
The Development and Preliminary Application of the Chinese Version of the COVID-19 Vaccine Literacy Scale


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Collection
2.3. Statistical Analysis
2.4. Ethics
3. Results
3.1. Item Analysis and Reliability and Validity
3.2. Sociodemographic Characteristics of Participants
3.3. COVID-19 Vaccine Literacy Scores
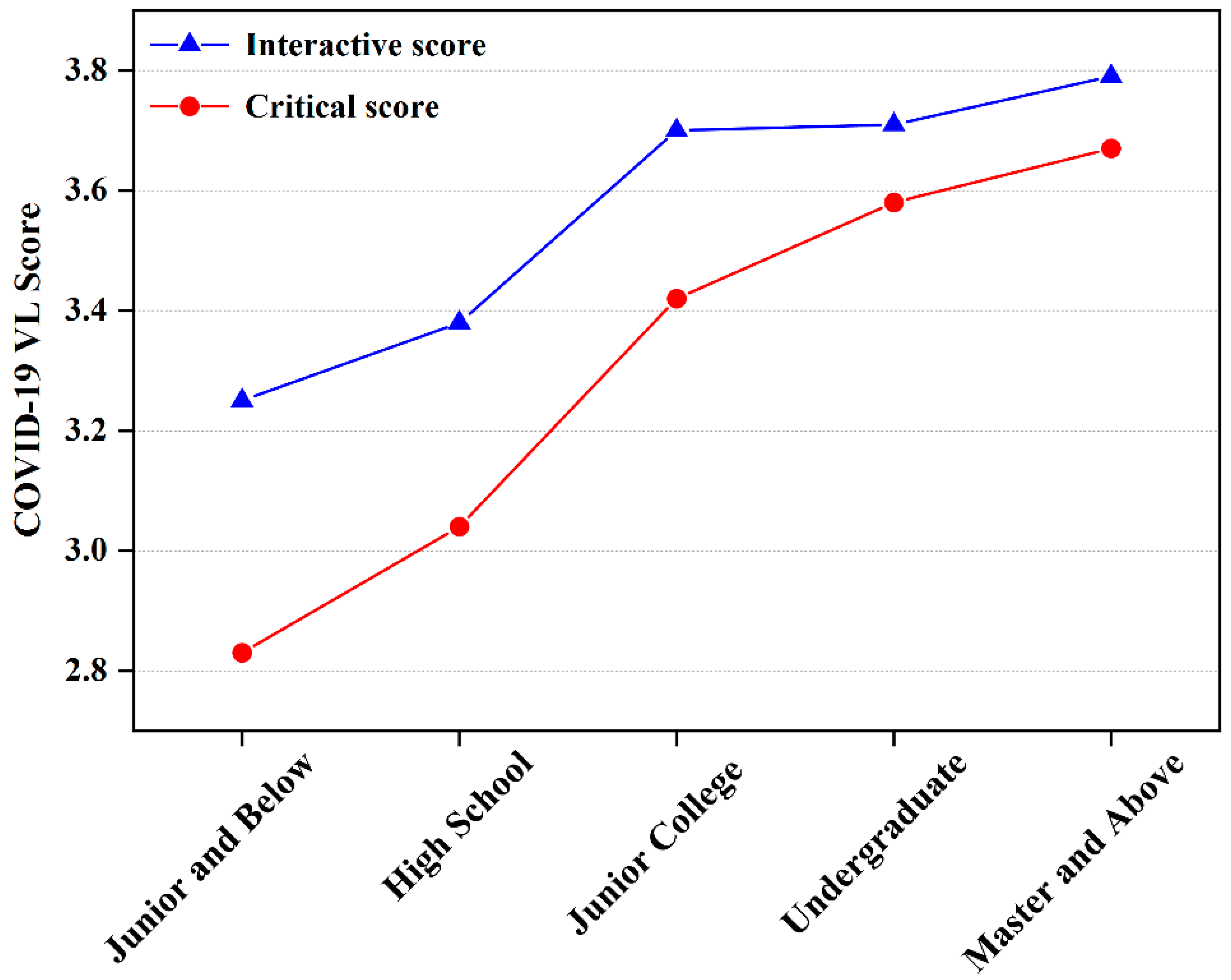
3.4. The Relationship between Sociodemographic Characteristics and COVID-19 VL
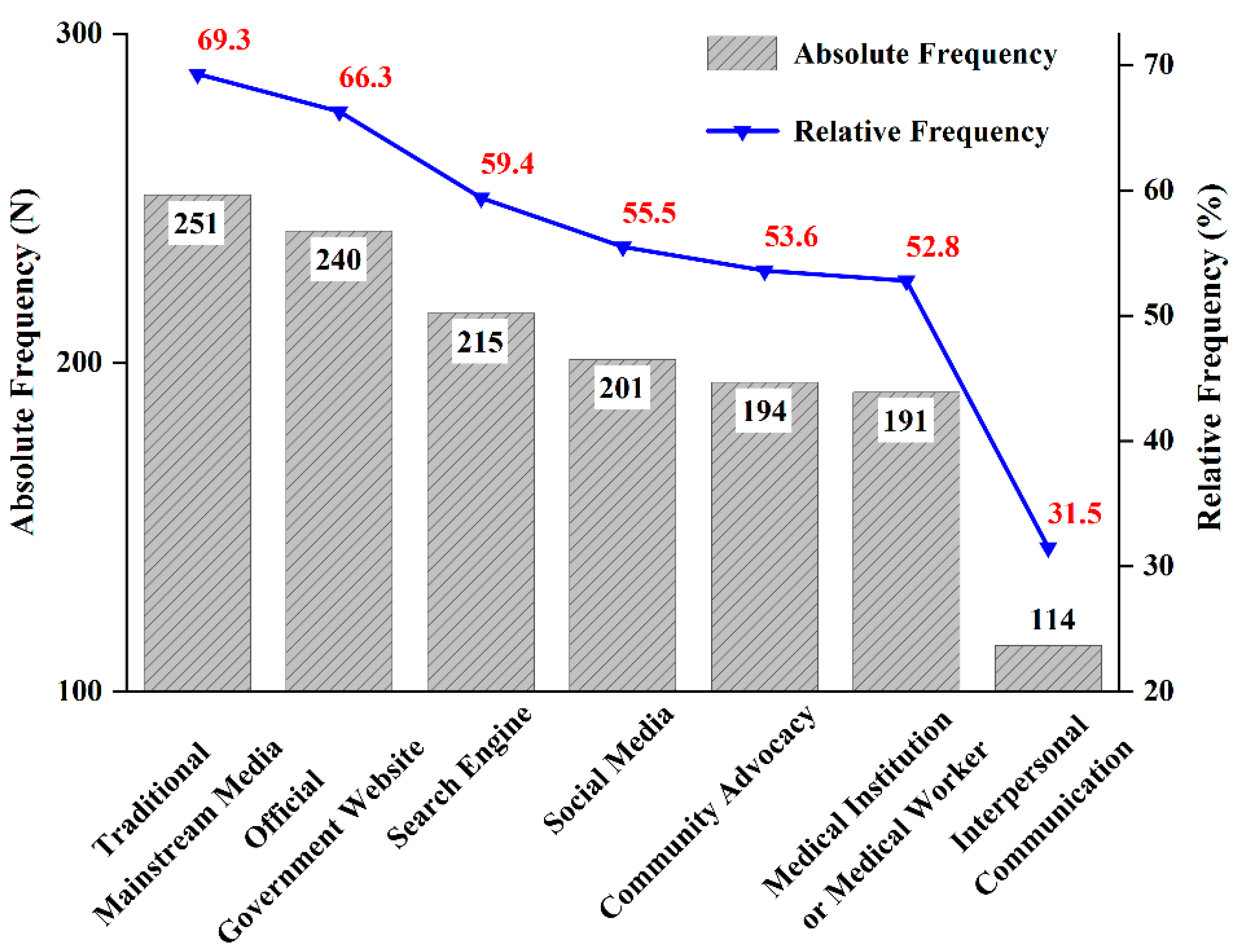
3.5. Source of Information and Vaccination History
4. Discussion
4.1. Main Findings
4.2. Limitations and Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Variable | Items | Measurement (Score) |
|---|---|---|
| VL functional skills | When reading or listening to information about COVID-19 vaccines: | 5 points Likert scale: 5-none; 4-less; 3-once in a while; 2-often; 1-Always |
| 1. Did you find the material as a whole difficult to read or browse? | ||
| 2. Did you find words in the material that you did not know? | ||
| 3. Did you find that the material was difficult to understand? | ||
| 4. Did you need much time to understand them? | ||
| 5. Did you or would you need someone to help you understand them? (e.g., asking others what the material means) | ||
| VL interactive skills | When looking for information about COVID-19 vaccines: | 5 points Likert scale: 5-none; 4-less; 3-once in a while; 2-often; 1-Always |
| 1. Did you know where to get information about the COVID-19 vaccine? | ||
| 2. Have you consulted more than one source of information? | ||
| 3. Did you or would you specify the vaccine information you want? | ||
| 4. Did you find the COVID-19 vaccine information you are looking for? | ||
| 5. Did you understand the information you found about the COVID-19 vaccine? | ||
| 6. Have you had the opportunity to use the COVID-19 vaccine information? | ||
| 7. Did you discuss information about the COVID-19 vaccination with your doctor, family and friends? | ||
| VL critical skills | When looking for information about COVID-19 vaccines: | 5 points Likert scale: 5-none; 4-less; 3-once in a while; 2-often; 1-Always |
| 1. Did you consider whether the COVID-19 vaccine information collected was about your condition? | ||
| 2. Have you considered the credibility of the information sources regarding COVID-19 vac-cines? | ||
| 3. Did you check whether the COVID-19 vaccine information was correct? | ||
| 4. Did you find any useful information to make a decision on whether or not to get COVID-19 vaccinated? |
References
- World Health Organization. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 23 July 2022).
