in Women of Childbearing Age. South Med. J. 2020, 113, 448–494. [Google Scholar] [CrossRef]
- Wang, J.B.; Olgin, J.E.; Nah, G.; Vittinghoff, E.; Cataldo, J.K.; Pletcher, M.J.; Marcus, G.M. Cigarette and e-cigarette dual use and risk of cardiopulmonary symptoms in the Health eHeart Study. PLoS ONE 2018, 13, e0198681. [Google Scholar] [CrossRef]
- Wills, T.A.; Pagano, I.; Williams, R.J.; Tam, E.K. E-cigarette use and respiratory disorder in an adult sample. Drug Alcohol Depend. 2019, 194, 363–370. [Google Scholar] [CrossRef]
- Wills, T.A.; Choi, K.; Pagano, I. E-Cigarette Use Associated with Asthma Independent of Cigarette Smoking and Marijuana in a 2017 National Sample of Adolescents. J. Adolesc. Health 2020, 67, 524–530. [Google Scholar] [CrossRef]
- Choi, D.W.; Jeon, J.; Lee, S.; Han, K.T.; Park, E.C.; Jang, S.I. Association between Smoking Behavior Patterns and Glycated Hemoglobin Levels in a General Population. Int. J. Environ. Res. Public Health 2018, 15, 2260. [Google Scholar] [CrossRef] [PubMed]
- Fetterman, J.L.; Keith, R.J.; Palmisano, J.N.; McGlasson, K.L.; Weisbrod, R.M.; Majid, S.; Bastin, R.; Stathos, M.M.; Stokes, A.C.; Robertson, R.M.; et al. Alterations in Vascular Function Associated with the Use of Combustible and Electronic Cigarettes. JAHA 2020, 9, e014570. [Google Scholar] [CrossRef] [PubMed]
- Mainous, A.G.; Yadav, S.; Hong, Y.R.; Huo, J. E-Cigarette and Conventional Tobacco Cigarette Use, Dual Use, and C-Reactive Protein. J. Am. Coll. Cardiol. 2020, 75, 2271–2273. [Google Scholar] [CrossRef]
- Orimoloye, O.A.; Uddin, S.I.; Chen, L.C.; Osei, A.D.; Mirbolouk, M.; Malovichko, M.V.; Sithu, I.D.; Dzaye, O.; Conklin, D.J.; Srivastava, S.; et al. Electronic cigarettes and insulin resistance in animals and humans: Results of a controlled animal study and the National Health and Nutrition Examination Survey (NHANES 2013–2016). PLoS ONE 2019, 14, e0226744. [Google Scholar] [CrossRef] [PubMed]
- Parekh, T.; Pemmasani, S.; Desai, R. Risk of Stroke with E-Cigarette and Combustible Cigarette Use in Young Adults. Am. J. Prev. Med. 2020, 58, 446–452. [Google Scholar] [CrossRef] [PubMed]
- Vindhyal, M.R.; Okut, H.; Ablah, E.; Ndunda, P.M.; Kallail, K.J.; Choi, W.S. Cardiovascular Outcomes Associated with Adult Electronic Cigarette Use. Cureus 2020, 12, e9618. Available online: https://www.cureus.com/articles/38144-cardiovascular-outcomes-associated-with-adult-electronic-cigarette-use (accessed on 10 October 2022). [CrossRef]
- Akinkugbe, A.A. Cigarettes, E-cigarettes, and Adolescents’ Oral Health: Findings from the Population Assessment of Tobacco and Health (PATH) Study. JDR Clin. Transl. Res. 2019, 4, 276–283. [Google Scholar] [CrossRef]
- Dinkeloo, E.; Grier, T.L.; Brooks, R.D.; Jones, B.H. Vaping, Smoking, and the Physical Fitness of Active Young Men. Am. J. Prev. Med. 2020, 58, e31–e37. [Google Scholar] [CrossRef]
- Gaiha, S.M.; Cheng, J.; Halpern-Felsher, B. Association Between Youth Smoking, Electronic Cigarette Use, and COVID-19. J. Adolesc. Health 2020, 67, 519–523. [Google Scholar] [CrossRef]
- Leavens, E.L.; Ford, B.R.; Ojo-Fati, O.; Winkelman, T.N.; Vickery, K.D.; Japuntich, S.J.; Busch, A.M. Electronic cigarette use patterns and chronic health conditions among people experiencing homelessness in MN: A statewide survey. BMC Public Health 2020, 20, 1889. [Google Scholar] [CrossRef]
- Merianos, A.L.; Jandarov, R.A.; Choi, K.; Fiser, K.A.; Mahabee-Gittens, E.M. Combustible and electronic cigarette use and insufficient sleep among U.S. high school students. Prev. Med. 2021, 147, 106505. [Google Scholar] [CrossRef] [PubMed]
- YYe, D.; Gajendra, S.; Lawyer, G.; Jadeja, N.; Pishey, D.; Pathagunti, S.; Lyons, J.; Veazie, P.; Watson, G.; McIntosh, S.; et al. Inflammatory biomarkers and growth factors in saliva and gingival crevicular fluid of e-cigarette users, cigarette smokers, and dual smokers: A pilot study. J. Periodontol. 2020, 91, 1274–1283. [Google Scholar] [CrossRef] [PubMed]
