
Cardiorespiratory Coordination in Collegiate Rowing: A Network Approach to Cardiorespiratory Exercise Testing




Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
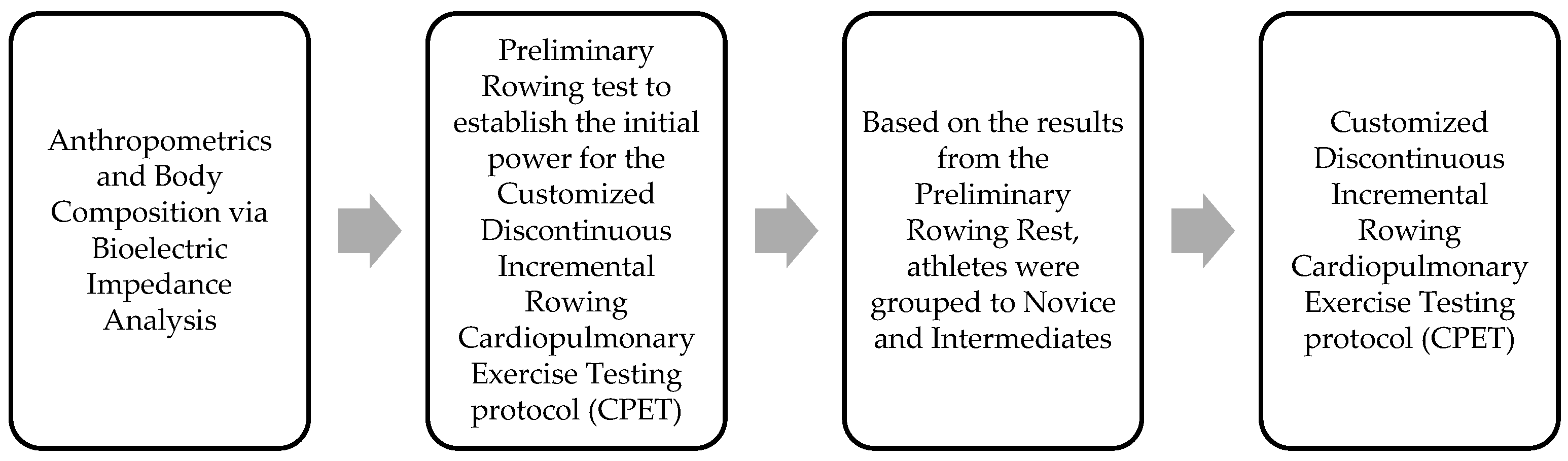
2.2. Procedures
2.2.1. Anthropometrics and Body Composition
2.2.2. Preliminary Customized Discontinuous Incremental Rowing Protocol—Initial Rowing Power
2.2.3. Cardiopulmonary Exercise Testing (CPET) Protocol
2.2.4. Principal Components Analysis (PCA)
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zimmermann, P.; Schoffl, I.; Schoffl, V.; Zimmermann, L.; Eckstein, M.L.; Moser, O.; Wustenfeld, J. Physiological Effects of Training in Elite German Winter Sport Athletes: Sport Specific Remodeling Determined Using Echocardiographic Data and CPET Performance Parameters. J. Cardiovasc. Dev. Dis. 2022, 9, 235. [Google Scholar] [CrossRef] [PubMed]
- Bosquet, L.; Leger, L.; Legros, P. Methods to determine aerobic endurance. Sports Med. 2002, 32, 675–700. [Google Scholar] [CrossRef] [PubMed]
- Van den Tillaar, R.; von Heimburg, E.; Solli, G.S. Comparison of a Traditional Graded Exercise Protocol With a Self-Paced 1-km Test to Assess Maximal Oxygen Consumption. Int. J. Sports Physiol. Perform. 2020, 15, 1334–1339. [Google Scholar] [CrossRef] [PubMed]
- Wiecha, S.; Price, S.; Cieslinski, I.; Kasiak, P.S.; Tota, L.; Ambrozy, T.; Sliz, D. Transferability of Cardiopulmonary Parameters between Treadmill and Cycle Ergometer Testing in Male Triathletes-Prediction Formulae. Int. J. Environ. Res. Public Health 2022, 19, 1830. [Google Scholar] [CrossRef] [PubMed]
- Christle, J.W.; Arena, R. Cardiopulmonary exercise testing and prescription of exercise. In Textbook of Sports and Exercise Cardiology; Springer: Berlin, Germany, 2020; pp. 897–912. [Google Scholar]
- Mazaheri, R.; Tavana, B.; Halabchi, F. Cardiopulmonary Exercise Testing in Athletes; a case-based review. Red 2019, 1009, 5–6. [Google Scholar]
- Balady, G.J.; Arena, R.; Sietsema, K.; Myers, J.; Coke, L.; Fletcher, G.F.; Forman, D.; Franklin, B.; Guazzi, M.; Gulati, M.; et al. Clinician’s Guide to cardiopulmonary exercise testing in adults: A scientific statement from the American Heart Association. Circulation 2010, 122, 191–225. [Google Scholar] [CrossRef] [PubMed]
- Kaminsky, L.A.; Arena, R.; Ellingsen, O.; Harber, M.P.; Myers, J.; Ozemek, C.; Ross, R. Cardiorespiratory fitness and cardiovascular disease—The past, present, and future. Prog. Cardiovasc. Dis. 2019, 62, 86–93. [Google Scholar] [CrossRef] [PubMed]
- Bentley, D.J.; Newell, J.; Bishop, D. Incremental exercise test design and analysis: Implications for performance diagnostics in endurance athletes. Sports Med. 2007, 37, 575–586. [Google Scholar] [CrossRef] [PubMed]
- Hill, A.V.; Long, C.; Lupton, H. Muscular exercise, lactic acid, and the supply and utilisation of oxygen—Parts I–III. Proc. R. Soc. Lond. Ser. B Contain. Pap. A Biol. Character 1924, 96, 438–475. [Google Scholar]
- Pompeu, F.A. Why Pheidippides could not believe in the ‘Central Governor Model’: Popper’s philosophy applied to choose between two exercise physiology theories. Sports Med. Health Sci. 2022, 4, 1–7. [Google Scholar] [CrossRef]
- Kolodziej, F.; O’Halloran, K.D. Re-evaluating the oxidative phenotype: Can endurance exercise save the western world? Antioxidants 2021, 10, 609. [Google Scholar] [CrossRef] [PubMed]
