
Suicide and Suicide Prevention Activities Following the Great East Japan Earthquake 2011: A Literature Review


Abstract
1. Introduction
2. Materials and Methods
2.1. Definition of the Disaster: The Great East Japan Earthquake
2.2. Study Process for the Literature Review
2.2.1. Database
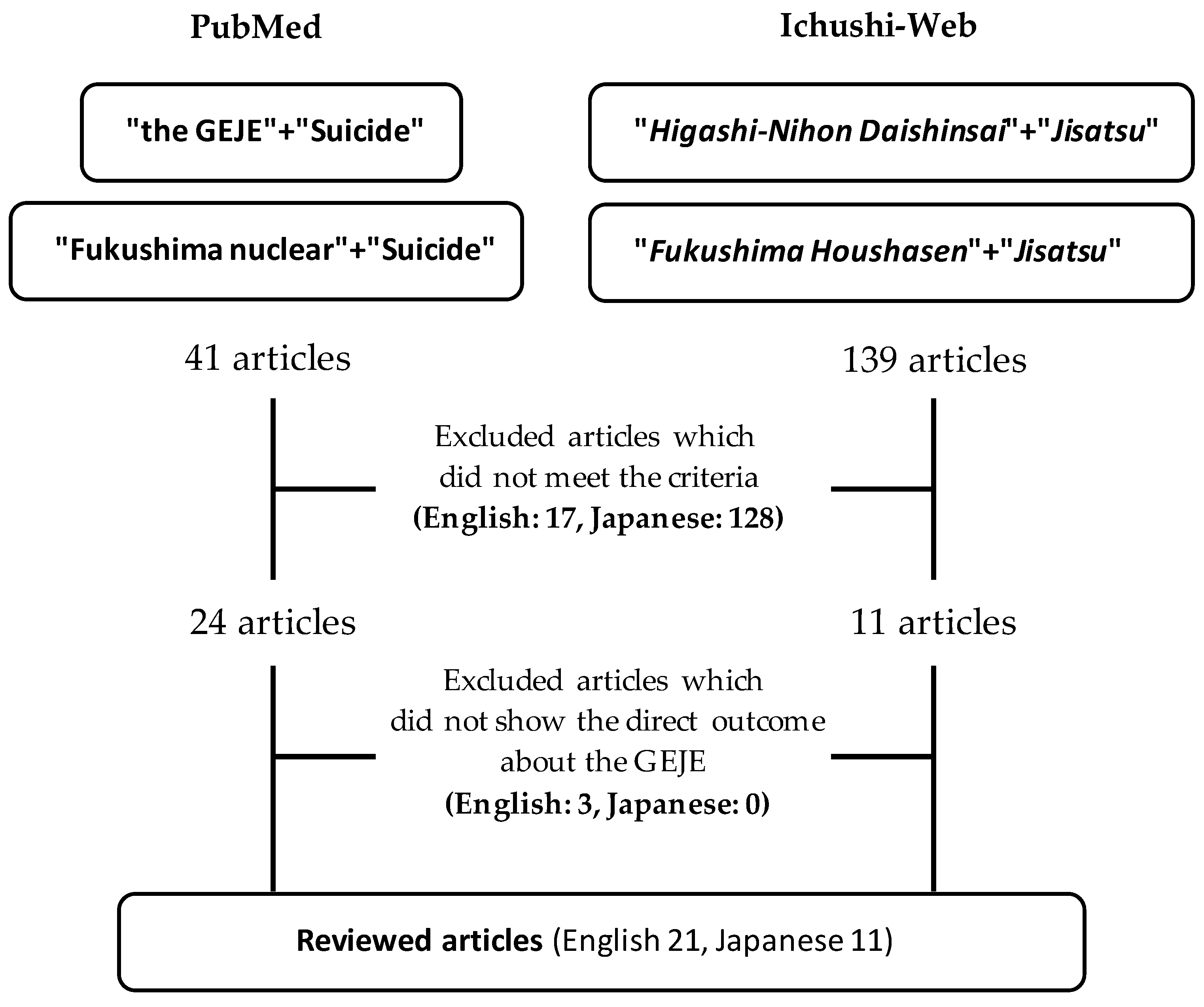
2.2.2. Search Strategy and Inclusion/Exclusion Criteria
2.2.3. Literature Selection Process
2.2.4. Categorizing Selected Articles
2.3. Ethical Considerations
3. Results
3.1. Descriptive Epidemiological Study about Regional Suicide Rates in the Affected Area or Other Areas
3.2. Ecological Study Examining the Factors Related to the Suicide Rates
3.3. Cross-Sectional or Longitudinal Study Examining Factors Related to Suicidal Ideation or Behaviors
3.4. Descriptive Study Concerning Those Who Attempted Suicide and Visited Emergency Hospitals
3.5. Case Reports
3.6. Practical Reports Regarding Suicide Prevention Activities and Disaster-Related Mental Health Activities
3.7. Review Study of Counselors’ Daily Records and Training Interventions for Counselors

{kind=link}
| Authors | Measures of Suicidal Behavior | Time Period | Location | Subjects | Analysis | Main Findings |
|---|---|---|---|---|---|---|
| ||||||
| Liu Y. et al. (2015) [5] | Suicide rates (annual and monthly) | A year after the GEJE; comparison of 2005 with 2011 | Nationwide | All residents in Japan | Prais–Winsten regression using 11 dummy variables (January taken as the reference) to detect any seasonal variations separately for men and women. | There was no significant difference in any 2 years adjacent to 2011 for either gender. However, with respect to women, the suicide number in 2011 was higher than that in 2010; in particular, the 10 months from March to December 2011 showed a significant difference compared with 2010 for women but not for men. |
| Osaki Y. et al. (2021) [6] | Suicide rates (SMR, monthly) | 2 years in 2011 and 2020 (at the time of the GEJE and during the COVID-19 pandemic in 2020) | Nationwide | All residents of the prefectures | The 95% confidence intervals for the ratio were calculated to determine any statistically significant increases or decreases in the suicide rate nationwide and in the three affected prefectures. | After the earthquake, the male suicide rate in March 2011 was 18% lower than the average mortality rate for the previous 3 years. However, it increased by 18% in May and 8% in June, and increased mortality was observed in women. |
| Matsubayashi T. et al. (2021) [7] | Suicide rates (annual) | 8 years after the GEJE and baseline (from 2002 to 2019) | Nationwide | All residents of the prefectures | Event-study estimates of the GEJE on sex–age specific suicide rates. | Using prefecture-level data, suicide by men aged 40–64 years and 65 years and over showed a significant decline in the years following the GEJE, and this decline attenuated over time. |
| Tsuboi S. et al. (2012) (in Japanese) [8] | Suicide number and suicide rates (monthly) | From January to June in 2008, 2009, 2010, and 2011 | Tochigi Prefecture (next to southern Fukushima) | All residents in Tochigi Prefecture | Time series analysis was used to examine the trend in monthly suicide rates during the same period (January to June) in 2008, 2009, 2010, and 2011. | The monthly suicide rates in Tochigi Prefecture increased in March in 2008, 2009, and 2010; however, it increased from March to May in 2011, peaking in May. |
| Masaki N. et al. (2018) (in Japanese) [9] | Suicide rates (SMR, monthly, annual) | 2 years after the GEJE and baseline (from 2010 to 2013) | The municipalities in the coastal area of the Iwate, Miyagi, and Fukushima prefectures | All residents of the municipalities in the coastal areas of the Iwate, Miyagi, and Fukushima prefectures | The SMRs of the subject area in the affected area were calculated, and then compared with the pre-disaster SMR. | The ratio of the SMR was 0.92 in the first post-disaster period (from 2011 to 2012), and 0.93 in the second period (from 2012 to 2013), which was significantly lower compared with the pre-disaster SMR. |
| Orui M. et al. (2015) [10] | Suicide rates (monthly, annual) | 3 years after the GEJE and baseline (from March 2009 to February 2014) | 16 municipalities in the coastal area of Miyagi Prefecture | All residents of the 16 municipalities in the coastal area of Miyagi | Suicide rates were assessed using a time series, in which suicide rates were compared with corresponding national averages. | In tsunami disaster-stricken areas, male suicide rates were initially significantly lower than the national average but began to increase after 2 years. Similarly, male suicide rates in the inland areas decreased for 7 months, and then increased to exceed the national average. |