- Committee on the Review of the Health Effects of Electronic Nicotine Delivery Systems; Board on Population Health and Public Health Practice, Health and Medicine Division; National Academies of Sciences, Engineering, and Medicine. Public Health Consequences of E-Cigarettes; Stratton, K., Kwan, L.Y., Eaton, D.L., Eds.; National Academies Press: Washington, DC, USA, 2018; Available online: https://www.nap.edu/catalog/24952 (accessed on 10 October 2022).
- Czoli, C.D.; Fong, G.T.; Goniewicz, M.L.; Hammond, D. Biomarkers of Exposure Among “Dual Users” of Tobacco Cigarettes and Electronic Cigarettes in Canada. Nicotine Tob. Res. 2019, 21, 1259–1266. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Lee, S. Daily Cigarette Consumption and Urine Cotinine Level between Dual Users of Electronic and Conventional Cigarettes, and Cigarette-Only Users. J. Psychoact. Drugs 2020, 52, 20–26. [Google Scholar] [CrossRef]
- Beard, E.; Brown, J.; Michie, S.; West, R. Is prevalence of e-cigarette and nicotine replacement therapy use among smokers associated with average cigarette consumption in England? A time-series analysis. BMJ Open 2018, 8, e016046. [Google Scholar] [CrossRef]
- Tehrani, M.W.; Newmeyer, M.N.; Rule, A.M.; Prasse, C. Characterizing the Chemical Landscape in Commercial E-Cigarette Liquids and Aerosols by Liquid Chromatography–High-Resolution Mass Spectrometry. Chem. Res. Toxicol. 2021, 34, 2216–2226. [Google Scholar] [CrossRef]
- Pisinger, C.; Døssing, M. A systematic review of health effects of electronic cigarettes. Prev. Med. 2014, 69, 248–260. [Google Scholar] [CrossRef]
- Wills, T.A.; Soneji, S.S.; Choi, K.; Jaspers, I.; Tam, E.K. E-cigarette use and respiratory disorders: An integrative review of converging evidence from epidemiological and laboratory studies. Eur. Respir. J. 2021, 57, 1901815. [Google Scholar] [CrossRef]
- Davis, L.C.; Sapey, E.; Thickett, D.R.; Scott, A. Predicting the pulmonary effects of long-term e-cigarette use: Are the clouds clearing? Eur. Respir. Rev. 2022, 31, 210121. [Google Scholar] [CrossRef]
- Espinoza-Derout, J.; Shao, X.M.; Lao, C.J.; Hasan, K.M.; Rivera, J.C.; Jordan, M.C.; Echeverria, V.; Roos, K.P.; Sinha-Hikim, A.P.; Friedman, T.C. Electronic Cigarette Use and the Risk of Cardiovascular Diseases. Front. Cardiovasc. Med. 2022, 9, 879726. [Google Scholar] [CrossRef]
- Skotsimara, G.; Antonopoulos, A.S.; Oikonomou, E.; Siasos, G.; Ioakeimidis, N.; Tsalamandris, S.; Charalambous, G.; Galiatsatos, N.; Vlachopoulos, C.; Tousoulis, D. Cardiovascular effects of electronic cigarettes: A systematic review and meta-analysis. Eur. J. Prev. Cardiolog. 2019, 26, 1219–1228. [Google Scholar] [CrossRef] [PubMed]
- Armendáriz-Castillo, I.; Guerrero, S.; Vera-Guapi, A.; Cevallos-Vilatuña, T.; García-Cárdenas, J.M.; Guevara-Ramírez, P.; López-Cortés, A.; Pérez-Villa, A.; Yumiceba, V.; Zambrano, A.K.; et al. Genotoxic and Carcinogenic Potential of Compounds Associated with Electronic Cigarettes: A Systematic Review. BioMed. Res. Int. 2019, 2019, 1386710. [Google Scholar] [CrossRef]
- Alzahrani, T.; Pena, I.; Temesgen, N.; Glantz, S.A. Association between electronic cigarette use and myocardial infarction. Am. J. Prev. Med. 2018, 55, 455–461, Erratum in Am. J. Prev. Med. 2019, 57, 579–584. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Gupta, I.; Venkatesh, U.; Singh, A.K.; Golamari, R.; Arya, P. E-cigarettes and myocardial infarction: A systematic review and meta-analysis. Int. J. Cardiol. 2022, 28, S0167527322013158. [Google Scholar] [CrossRef]
- Patel, U.; Patel, N.; Khurana, M.; Parulekar, A.; Patel, A.; Ortiz, J.F.; Patel, R.; Urhoghide, E.; Mistry, A.; Bhriguvanshi, A.; et al. Effect Comparison of E-Cigarette and Traditional Smoking and Association with Stroke—A Cross-Sectional Study of NHANES. Neurol. Int. 2022, 14, 441–452. [Google Scholar] [CrossRef] [PubMed]
