
Hand-to-Face Contact of Preschoolers during Indoor Activities in Childcare Facilities in the Republic of Korea


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Videotaping and Data Collection
2.3. Definition of Terms
2.4. Data Analysis
2.5. Ethical Considerations
3. Results
3.1. General Characteristics of the Participants and Their Parents
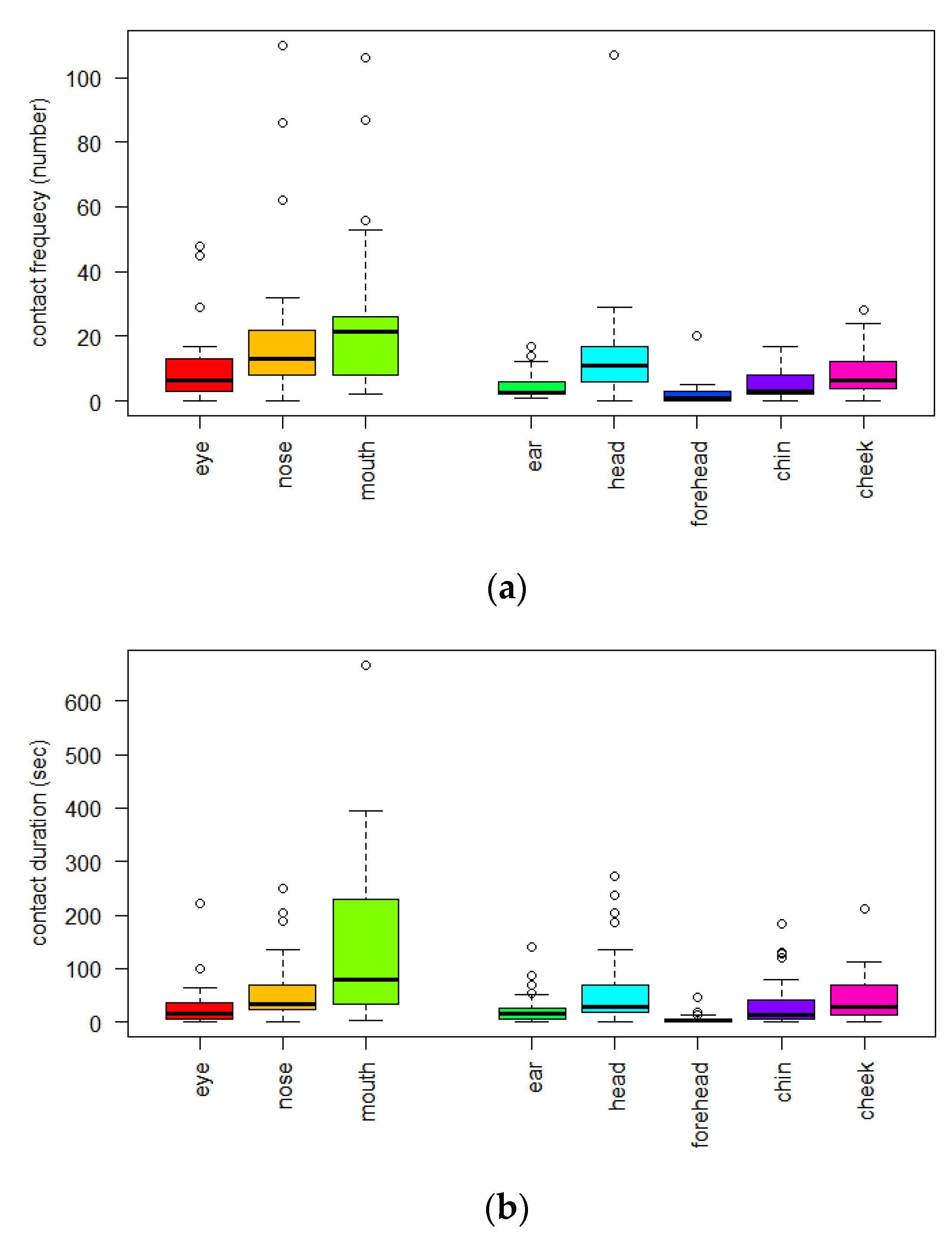
3.2. Descriptive Statistics of Frequency and Duration for Hand-to-Face Contact
3.3. Density Distribution of Frequency and Duration for Hand-to-Face Contact by Gender
3.4. Differences in CF and CD by the Child’s Age and Gender
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Guidelines on Hand Hygiene in Health Care: First Global Patient Safety Challenge Clean Care Is Safer Care; WHO: Geneva, Switzerland, 2009. [Google Scholar]
- Van Vonderen, J.J.; Stol, K.; Buddingh, E.P.; van der Kaay, D.C. Herpes simplex transmission to chest and face through autoinoculation in an infant. BMJ Case Rep. 2017, 2017, bcr2017220447. [Google Scholar] [CrossRef] [PubMed]
- Fukunaka, Y.; Sawada, S.S.; Nishiura, C.; Noguchi, J.; Tsukamoto, K.; Otsuji, Y.; Marui, E. Susceptibility to upper respiratory tract infection and touching of the eyes or nose: A cross-sectional study of Japanese workers. J. Occup. Health 2013, 55, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Kwok, Y.L.; Gralton, J.; McLaws, M.L. Face touching: A frequent habit that has implications for hand hygiene. Am. J. Infect. Control. 2015, 43, 112–114. [Google Scholar] [CrossRef] [PubMed]
- Nicas, M.; Best, D. A study quantifying the hand-to-face contact rate and its potential application to predicting respiratory tract infection. J. Occup. Environ. Hyg. 2008, 5, 347–352. [Google Scholar] [CrossRef]
- Erdozain, G.; KuKanich, K.; Chapman, B.; Powell, D. Observation of public health risk behaviours, risk communication and hand hygiene at Kansas and Missouri petting zoos—2010–2011. Zoonoses Public Health 2013, 60, 304–310. [Google Scholar] [CrossRef]
- Furuya, H. Prediction of potential respiratory tract infection from SARS-CoV-2 through hand-to-face contact transmission. Tokai J. Exp. Clin. Med. 2020, 45, 170–175. [Google Scholar]
- Carrillo-Díaz, M.; Lacomba-Trejo, L.; Romero-Maroto, M.; González-Olmo, M.J. Facial self-touching and the propagation of COVID-19: The role of gloves in the dental practice. Int. J. Environ. Res. Public Health 2021, 18, 6983. [Google Scholar] [CrossRef]
- Rahman, J.; Mumin, J.; Fakhruddin, B. How frequently do we touch facial T-Zone: A systematic review. Ann. Glob. Health 2020, 86, 75. [Google Scholar] [CrossRef]
- Heinicke, M.R.; Stiede, J.T.; Miltenberger, R.G.; Woods, D.W. Reducing risky behavior with habit reversal: A review of behavioral strategies to reduce habitual hand-to-head behavior. J. Appl. Behav. Anal. 2020, 53, 1225–1236. [Google Scholar] [CrossRef]
- Tsou, M.C.; Ozkaynak, H.; Beamer, P.; Dang, W.; Hsi, H.C.; Jiang, C.B.; Chien, L.C. Mouthing activity data for children aged 7 to 35 months in Taiwan. J. Expo. Sci. Environ. Epidemiol. 2015, 25, 388–398. [Google Scholar] [CrossRef]