- Martin-Rincon, M.; Calbet, J.A.L. Progress Update and Challenges on VO2max Testing and Interpretation. Front. Physiol. 2020, 11, 1070. [Google Scholar] [CrossRef] [PubMed]
- Lima, T.B.; Santos, T.M.; Damasceno, V.d.O.; Campos, E.Z. Graded and ramp protocols present similar results in apparently healthy subjects. Rev. Bras. De Cineantropometria Desempenho Hum. 2020, 22, e57565. [Google Scholar] [CrossRef]
- Whipp, B.J.; Davis, J.A.; Torres, F.; Wasserman, K. A test to determine parameters of aerobic function during exercise. J. Appl. Physiol. Respir. Environ. Exerc. Physiol. 1981, 50, 217–221. [Google Scholar] [CrossRef] [PubMed]
- Iannetta, D.; Murias, J.M.; Keir, D.A. A Simple Method to Quantify the VO2 Mean Response Time of Ramp-Incremental Exercise. Med. Sci. Sports Exerc. 2019, 51, 1080–1086. [Google Scholar] [CrossRef]
- Lakomy, H.K.; Lakomy, J. Estimation of maximum oxygen uptake from submaximal exercise on a Concept II rowing ergometer. J. Sports Sci. 1993, 11, 227–232. [Google Scholar] [CrossRef]
- Kendall, K.L.; Fukuda, D.H.; Smith, A.E.; Cramer, J.T.; Stout, J.R. Predicting maximal aerobic capacity (VO2max) from the critical velocity test in female collegiate rowers. J. Strength Cond. Res. 2012, 26, 733–738. [Google Scholar] [CrossRef]
- Klusiewicz, A.; Borkowski, L.; Sitkowski, D.; Burkhard-Jagodzinska, K.; Szczepanska, B.; Ladyga, M. Indirect Methods of Assessing Maximal Oxygen Uptake in Rowers: Practical Implications for Evaluating Physical Fitness in a Training Cycle. J. Hum. Kinet. 2016, 50, 187–194. [Google Scholar] [CrossRef]
- Nevill, A.M.; Allen, S.V.; Ingham, S.A. Modelling the determinants of 2000 m rowing ergometer performance: A proportional, curvilinear allometric approach. Scand. J. Med. Sci. Sports 2011, 21, 73–78. [Google Scholar] [CrossRef]
- Mahler, D.A.; Andrea, B.E.; Andresen, D.C. Comparison of 6-min “all-out” and incremental exercise tests in elite oarsmen. Med. Sci. Sports Exerc. 1984, 16, 567–571. [Google Scholar] [CrossRef]
- Pripstein, L.P.; Rhodes, E.C.; McKenzie, D.C.; Coutts, K.D. Aerobic and anaerobic energy during a 2-km race simulation in female rowers. Eur. J. Appl. Physiol. Occup. Physiol. 1999, 79, 491–494. [Google Scholar] [CrossRef] [PubMed]
- Smith, T.B.; Hopkins, W.G. Measures of rowing performance. Sports Med. 2012, 42, 343–358. [Google Scholar] [CrossRef] [PubMed]
- Hahn, A.; Bourdon, P.; Tanner, R. Protocols for the physiological assessment of rowers. In Physiological Tests for Elite Athletes; Human Kinetics: Champaign, IL USA, 2000; pp. 311–326. [Google Scholar]
- Maestu, J.; Jurimae, J.; Jurimae, T. Monitoring of performance and training in rowing. Sports Med. 2005, 35, 597–617. [Google Scholar] [CrossRef] [PubMed]
- Huntsman, H.D.; DiPietro, L.; Drury, D.G.; Miller, T.A. Development of a rowing-specific VO2max field test. J. Strength Cond. Res. 2011, 25, 1774–1779. [Google Scholar] [CrossRef]
- Ingham, S.A.; Whyte, G.P.; Jones, K.; Nevill, A.M. Determinants of 2000 m rowing ergometer performance in elite rowers. Eur. J. Appl. Physiol. 2002, 88, 243–246. [Google Scholar] [CrossRef]
- Secher, N.H.; Vaage, O.; Jensen, K.; Jackson, R.C. Maximal aerobic power in oarsmen. Eur. J. Appl. Physiol. Occup. Physiol. 1983, 51, 155–162. [Google Scholar] [CrossRef]
- Cosgrove, M.J.; Wilson, J.; Watt, D.; Grant, S.F. The relationship between selected physiological variables of rowers and rowing performance as determined by a 2000 m ergometer test. J. Sports Sci. 1999, 17, 845–852. [Google Scholar] [CrossRef]