- Yang, I.; Sandeep, S.; Rodriguez, J. The oral health impact of electronic cigarette use: A systematic review. Crit. Rev. Toxicol. 2020, 50, 97–127. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, C.D.; van Schalkwyk, M.C.I.; McKee, M.; Pisinger, C. The cardiovascular effects of electronic cigarettes: A systematic review of experimental studies. Prev. Med. 2019, 127, 105770. [Google Scholar] [CrossRef]
- Banks, E.; Yazidjoglou, A.; Brown, S.; Nguyen, M.; Martin, M.; Beckwith, K.; Daluwatta, A.; Campbell, S.; Joshy, G. Electronic Cigarettes and Health Outcoomes: Systematic Review of Global Evidence. National Centre for Epidemiology and Population Health: Australian National University. Available online: https://openresearch-repository.anu.edu.au/bitstream/1885/262914/1/Electronic%20cigarettes%20health%20outcomes%20review_2022_WCAG.pdf (accessed on 10 October 2022).
- Williams, M.; Talbot, P. Design Features in Multiple Generations of Electronic Cigarette Atomizers. Int. J. Environ. Res. Public Health 2019, 16, 2904. [Google Scholar] [CrossRef]
- PATH Study Findings Give Insight into Flavored Tobacco, Health Effects of E-Cigarettes, and Adult Use of Cigars and Hookah. U.S. Food & Drug Administration. Available online: https://www.fda.gov/tobacco-products/research/path-study-findings-give-insight-flavored-tobacco-health-effects-e-cigarettes-and-adult-use-cigars (accessed on 10 October 2022).
- Soule, E.; Bansal-Travers, M.; Grana, R.; McIntosh, S.; Price, S.; Unger, J.B.; Walton, K. Electronic cigarette use intensity measurement challenges and regulatory implications. Tob. Control 2021. [Google Scholar] [CrossRef]


{kind=link}
| First Author, Year of Publication, Country, Conflict of Interest | Method | Participants | Risk of Selection Bias/Weighted Data/Adjusted Analyses/Adjusted for Former Tobacco Consumption | Major Outcomes | Overall Findings Significantly (Higher Risk/Prevalence/Level in ESCC = ## Higher Risk/Prevalence/Level in ESCC, Significance Level Not Tested or Not Significant = # Same Risk/Prevalence/Level in ESCC and DUs = ¤ Higher Risk/Prevalence/Level in DUs, Significance Level Not Tested or Not Significant = * Significantly Higher Risk/Prevalence/Level in DUs = **) | |
|---|---|---|---|---|---|---|
| Pregnancy and fertility | Cardenas V.M. [42] 2020, USA None | Pregnancy Risk Assessment Monitoring | 1594 pregnant women | Low/yes/yes/no | Risk of small-for-gestational-age | DUs: higher odds of giving birth to a small-for-gestational-age child than ESCC, but significance level not tested * |
| Clemens M.M. [43] § 2019, USA None | Pregnancy Risk Assessment Monitoring | 248 pregnant women | Low/yes/yes/no | Carcinogen metabolites (TSNAs) in hair samples + Risk of small-for-gestational-age (SGA) | DUs same level of carcinogen biomarkers as ESCC ¤ DUs had higher risk of small-for-gestational-age than ESCC, but significance not tested * | |
| Harlow A. [44] 2020, USA None | Cohort study, online survey | 4586 young women trying to conceive | Low/no/yes/ yes | Fecundability (menstrual cycle and achieved pregnancy) | DUs: lower fecundability ratio than ESCC, but not significantly different * | |
| McDonnell BP. [45] 2020, Ireland None | Pregnancy Risk Assessment Monitoring | 620 pregnant women | Low/no/yes/no | Delivery and neonatal outcomes | DUs: same birthweight, Apgar score and mean gestation at delivery as ESCC ¤ DUs: higher rate of admission to neonatal intensive care unit and higher incidence of birthweight <10th centile than ESCC but significance level not tested * | |
| Wang X. [46] 2020, USA None | Pregnancy Risk Assessment Monitoring | 31,973 pregnant women | Low/yes/yes/no | Preterm birth and small-for-gestational-age (SGA) | Similar (elevated) risk of preterm birth and of small-for-gestational-age in DU as ESCC ¤ | |