- Xue, J.; Zartarian, V.; Moya, J.; Freeman, N.; Beamer, P.; Black, K.; Tulve, N.; Shalat, S. A meta-analysis of children’s hand-to-mouth frequency data for estimating nondietary ingestion exposure. Risk Anal. 2007, 27, 411–420. [Google Scholar] [CrossRef] [PubMed]
- Wilson, A.M.; Verhougstraete, M.P.; Beamer, P.I.; King, M.F.; Reynolds, K.A.; Gerba, C.P. Frequency of hand-to-head, -mouth, -eyes, and -nose contacts for adults and children during eating and non-eating macro-activities. J. Expo. Sci. Environ. Epidemiol. 2021, 31, 34–44. [Google Scholar] [CrossRef] [PubMed]
- KOSIS. Daycare Center and User Statistics 2019; KOSIS: Daejeon, Korea, 2019. [Google Scholar]
- Chan, J.H.; Law, C.K.; Hamblion, E.; Fung, H.; Rudge, J. Best practices to prevent transmission and control outbreaks of hand, foot, and mouth disease in childcare facilities: A systematic review. Hong Kong Med. J. 2017, 23, 177–190. [Google Scholar] [CrossRef] [PubMed]
- Oh, H.S.; Jeong, S.Y.; Ryu, M.; Yang, Y. An observational study of hand-to-face contact via videotaping of Korean older people in daily life settings. Int. J. Older People Nurs. 2022, 17, e12414. [Google Scholar] [CrossRef] [PubMed]
- Garland, A.F.; Deyessa, N.; Desta, M.; Alem, A.; Zerihun, T.; Hall, K.G.; Goren, N.; Fish, I. Use of the WHO’s Perceived Well-Being Index (WHO-5) as an efficient and potentially valid screen for depression in a low income country. Fam. Syst. Health 2018, 36, 148. [Google Scholar] [CrossRef] [PubMed]
- Kwong, L.H.; Ercumen, A.; Pickering, A.J.; Unicomb, L.; Davis, J.; Luby, S.P. Age-related changes to environmental exposure: Variation in the frequency that young children place hands and objects in their mouths. J. Expo. Sci. Environ. Epidemiol. 2020, 30, 205–216. [Google Scholar] [CrossRef] [PubMed]
- Tsou, M.C.; Ozkaynak, H.; Beamer, P.; Dang, W.; Hsi, H.C.; Jiang, C.B.; Chien, L.C. Mouthing activity data for children age 3 to <6 years old and fraction of hand area mouthed for children age <6 years old in Taiwan. J. Expo. Sci. Environ. Epidemiol. 2018, 28, 182–192. [Google Scholar] [CrossRef]
- Oh, H.S.; Ryu, M.; Yang, Y. Hand-to-face contact behaviors during indoor activities in daily life among Korean adults: An observational pilot study using videotaping. Epidemiol. Health 2021, 43, e2021030. [Google Scholar] [CrossRef]
- Black, K.; Shalat, S.L.; Freeman, N.C.; Jimenez, M.; Donnelly, K.C.; Calvin, J.A. Children’s mouthing and food-handling behavior in an agricultural community on the US/Mexico border. J. Expo. Anal. Environ. Epidemiol. 2005, 15, 244–251. [Google Scholar] [CrossRef]
- Kwong, L.H.; Ercumen, A.; Pickering, A.J.; Unicomb, L.; Davis, J.; Luby, S.P. Hand- and Object-Mouthing of Rural Bangladeshi Children 3–18 Months Old. Int. J. Environ. Res. Public Health 2016, 13, 563. [Google Scholar] [CrossRef]
- Jepsen, M.T.; Trebbien, R.; Emborg, H.D.; Krause, T.G.; Schonning, K.; Voldstedlund, M.; Nielsen, J.; Fischer, T.K. Incidence and seasonality of respiratory syncytial virus hospitalisations in young children in Denmark, 2010 to 2015. Eurosurveillance 2018, 23, 17-00163. [Google Scholar] [CrossRef] [PubMed]