- Turnes, T.; Possamai, L.T.; Penteado dos Santos, R.; de Aguiar, R.A.; Ribeiro, G.; Caputo, F. Mechanical power during an incremental test can be estimated from 2000-m rowing ergometer performance. J. Sports Med. Phys. Fit. 2019, 60, 214–219. [Google Scholar] [CrossRef]
- Wagner, P.D. Determinants of maximal oxygen transport and utilization. Annu. Rev. Physiol. 1996, 58, 21–50. [Google Scholar] [CrossRef]
- Klusiewicz, A.; Faff, J.; Starczewska-Czapowska, J. Prediction of maximal oxygen uptake from submaximal and maximal exercise on a ski ergometer. Biol. Sport 2011, 28, 31–35. [Google Scholar] [CrossRef][Green Version]
- Hagerman, F.C.; Connors, M.C.; Gault, J.A.; Hagerman, G.R.; Polinski, W.J. Energy expenditure during simulated rowing. J. Appl. Physiol. Respir. Environ. Exerc. Physiol. 1978, 45, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Bourdin, M.; Messonnier, L.; Lacour, J.R. Laboratory blood lactate profile is suited to on water training monitoring in highly trained rowers. J. Sports Med. Phys. Fit. 2004, 44, 337–341. [Google Scholar]
- Messonnier, L.; Freund, H.; Bourdin, M.; Belli, A.; Lacour, J.R. Lactate exchange and removal abilities in rowing performance. Med. Sci. Sports Exerc. 1997, 29, 396–401. [Google Scholar] [CrossRef]
- Steinacker, J.M. Physiological aspects of training in rowing. Int. J. Sports Med. 1993, 14, S3–S10. [Google Scholar] [PubMed]
- Nevill, A.; Brown, D.; Godfrey, R.; Johnson, P.; Romer, L.; Stewart, A.D.; Winter, E.M. Modeling maximum oxygen uptake of elite endurance athletes. Med. Sci. Sports Exerc. 2003, 35, 488–494. [Google Scholar] [CrossRef]
- Egan-Shuttler, J.D.; Edmonds, R.; Eddy, C.; O’Neill, V.; Ives, S.J. Beyond Peak, a Simple Approach to Assess Rowing Power and the Impact of Training: A Technical Report. Int. J. Exerc. Sci. 2019, 12, 233–244. [Google Scholar] [PubMed]
- Treff, G.; Winkert, K.; Steinacker, J. Olympic Rowing—Maximum Capacity over 2000 Meters. Dtsch. Z. Sportmed 2021, 72, 203–211. [Google Scholar] [CrossRef]
- Ingham, S.A.; Pringle, J.S.; Hardman, S.L.; Fudge, B.W.; Richmond, V.L. Comparison of step-wise and ramp-wise incremental rowing exercise tests and 2000-m rowing ergometer performance. Int. J. Sports Physiol. Perform. 2013, 8, 123–129. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Steinacker, J.M.; Lormes, W.; Kellmann, M.; Liu, Y.; Reissnecker, S.; Opitz-Gress, A.; Baller, B.; Gunther, K.; Petersen, K.G.; Kallus, K.W.; et al. Training of junior rowers before world championships. Effects on performance, mood state and selected hormonal and metabolic responses. J. Sports Med. Phys. Fit. 2000, 40, 327–335. [Google Scholar]
- Treff, G.; Winkert, K.; Machus, K.; Steinacker, J.M. Computer-Aided Stroke-by-Stroke Visualization of Actual and Target Power Allows for Continuously Increasing Ramp Tests on Wind-Braked Rowing Ergometers. Int. J. Sports Physiol. Perform. 2018, 13, 729–734. [Google Scholar] [CrossRef] [PubMed]
- Scott, B.R.; Duthie, G.M.; Thornton, H.R.; Dascombe, B.J. Training Monitoring for Resistance Exercise: Theory and Applications. Sports Med. 2016, 46, 687–698. [Google Scholar] [CrossRef] [PubMed]
- Bourdin, M.; Lacour, J.R.; Imbert, C.; Messonnier, L.A. Factors of Rowing Ergometer Performance in High-Level Female Rowers. Int. J. Sports Med. 2017, 38, 1023–1028. [Google Scholar] [CrossRef]