- Ahorsu, D.K.; Imani, V.; Lin, C.Y.; Timpka, T.; Brostrom, A.; Updegraff, J.A.; Arestedt, K.; Griffiths, M.D.; Pakpour, A.H. Associations Between Fear of COVID-19, Mental Health, and Preventive Behaviours Across Pregnant Women and Husbands: An Actor-Partner Interdependence Modelling. Int. J. Ment. Health Addict. 2022, 20, 68–82. [Google Scholar] [CrossRef] [PubMed]
- Ahorsu, D.K.; Lin, C.Y.; Pakpour, A.H. The Association Between Health Status and Insomnia, Mental Health, and Preventive Behaviors: The Mediating Role of Fear of COVID-19. Gerontol. Geriatr. Med. 2020, 6, 9. [Google Scholar] [CrossRef] [PubMed]
- Fazeli, S.; Mohammadi Zeidi, I.; Lin, C.-Y.; Namdar, P.; Griffiths, M.D.; Ahorsu, D.K.; Pakpour, A.H. Depression, anxiety, and stress mediate the associations between internet gaming disorder, insomnia, and quality of life during the COVID-19 outbreak. Addict. Behav. Rep. 2020, 12, 100307. [Google Scholar] [CrossRef] [PubMed]
- Hasannia, E.; Mohammadzadeh, F.; Tavakolizadeh, M.; Davoudian, N.; Bay, M. Assessment of the anxiety level and trust in information resources among iranian health-care workers during the pandemic of coronavirus disease 2019. Asian J. Soc. Health Behav. 2021, 4, 163–168. [Google Scholar] [CrossRef]
- Patel, B.; Khanpara, B.; Mehta, P.; Patel, K.; Marvania, N. Evaluation of perceived social stigma and burnout, among health-care workers working in covid-19 designated hospital of India: A cross-sectional study. Asian J. Soc. Health Behav. 2021, 4, 156–162. [Google Scholar] [CrossRef]
- Rad, M.; Fakhri, A.; Stein, L.; Araban, M. Health-care staff beliefs and coronavirus disease 2019 vaccinations: A cross-sectional study from Iran. Asian J. Soc. Health Behav. 2022, 5, 40–46. [Google Scholar] [CrossRef]
- Zaroushani, V.; Khajehnasiri, F. Errors and preventive measures of health-care systems during COVID-19 pandemic. Asian J. Soc. Health Behav. 2022, 5, 49–50. [Google Scholar] [CrossRef]
- Asante, L.A.; Mills, R.O. Exploring the Socio-Economic Impact of COVID-19 Pandemic in Marketplaces in Urban Ghana. Afr. Spectr. 2020, 55, 170–181. [Google Scholar] [CrossRef]
- Gossling, S.; Scott, D.; Hall, C.M. Pandemics, tourism and global change: A rapid assessment of COVID-19. J. Sustain. Tour. 2021, 29, 1–20. [Google Scholar] [CrossRef]
- Nicola, M.; Alsafi, Z.; Sohrabi, C.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, M.; Agha, R. The socio-economic implications of the coronavirus pandemic (COVID-19): A review. Int. J. Surg. 2020, 78, 185–193. [Google Scholar] [CrossRef]
- Balanza-Martinez, V.; Atienza-Carbonell, B.; Kapczinski, F.; De Boni, R.B. Lifestyle behaviours during the COVID-19-time to connect. Acta Psychiatr. Scand. 2020, 141, 399–400. [Google Scholar] [CrossRef] [PubMed]
- Lippi, G.; Henry, B.M.; Sanchis-Gomar, F. Physical inactivity and cardiovascular disease at the time of coronavirus disease 2019 (COVID-19). Eur. J. Prev. Cardiol. 2020, 27, 906–908. [Google Scholar] [CrossRef] [PubMed]
- Van Lancker, W.; Parolin, Z. COVID-19, school closures, and child poverty: A social crisis in the making. Lancet Public Health 2020, 5, E243–E244. [Google Scholar] [CrossRef]
- Liu, E.; Arledge, S. Individual characteristics and demographics associated with mask wearing during the COVID-19 pandemic in the United States. Asian J. Soc. Health Behav. 2022, 5, 3–9. [Google Scholar] [CrossRef]
- Prasiska, D.; MUHLIS, A.; Megatsari, H. Effectiveness of the emergency public activity restrictions on COVID-19 epidemiological parameter in East Java Province, Indonesia: An ecological study. Asian J. Soc. Health Behav. 2022, 5, 33–39. [Google Scholar] [CrossRef]
- Shirali, G.; Rahimi, Z.; Araban, M.; Mohammadi, M.; Cheraghian, B. Social-distancing compliance among pedestrians in Ahvaz, South-West Iran during the Covid-19 pandemic. Asian J. Soc. Health Behav. 2021, 4, 131–136. [Google Scholar] [CrossRef]
- World Health Organisation. Available online: https://covid19.who.int/ (accessed on 22 July 2022).
- National Health Commission of the People’s Republic of China. Available online: http://www.nhc.gov.cn/ (accessed on 22 July 2022).