- Brazo-Sayavera, J.; Aubert, S.; Barnes, J.D.; González, S.A.; Tremblay, M.S. Gender differences in physical activity and sedentary behavior: Results from over 200,000 Latin-American children and adolescents. PLoS ONE 2021, 16, e0255353. [Google Scholar] [CrossRef] [PubMed]
- Morrongiello, B.A.; Corbett, M.; Stewart, J. Understanding sex differences in children’s injury risk as pedestrians. J. Pediatr. Psychol. 2020, 45, 1144–1152. [Google Scholar] [CrossRef] [PubMed]
- How to Protect Yourself & Others. Available online: https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/prevention.html (accessed on 9 August 2022).
- Demographic Trends of COVID-19 Cases and Deaths in the US Reported to CDC. Available online: https://covid.cdc.gov/covid-data-tracker/#demographics (accessed on 9 August 2022).
- Lopez, A.S.; Hill, M.; Antezano, J.; Vilven, D.; Rutner, T.; Bogdanow, L.; Claflin, C.; Kracalik, I.T.; Fields, V.L.; Dunn, A.; et al. Transmission Dynamics of COVID-19 Outbreaks Associated with Child Care Facilities—Salt Lake City, Utah, April–July 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 1319–1323. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Classification | Number of Participants n (%) or Mean ± SD |
|---|---|---|
| 30 | ||
| Age of children (month) | 53.1 ± 13.7 | |
| 13–36 | 3 (10.0) | |
| 37–60 | 21 (70.0) | |
| 61–84 | 6 (20.0) | |
| Gender of child | ||
| Boy | 17 (56.7) | |
| Girl | 13 (43.3) | |
| Number of people living together | 3.7 ± 0.7 | |
| ≤3 | 11 (36.7) | |
| >4 | 19 (63.3) | |
| Residential area | ||
| Seoul | 16 (53.3) | |
| Gyeonggi-do | 14 (46.7) | |
| Child’s parents Age (year) | 37.0 ± 3.7 | |
| 25–39 | 21 (70.0) | |
| 40–49 | 9 (30.0) | |
| Education | ||
| High school | 2 (6.7) | |
| College/University | 22 (73.3) | |
| Graduate school | 6 (20.0) | |
| Employment status | ||
| No | 18 (60.0) | |
| Yes | 12 (40.0) | |
| Type of work | ||
| Permanent employee | 8 (26.7) | |
| Part-time work | 4 (13.3) | |
| Unemployed, including housewife | 18 (60.0) | |
| Household income (won) | ||
| ≤4 million | 15 (50.0) | |
| >4 million | 15 (50.0) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oh, H.S.; Ryu, M. Hand-to-Face Contact of Preschoolers during Indoor Activities in Childcare Facilities in the Republic of Korea. Int. J. Environ. Res. Public Health 2022, 19, 13282. https://doi.org/10.3390/ijerph192013282
Oh HS, Ryu M. Hand-to-Face Contact of Preschoolers during Indoor Activities in Childcare Facilities in the Republic of Korea. International Journal of Environmental Research and Public Health. 2022; 19(20):13282. https://doi.org/10.3390/ijerph192013282
Chicago/Turabian StyleOh, Hyang Soon, and Mikyung Ryu. 2022. "Hand-to-Face Contact of Preschoolers during Indoor Activities in Childcare Facilities in the Republic of Korea" International Journal of Environmental Research and Public Health 19, no. 20: 13282. https://doi.org/10.3390/ijerph192013282
APA StyleOh, H. S., & Ryu, M. (2022). Hand-to-Face Contact of Preschoolers during Indoor Activities in Childcare Facilities in the Republic of Korea. International Journal of Environmental Research and Public Health, 19(20), 13282. https://doi.org/10.3390/ijerph192013282