| Other | McRobbie H. [47] 2015, UK  Yes Yes | Smoking cessation study with 4 weeks follow-up | 44 healthy volunteer smokers Use of EC ad libitum | High/-/no/no | Urinary 3-HPMA, a major metabolite of acrolein and carbon-monoxide (CO) | DUs had sign. reductions in 3-HPMA and CO after switching from ESCC (significant reduction in cotinine in DU) ## |
| Bhatta D. N. [48] 2020, USA None | Nationally representative cohort study | 32,320 adults | Low/yes/yes/no | Self-reported respiratory disease (chronic obstructive pulmonary Disease (COPD), chronic bronchitis, emphysema, or asthma) | DUs: higher odds of reporting of respiratory disease than ESCC but significance level not tested * | |
| Sanou A. Z. [49] 2020, USA None | Register study using a cohort | 802,621 adult military members | Low/no/yes/no | Incident cases of acute respiratory infections (in- and outpatient diagnoses) | DUs had higher incident rate of acute respiratory infections than ESCC but significance level not tested * | |
| Flacco M. E. [50] ^^ 2019, Italy  Yes Yes | Cohort study 48 months | 915 adults | High/no/yes/yes | Changes in self-reported health score and possibly smoking-related disease | DUs: no significant difference in self-reported health score and possible smoking related disease after 4 years than ESCC, but generally worse outcomes in DUs ¤ | |
| Flacco M. E. [29] ^^ 2020, Italy  Yes Yes | Cohort study 72 months | 912 adults | High/no/yes/yes | Changes in self-reported health score and possibly smoking-related disease | DUs had higher odds of possibly smoking related disease after 6 years than ESCC but not significant ¤ | |
| Manzoli L. [35] ^^ 2015, Italy None, first 2 years | Cohort study 12 months | 959 adults with 1-year data | High/no/yes/yes | Self-reported health | DUs: same self-reported health as ESCC ¤ | |
| Manzoli L. [28] ^^ 2017, Italy None, first 2 years | Cohort study 24 months | 932 adults with 2-year data | High/no/yes/yes | Self-reported health | DUs at baseline: same self-rated health as ESCC and significantly higher probability of serious adverse events than ESCC ¤ ** DUs at 24 months follow-up: significant improvement in self-rated health compared with ESCC ## | |
| Riehm K. E. [51] 2019, USA Yes | Nationally representative cohort | 9588 adolescents | Low/yes/yes/no | Sleep-related complaints | DUs: higher risk of sleep-related complaints than ESCC, but not significant * |
| First Author, Year of Publication, Country, Conflict 0f Interest | Method | Participants | Risk of Selection Bias/Weighted Data/Adjusted Analyses/Adjusted for Former Tobacco Consumption | Major Outcomes | Overall Findings Significantly (Higher Risk/Prevalence/Level in ESCC = ## Higher Risk/Prevalence/Level in ESCC, Significance Level Not Tested or Not Significant = # Same Risk/Prevalence/Level in ESCC and DUs = ¤ Higher Risk/Prevalence/Level in DUs, Significance Level Not Tested or Not Significant = * Significantly Higher Risk/Prevalence/Level in DUs = ** | |
|---|---|---|---|---|---|---|
| Harmful substances | Carroll D.M. [53] 2018, USA None | Cross-sectional study | 94 volunteer adults of American Indian descent | High/-/(no)/no | Carcinogen metabolite (NNAL) in urine | DUs same level of carcinogen biomarker as ESCC ¤ |
| Goniewicz M. [15] 2018, USA Yes | Cross-sectional analyses of nationally representative cohort study | 5105 adults | Low/yes/yes/no | 50 biomarkers of toxicity (TSNAs, metals, PAHs, and VOCs) in urine | DUs: significantly higher concentration of most biomarkers of toxicity/carcinogenicity than ESCC ** | |
| Jain R. [54] 2019, USA None | Cross-sectional analyses of population-based survey | 1139 adults | Low/yes/yes/no | Harmful metals (cadmium, lead, and mercury) in blood | DUs same levels of harmful metals in blood as ESCC ¤ | |