- Coutts, A.J.; Crowcroft, S.; Kempton, T. Developing athlete monitoring systems: Theoretical basis and practical applications. In Recovery and Well-Being in Sport and Exercise; Routledge: London, UK, 2021; pp. 17–31. [Google Scholar]
- Marcora, S.M.; Bosio, A.; de Morree, H.M. Locomotor muscle fatigue increases cardiorespiratory responses and reduces performance during intense cycling exercise independently from metabolic stress. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2008, 294, R874–R883. [Google Scholar] [CrossRef] [PubMed]
- Marcora, S.M.; Staiano, W.; Manning, V. Mental fatigue impairs physical performance in humans. J. Appl. Physiol. 2009, 106, 857–864. [Google Scholar] [CrossRef] [PubMed]
- Chicharro, J.L. Fisiología del Entrenamiento Aeróbico: Una Visión Integrada; Medica Panamericana: Madrid, Spain, 2013; Available online: https://www.medicapanamericana.com/mx/libro/fisiologia-del-entrenamiento-aerobico-incluye-version-digital (accessed on 13 October 2022).
- Muniesa, C.; Diaz, G. Características generales del remo. Deporte cíclico del programa olímpico. Rev. Kronos 2010, 9, 93–100. [Google Scholar]
- Bartsch, R.P.; Liu, K.K.; Bashan, A.; Ivanov, P. Network Physiology: How Organ Systems Dynamically Interact. PLoS ONE 2015, 10, e0142143. [Google Scholar] [CrossRef] [PubMed]
- Ivanov, P.C.; Liu, K.K.L.; Bartsch, R.P. Focus on the emerging new fields of Network Physiology and Network Medicine. New J. Phys. 2016, 18, 100201. [Google Scholar] [CrossRef] [PubMed]
- Balague, N.; Gonzalez, J.; Javierre, C.; Hristovski, R.; Aragones, D.; Alamo, J.; Nino, O.; Ventura, J.L. Cardiorespiratory Coordination after Training and Detraining. A Principal Component Analysis Approach. Front. Physiol. 2016, 7, 35. [Google Scholar] [CrossRef]
- Balague, N.; Hristovski, R.; Almarcha, M.; Garcia-Retortillo, S.; Ivanov, P.C. Network Physiology of Exercise: Vision and Perspectives. Front. Physiol. 2020, 11, 611550. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Retortillo, S.; Rizzo, R.; Wang, J.; Sitges, C.; Ivanov, P.C. Universal spectral profile and dynamic evolution of muscle activation: A hallmark of muscle type and physiological state. J. Appl. Physiol. (1985) 2020, 129, 419–441. [Google Scholar] [CrossRef] [PubMed]
- Ivanov, P.C.; Wang, J.W.; Zhang, X.; Chen, B. The new frontier of Network Physiology: Emerging physiologic states in health and disease from integrated organ network interactions. In 2019-20 MATRIX Annals; Springer: Berlin, Germany, 2021; pp. 237–254. [Google Scholar]
- Ivanov, P.C. The new field of network physiology: Building the human physiolome. Front. Netw. Physiol. 2021, 1, 711778. [Google Scholar] [CrossRef]
- Balagué, N.; Hristovski, R.; Almarcha, M.; Garcia-Retortillo, S.; Ivanov, P.C. Network Physiology of Exercise: Beyond molecular and omics perspectives. Sports Med.-Open 2022, 8, 119. [Google Scholar] [CrossRef] [PubMed]
- Balagué, N.; Garcia-Retortillo, S.; Hristovski, R.; Ivanov, P.C. From Exercise Physiology to Network Physiology of Exercise. In Exercise Physiology; IntechOpen Limited: London, UK, 2022. [Google Scholar] [CrossRef]
- Schulz, S.; Adochiei, F.C.; Edu, I.R.; Schroeder, R.; Costin, H.; Bar, K.J.; Voss, A. Cardiovascular and cardiorespiratory coupling analyses: A review. Philos. Trans. A Math Phys. Eng. Sci. 2013, 371, 20120191. [Google Scholar] [CrossRef] [PubMed]
