


When a Pandemic Strikes: Resilience of Swedish Academics in the Face of Coronavirus




Abstract
1. Introduction
1.1. Previous Research
1.2. Theoretical Framework: Personal and Social/Collective Resilience
In the context of exposure to significant adversity, whether psychological, environmental, or both, resilience is both the capacity of individuals to navigate their way to health-sustaining resources, including opportunities to experience feelings of well-being, and a condition of the individual’s family, community and culture to provide these health resources and experiences in culturally meaningful ways. (p. 225)
1.3. Aims
- Q1. How strongly do academics in Sweden rate their level of personal/individual and social/collective resilience (disaggregated by gender, age group, residence, and employment status)?
- Q2. How strongly do academics in Sweden rate their general health (disaggregated by gender, age group, residence, and employment status)?
- Q3. Is there a relationship between general health, personal/individual resilience, social/collective resilience, and meaning-making coping methods among academics in Sweden?
- Q4. What resilience factors contribute most strongly to meaning-making among Swedish academics, and how can this be culturally interpreted?
2. Materials and Methods
2.1. Sampling
2.2. Procedure
2.3. Measures
2.4. Data Analysis Methods
3. Results
3.1. Personal/Individual Resilience
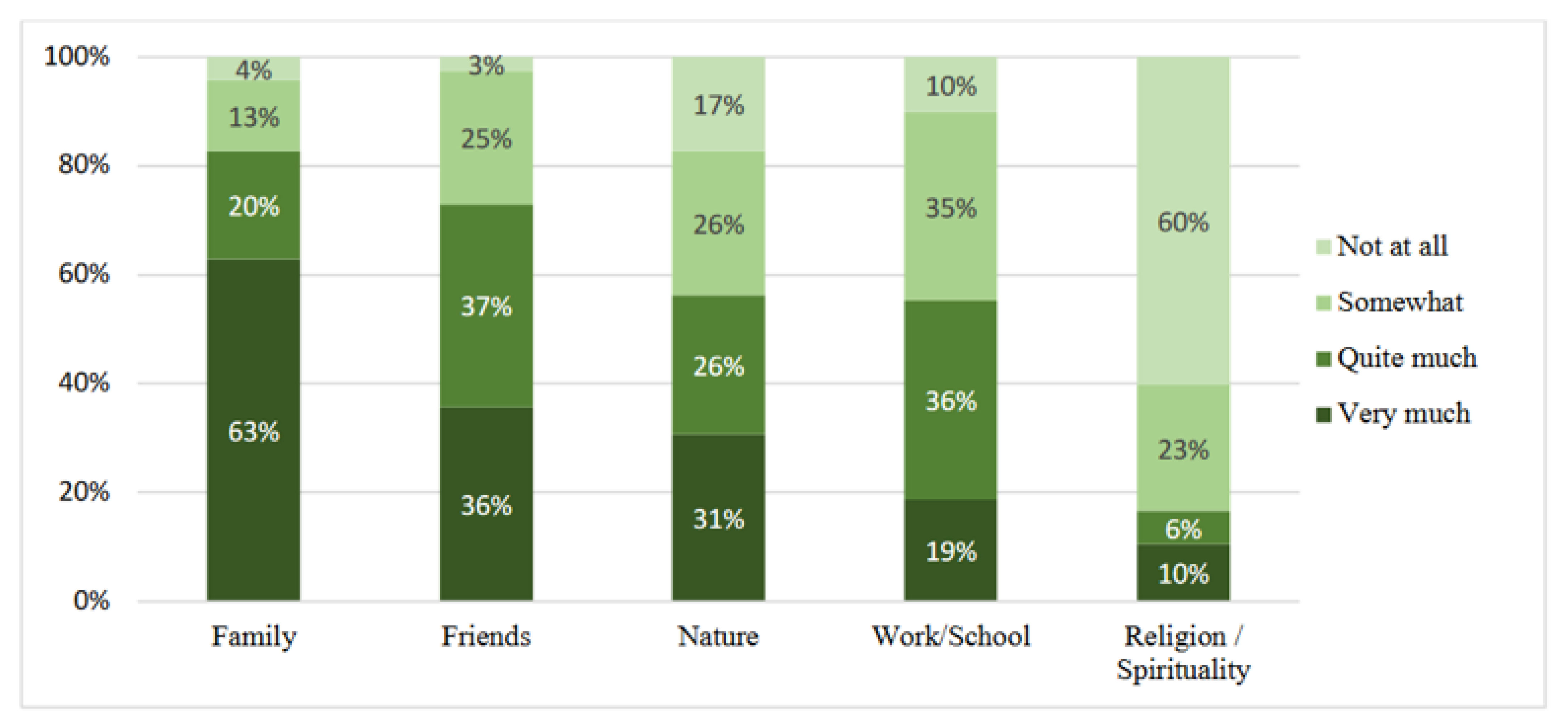
3.2. Social and Collective Resilience
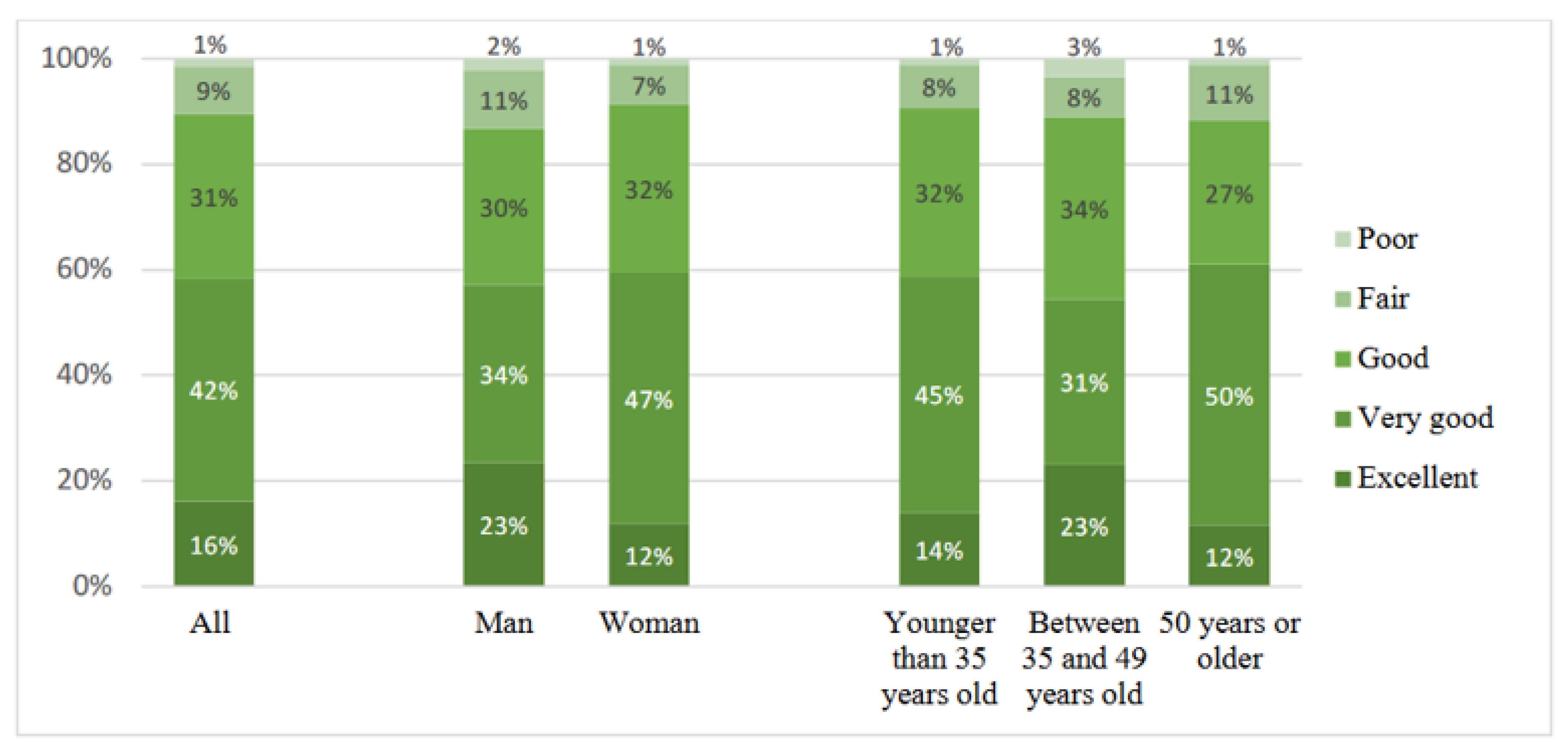
3.3. General Health
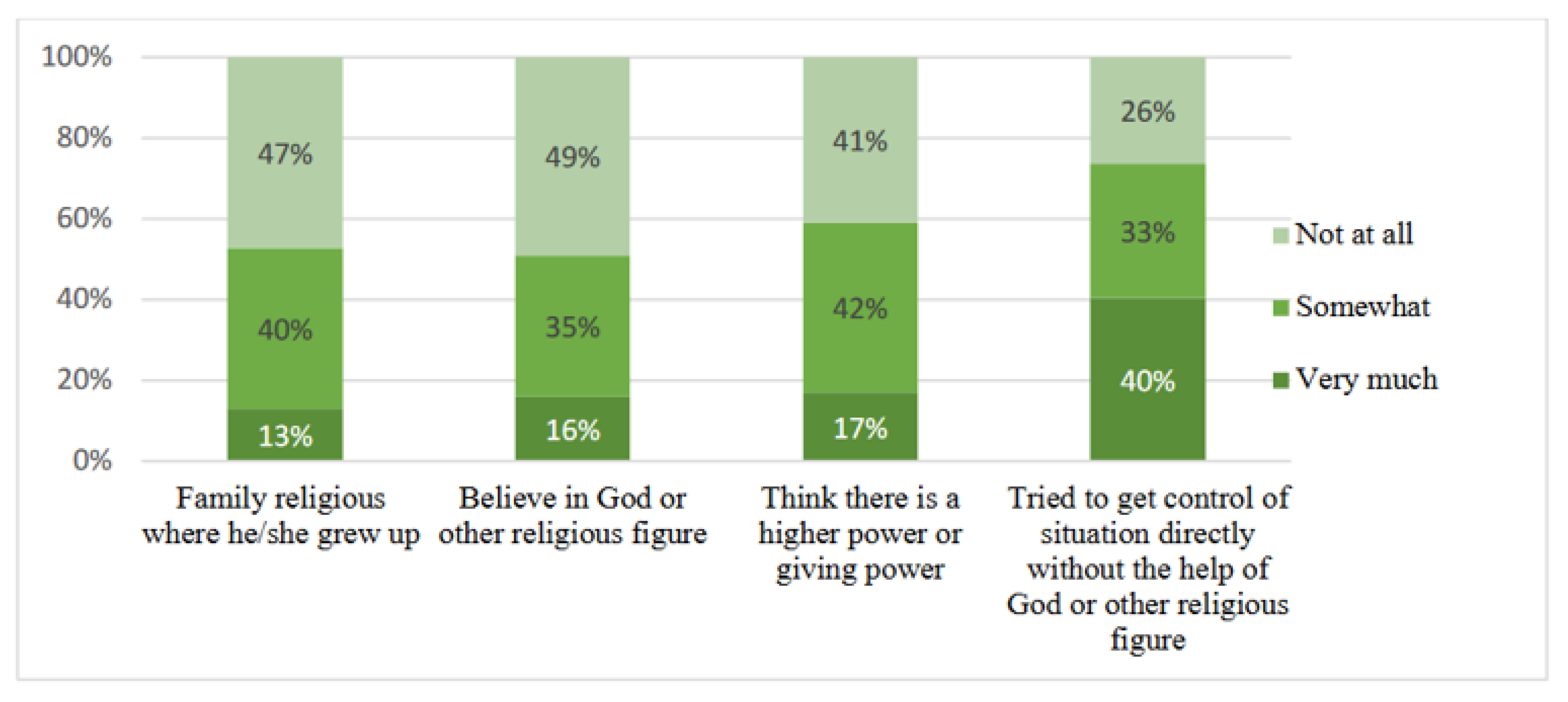