- Farooq, F.; Rathore, F.A. COVID-19 Vaccination and the Challenge of Infodem’c and Disinformation. J. Korean Med. Sci. 2021, 36, 4. [Google Scholar] [CrossRef]
- Hatcher, W. President Trump and health care: A content analysis of misleading statements. J. Public Health 2020, 42, E482–E486. [Google Scholar] [CrossRef]
- Caravaggio, F.; Porco, N.; Kim, J.; Fervaha, G.; Graff-Guerrero, A.; Gerretsen, P. Anti-vaccination attitudes are associated with less analytical and more intuitive reasoning. Psychol. Health Med. 2021, 1–13. [Google Scholar] [CrossRef]
- Mohammed, M.; Sha’aban, A.; Jatau, A.I.; Yunusa, I.; Isa, A.M.; Wada, A.S.; Obamiro, K.; Zainal, H.; Ibrahim, B. Assessment of COVID-19 Information Overload Among the General Public. J. Racial Ethn. Health Disparities 2022, 9, 184–192. [Google Scholar] [CrossRef]
- Bin Naeem, S.; Bhatti, R. The Covid-19 ‘infodemic’: A new front for information professionals. Heatlth Info. Libr. J. 2020, 37, 233–239. [Google Scholar] [CrossRef] [PubMed]
- Lazcano-Ponce, E.; Alpuche-Aranda, C. Public health literacy in the face of the COVID-19 pandemic emergency. Salud Publica Mex. 2020, 62, 331–340. [Google Scholar] [CrossRef]
- Jiang, F.; Zhao, Y.; Bai, J.; Yang, X.; Zhang, J.; Lin, D.; Li, X. Perceived health literacy and COVID-19 vaccine acceptance among Chinese college students: A mediation analysis. PLoS ONE 2022, 17, e0273285. [Google Scholar] [CrossRef]
- Ratzan, S.C. Vaccine Literacy: A New Shot for Advancing Health. J. Health Commun. 2011, 16, 227–229. [Google Scholar] [CrossRef] [PubMed]
- Biasio, L.R.; Giambi, C.; Fadda, G.; Lorini, C.; Bonaccorsi, G.; D’Ancona, F. Validation of an Italian tool to assess vaccine literacy in adulthood vaccination: A pilot study. Ann. Ig. Med. Prev. Comunita 2020, 32, 205–222. [Google Scholar] [CrossRef]
- Biasio, L.R.; Bonaccorsi, G.; Lorini, C.; Pecorelli, S. Assessing COVID-19 vaccine literacy: A preliminary online survey. Hum. Vaccines Immunother. 2021, 17, 1304–1312. [Google Scholar] [CrossRef] [PubMed]
- Biasio, L.R.; Bonaccorsi, G.; Lorini, C.; Mazzini, D.; Pecorelli, S. Italian Adults’ Likelihood of Getting COVID-19 Vaccine: A Second Online Survey. Vaccines 2021, 9, 268. [Google Scholar] [CrossRef]
- Ratzan, S.C.; Parker, R.M. Vaccine Literacy-helping Everyone Decide to Accept Vaccination. J. Health Commun. 2020, 25, 750–752. [Google Scholar] [CrossRef]
- Ishikawa, H.; Takeuchi, T.; Yano, E. Measuring functional, communicative, and critical health literacy among diabetic patients. Diabetes Care 2008, 31, 874–879. [Google Scholar] [CrossRef]
- Nutbeam, D. Health literacy as a public health goal: A challenge for contemporary health education and communication strategies into the 21st century. Health Promot. Int. 2000, 15, 259–267. [Google Scholar] [CrossRef]
- Maneesriwongul, W.; Butsing, N.; Visudtibhan, P.J.; Leelacharas, S.; Kittipimpanon, K. Translation and Psychometric Testing of the Thai COVID-19 Vaccine Literacy Scale. Pac. Rim Int. J. Nurs. Res. 2022, 26, 175–186. [Google Scholar]
- Durmus, A.; Akbolat, M.; Amarat, M. Turkish validity and reliability of COVID-19 Vaccine Literacy Scale. Cukurova Med. J. 2021, 46, 732–741. [Google Scholar] [CrossRef]
- Correa-Rodriguez, M.; Rueda-Medina, B.; Callejas-Rubio, J.L.; Rios-Fernandez, R.; de la Hera-Fernandez, J.; Ortego-Centeno, N. COVID-19 vaccine literacy in patients with systemic autoimmune diseases. Curr. Psychol. 2022, 16. [Google Scholar] [CrossRef] [PubMed]
- Meng Fanli, S.F.; Ye, J.; Wu, X.; Su, Y.; Wang, D. Human papillomavirus and vaccine awareness and vaccination willingness among female college students in Hangzhou. Chin. J. Sch. Health 2020, 41, 1737–1741. [Google Scholar] [CrossRef]
- Chenhui, S. A Study on the Influence of Vaccine Safety Events on Parents’ Willingness to Vaccinate Their Children from the Perspective of Communication—Example of the Changchun Changsheng Vaccine Event. Ph.D. Dissertation, Zhejiang University, Hangzhou, China, 2020. [Google Scholar] [CrossRef]