| Keith R. [55] 2020, USA None | Cross-sectional analysis of cohort study | 371 volunteer adults | Low/no/yes/no | Volatile organic compound (VOC) metabolites in urine | DUs and ESCC had similar levels of most VOC metabolites, except four, which were significantly higher in ESCC than in DU ¤ ## | |
| Piper M [34] 2018, USA None | Cross-sectional analysis of cohort study | 422 volunteer adults | Low/no/yes/no | Carcinogen metabolite (NNAL) in urine | DUs had significantly lower levels of NNAL than ESCC ## | |
| Prokopowicz A. [52] 2019, Poland Yes | Cross-sectional study | 156 young volunteer adults | High/-/yes/no | Harmful metals cadmium and lead in blood | DUs: levels of harmful metals not significantly different than ESCC ¤ | |
| Prokopowicz A. [56] 2020, Poland Yes | Cross-sectional study | 88 young volunteer adults | High/-/yes/no | 11 toxic metals in urine | Significance level between ESCC and DUs not tested, but DUs had higher values for 8 out of 11 metals in urine * | |
| Rostron B. L. [57] 2019, USA None | Cross-sectional analysis of a nationally representative cohort | 2710 adults | Low/yes/yes/no | Carcinogen and toxin exposure, biomarkers (VOCs, PAHs and TSNAs) in urine and blood | DUs: significantly higher levels of some toxic and carcinogenic biomarkers (NNAL, 1-HOP, HPMA and MHB3) compared to ESCC ** ¤ | |
| Shahab L. [58] 2017, UK Yes | Cross-sectional study | 181 volunteer adults with long-term use | High/-/yes/yes | Carcinogen and toxin exposure, biomarkers (VOCs and TSNAs) in urine and saliva | DUs and ESCC had similar levels of toxic and carcinogenic substances, but DU had significantly higher level of one carcinogenic substance, benzene than ESCC ¤ ** | |
| Smith D. ^ [59] 2020, Poland, UK and USA Yes | Cross-sectional study | 456 volunteer adults with long-term use | High/-/yes/no | Carcinogen and toxin exposure biomarkers (VOCs, TSNAs and minor alkaloids) in urine and saliva | DUs and ESCC had similar levels of toxic and carcinogenic substances, but ESCC had significantly higher level of three TSNAs and acrylonitrile than DUs ¤ ## | |
| Cho J. H. [60] 2016, South Korea None | Nationally representative survey | 35,904 adolescents | Low/no?/yes/no | Self-reported diagnosed with asthma | DUs higher odds of reporting asthma than ESCC but not significant in adjusted analyses * | |
| Chung S. J. [61] 2019, South Korea None | Nationally representative survey | 60,040 adolescents | Low/yes/yes/no | Self-reported diagnosed with asthma or/and allergic rhinitis | DUs had higher odds for current allergic rhinitis but lower odds of current asthma than ESCC, but significance level not tested * # | |
| Hedman L. [12] 2018, Sweden Yes | 2 population-based surveys | 30,272 adults | Low/no/yes/no | Self-reported respiratory symptoms: long-standing cough, sputum production, wheeze | DUs had higher odds of self-reported respiratory symptoms than than ESCC but significance level not tested * | |
| Lee A. [62] 2019, South Korea None | Population-based survey | 58,336 adolescents | Low/yes/yes/no | Self-reported asthma, allergic rhinitis and atopic dermatitis | DUs har lower odds of asthma than ESCC, but comparable odds of allergic rhinitis and atopic dermatitis. Significance level not tested # ¤ | |
| Li D. [63] § 2020, USA Yes | Nationally representative survey | 28,171 adults | Low/yes/yes/no | Self-reported respiratory symptoms and physical health | DUs same odds of respiratory symptoms as ESCC ¤ DUs: same prevalence of poor physical health as ESCC ¤ | |
| Osei A. [64] 2020, USA Yes | Nationally representative survey | 705,159 adults | Low/yes/yes/no | Self-reported diagnosed with COPD/emphysema/chronic bronchitis | DUs had significantly higher odds of COPD/emphysema/chronic bronchitis than ESCC ** | |
| Parekh T. [65] 2020, USA None | Nationally representative survey | 161,965 young adult women | Low/yes/yes/no | Self-reported diagnosed with COPD/emphysema/chronic bronchitis and asthma | DUs had higher odds of asthma and COPD compared than ESCC, but significance level not tested * | |