- Rivera, A.L.; Estanol, B.; Senties-Madrid, H.; Fossion, R.; Toledo-Roy, J.C.; Mendoza-Temis, J.; Morales, I.O.; Landa, E.; Robles-Cabrera, A.; Moreno, R.; et al. Heart Rate and Systolic Blood Pressure Variability in the Time Domain in Patients with Recent and Long-Standing Diabetes Mellitus. PLoS ONE 2016, 11, e0148378. [Google Scholar] [CrossRef] [PubMed]
- Rivera, A.L.; Estañol, B.; Robles-Cabrera, A.; Toledo-Roy, J.C.; Fossion, R.; Frank, A. Looking for biomarkers in physiological time series. In Quantitative Models for Microscopic to Macroscopic Biological Macromolecules and Tissues; Springer: Berlin, Germany, 2018; pp. 111–131. [Google Scholar]
- Barajas-Martínez, A.; Tello-Santoyo, G.; Berumen-Cano, P.; Robles-Cabrera, A.; López-Rivera, J.A.; Fossion, R.; Toledo-Roy, J.C.; Frank, A.; Estañol, B.; Rivera, A.L. Cardio-respiratory variability of healthy young subjects. In AIP Conference Proceedings; AIP Publishing LLC: Melville, NY, USA, 2021; p. 030003. [Google Scholar]
- Esquius, L.; Garcia-Retortillo, S.; Balague, N.; Hristovski, R.; Javierre, C. Physiological- and performance-related effects of acute olive oil supplementation at moderate exercise intensity. J. Int. Soc. Sports Nutr. 2019, 16, 12. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Retortillo, S.; Javierre, C.; Hristovski, R.; Ventura, J.L.; Balague, N. Cardiorespiratory Coordination in Repeated Maximal Exercise. Front. Physiol. 2017, 8, 387. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Retortillo, S.; Javierre, C.; Hristovski, R.; Ventura, J.L.; Balagué, N. Principal component analysis as a novel approach for cardiorespiratory exercise testing evaluation. Physiol. Meas. 2019, 40, 084002. [Google Scholar] [CrossRef]
- Oviedo, G.R.; Garcia-Retortillo, S.; Carbo-Carrete, M.; Guerra-Balic, M.; Balague, N.; Javierre, C.; Guardia-Olmos, J. Cardiorespiratory Coordination during Exercise in Adults with Down Syndrome. Front. Physiol. 2021, 12, 704062. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Retortillo, S.; Gacto, M.; O’Leary, T.J.; Noon, M.; Hristovski, R.; Balague, N.; Morris, M.G. Cardiorespiratory coordination reveals training-specific physiological adaptations. Eur. J. Appl. Physiol. 2019, 119, 1701–1709. [Google Scholar] [CrossRef] [PubMed]
- Haken, H. Information and Self-Organization: A Macroscopic Approach to Complex Systems; Springer Science & Business Media: Berlin, Germany, 2006. [Google Scholar]
- Papadakis, Z.; Garcia-Retortillo, S.; Koutakis, P. Effects of Acute Partial Sleep Deprivation and High-Intensity Interval Exercise on Postprandial Network Interactions. Front. Netw. Physiol. 2022, 2, 869787. [Google Scholar] [CrossRef]
- Muller, A.; Kraemer, J.F.; Penzel, T.; Bonnemeier, H.; Kurths, J.; Wessel, N. Causality in physiological signals. Physiol. Meas. 2016, 37, R46–R72. [Google Scholar] [CrossRef] [PubMed]
- Papadakis, Z.; Forsse, J.S.; Peterson, M.N. Effects of High-Intensity Interval Exercise and Acute Partial Sleep Deprivation on Cardiac Autonomic Modulation. Res. Q Exerc. Sport 2021, 92, 824–842. [Google Scholar] [CrossRef]
- Papadakis, Z.; Forsse, J.S.; Peterson, M.N. Acute partial sleep deprivation and high-intensity interval exercise effects on postprandial endothelial function. Eur. J. Appl. Physiol. 2020, 120, 2431–2444. [Google Scholar] [CrossRef]
- Albouaini, K.; Egred, M.; Alahmar, A.; Wright, D.J. Cardiopulmonary exercise testing and its application. Postgrad. Med. J. 2007, 83, 675–682. [Google Scholar] [CrossRef] [PubMed]