- Nutbeam, D. The evolving concept of health literacy. Soc. Sci. Med. 2008, 67, 2072–2078. [Google Scholar] [CrossRef] [PubMed]
- Sousa, V.D.; Rojjanasrirat, W. Translation, adaptation and validation of instruments or scales for use in cross-cultural health care research: A clear and user-friendly guideline. J. Eval. Clin. Pract. 2011, 17, 268–274. [Google Scholar] [CrossRef]
- Gendler, Y.; Ofri, L. Investigating the Influence of Vaccine Literacy, Vaccine Perception and Vaccine Hesitancy on Israeli Parents’ Acceptance of the COVID-19 Vaccine for Their Children: A Cross-Sectional Study. Vaccines 2021, 9, 1391. [Google Scholar] [CrossRef]
- Gusar, I.; Konjevoda, S.; Babic, G.; Hnatesen, D.; Cebohin, M.; Orlandini, R.; Dzelalija, B. Pre-Vaccination COVID-19 Vaccine Literacy in a Croatian Adult Population: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 7073. [Google Scholar] [CrossRef]
- Nunally, J.C. Psychometric Theory, 2nd ed.; McGraw-Hill: New York, NY, USA, 1978. [Google Scholar]
- Engelbrecht, M.C.; Kigozi, N.G.; Heunis, J.C. Factors Associated with Limited Vaccine Literacy: Lessons Learnt from COVID-19. Vaccines 2022, 10, 865. [Google Scholar] [CrossRef] [PubMed]
- Clouston, S.A.P.; Manganello, J.A.; Richards, M. A life course approach to health literacy: The role of gender, educational attainment and lifetime cognitive capability. Age Ageing 2017, 46, 493–499. [Google Scholar] [CrossRef]
- Joveini, H.; Rohban, A.; Askarian, P.; Maheri, M.; Hashemian, M. Health literacy and its associated demographic factors in 18-65-year-old, literate adults in Bardaskan, Iran. J. Educ. Health Promot. 2019, 8, 8. [Google Scholar] [CrossRef]
- Oliffe, J.L.; Rossnagel, E.; Kelly, M.T.; Bottorff, J.L.; Seaton, C.; Darroch, F. Men’s health literacy: A review and recommendations. Health Promot. Int. 2020, 35, 1037–1051. [Google Scholar] [CrossRef] [PubMed]
- Sorensen, K.; Van den Broucke, S.; Fullam, J.; Doyle, G.; Pelikan, J.; Slonska, Z.; Brand, H.; Literacy, H.-E.C.H. Health literacy and public health: A systematic review and integration of definitions and models. BMC Public Health 2012, 12, 13. [Google Scholar] [CrossRef] [PubMed]
- Espanha, R.; Avila, P. Health Literacy Survey Portugal: A Contribution for the Knowledge on Health and Communications. In Proceedings of the International Conference on ENTERprise Information Systems/International Conference on Project MANagement/International Conference on Health and Social Care Information Systems and Technologies (CENTERIS/ProjMAN/HCist), Porto, Portugal, 5–7 October 2016; pp. 1033–1041. [Google Scholar]
- Biasio, L.R.; Lorini, C.; Abbattista, G.; Bozzola, E.; De Castro, P.; Della Seta, M.; Villani, A.; Bonaccorsi, G. Assessment of health literacy skills in family doctors’ patients by two brief, self-administered Italian measures. Ann. Ist. Super. Sanita 2018, 54, 214–222. [Google Scholar] [CrossRef] [PubMed]
- Bertoncello, C.; Ferro, A.; Fonzo, M.; Zanovello, S.; Napoletano, G.; Russo, F.; Baldo, V.; Cocchio, S. Socioeconomic Determinants in Vaccine Hesitancy and Vaccine Refusal in Italy. Vaccines 2020, 8, 276. [Google Scholar] [CrossRef]
- van der Heide, I.; Wang, J.; Droomers, M.; Spreeuwenberg, P.; Rademakers, J.; Uiters, E. The Relationship Between Health, Education, and Health Literacy: Results From the Dutch Adult Literacy and Life Skills Survey. J. Health Commun. 2013, 18, 172–184. [Google Scholar] [CrossRef] [PubMed]
- Vanderpool, R.C.; Gaysynsky, A.; Chou, W.Y.S. Using a Global Pandemic as a Teachable Moment to Promote Vaccine Literacy and Build Resilience to Misinformation. Am. J. Public Health 2020, 110, S284–S285. [Google Scholar] [CrossRef]
- Chou, W.Y.S.; Oh, A.; Klein, W.M.P. Addressing Health-Related Misinformation on Social Media. JAMA-J. Am. Med. Assoc. 2018, 320, 2417–2418. [Google Scholar] [CrossRef]