| Ohto et al. (2015) [11] | Suicide rates (SMR, annual) | 3 years after the GEJE and baseline (from 2010 to 2014) | Disaster affected prefectures (Iwate, Miyagi, Fukushima) | All residents in the affected prefectures | SMR comparison with national average. | SMR decreased during the first 2 years after the disaster in each affected prefecture compared with 2010 (table), and then rose in 2014 to pre-disaster levels in the Iwate and Miyagi prefectures and exceeded the pre-disaster level in Fukushima Prefecture. |
| Orui M. et al. (2018) [12] | Suicide rates (annual and monthly) | Almost 5 years after the GEJE and baseline (from March 2009 to February 2011) | Fukushima Prefecture, including the evacuation area related to the Fukushima Daiichi Nuclear Power Plant accident | All residents in the Fukushima Prefecture | The exponential smoothing time series model was used to examine the trend of monthly suicide rates. Additionally, period analysis was performed for each 12-month period from March 2009 to February 2015 (and the 9 months from March 2015 to December 2015) and compared to the national average. | Male suicide rates in the evacuation areas increased significantly immediately after the disaster, and then began to increase again 4 years after the disaster. Female suicide rates declined slightly during the first year and then increased significantly over the subsequent 3-year period. |
| Orui M. (2020) [14] | Suicide rates (annual) | 7 years after the GEJE and baseline (from 2009 to 2018) | 14 municipalities in the coastal area of Miyagi Prefecture | All residents of the 14 municipalities in the coastal area of Miyagi | Period analysis was used to divide the total 108-month study period into nine segments, in which suicide rates were compared with corresponding national averages using a Poisson distribution. | Male suicide rates in the affected area from March 2013 to February 2014 increased to a level higher than the national average. After subsequently dropping, the male suicide rates increased again from March 2016 to February 2018 and showed a significant difference compared with the national averages. |
| Orui M. et al. (2020) (in Japanese) [13] | Suicide rates (monthly) | 8 years after the GEJE and baseline (from 2009 to 2019) | 14 municipalities in the coastal area of Miyagi Prefecture | All residents of the 14 municipalities in the coastal area of Miyagi | Moving average time series analysis was used to remove the seasonal changes. | Male suicide rates increased gradually from May 2016 when the provision of free temporary housing began to be phased out. A little later, from December 2017, female suicide rates also increased. |
| Kuroda Y. et al. (2021) [15] | Suicide rates (monthly, annual) | 8 years after the GEJE and baseline (from June 2009 to December 2018) | Evacuation area in Fukushima Prefecture following the Fukushima Daiichi Nuclear Power Plant accident | All residents of the municipalities in the evacuation area | Time series model using exponential smoothing between the evacuation and the non-evacuation areas in Fukushima Prefecture. | In the evacuation areas, the male suicide rate increased immediately after the disaster and then decreased steeply around 1.5 years after the disaster. However, with the lifting of the evacuation order, it again exceeded that of non-evacuation areas and continued to do so for the next 3 years. On the other hand, the suicide rate in women in the evacuation areas started to increase later than that in men. |
| Inoue K. et al. (2015) [16] | Disaster-related suicide and its motives | 2 years after the GEJE (from 2011 to 2013) | Disaster-stricken prefectures and the prefectures to which evacuees were relocated | All residents of disaster-stricken prefectures and prefectures to which evacuees were relocated | Descriptive analysis of suicide number by gender reported from suicide statistics. | Among the cases of disaster-related suicide, men accounted for a large proportion of suicides in the year that the disaster occurred, but the proportion of suicides among women increased 2 years after the disaster. The main motives for the related suicides were health problems, which increased significantly after the GEJE. |
| Takebayashi Y. et al. (2020) [17] | Disaster-related suicide numbers and rates | 7 years after the GEJE | Fukushima Prefecture | 99 suicide cases which were determined to be disaster-related suicides | Descriptive analysis of suicide rates by age, gender, means, and occupation among disaster-related suicide cases as defined by the Cabinet Office. | Age-standardized disaster-related suicide rates were notably higher in men than in women. In addition, disaster-related suicide rates in Fukushima were higher in women in their 50s and 80s compared with overall suicide rates in Fukushima or Japan. |