3.4. Religious and Spiritual Background and Thinking
3.5. Resilience, Self-Rated Health and Coping Methods
4. Discussion
4.1. Meaning-Giving Factors in Social/Collective and Personal/Individual Resilience
4.2. Resilience and Health
5. Conclusions
6. Limitations
7. Future Research and Policy Recommendations
- Focus on the bioecological framework of resilience in the context of COVID-19 by paying attention to individual, environmental, and meaning dimensions among academic staff.
- This study conducted a simple analysis univariate correlation (Pearson’s correlation). A multivariate analysis, such as regression analysis, adjusting for age, sex, and location, is required for future research to strengthen our findings.
- Set up structural resources in society to better balance individual capacity resources for resilience. Here, we refer to social resources such as social networks, stronger and wider connections to meaningful groups such as families and workmates, and also engaging in activities related to university or other groups, such as neighbourhood groups.
- Give due credit to academic staff as first responders within the education sector during pandemics as they show success in fulfilling their work duties without taking away the responsibility of their institutions to provide the necessary resources.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cao, W.; Fang, Z.; Hou, G.; Han, M.; Xu, X.; Dong, J.; Zheng, J. The psychological impact of the COVID-19 epidemic on college students in China. Psychiatry Res. 2020, 287, 112934. [Google Scholar] [CrossRef] [PubMed]