- Mezzani, A. Cardiopulmonary Exercise Testing: Basics of Methodology and Measurements. Ann. Am. Thorac. Soc. 2017, 14, S3–S11. [Google Scholar] [CrossRef] [PubMed]
- Saw, A.E.; Main, L.C.; Gastin, P.B. Monitoring the athlete training response: Subjective self-reported measures trump commonly used objective measures: A systematic review. Br. J. Sports Med. 2016, 50, 281–291. [Google Scholar] [CrossRef]
- Messonnier, L.; Aranda-Berthouze, S.E.; Bourdin, M.; Bredel, Y.; Lacour, J.R. Rowing performance and estimated training load. Int. J. Sports Med. 2005, 26, 376–382. [Google Scholar] [CrossRef] [PubMed]
- Battista, R.A.; Pivarnik, J.M.; Dummer, G.M.; Sauer, N.; Malina, R.M. Comparisons of physical characteristics and performances among female collegiate rowers. J. Sports Sci. 2007, 25, 651–657. [Google Scholar] [CrossRef]
- Les, K.R. Changes in Simulated 2000 Meter Rowing Performance during 4 Years of Intercollegiate Women’s Rowing. Master’s Thesis, University of Connecticut, Storrs, CT, USA, 2011. [Google Scholar]
- Liguori, G.; Medicine, A.C.O.S. ACSM’s Guidelines for Exercise Testing and Prescription; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2020. [Google Scholar]
- Heyward, V. ASEP methods recommendation: Body composition assessment. J. Exerc. Physiol. Online 2001, 4, 4. [Google Scholar]
- Riechman, S.E.; Zoeller, R.F.; Balasekaran, G.; Goss, F.L.; Robertson, R.J. Prediction of 2000 m indoor rowing performance using a 30 s sprint and maximal oxygen uptake. J. Sports Sci. 2002, 20, 681–687. [Google Scholar] [CrossRef] [PubMed]
- Steinacker, J.M.; Marx, T.R.; Marx, U.; Lormes, W. Oxygen consumption and metabolic strain in rowing ergometer exercise. Eur. J. Appl. Physiol. Occup. Physiol. 1986, 55, 240–247. [Google Scholar] [CrossRef] [PubMed]
- Jolicoeur, P. Principal components, factor analysis, and multivariate allometry: A small-sample direction test. Biometrics 1984, 40, 685–690. [Google Scholar] [CrossRef]
- Lang, W.; Zou, H. A simple method to improve principal components regression. Stat 2020, 9, e288. [Google Scholar] [CrossRef]
- Kaufman, A.S. Kaufman Brief Intelligence Test: KBIT; AGS, American Guidance Service: Circle Pines, MN, USA, 1990. [Google Scholar]
- Lakens, D. Calculating and reporting effect sizes to facilitate cumulative science: A practical primer for t-tests and ANOVAs. Front. Psychol. 2013, 4, 863. [Google Scholar] [CrossRef] [PubMed]
- Adams, S.C.; DeLorey, D.S.; Davenport, M.H.; Fairey, A.S.; North, S.; Courneya, K.S. Effects of high-intensity interval training on fatigue and quality of life in testicular cancer survivors. Br. J. Cancer 2018, 118, 1313–1321. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. The earth is round (p < 0.05). In What If There Were No Significance Tests? Psychology Press: London, UK, 2016; pp. 69–82. [Google Scholar]
- Robergs, R.A.; Dwyer, D.; Astorino, T. Recommendations for Improved Data Processing from Expired Gas Analysis Indirect Calorimetry. Sports Med. 2010, 40, 95–111. [Google Scholar] [CrossRef]
- Skinner, J.S.; McLellan, T.M. The transition from aerobic to anaerobic metabolism. Res. Q Exerc. Sport 1980, 51, 234–248. [Google Scholar] [CrossRef] [PubMed]
- Shamailov, B.; Paton, J. Evaluating the physiological significance ofrespiratory sinus arrhythmia: Looking beyond ventilation-perfusionefficiency. J. Physiol. 2012, 590, 1989–2008. [Google Scholar]