| ||||||
| Orui M. et al. (2014) [18] | Suicide rates (monthly) | 2 years after the GEJE and baseline (from March 2009 to February 2014) | Disaster-stricken prefectures and neighboring prefectures (Aomori, Akita, Yamagata) | All residents of disaster-stricken and neighboring prefectures | Using the multiple regression model, the association between suicide rates and economic variables was evaluated based on the number of bankruptcy cases and ratio of effective job offers and comparing the disaster-stricken and neighboring prefectures. | In disaster-stricken areas, male suicide rates decreased during the 24 months following the earthquake. Multiple regression analysis showed that bankruptcy cases and ratio of effective job offers were only significantly associated with male post-disaster suicide rates in the neighboring prefectures rather than in the disaster-stricken prefectures. |
| Shiga Y. et al. (2016) (in Japanese) [19] | Suicide rates (SMR) | Two periods before and after the GEJE (2008–2010 and 2011–2013) | Iwate Prefecture | All residents in Iwate Prefecture | The suicide SMR was calculated for the nine medical health areas in Iwate Prefecture and the correlation between SMR and economic status, medical care, and disaster damage was examined. | The high suicide rate in Iwate Prefecture was found to be related to the small number of temporary houses and small disaster recovery budgets. |
| ||||||
| Fujiwara T. et al. (2017) [20] | Suicide risk (suicidal ideation, self-injury behavior and suicide attempts in a lifetime); MINI-KID | Baseline: 2 years after the GEJE (from September 2012 to June 2013) Follow-up: 3 years later (from July 2013 to May 2014) | The municipalities in the coastal area in the Iwate, Miyagi, and Fukushima prefectures (Control: Mie Prefecture located in the western region of Japan) | 198 children aged 5–8 in the Iwate, Miyagi, and Fukushima prefectures (Control: 82 children aged 5–8 in the Mie Prefecture) | A logistic regression analysis between suicide risks and earthquake-related events, exposure to other trauma before the GEJE, psychological distress (K6), and PTSD symptoms (IES-R). | Four or more trauma experiences related to the GEJE was associated with suicide risk only among girls (Odds ratio: 5.74, 95%CI: 0.83–39.6, p = 0.076) compared to no trauma experience related to the GEJE. This showed that young girls who experienced earthquake-related trauma at preschool age had a higher suicidal ideation 3 years after the GEJE. |
| Xu Q. et al. (2018) [21] | Suicidal ideation (WHO-CIDI) version 3.0 | 3 years after the GEJE (Iwate, Miyagi: June and August 2014, Fukushima: from October 2013 to February 2014, Control: from August to November 2014) | Severely damaged areas in Iwate, Miyagi, and Fukushima (Control: Eastern Japan excluding Kanto region) | More than 2000 adults aged 20 years and older residing in temporary housing in Iwate, Miyagi, and Fukushima (Control: 1850 individuals) | (1) The cumulative incidence of suicidal ideation using the Cox proportional hazard model. (2) A multiple logistic regression analysis was conducted to examine risk factors for the onset of suicidal ideation. | (1) Amongst 1019 respondents, the cumulative incidence of suicidal ideation 1, 2, and 3 years after the earthquake was 1.4%, 2.4%, and 2.8%, respectively—significantly higher than that in the control. (2) Not being married, being injured in the disaster, and poor subjective physical health were associated with suicide ideation. |
| Morishima R. et al. (2019) [22] | Suicidal ideation (investigator-designed query) | 1, 2 and 3 years after the GEJE (May and June in 2012, 2013, and 2014) | Higashi-Matsushima City in Miyagi Prefecture, where serious damage was inflicted by the tsunami | 11,855 residents who were 19 years or older, and had enrolled for the national health insurance | A logistic regression analysis was conducted to evaluate the effect of suicidal ideation risk on the onset of mental illness (K6 > 13 points) for three years, adjusting for age, sex, house damage, presence of cohabitants, residence situation, working status, and seeking counselling for mental health. | Many residents, who showed a high risk of suicidality, still suffer from a mental illness, requiring housing, occupation, and psychological support. Chronic or delayed onset mental illness showed a higher risk of suicidal ideation (Odds ratio: 23.3 and 60.6, respectively). |