- Di Mauro, A.; Di Mauro, F.; De Nitto, S.; Rizzo, L.; Greco, C.; Stefanizzi, P.; Tafuri, S.; Baldassarre, M.E.; Laforgia, N. Social Media Interventions Strengthened COVID-19 Immunization Campaign. Front. Pediatr. 2022, 10, 869893. [Google Scholar] [CrossRef]
- Walsh, S.; Thomas, D.R.; Mason, B.W.; Evans, M.R. The impact of the media on the decision of parents in South Wales to accept measles-mumps-rubella (MMR) immunization. Epidemiol. Infect. 2015, 143, 550–560. [Google Scholar] [CrossRef]
- Restivo, V.; Napoli, G.; Marsala, M.G.L.; Bonanno, V.; Sciuto, V.; Amodio, E.; Calamusa, G.; Vitale, F.; Firenze, A. Factors associated with poor adherence to MMR vaccination in parents who follow vaccination schedule. Hum. Vaccines Immunother. 2015, 11, 140–145. [Google Scholar] [CrossRef]
- Alvi, S. Marrying Digital and Analog with Generation Z: Confronting the Moral Panic of Digital Learning in Late Modern Society. In Proceedings of the Universal Design and Higher Education in Transformation Congress (UDHEIT), Dublin, Ireland, 30 October–2 November 2018; pp. 444–453. [Google Scholar]
- Kennedy, A.; Glasser, J.; Covello, V.; Gust, D. Development of Vaccine Risk Communication Messages Using Risk Comparisons and Mathematical Modeling. J. Health Commun. 2008, 13, 793–807. [Google Scholar] [CrossRef]
- Wangdahl, J.M.; Martensson, L.I. Measuring health literacy—The Swedish Functional Health Literacy scale. Scand. J. Caring Sci. 2015, 29, 165–172. [Google Scholar] [CrossRef]


| Variable | Item | Factor Loading | CR | AVE | Cronbach’s α | Split-Half Reliability |
|---|---|---|---|---|---|---|
| Functional vaccine literacy | FVL1 1 | 0.714 | 0.841 | 0.571 | 0.838 | 0.818 |
| FVL2 2 | 0.848 | |||||
| FVL3 3 | 0.759 | |||||
| FVL4 4 | 0.693 | |||||
| Interactive vaccine literacy | IVL1 5 | 0.675 | 0.894 | 0.551 | 0.891 | 0.844 |
| IVL2 6 | 0.716 | |||||
| IVL3 7 | 0.776 | |||||
| IVL4 8 | 0.830 | |||||
| IVL5 9 | 0.841 | |||||
| IVL6 10 | 0.740 | |||||
| IVL7 11 | 0.584 | |||||
| Critical vaccine literacy | CVL1 12 | 0.757 | 0.858 | 0.601 | 0.857 | 0.844 |
| CVL2 13 | 0.804 | |||||
| CVL3 14 | 0.756 | |||||
| CVL4 15 | 0.783 |
| Variable | Category | Number (n) | Percentage (%) |
|---|---|---|---|
| Gender | Male | 167 | 46.1 |
| Female | 195 | 53.9 | |
| Age | 18–25 | 109 | 30.1 |
| 26–35 | 80 | 22.1 | |
| 36–45 | 121 | 33.4 | |
| 46–55 | 45 | 12.4 | |
| >55 | 7 | 1.9 | |
| Education | Junior and below | 67 | 18.5 |
| High school | 98 | 27.1 | |
| Junior college | 55 | 15.2 | |
| Undergraduate | 93 | 25.7 | |
| Master and above | 49 | 13.5 | |
| Permanent residence | Urban | 252 | 69.6 |
| Rural | 110 | 30.4 | |
| Marital status | Single | 128 | 35.4 |
| Married | 224 | 61.9 | |
| Widowed or divorced | 10 | 2.8 | |
| Occupation | Civil Servants | 9 | 2.5 |
| Personnel of public institutions | 44 | 12.2 | |
| Employees of enterprises | 65 | 18.0 | |
| Self-employed/Freelance | 98 | 27.1 | |
| Farmers | 45 | 12.4 | |
| Students | 67 | 18.5 | |
| Retired | 5 | 1.4 | |
| Others | 29 | 8.0 | |
| Average monthly income (RMB) 1 | 0–2999 | 173 | 47.8 |
| 3000–5999 | 136 | 37.6 | |
| 6000–8999 | 30 | 8.3 | |
| 9000–11,999 | 14 | 3.9 | |
| ≥12,000 | 9 | 2.5 | |
| COVID-19 vaccination status | The first injection completed (Booster injection uncompleted) | 7 | 1.9 |
| The first and second injections completed (booster injections uncompleted) | 35 | 9.7 | |
| Booster injections completed 2 | 112 | 30.9 | |
| Full vaccination has been completed 3 | 204 | 56.4 | |
| Not yet vaccinated against COVID-19 | 4 | 1.1 |
| Variable | Item | N (%) | M (SD) | Min | Max | ||||
|---|---|---|---|---|---|---|---|---|---|
| Never | Rarely | Sometimes | Often | Always | |||||
| Functional vaccine literacy | FVL2 | 186 (51.4) | 91 (25.1) | 68 (18.8) | 14 (3.9) | 3 (0.8) | 4.22 (0.94) | 1 | 5 |