- Pfefferbaum, B.; North, C.S. Mental Health and the COVID-19 Pandemic. New Engl. J. Med. 2020, 383, 510–512. [Google Scholar] [CrossRef] [PubMed]
- Dubey, S.; Biswas, P.; Ghosh, R.; Chatterjee, S.; Dubey, M.J.; Chatterjee, S.; Lahiri, D.; Lavie, C.J. Psychosocial impact of COVID-19. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 779–788. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.H.; Sultana, S.; Hossain, S.; Hasan, M.T.; Ahmed, H.U.; Sikder, T. The impact of COVID-19 pandemic on mental health & wellbeing among home-quarantined Bangladeshi students: A cross-sectional pilot study. J. Affect. Disord. 2020, 277, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Killgore, W.; Taylor, E.C.; Cloonan, S.A.; Dailey, N.S. Psychological resilience during the COVID-19 lockdown. Psychiatry Res. 2020, 291, 113216. [Google Scholar] [CrossRef] [PubMed]
- Ju, G.; Lee, J.; Ahn, M.H.; Lee, J.; Kim, E.J.; Suh, S.; Chung, S. Effects of Depression and Resilience of Public Workers on Work-related Stress and Anxiety in Response to the COVID-19 Pandemic. J. Korean Med. Sci. 2021, 36, e262. [Google Scholar] [CrossRef] [PubMed]
- de Diego-Cordero, R.; Ávila-Mantilla, A.; Vega-Escaño, J.; Lucchetti, G.; Badanta, B. The Role of Spirituality and Religiosity in Healthcare During the COVID-19 Pandemic: An Integrative Review of the Scientific Literature. J. Relig. Health 2022, 61, 2168–2197. [Google Scholar] [CrossRef]
- Harpaz, I. Advantages and disadvantages of telecommuting for the individual, organization and society. Work Study 2002, 51, 74–80. [Google Scholar] [CrossRef]