| Kawahara K. et al. (2020) [23] | Suicide risk (suicidal ideation, self-injury behavior and suicide attempts in a lifetime); MINI-KID | 5 years after the GEJE | Ishinomaki City, Miyagi Prefecture, which was damaged severely by the tsunami disaster | 262 students in two junior high schools | A logistic regression analysis between suicide risks and psychological symptoms (PTSD, depression, anxiety), disaster experiences (housing damage or evacuation), and current residents (temporary or own housing). | Disaster experience was not associated with psychological symptoms (PTSD, depression, anxiety) or suicide risk in junior high school students 5 years after the GEJE. The suicide risk appeared to be the same as that in the general population in Japan. |
| ||||||
| Kato K. et al. (2014) [24] | Suicide attempts involving visits to hospital (cases of minor self-injury excluded) | Pre-disaster (from September 2010 to February 2011) and post-disaster (from April 2011 to September 2011) | Kanagawa Prefecture, next to the Tokyo metropolitan area; this was not the disaster area, but was significantly indirectly affected | 286 attempted suicides in the pre-disaster period, 306 in the post-disaster period | The psychiatric characteristics of suicide attempts were assessed, with one or two trained psychiatrists making a diagnosis according to the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition DSM-IV). | With regard to mood, anxiety, schizophrenia, and substance-related disorders, no significant difference in the number of patients with psychiatric disorders was observed between the pre- and post-disaster periods. The number of patients in a serious condition in the post-disaster period was significantly higher than that in the pre-disaster period. |
| Aoki Y. et al. (2014) [25] | The number of suicide attempts at a tertiary medical center which accepts the most critically ill patients | A year after the GEJE and control period (11 March 2010 to 10 March 2012) | The medical center located in the middle-southern area of the Fukushima Prefecture and 58 km west of Fukushima Daiichi Nuclear Power Plant | Individuals who attempted suicide who were transferred to this medical center | The clinical records of all patients who visited the medical center near the nuclear plant from 1 year before to 1 year after the disaster were reviewed (n = 981). | The risk of nonfatal suicide attempts (those who survived) using high mortality methods (methods other than self-poisoning and wrist-slitting) was significantly higher, by three to four times, for 4 months after the series of disasters, and then decreased. There was no significant increase in nonfatal suicide attempts using low-mortality methods (self-poisoning and wrist slitting) after the disaster. |
| Yoshioka Y. et al. (2015) (in Japanese) [26] | Suicide attempts (those who were admitted to a tertiary medical center) | During the 1-year period after the GEJE | Morioka City, Iwate Prefecture, which is a central city in Iwate Prefecture | 10 suicide attempt cases who had problems related to the GEJE | A review of clinical records relating to 10 cases with regards to age, sex, methods of suicide, psychiatric diagnosis, and background of suicide behavior. | The clinical features of cases within 4 weeks were classed as acute stress, and after 4 weeks they were classed as secondary stress reactions, such as drastic environmental changes in lifestyle. Depressive states were also noted. |
| Ikemoto K. et al. (2011) (in Japanese) [27] | Suicide attempts (those who were admitted to the department of psychiatry at a tertiary medical center) | During the 3-month period after the GEJE | Iwaki City, Fukushima Prefecture, close to Fukushima Daiichi Nuclear Power Plant | 11 suicide attempt cases admitted to the psychiatry department | A review of clinical records relating to 11 cases with regards to age, sex, methods of suicide, psychiatric diagnosis, and background of suicidal behavior | The background psychosocial factors relating to the suicide attempts varied between cases (e.g., family problems, intersexual problems, and alcohol-related), which almost had little to no direct relation to the GEJE or the nuclear power plant accident, even in evacuees. |
| ||||||
| Yamashita J. et al. (2013) [28] | Suicide cases | Within 6 months of the GEJE | Minami-soma City, Fukushima Prefecture | Residents evacuated because of the GEJE and Fukushima Daiichi Nuclear Power Plant accident | Searching the articles in newspapers | In a note that she left behind, a woman wrote that she did not want to bother her son’s family and had chosen to take refuge in the grave. In the months following the disaster, many people perceived that they were going to lose their neighborhood support networks and had diminished hope for the future, in the absence of any concrete financial support provided by the government. |
| ||||||