| Wang J. B. [66] § 2018, USA Yes | Internet population -based survey | 39,747 adults | Low/no/yes/no | Self-reported cardiopulmonary symptoms in the last months General health in the last month (SF-12) | DUs had significantly higher/worse breathing difficulty score than ESCC ** DUs: significantly worse median general health scores than ESCC** DUs: significantly higher prevalence of history of an arrhythmia than ESCC ** | |
| Wills T. A. [67] 2019, USA None | Population-based survey | 8087 adults | Low/yes/yes/no | Self-reported diagnosed with asthma, COPD | DUs and ESCC same odds of asthma ¤ DUs higher odds of COPD than ESCC but not significant * | |
| Wills T.A. [68] 2020, USA None | Nationally representative youth survey | 14,765 adolescents | Low/yes/yes/no | Self-reported asthma diagnosis | DUs had higher odds of asthma than ESCC but not sign. ¤ Significantly higher in a sensitivity analysis tested in a sample with complete data ** | |
| Xie Z. [24] 2020, USA None | Nationally representative youth survey | 887,182 adults | Low/yes/yes/no | Self-reported COPD diagnosis told by doctor | DUs had significantly higher risk of self-reported COPD diagnosis told by doctor than ESCC ** | |
| Cardiovascular and metabolic outcomes | Choi D-W [69] 2018, South Korea None | Nationally representative survey | 8809 adults | Low/yes/yes/yes | Diabetes (HbA1c) | DUs had higher HbA1c levels than ESCC but significance level not tested * |
| Fetterman J. [70] 2020, USA None | Human clinical study with noninvasive vascular function testing | 467 younger adults | High/-/yes/no | Cardiovascular health (augmentation index) | DUs had similar arterial stiffness as ESCC ¤ | |
| Kim C. [21] 2020, South Korea None | Population-based survey | 7505 adult men | Low/yes/yes/no | Cardiovascular risk factors (waist circumference, blood pressure, triglycerides, fasting glucose, HDL-cholesterol, diagnosis of metabolic syndrome) | DUs had significantly higher prevalence odds ratio of cardiovascular risk factors (waist circumference, triglycerides, HDL-cholesterol, blood pressure) and diagnosis of metabolic syndrome than ESCC DUs had similar fasting glucose as ESCC ¤ ** | |
| Kim T. [22] 2020, South Korea None | Nationally representative survey | 14,738 adults | Low/yes/yes/no | Cardiovascular risk factors (waist circumference, blood pressure, triglycerides, fasting glucose, HDL-cholesterol, diagnosis of metabolic syndrome) | DUs had significantly higher odds of abdominal obesity than ESCC ** Other outcomes: no s significant difference but tendency to higher odds in DUs (except blood pressure) # * | |
| Mainous A. [71] 2020, USA None | Nationally representative survey | 4659 adults | Low/yes/yes/no | Biomarker of inflammation and predictor of cardiovascular disease (CRP) | DUs had significantly higher odds of elevated CRP than ESCC ** | |
| Miller C. R. [27] 2021, USA Yes | Population-based survey | 19,147 adults | Low/yes/yes/no | Self-reported diagnosis of hypertension in the last 12 months | DUs had higher odds for hypertension than ESCC, but significance not reached (0.99 for lower 95%CI) * | |
| Orimoloye O. [72] 2019, USA None | Population-based survey | 3415 adults | Low/yes/yes/no | Insulin resistance (measured by HOMA-IR and GTT levels) | DUs had same risk of insulin resistance as ESCC ¤ | |
| Osei A. [26] 2019, USA None | Nationally representative survey | 449,092 adults | Low/yes/yes/no | Self-reported diagnosed with cardiovascular disease (stroke, myocardial infarction or coronary heart disease) | DUs had significantly higher odds of CVD than ESCC ** DUs had significantly higher odds of premature CVD than ESCC ** | |
| Parekh T. [73] 2019, USA None | Nationally representative survey | 161,529 young adults | Low/yes/yes/no | Self-reported stroke | DUs had significantly higher risk of stroke than ESCC ** | |