- De los Reyes, E.J.; Blannin, J.; Cohrssen, C.; Mahat, M. Resilience of higher education academics in the time of 21st century pandemics: A narrative review. J. High. Educ. Policy Manag. 2022, 44, 39–56. [Google Scholar] [CrossRef]
- Carriedo, A.; Cecchini, J.A.; Fernandez-Rio, J.; Méndez-Giménez, A. COVID-19, Psychological Well-being and Physical Activity Levels in Older Adults During the Nationwide Lockdown in Spain. Am. J. Geriatr. Psychiatry Off. J. Am. Assoc. Geriatr. Psychiatry 2020, 28, 1146–1155. [Google Scholar] [CrossRef]
- Yusefi, A.R.; Daneshi, S.; Davarani, E.R.; Nikmanesh, P.; Mehralian, G.; Bastani, P. Resilience level and its relationship with hypochondriasis in nurses working in COVID-19 reference hospitals. BMC Nurs. 2021, 20, 219. [Google Scholar] [CrossRef] [PubMed]
- Song, S.; Yang, X.; Yang, H.; Zhou, P.; Ma, H.; Teng, C.; Chen, H.; Ou, H.; Li, J.; Mathews, C.A.; et al. Psychological Resilience as a Protective Factor for Depression and Anxiety among the Public during the Outbreak of COVID-19. Front. Psychol. 2021, 11, 618509. [Google Scholar] [CrossRef] [PubMed]
- Sharif Nia, H.; Akhlaghi, E.; Torkian, S.; Khosravi, V.; Etesami, R.; Froelicher, E.S.; Pahlevan Sharif, S. Predictors of Persistence of Anxiety, Hyperarousal Stress, & Resilience During the COVID-19 Epidemic: A National Study in Iran. Front. Psychol. 2021, 12, 671124. [Google Scholar] [CrossRef] [PubMed]
- Román-Mata, S.S.; Zurita-Ortega, F.; Puertas-Molero, P.; Badicu, G.; González-Valero, G. A Predictive Study of Resilience and Its Relationship with Academic and Work Dimensions during the COVID-19 Pandemic. J. Clin. Med. 2020, 9, 3258. [Google Scholar] [CrossRef]