| FVL3 | 231 (63.8) | 74 (20.4) | 42 (11.6) | 11 (3.0) | 4 (1.1) | 4.43 (0.89) | 1 | 5 | |
| FVL4 | 228 (63.0) | 75 (20.7) | 44 (12.2) | 7 (1.9) | 8 (2.2) | 4.40 (0.93) | 1 | 5 | |
| FVL5 | 265 (73.2) | 53 (14.6) | 35 (9.7) | 5 (1.4) | 4 (1.1) | 4.57 (0.81) | 1 | 5 | |
| Interactive vaccine literacy | IVL1 | 52 (14.4) | 34 (9.4) | 54 (14.9) | 120 (33.1) | 102 (28.2) | 3.51 (1.37) | 1 | 5 |
| IVL2 | 28 (7.7) | 39 (10.8) | 63 (17.4) | 146 (40.3) | 86 (23.8) | 3.62 (1.18) | 1 | 5 | |
| IVL3 | 44 (12.2) | 44 (12.2) | 66 (18.2) | 122 (33.7) | 86 (23.8) | 3.45 (1.30) | 1 | 5 | |
| IVL4 | 25 (6.9) | 37 (10.2) | 56 (15.5) | 142 (39.2) | 102 (28.2) | 3.72 (1.18) | 1 | 5 | |
| IVL5 | 23 (6.4) | 26 (7.2) | 72 (19.9) | 140 (38.7) | 101 (27.9) | 3.75 (1.13) | 1 | 5 | |
| IVL6 | 27 (7.5) | 52 (7.5) | 84 (23.2) | 127 (35.1) | 72 (19.9) | 3.46 (1.18) | 1 | 5 | |
| IVL7 | 30 (8.3) | 56 (15.5) | 102 (28.2) | 116 (32.0) | 58 (16.0) | 3.32 (1.16) | 1 | 5 | |
| Critical vaccine literacy | CVL1 | 42 (11.6) | 61 (16.9) | 91 (25.1) | 97 (26.8) | 71 (19.6) | 3.26 (1.27) | 1 | 5 |
| CVL2 | 55 (15.2) | 49 (13.5) | 91 (25.1) | 90 (24.9) | 77 (21.3) | 3.23 (1.34) | 1 | 5 | |
| CVL3 | 56 (15.5) | 47 (13.0) | 89 (24.6) | 102 (28.2) | 68 (18.8) | 3.22 (1.32) | 1 | 5 | |
| CVL4 | 47 (13.0) | 38 (10.5) | 77 (21.3) | 117 (32.3) | 83 (22.9) | 3.42 (1.30) | 1 | 5 | |
| Variable | Category | VL Functional Score | VL Interactive Score | VL Critical Score | VL Score | ||||
|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | p Value | Mean ± SD | p Value | Mean ± SD | p Value | Mean ± SD | p Value | ||
| Gender | Male | 4.25 ± 0.80 | <0.001 1 | 3.38 ± 0.97 | 0.002 | 3.09 ± 1.08 | 0.002 | 3.53 ± 0.74 | <0.001 |
| Female | 4.55 ± 0.65 | 3.69 ± 0.90 | 3.45 ± 1.08 | 3.85 ± 0.67 | |||||
| Age | 18–25 | 4.28 ± 0.82 | 0.049 | 3.64 ± 0.93 | 0.241 | 3.44 ± 0.92 | 0.164 | 3.76 ± 0.67 | 0.324 |
| 26–35 | 4.45 ± 0.64 | 3.45 ± 0.93 | 3.37 ± 1.06 | 3.70 ± 0.69 | |||||
| 36–45 | 4.42 ± 0.75 | 3.44 ± 0.98 | 3.09 ± 1.21 | 3.61 ± 0.77 | |||||
| 46–55 | 4.58 ± 0.63 | 3.71 ± 0.92 | 3.19 ± 1.18 | 3.80 ± 0.78 | |||||
| >55 | 4.79 ± 0.22 | 3.78 ± 0.79 | 3.64 ± 1.11 | 4.01 ± 0.61 | |||||
| Education | Junior and below | 4.32 ± 0.82 | 0.093 | 3.25 ± 0.96 | 0.001 | 2.83 ± 1.13 | <0.001 | 3.42 ± 0.78 | <0.001 |
| High school | 4.52 ± 0.68 | 3.38 ± 0.93 | 3.04 ± 1.04 | 3.59 ± 0.65 | |||||
| Junior college | 4.34 ± 0.81 | 3.70 ± 0.95 | 3.42 ± 1.15 | 3.80 ± 0.77 | |||||
| Undergraduate | 4.33 ± 0.73 | 3.71 ± 0.94 | 3.58 ± 0.97 | 3.84 ± 0.70 | |||||
| Master and above | 4.53 ± 0.58 | 3.79 ± 0.84 | 3.67 ± 1.02 | 3.95 ± 0.63 | |||||
| Permanent residence | Rural | 4.48 ± 0.73 | 0.065 | 3.44 ± 0.99 | 0.184 | 3.05 ± 1.13 | 0.010 | 3.62 ± 0.76 | 0.172 |
| Urban | 4.37 ± 0.73 | 3.59 ± 0.92 | 3.38 ± 1.07 | 3.74 ± 0.70 | |||||
| Marital status | Single | 4.27 ± 0.80 | 0.005 | 3.65 ± 0.91 | 0.259 | 3.43 ± 0.93 | 0.250 | 3.76 ± 0.66 | 0.730 |
| Married | 4.49 ± 0.66 | 3.49 ± 0.96 | 3.21 ± 1.16 | 3.68 ± 0.74 | |||||
| Widowed or divorced | 4.30 ± 1.17 | 3.47 ± 1.06 | 3.00 ± 1.40 | 3.57 ± 1.00 | |||||
| Occupation | Civil Servants | 3.94 ± 0.91 | 0.012 | 4.10 ± 0.92 | 0.051 | 4.06 ± 1.11 | 0.007 | 4.04 ± 0.90 | 0.057 |
| Personnel of public institutions | 4.65 ± 0.57 | 3.64 ± 0.99 | 3.50 ± 1.13 | 3.87 ± 0.72 | |||||
| Employees of enterprises | 4.35 ± 0.73 | 3.58 ± 0.88 | 3.48 ± 0.94 | 3.76 ± 0.66 | |||||
| Self-employed/Freelance | 4.45 ± 0.71 | 3.33 ± 0.98 | 3.02 ± 1.14 | 3.54 ± 0.74 | |||||
| Farmers | 4.43 ± 0.78 | 3.38 ± 1.00 | 2.89 ± 1.17 | 3.53 ± 0.81 | |||||
| Students | 4.22 ± 0.84 | 3.68 ± 0.87 | 3.49 ± 0.86 | 3.78 ± 0.62 | |||||
| Retired | 4.65 ± 0.29 | 3.80 ± 0.82 | 3.15 ± 1.10 | 3.85 ± 0.60 | |||||
| Others | 4.52 ± 0.56 | 3.78 ± 0.91 | 3.34 ± 1.26 | 3.86 ± 0.73 | |||||
| Average monthly income (RMB) | 0–2999 | 4.43 ± 0.75 | 0.852 | 3.59 ± 0.91 | 0.041 | 3.26 ± 1.02 | 0.095 | 3.73 ± 0.68 | 0.108 |