| Vindhyal M. [74] 2020, USA None | Nationally representative survey | 16,855 adults | Low/yes/yes/no | Self-reported diagnosed with cardiovascular disease | DUs had higher odds of myocardial infarction and stroke than ESCC, but significantly level not tested * | |
| Other | Akinkugbe A. A. [75] 2019, USA None | Population-based survey | 13,650 adolescents | Low/yes/yes/no | Self-reported past-year diagnosis with dental problems | DUs: higher odds of dental problems than ESCC, but significance level not tested * |
| Chen D. TH. [25] 2021, United Kingdom None | 4 population-based surveys | 13,077 adults | Low/yes/yes/no | Self-reported experience of COVID-19 symptoms and diagnosis | DUs had higher odds of covid-19 symptoms and higher odds of confirmed/suspected covid-19 diagnosis than ESCC but significance level not tested * | |
| Dinkeloo E. [76] 2019, USA None | Online survey | 2854 men, soldiers | Low/no/yes/no | Physical activity | DUs: significantly worse fitness than ESCC ** | |
| Gaiha S. M. [77] 2020, USA None | National online survey | 4351 young adults | Low/yes/yes/no | Self-reported COVID-19 symptoms, testing and diagnosis | DUs higher risk of COVID-19 symptoms and diagnosis than ESCC but significance level not tested * | |
| Kim T. [23] 2021, South Korea None | Nationally representative population-based survey | 10,692 adults | Low/yes/yes/no | Levels of serum uric acid and hyperuricemia | DUs significantly higher levels of uric acid and prevalence of hyperuricemia than ESCC ** | |
| Leavens E. [78] 2020, USA None | Interview-survey | 4148 homeless adults | High/no/no/no | Self-reported chronic health conditions | DUs significantly higher rates of asthma ** and cancer compared to ESCC ** | |
| Merianos A. [79] 2021, USA None | School based nationally representative survey | 11,296 high school students | Low/yes/yes/no | Self-reported duration of sleep | DUs were significantly more likely to report insufficient sleep compared with ESCC ** | |
| Ye D. [80] 2020, USA None | Human clinical study | 48 adults | High/-/no/no | Systemic inflammation, oxidative stress, angiogenesis and tissue injury/repair in saliva and gingival crevicular fluid (GCF) | DUs: higher levels of most biomarkers of systemic inflammation than ESCC, but no significant difference * |
Conflict of interest: pharmaceutical industry. Conflict of interest with the tobacco or e-cigarette industry.Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pisinger, C.; Rasmussen, S.K.B. The Health Effects of Real-World Dual Use of Electronic and Conventional Cigarettes versus the Health Effects of Exclusive Smoking of Conventional Cigarettes: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 13687. https://doi.org/10.3390/ijerph192013687
Pisinger C, Rasmussen SKB. The Health Effects of Real-World Dual Use of Electronic and Conventional Cigarettes versus the Health Effects of Exclusive Smoking of Conventional Cigarettes: A Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(20):13687. https://doi.org/10.3390/ijerph192013687
Chicago/Turabian StylePisinger, Charlotta, and Sofie K. Bergman Rasmussen. 2022. "The Health Effects of Real-World Dual Use of Electronic and Conventional Cigarettes versus the Health Effects of Exclusive Smoking of Conventional Cigarettes: A Systematic Review" International Journal of Environmental Research and Public Health 19, no. 20: 13687. https://doi.org/10.3390/ijerph192013687
APA StylePisinger, C., & Rasmussen, S. K. B. (2022). The Health Effects of Real-World Dual Use of Electronic and Conventional Cigarettes versus the Health Effects of Exclusive Smoking of Conventional Cigarettes: A Systematic Review. International Journal of Environmental Research and Public Health, 19(20), 13687. https://doi.org/10.3390/ijerph192013687