| Son D. et al. (2015) (in Japanese) [29] | Mental health issues, including suicidal ideation and other social issues | From August 2011 to May 2012 | Higashi-Matsushima City, Ishinomaki City and Kesennuma City in Miyagi Prefecture | Almost 1500 evacuees who relocated to temporary housing | Unknown | Evacuees who had experienced a depressive state, PTSD, anxiety disorders, insomnia, alcoholism, and suicidal ideation were referred to a psychiatrist or public health nurse in the public health centers. |
| Orui M. et al. (2019) (in Japanese) [30] | The number of suicides in the subject area | Almost 6 years after the GEJE | Iitate Village in the evacuation area due to Fukushima Daiichi Nuclear Power Plant accident | All residents in Iitate Village, Fukushima Prefecture, including evacuees who relocated outside the evacuation area | To implement suicide measures, namely: (1) screening for evacuees regarding mental health issues and outreach to those who have been at high risk; (2) gatekeeper training for public office workers; and (3) supervision and support for public health nurses in Iitate. | Although the direct reason was unknown, the number of suicides in Iitate did not exhibit a sharp increase after the GEJE, with the number staying flat at 0–2 per year, pre- and post-disaster. |
| Orui M. et al. (2017) [31] | Suicide rates | 4.5 years after the GEJE | Sendai City in the disaster-affected area in Miyagi Prefecture | All residents in Sendai City | To address the psychosocial issues of evacuees, the disaster mental health team provided psychosocial and social support. The suicide rate in the disaster-affected area was used as one of the outcome indicators of this activity. | Although the direct effect of this disaster-related mental health activity was unknown, at the time of the report the suicide rate in Sendai City had not increased since the GEJE. |
| Orui M. et al. (2021) [32] | Suicide rates (monthly) | 9 years after the GEJE during the COVID-19 pandemic | 14 municipalities in the coastal area of the Miyagi Prefecture | All residents of the 14 municipalities in the coastal area of Miyagi | The suicide rate trends were assessed using exponential smoothing time series modelling. The area in question is the disaster-affected area which has seen the implementation of disaster-related mental health activities on an ongoing basis, including during the COVID-19 pandemic. | During the COVID-19 pandemic, the suicide rate in the affected areas showed a declining trend, whereas the national rates and the rates in the non-affected areas showed an increasing trend, although the affected areas were higher than the national average at the beginning of the COVID-19 pandemic. |
| ||||||
| Shiragami K. et al. (2013) (in Japanese) [33] | Suicidal ideation | First survey: December 2011 Second survey: May 2012 | A municipality in Iwate Prefecture | 24 livelihood support counselors | 24 counselors were asked whether they had the experience to address evacuees with suicidal ideation. | At the time of the first survey, none of the counselors had the experience to address suicide ideation among evacuees, although 21.1% of counselors had addressed evacuees with suicide ideation at the time of the second survey. |
| Ueno M. et al. (2016) (in Japanese) [34] | Suicide-related problems (e.g., suicidal ideation) | 18-month follow-up of support for evacuees from May 2011 | Disaster-affected area in Miyagi Prefecture | 1669 evacuees who relocated to temporary housing | A review of records concerning support for evacuees, and evaluation of the safety status, and physical and mental health condition (e.g., alcoholism, depression, suicidal ideation). | More than 50% of those evacuees who had suicidal ideation have continued to experience mental health issues, even after 18 months of support. |
| Akazawa M. et al. (2016) (in Japanese) [35] | Self-confidence in counselling and responding to residents’ mental health issues | November and December 2014 | Two municipalities in the disaster-affected area in Miyagi | 101 livelihood support counselors in the disaster-affected area | To evaluate the outcomes of the training seminar, pre- and immediate post-intervention surveys were conducted. | Counselors’ confidence to cope with the suicidal ideation of residents showed a significant increase at the post-intervention survey. |
| Orui M. et al. (2020) [36] | Self-confidence in counselling and responding to residents’ mental health issues | November and December 2019 | Minami-soma City and Iitate Village in Fukushima Prefecture, in the evacuation areas | 26 livelihood support counselors from Iitate Village and Minami-Soma City Social Welfare Council participated in the training program | To evaluate the outcomes of the training program, including a pre- and post-survey, and a follow-up survey 2 months after the intervention was conducted. | The program content regarding suicide was as follows: specific ways to communicate with residents who have suicidal thoughts: (a) questioning about the suicidal thoughts, and (b) encouraging a person to seek appropriate professional help. As a result, counselors’ confidence to cope with the resident’s suicidal thoughts showed a significant increase. |