| 3000–5999 | 4.41 ± 0.70 | 3.41 ± 1.00 | 3.19 ± 1.18 | 3.62 ± 0.77 | |||||
| 6000–8999 | 4.36 ± 0.72 | 3.81 ± 0.82 | 3.78 ± 0.92 | 3.95 ± 0.65 | |||||
| 9000–11,999 | 4.41 ± 0.68 | 3.98 ± 0.86 | 3.30 ± 1.31 | 3.91 ± 0.77 | |||||
| ≥12,000 | 4.03 ± 1.13 | 3.21 ± 1.03 | 3.36 ± 1.18 | 3.47 ± 0.76 | |||||
| Whether to get the COVID-19 vaccine | Yes | 4.41 ± 0.73 | 0.488 | 3.54 ± 0.95 | 0.799 | 3.28 ± 1.10 | 0.473 | 3.70 ± 0.72 | 0.836 |
| No | 4.19 ± 0.80 | 3.79 ± 0.72 | 3.69 ± 0.63 | 3.87 ± 0.64 | |||||
| COVID-19 vaccination status | The first injection completed (Booster injection uncompleted) | 4.46 ± 0.81 | 0.440 | 3.14 ± 0.87 | 0.194 | 2.93 ± 1.03 | 0.108 | 3.44 ± 0.66 | 0.139 |
| The first and second injections completed (Booster injections uncompleted) | 4.28 ± 0.82 | 3.34 ± 1.05 | 3.09 ± 1.25 | 3.53 ± 0.84 | |||||
| Booster injections completed 2 | 4.42 ± 0.65 | 3.67 ± 0.93 | 3.49 ± 1.00 | 3.82 ± 0.69 | |||||
| Full vaccination has been completed 3 | 4.43 ± 0.76 | 3.52 ± 0.94 | 3.21 ± 1.11 | 3.68 ± 0.72 | |||||
| Category | N | VL Functional Score | VL Interactive Score | VL Critical Score | VL Score | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | p Value | Mean ± SD | p Value | Mean ± SD | p Value | Mean ± SD | p Value | |||
| Traditional mainstream media | Yes | 251 | 4.46 ± 0.68 | 0.028 1 | 3.60 ± 0.95 | 0.035 | 3.33 ± 1.05 | 0.274 | 3.76 ± 0.69 | 0.034 |
| No | 111 | 4.28 ± 0.83 | 3.41 ± 0.93 | 3.18 ± 1.19 | 3.58 ± 0.78 | |||||
| Official government websites | Yes | 240 | 4.49 ± 0.69 | 0.003 | 3.69 ± 0.92 | <0.001 | 3.39 ± 1.07 | 0.014 | 3.82 ± 0.69 | <0.001 |
| No | 122 | 4.25 ± 0.79 | 3.25 ± 0.93 | 3.08 ± 1.11 | 3.47 ± 0.73 | |||||
| Community advocacy | Yes | 194 | 4.48 ± 0.70 | 0.025 | 3.73 ± 0.90 | <0.001 | 3.41 ± 1.11 | 0.013 | 3.84 ± 0.70 | <0.001 |
| No | 168 | 4.32 ± 0.76 | 3.33 ± 0.96 | 3.13 ± 1.07 | 3.54 ± 0.72 | |||||
| Interpersonal communication | Yes | 114 | 4.39 ± 0.80 | 0.601 | 3.73 ± 0.96 | 0.006 | 3.41 ± 1.13 | 0.069 | 3.82 ± 0.74 | 0.033 |
| No | 248 | 4.42 ± 0.70 | 3.46 ± 0.93 | 3.22 ± 1.08 | 3.65 ± 0.71 | |||||
| Medical Institution or Medical Worker | Yes | 191 | 4.45 ± 0.70 | 0.281 | 3.69 ± 0.90 | 0.001 | 3.38 ± 1.05 | 0.060 | 3.81 ± 0.68 | 0.004 |
| No | 171 | 4.36 ± 0.77 | 3.38 ± 0.97 | 3.17 ± 1.13 | 3.59 ± 0.75 | |||||
| Social media | Yes | 201 | 4.45 ± 0.70 | 0.268 | 3.72 ± 0.91 | <0.001 | 3.42 ± 1.06 | 0.004 | 3.84 ± 0.71 | <0.001 |
| No | 161 | 4.36 ± 0.77 | 3.32 ± 0.94 | 3.11 ± 1.12 | 3.54 ± 0.71 | |||||
| Search engine | Yes | 215 | 4.43 ± 0.73 | 0.273 | 3.65 ± 0.91 | 0.019 | 3.34 ± 1.07 | 0.234 | 3.77 ± 0.71 | 0.047 |
| No | 147 | 4.38 ± 0.74 | 3.40 ± 0.98 | 3.20 ± 1.12 | 3.61 ± 0.74 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, Y.; Guo, Y.; Wu, X.; Hu, Q.; Hu, D. The Development and Preliminary Application of the Chinese Version of the COVID-19 Vaccine Literacy Scale. Int. J. Environ. Res. Public Health 2022, 19, 13601. https://doi.org/10.3390/ijerph192013601
Li Y, Guo Y, Wu X, Hu Q, Hu D. The Development and Preliminary Application of the Chinese Version of the COVID-19 Vaccine Literacy Scale. International Journal of Environmental Research and Public Health. 2022; 19(20):13601. https://doi.org/10.3390/ijerph192013601
Chicago/Turabian StyleLi, Yihui, Yi Guo, Xusheng Wu, Qingyuan Hu, and Dehua Hu. 2022. "The Development and Preliminary Application of the Chinese Version of the COVID-19 Vaccine Literacy Scale" International Journal of Environmental Research and Public Health 19, no. 20: 13601. https://doi.org/10.3390/ijerph192013601
APA StyleLi, Y., Guo, Y., Wu, X., Hu, Q., & Hu, D. (2022). The Development and Preliminary Application of the Chinese Version of the COVID-19 Vaccine Literacy Scale. International Journal of Environmental Research and Public Health, 19(20), 13601. https://doi.org/10.3390/ijerph192013601