- Ahmadi, F.; Cetrez, Ö.A.; Akhavan, S.; Zandi, S. Meaning-Making Coping With COVID-19 in Academic Settings: The Case of Sweden. Illn. Crisis Loss 2022, 30, 770–794. [Google Scholar] [CrossRef]
- Ahmadi, F.; Cetrez, Ö.A.; Akhavan, S.; Khodayarifard, M.; Zandi, S. How has the University Community Been Coping During the COVID-19 Pandemic? An Iranian Survey. Front. Sociol. 2022, 6, 645670. [Google Scholar] [CrossRef]
- Roberto, A.; Sellon, A.; Cherry, S.T.; Hunter-Jones, J.; Winslow, H. Impact of spirituality on resilience and coping during the COVID-19 crisis: A mixed-method approach investigating the impact on women. Health Care Women Int. 2020, 41, 1313–1334. [Google Scholar] [CrossRef]
- Ungar, M. (Ed.) The Social Ecology of Resilience: A Handbook of Theory and Practice; Springer: New York, NY, USA, 2012. [Google Scholar]
- Panter-Brick, C.; Eggerman, M. Understanding culture, resilience, and mental health: The production of hope. In The Social Ecology of Resilience: A Handbook of Theory and Practice; Ungar, M., Ed.; Springer: New York, NY, USA, 2012; pp. 369–386. [Google Scholar]
- Ungar, M. Resilience across Cultures. Br. J. Social Work 2008, 38, 218–235. [Google Scholar] [CrossRef]
- Zittoun, T.; Brinkmann, S. Learning as Meaning Making. In Encyclopedia of the Sciences of Learning; Seel, N.M., Ed.; Springer: New York, NY, USA, 2012; pp. 1809–1811. [Google Scholar]
- SCB. Higher Education. Employees in Higher Education 2020. Available online: https://www.scb.se/contentassets/e3e2c2f3c5574ef3847db70c04bcbacf/uf0202_2020a01_sm_uf23sm2101.pdf (accessed on 26 June 2022).