4. Discussion
4.1. Gender Differences in Suicide Rates in the Affected Area and Nationwide in the Period of Two to Three Years
4.2. Suicide Rates Increasing Again in the Recovery Phase
4.3. Background to the Case of Suicide and Suicidal Behaviors Following the GEJE
4.4. Suicide Prevention Measures Following the GEJE
4.5. Limitations and Strengths of This Literature Study
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kõlves, K.; Kõlves, K.E.; De Leo, D. Natural disasters and suicidal behaviours: A systematic literature review. J. Affect. Disord. 2013, 146, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Jafari, H.; Heidari, M.; Heidari, S.; Sayfouri, N. Risk Factors for Suicidal Behaviours after Natural Disasters: A Systematic Review. Malays. J. Med. Sci. 2020, 27, 20–33. [Google Scholar] [CrossRef] [PubMed]
- Matsubayashi, T.; Sawada, Y.; Ueda, M. Natural disasters and suicide: Evidence from Japan. Soc. Sci. Med. 2013, 82, 126–133. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Page, A.; Martin, G.; Taylor, R. Attributable risk of psychiatric and socio-economic factors for suicide from individual-level, population-based studies: A systematic review. Soc. Sci. Med. 2011, 72, 608–616. [Google Scholar] [CrossRef]
- Liu, Y.; Zhang, Y.; Arai, A.; Obayashi, Y.; Tamashiro, H. Gender-based seasonality of suicide in Japan, 2005–2012. Asia Pac. J. Public Health 2015, 27, NP1999–NP2007. [Google Scholar] [CrossRef] [PubMed]
- Osaki, Y.; Otsuki, H.; Imamoto, A.; Kinjo, A.; Fujii, M.; Kuwabara, Y.; Kondo, Y.; Suyama, Y. Suicide rates during social crises: Changes in the suicide rate in Japan after the Great East Japan earthquake and during the COVID-19 pandemic. J. Psychiatr. Res. 2021, 140, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Matsubayashi, T.; Kamada, T. The Great East Japan Earthquake and suicide: The long-term consequences and underlying mechanisms. Prev. Med. 2021, 153, 106755. [Google Scholar] [CrossRef]
- Tsuboi, S.; Uehara, R.; Enkh-Oyun, T.; Kotani, K.; Aoyama, Y.; Nakamura, Y. Suicide trends in Tochigi prefecture following the 2011 Tohoku Earthquake off the Pacific coast of Japan. Jichi Med. Univ. J. 2012, 35, 63–66. (In Japanese) [Google Scholar]
- Masaki, N.; Hashimoto, S.; Kawado, M.; Ojima, T.; Takeshima, T.; Matsubara, M.; Mitoku, K.; Ogata, Y. The number of deaths by suicide after the Great East Japan Earthquake based on demographic statistics in the coastal and non-coastal areas of Iwate, Miyagi, and Fukushima prefectures. Nihon Koshu Eisei Zasshi. 2018, 65, 164–169. (In Japanese) [Google Scholar] [CrossRef]
- Orui, M.; Sato, Y.; Tazaki, K.; Kawamura, I.; Harada, S.; Hayashi, M. Delayed increase in male suicide rates in tsunami disaster-stricken areas following the great east japan earthquake: A three-year follow-up study in Miyagi Prefecture. Tohoku J. Exp. Med. 2015, 235, 215–222. [Google Scholar] [CrossRef][Green Version]
- Ohto, H.; Maeda, M.; Yabe, H.; Yasumura, S.; Bromet, E.E. Suicide rates in the aftermath of the 2011 earthquake in Japan. Lancet 2015, 385, 1727. [Google Scholar] [CrossRef] [PubMed]
- Orui, M.; Suzuki, Y.; Maeda, M.; Yasumura, S. Suicide Rates in Evacuation Areas After the Fukushima Daiichi Nuclear Disaster. Crisis 2018, 39, 353–363. [Google Scholar] [CrossRef]
- Orui, M.; Harada, S.; Saeki, S.; Sato, K.; Kozakai, Y.; Hayashi, M. Trend in the Suicide Rate Following the Great East Japan Earthquake: An Eight-year Follow-up Study in Miyagi Prefecture. Psychiatr. Neurol. Jpn. 2022, 122, 573–584. (In Japanese) [Google Scholar]
- Orui, M. Re-Increased Male Suicide Rates in the Recovery Phase Following the Great East Japan Earthquake. Crisis 2020, 41, 422–428. [Google Scholar] [CrossRef] [PubMed]
- Kuroda, Y.; Orui, M.; Hori, A. Trends in Suicide Mortality in 10 Years around the Great East Japan Earthquake: Analysis of Evacuation and Non-Evacuation Areas in Fukushima Prefecture. Int. J. Environ. Res. Public Health 2021, 18, 6005. [Google Scholar] [CrossRef] [PubMed]
- Inoue, K.; Fujita, Y.; Miyaoka, T.; Ezoe, S.; Horiguchi, J. Importance of measures to prevent suicides related to the Great East Japan Earthquake among women. Psychiatry Clin. Neurosci. 2015, 69, 596. [Google Scholar] [CrossRef]
- Takebayashi, Y.; Hoshino, H.; Kunii, Y.; Niwa, S.I.; Maeda, M. Characteristics of Disaster-Related Suicide in Fukushima Prefecture After the Nuclear Accident. Crisis 2020, 41, 475–482. [Google Scholar] [CrossRef]