- Bartsch, R.P.; Schumann, A.Y.; Kantelhardt, J.W.; Penzel, T.; Ivanov, P. Phase transitions in physiologic coupling. Proc. Natl. Acad. Sci. USA 2012, 109, 10181–10186. [Google Scholar] [CrossRef] [PubMed]
- Bashan, A.; Bartsch, R.P.; Kantelhardt, J.W.; Havlin, S.; Ivanov, P. Network physiology reveals relations between network topology and physiological function. Nat. Commun. 2012, 3, 702. [Google Scholar] [CrossRef]
- Benarroch, E.E. Brainstem integration of arousal, sleep, cardiovascular, and respiratory control. Neurology 2018, 91, 958–966. [Google Scholar] [CrossRef] [PubMed]
- Żebrowska, M.; Garcia-Retortillo, S.; Sikorski, K.; Balagué, N.; Hristovski, R.; Casimiro, J.; Petelczyc, M. Decreased coupling among respiratory variables with effort accumulation. EPL (Europhys. Lett.) 2021, 132, 28001. [Google Scholar] [CrossRef]
- Krivoshchekov, S.G.; Uryumtsev, D.Y.; Gultyaeva, V.V.; Zinchenko, M.I. Cardiorespiratory Coordination in Acute Hypoxia in Runners. Hum. Physiol. 2021, 47, 429–437. [Google Scholar] [CrossRef]
- Zinner, C.; Morales-Alamo, D.; Ørtenblad, N.; Larsen, F.J.; Schiffer, T.A.; Willis, S.J.; Gelabert-Rebato, M.; Perez-Valera, M.; Boushel, R.; Calbet, J.A. The physiological mechanisms of performance enhancement with sprint interval training differ between the upper and lower extremities in humans. Front. Physiol. 2016, 7, 426. [Google Scholar] [CrossRef]
- Saltin, B.; Calbet, J.A. Point: In health and in a normoxic environment, VO2max is limited primarily by cardiac output and locomotor muscle blood flow. J. Appl. Physiol. 2006, 100, 744–748. [Google Scholar] [CrossRef] [PubMed]
- Skattebo, O.; Calbet, J.A.L.; Rud, B.; Capelli, C.; Hallen, J. Contribution of oxygen extraction fraction to maximal oxygen uptake in healthy young men. Acta Physiol. 2020, 230, e13486. [Google Scholar] [CrossRef] [PubMed]
- Skattebo, O.; Capelli, C.; Rud, B.; Auensen, M.; Calbet, J.A.L.; Hallen, J. Increased oxygen extraction and mitochondrial protein expression after small muscle mass endurance training. Scand. J. Med. Sci. Sports 2020, 30, 1615–1631. [Google Scholar] [CrossRef]
- Kelso, J.S. Dynamic Patterns: The Self-Organization of Brain and Behavior; MIT press: Cambridge, MA, USA, 1995. [Google Scholar]
- Latash, M.L. Synergy; Oxford University Press: Oxford, UK, 2008. [Google Scholar]
- Bonafiglia, J.T.; Rotundo, M.P.; Whittall, J.P.; Scribbans, T.D.; Graham, R.B.; Gurd, B.J. Inter-Individual Variability in the Adaptive Responses to Endurance and Sprint Interval Training: A Randomized Crossover Study. PLoS ONE 2016, 11, e0167790. [Google Scholar] [CrossRef]
- Astorino, T.A.; deRevere, J.; Anderson, T.; Kellogg, E.; Holstrom, P.; Ring, S.; Ghaseb, N. Change in VO2max and time trial performance in response to high-intensity interval training prescribed using ventilatory threshold. Eur. J. Appl. Physiol. 2018, 118, 1811–1820. [Google Scholar] [CrossRef]
- Edvardsen, E.; Hem, E.; Anderssen, S.A. End criteria for reaching maximal oxygen uptake must be strict and adjusted to sex and age: A cross-sectional study. PLoS ONE 2014, 9, e85276. [Google Scholar] [CrossRef]
- Beltz, N.M.; Gibson, A.L.; Janot, J.M.; Kravitz, L.; Mermier, C.M.; Dalleck, L.C. Graded Exercise Testing Protocols for the Determination of VO2max: Historical Perspectives, Progress, and Future Considerations. J. Sports Med. 2016, 2016, 3968393. [Google Scholar] [CrossRef]