- SCB. Utbildningsnivån i Sverige [Educational level in Sweden]. Available online: https://www.scb.se/hitta-statistik/sverige-i-siffror/utbildning-jobb-och-pengar/utbildningsnivan-i-sverige/ (accessed on 26 June 2022).
- Connor, K.M.; Davidson, J.R.T. Development of a new resilience scale: The Connor-Davidson resilience scale (CD-RISC). Depress. Anxiety 2003, 18, 76–82. [Google Scholar] [CrossRef]
- Çetrez, Ö.; DeMarinis, V.; Sundvall, M.; Fernandez, M.; Borisova, L.; Titelman, D. A Public Mental Health Study Among Iraqi Refugees in Sweden: Social Determinants, Resilience, Gender and Cultural Context. Front. Sociol. Med. Sociol. 2021, 6, 551105. [Google Scholar] [CrossRef]
- Rand Healthcare. Available online: https://www.rand.org/health-care/surveys_tools/mos/36-item-short-form/survey-instrument.html (accessed on 28 September 2022).
- Pargament, K.I.; Koenig, H.G.; Perez, L.M. The many methods of religious coping: Development and initial validation of the RCOPE. J. Clin. Psychol. 2000, 56, 519–543. [Google Scholar] [CrossRef]
- Ahmadi, N.; Ahmadi, F. Iranian Islam: The Concept of the Individual; Macmillan Press Ltd.: London, UK, 2018. [Google Scholar]
- Thurfjell, D. Granskogsfolk: Hur Naturen Blev Svenskarnas Religion; [Spruce Forest People: How Nature Became the Swedes’ Religion]; Norstedts: Stockholm, Sweden, 2020. [Google Scholar]
- Uddenberg, N. Det Stora Sammanhanget. Moderna Svenskars Syn på Människans Plats i Naturen; [The great whole: The modern Swede’s view of the human beings’ place in nature]; Nya Doxa: Nora, Sweden, 1995. [Google Scholar]
- Hu, J.; Huang, Y.; Liu, J.; Zheng, Z.; Xu, X.; Zhou, Y.; Wang, J. COVID-19 Related Stress and Mental Health Outcomes 1 Year After the Peak of the Pandemic Outbreak in China: The Mediating Effect of Resilience and Social Support. Front. Psychiatry 2022, 13, 828379. [Google Scholar] [CrossRef]
- Walsh, F. Family Resilience: A Dynamic Systemic Framework. In Multisystemic Resilience: Adaptation and Transformation in Contexts of Change; Ungar, M., Ed.; Oxford University Press: New York, NY, USA, 2021. [Google Scholar] [CrossRef]
- Johansson, P.; Sennemark, E.; Magnusson, L.; Hanson, E. Konsekvenser av COVID-19 Pandemin För Barn Som Anhöriga Och Unga Omsorgsgivare [Consequences of COVID-19 Pandemic for Children as Relatives and Young Care Providers]. Nationellt Kompetenscentrum Anhöriga. 2021. Available online: https://www.diva-portal.org/smash/get/diva2:1597309/FULLTEXT01.pdf (accessed on 28 June 2022).