- Orui, M.; Harada, S.; Hayashi, M. Changes in suicide rates in disaster-stricken areas following the Great East Japan Earthquake and their effect on economic factors: An ecological study. Environ. Health Prev. Med. 2014, 19, 459–466. [Google Scholar] [CrossRef]
- Shiga, Y.; Otsuka, K.; Endo, J.; Honta, E.; Sato, H.; Nakamura, H.; Akahira, M.; Sakai, A. Relationship between the suicide standardized mortality ratio and local community indices before and after the Great East Japan Earthquake in Iwate prefecture. Iwate Igaku Zasshi 2016, 68, 207–222. [Google Scholar]
- Fujiwara, T.; Yagi, J.; Homma, H.; Mashiko, H.; Nagao, K.; Okuyama, M. Great East Japan Earthquake Follow-up for Children Study Team. Suicide risk among young children after the Great East Japan Earthquake: A follow-up study. Psychiatry Res. 2017, 253, 318–324. [Google Scholar] [CrossRef]
- Xu, Q.; Fukasawa, M.; Kawakami, N.; Baba, T.; Sakata, K.; Suzuki, R.; Tomita, H.; Nemoto, H.; Yasumura, S.; Yabe, H. Cumulative incidence of suicidal ideation and associated factors among adults living in temporary housing during the three years after the Great East Japan Earthquake. J. Affect. Disord. 2018, 232, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Morishima, R.; Ando, S.; Araki, T.; Usami, S.; Kanehara, A.; Tanaka, S.; Kasai, K. The course of chronic and delayed onset of mental illness and the risk for suicidal ideation after the Great East Japan Earthquake of 2011: A community-based longitudinal study. Psychiatry Res. 2019, 273, 171–177. [Google Scholar] [CrossRef]
- Kawahara, K.; Ushijima, H.; Usami, M.; Takebayashi, M. No Associations of Psychological Symptoms and Suicide Risk with Disaster Experiences in Junior High School Students 5 Years After the 2011 Great East Japan Earthquake and Tsunami. Neuropsychiatr. Dis. Treat. 2020, 16, 2377–2387. [Google Scholar] [CrossRef]
- Kato, K.; Mikami, K.; Kimoto, K.; Kimoto, K.; Takahashi, Y.; Sato, R.; Matsumoto, H. Changes in the frequency and clinical features of suicide attempts in the midwestern area of Kanagawa after the great East Japan earthquake. J. Forensic. Sci. 2014, 59, 417–419. [Google Scholar] [CrossRef] [PubMed]
- Aoki, Y.; Okada, M.; Inokuchi, R.; Matsumoto, A.; Kumada, Y.; Yokoyama, H.; Ishida, T.; Saito, I.; Ito, H.; Sato, H. Time-related changes in suicide attempts after the nuclear accident in Fukushima. Soc. Psychiatry Psychiatr. Epidemiol. 2014, 49, 1911–1918. [Google Scholar] [CrossRef]
- Yoshioka, Y.; Otsuka, K.; Hoshi, K.; Sanjo, K.; Hida, A.; Koizumi, T.; Umetsu, M.; Endo, S.; Sakai, A. Assessing Factors influencing Suicide Attempts Related to the Great East Japan Earthquake. Seishin Igaku 2015, 57, 285–291. (In Japanese) [Google Scholar]
- Ikemoto, K.; Komazawa, D.; Murao, R.; Koyama, A. Mental Health Care after Earthquake Disaster: Clinical Features of Suicidal Attempt Cases Admitted to the Tertiary Emergency Center at the Nearest Heart Hospital in the Fukushima No. 1 Nuclear Power Plant Area. Jpn. J. Gen. Hosp. Psychiatry 2015, 57, 1035–1039. [Google Scholar]
- Yamashita, M.; Kudo, C. How differently we should prepare for the next disaster? Nurs. Health Sci. 2014, 16, 56–59. [Google Scholar] [CrossRef]
- Son, D.; Azami, H.; Hozumi, S.; Hayashi, K. Health Prevention and Psychological Care Project for the 3.11 Earthquake Disaster Victims in Temporary Housing by Primary. J. Jpn. Prim. Care Assoc. 2015, 38, 125–127. (In Japanese) [Google Scholar] [CrossRef]
- Orui, M.; Kuroda, Y.; Yasumura, S. Suicide rates and mental health measures after the lifting of the evacuation orders following the Fukushima Daiichi Nuclear Power Plant accident: A practical report developed in collaboration with the local municipality. Nihon Koshu Eisei Zasshi 2019, 66, 407–416. [Google Scholar] [CrossRef]
- Orui, M.; Harada, S.; Hayashi, M. Disaster Mental Health Team of the Sendai City Mental Health and Welfare Center. Practical Report on Long-term Disaster Mental Health Services Following the Great East Japan Earthquake: Psychological and Social Background of Evacuees in Sendai City in the Mid- to Long-term Post-disaster Period. Disaster Med. Public Health Prep. 2017, 11, 439–450. [Google Scholar] [CrossRef]
- Orui, M.; Saeki, S.; Harada, S.; Hayashi, M. Practical Report of Disaster-Related Mental Health Interventions Following the Great East Japan Earthquake during the COVID-19 Pandemic: Potential for Suicide Prevention. Int. J. Environ. Res. Public Health 2021, 18, 10424. [Google Scholar] [CrossRef]
- Shiragami, K.; Kawano, K.; Masaki, N.; Matoba, Y.; Takeshima, T. Mental health and involvement of residents of the Life Support Advisor in Iwate prefecture after the Great East Japan Earthquake: Suicide prevention in the affected area. J. Ment. Health 2013, 59, 75–83. (In Japanese) [Google Scholar] [CrossRef]