- Ward, S.A. Physiology of breathing II. Surgery 2004, 22, 230–234. [Google Scholar] [CrossRef]
- Tenenbaum, J.B.; de Silva, V.; Langford, J.C. A global geometric framework for nonlinear dimensionality reduction. Science 2000, 290, 2319–2323. [Google Scholar] [CrossRef] [PubMed]
- Liao, J.C.; Boscolo, R.; Yang, Y.L.; Tran, L.M.; Sabatti, C.; Roychowdhury, V.P. Network component analysis: Reconstruction of regulatory signals in biological systems. Proc. Natl. Acad. Sci. USA 2003, 100, 15522–15527. [Google Scholar] [CrossRef] [PubMed]
- Bartsch, R.P.; Liu, K.K.; Ma, Q.D.; Ivanov, P.C. Three Independent Forms of Cardio-Respiratory Coupling: Transitions across Sleep Stages. Comput. Cardiol. 2014, 41, 781–784. [Google Scholar]


{kind=link}
| Age | BW (kg) | Height (cm) | BF (%) | |
|---|---|---|---|---|
| N | 18 | 18 | 18 | 18 |
| Mean | 20.17 | 70.89 | 170.17 | 22.01 |
| Standard deviation | 2.28 | 16.54 | 6.97 | 5.85 |
| Minimum | 18 | 47.50 | 159.50 | 12.30 |
| Maximum | 25 | 117.90 | 183.00 | 34.10 |
| Novice Rowers | Intermediate Rowers | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ID | VO2max (mL/kg/min) | VE | HR | FeO2 | FeCO2 | #PC | ID | VO2max (mL/kg/min) | VE | HR | FeO2 | FeCO2 | #PC |
| 1 | 45.1 | 0.87 | 0.93 | 0.78 | 0.91 | 1 | 10 | 32.6 | 0.79 | 0.80 | 0.77 | 0.90 | 1 |
| 2 | 45.1 | 0.17 | 0.01 | 0.97 | 0.95 | 2 | 11 | 50.2 | 0.89 | 0.48 | 0.82 | 0.96 | 1 |
| 3 | 41 | 0.69 | 0.87 | 0.78 | 0.90 | 1 | 12 | 38.5 | 0.94 | 0.89 | 0.71 | 0.08 | 2 |
| 4 | 40.8 | 0.96 | 0.92 | 0.03 | 0.63 | 2 | 13 | 45.7 | 0.78 | 0.67 | 0.80 | 0.94 | 1 |
| 5 | 34.9 | 0.07 | 0.08 | 0.97 | 0.96 | 2 | 14 | 46.4 | 0.86 | 0.87 | 0.64 | 0.91 | 1 |
| 6 | 54.4 | 0.92 | 0.89 | 0.13 | 0.50 | 2 | 15 | 48.3 | 0.83 | 0.88 | 0.61 | 0.95 | 1 |
| 7 | 25.2 | 0.94 | 0.89 | 0.15 | 0.46 | 2 | 16 | 47.4 | 0.84 | 0.50 | 0.90 | 0.92 | 1 |
| 8 | 41 | 0.88 | 0.03 | 0.96 | 0.98 | 2 | 17 | 41.8 | 0.84 | 0.90 | 0.69 | 0.91 | 1 |
| 9 | 43.3 | 0.72 | 0.68 | 0.87 | 0.93 | 1 | 18 | 54.2 | 0.93 | 0.94 | 0.17 | 0.48 | 2 |
| Mean | 0.69 | 0.59 | 0.63 | 0.80 | Mean | 0.86 | 0.77 | 0.68 | 0.78 | ||||
| SD | 0.34 | 0.42 | 0.40 | 0.21 | SD | 0.06 | 0.18 | 0.21 | 0.30 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Papadakis, Z.; Etchebaster, M.; Garcia-Retortillo, S. Cardiorespiratory Coordination in Collegiate Rowing: A Network Approach to Cardiorespiratory Exercise Testing. Int. J. Environ. Res. Public Health 2022, 19, 13250. https://doi.org/10.3390/ijerph192013250
Papadakis Z, Etchebaster M, Garcia-Retortillo S. Cardiorespiratory Coordination in Collegiate Rowing: A Network Approach to Cardiorespiratory Exercise Testing. International Journal of Environmental Research and Public Health. 2022; 19(20):13250. https://doi.org/10.3390/ijerph192013250
Chicago/Turabian StylePapadakis, Zacharias, Michelle Etchebaster, and Sergi Garcia-Retortillo. 2022. "Cardiorespiratory Coordination in Collegiate Rowing: A Network Approach to Cardiorespiratory Exercise Testing" International Journal of Environmental Research and Public Health 19, no. 20: 13250. https://doi.org/10.3390/ijerph192013250
APA StylePapadakis, Z., Etchebaster, M., & Garcia-Retortillo, S. (2022). Cardiorespiratory Coordination in Collegiate Rowing: A Network Approach to Cardiorespiratory Exercise Testing. International Journal of Environmental Research and Public Health, 19(20), 13250. https://doi.org/10.3390/ijerph192013250