- Simich, L.; Andermann, L. (Eds.) Refuge and Resilience: Promoting Resilience and Mental Health among Resettled Refugees and Forced Migrants; Springer: Dordrecht, The Netherlands, 2014. [Google Scholar]
- Inglehart, R. Religion’s Sudden Decline: What’s Causing It and What Comes Next? Oxford University Press: Oxford, UK, 2021. [Google Scholar]
- Hagevi, M. Religiös förändring under coronapandemin: Gav religion tröst? [Religious change during the Corona pandemic: Did religion give consolation?]. Surveyjournalen 2020, 7, 52–65. [Google Scholar] [CrossRef]
- Marsella, A.J. Culture and Conflict: Understanding, negotiating and reconciling, conflicting constructions of reality. Int. J. Intercult. Res. 2005, 29, 651–673. [Google Scholar] [CrossRef]
- The Inglehart-Welzel World Cultural Map-World Values Survey 7 [Provisional Version]. Available online: http://www.worldvaluessurvey.org/ (accessed on 26 June 2022).
- United Nations. Policy Brief: Education during Covid-19 and beyond, 2020. Available online: https://unsdg.un.org/resources/policy-brief-education-during-covid-19-and-beyond (accessed on 19 July 2022).




{kind=link}
{kind=link}
{kind=link}
| Variable | Variable Value | % |
|---|---|---|
| Gender | Man | 36 |
| Woman | 64 | |
| Age groups | Younger than 35 years old | 31 |
| Between 35–49 years old | 32 | |
| 50 years or older | 37 | |
| Education | University | 94 |
| Gymnasium or similar | 6 | |
| Country of birth | Sweden | 75 |
| Other countries | 25 | |
| Job/student situation | Full-time employment | 66 |
| Part-time employment | 15 | |
| Student | 19 | |
| Social status | Married | 50 |
| Divorced | 5 | |
| Engaged | 11 | |
| Widowed | 1 | |
| Single | 17 | |
| Other | 16 | |
| Children | Having children | 64 |
| No children | 36 | |
| Place of living | Capital | 18 |
| Medium-large city | 48 | |
| Small town | 34 |
| Family | Friends | Religion/ Spirituality | Work/ School | Nature | ||
|---|---|---|---|---|---|---|
| General health | Pearson Correlation | 0.027 | 0.044 | 0.045 | 0.048 | −0.020 |
| n | 278 | 278 | 278 | 278 | 278 | |
| P1 | P2 | P3 | P4 | P5 | P6 | P7 | P8 | P9 | P10 | P11 | P12 | P13 | P14 | P15 | P16 | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CD-RISC | Pearson Correlation | −0.029 | −0.009 | −0.059 | 0.081 | 0.038 | −0.049 | 0.010 | −0.189 | −0.157 | −0.167 | −0.026 | −0.239 | −0.062 | −0.113 | −0.119 | 0.050 |
| n | 278 | 278 | 278 | 278 | 278 | 278 | 278 | 278 | 278 | 278 | 278 | 278 | 278 | 278 | 278 | 278 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cetrez, Ö.A.; Zandi, S.; Ahmadi, F. When a Pandemic Strikes: Resilience of Swedish Academics in the Face of Coronavirus. Int. J. Environ. Res. Public Health 2022, 19, 13346. https://doi.org/10.3390/ijerph192013346
Cetrez ÖA, Zandi S, Ahmadi F. When a Pandemic Strikes: Resilience of Swedish Academics in the Face of Coronavirus. International Journal of Environmental Research and Public Health. 2022; 19(20):13346. https://doi.org/10.3390/ijerph192013346
Chicago/Turabian StyleCetrez, Önver Andreas, Saeid Zandi, and Fereshteh Ahmadi. 2022. "When a Pandemic Strikes: Resilience of Swedish Academics in the Face of Coronavirus" International Journal of Environmental Research and Public Health 19, no. 20: 13346. https://doi.org/10.3390/ijerph192013346
APA StyleCetrez, Ö. A., Zandi, S., & Ahmadi, F. (2022). When a Pandemic Strikes: Resilience of Swedish Academics in the Face of Coronavirus. International Journal of Environmental Research and Public Health, 19(20), 13346. https://doi.org/10.3390/ijerph192013346