- Ueno, M.; Shibuya, T.; Okamura, K.; Satoh, M. Outreach for people living in the temporary housing by nurses-report of the investigation after 18 months from the Great East Japan Earthquake. J. Grad. Sch. Nurs. Chiba Univ. 2016, 38, 75–80. [Google Scholar]
- Akazawa, M.; Kato, H. Evaluation of the training for supporters in the disaster area-awareness of support for residents and self-care-. Jpn. Bull. Trauma. Stress Stud. 2016, 12, 23–29. (In Japanese) [Google Scholar]
- Orui, M.; Fukasawa, M.; Horikoshi, N.; Suzuki, Y.; Kawakami, N. Development and Evaluation of a Gatekeeper Training Program Regarding Anxiety about Radiation Health Effects Following a Nuclear Power Plant Accident: A Single-Arm Intervention Pilot Trial. Int. J. Environ. Res. Public Health 2020, 17, 4594. [Google Scholar] [CrossRef]
- Shioiri, T.; Nishimura, A.; Nushida, H.; Tatsuno, Y.; Tang, S.W. The Kobe earthquake and reduced suicide rate in Japanese males. Arch. Gen. Psychiatry 1999, 56, 282–283. [Google Scholar] [CrossRef]
- Nishio, A.; Akazawa, K.; Shibuya, F.; Abe, R.; Nushida, H.; Ueno, Y.; Nishimura, A.; Shioiri, T. Influence on the suicide rate two years after a devastating disaster: A report from the 1995 Great Hanshin-Awaji Earthquake. Psychiatry Clin. Neurosci. 2009, 63, 247–250. [Google Scholar] [CrossRef]
- Horney, J.A.; Karaye, I.M.; Abuabara, A.; Gearhart, S.; Grabich, S.; Perez-Patron, M. The Impact of Natural Disasters on Suicide in the United States, 2003–2015. Crisis 2021, 42, 328–334. [Google Scholar] [CrossRef]
- Jahangiri, K.; Yousefi, K.; Mozafari, A.; Sahebi, A. The Prevalence of Suicidal Ideation after the Earthquake: A Systematic Review and Meta-Analysis. Iran J. Public Health 2020, 49, 2330–2338. [Google Scholar] [CrossRef]
- Orui, M.; Suzuki, Y.; Goto, A.; Yasumura, S. Factors Associated with Maintaining the Mental Health of Employees after the Fukushima Nuclear Disaster: Findings from Companies Located in the Evacuation Area. Int. J. Environ. Res. Public Health. 2017, 15, 53. [Google Scholar] [CrossRef] [PubMed]
- Ohira, T.; Hosoya, M.; Yasumura, S.; Satoh, H.; Suzuki, H.; Sakai, A.; Ohtsuru, A.; Kawasaki, Y.; Takahashi, A.; Fukushima Health Management Survey Group. Effect of Evacuation on Body Weight After the Great East Japan Earthquake. Am. J. Prev. Med. 2016, 50, 553–560. [Google Scholar] [CrossRef] [PubMed]
- Murakami, A.; Sasaki, H.; Pascapurnama, D.N.; Egawa, S. Noncommunicable Diseases After the Great East Japan Earthquake: Systematic Review, 2011–2016. Disaster Med. Public Health Prep. 2018, 12, 396–407. [Google Scholar] [CrossRef]
- Ikeda, T.; Aida, J.; Kawachi, I.; Kondo, K.; Osaka, K. Causal effect of deteriorating socioeconomic circumstances on new-onset arthritis and the moderating role of access to medical care: A natural experiment from the 2011 great east Japan earthquake and tsunami. Soc. Sci. Med. 2020, 264, 113385. [Google Scholar] [CrossRef] [PubMed]
- Yokoyama, Y.; Otsuka, K.; Kawakami, N.; Kobayashi, S.; Ogawa, A.; Tannno, K.; Onoda, T.; Yaegashi, Y.; Sakata, K. Mental health and related factors after the Great East Japan earthquake and tsunami. PLoS ONE 2014, 9, e102497. [Google Scholar] [CrossRef]
- Ribeiro, J.D.; Huang, X.; Fox, K.R.; Franklin, J.C. Depression and hopelessness as risk factors for suicide ideation, attempts and death: Meta-analysis of longitudinal studies. Br. J. Psychiatry 2018, 212, 279–286. [Google Scholar] [CrossRef]
- National Institute of Mental Health; National Center of Psychiatry and Neurology. Guidelines for Local Mental Health Care Activities after a Disaster [Translated by JICA: Japan International Cooperation Agency]. Available online: https://saigai-kokoro.ncnp.go.jp/document/pdf/mental_info_guide_en.pdf (accessed on 4 August 2022).

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Orui, M. Suicide and Suicide Prevention Activities Following the Great East Japan Earthquake 2011: A Literature Review. Int. J. Environ. Res. Public Health 2022, 19, 10906. https://doi.org/10.3390/ijerph191710906
Orui M. Suicide and Suicide Prevention Activities Following the Great East Japan Earthquake 2011: A Literature Review. International Journal of Environmental Research and Public Health. 2022; 19(17):10906. https://doi.org/10.3390/ijerph191710906
Chicago/Turabian StyleOrui, Masatsugu. 2022. "Suicide and Suicide Prevention Activities Following the Great East Japan Earthquake 2011: A Literature Review" International Journal of Environmental Research and Public Health 19, no. 17: 10906. https://doi.org/10.3390/ijerph191710906
APA StyleOrui, M. (2022). Suicide and Suicide Prevention Activities Following the Great East Japan Earthquake 2011: A Literature Review. International Journal of Environmental Research and Public Health, 19(17), 10906. https://doi.org/10.3390/ijerph191710906