

Mediterranean Diet versus Very Low-Calorie Ketogenic Diet: Effects of Reaching 5% Body Weight Loss on Body Composition in Subjects with Overweight and with Obesity—A Cohort Study

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
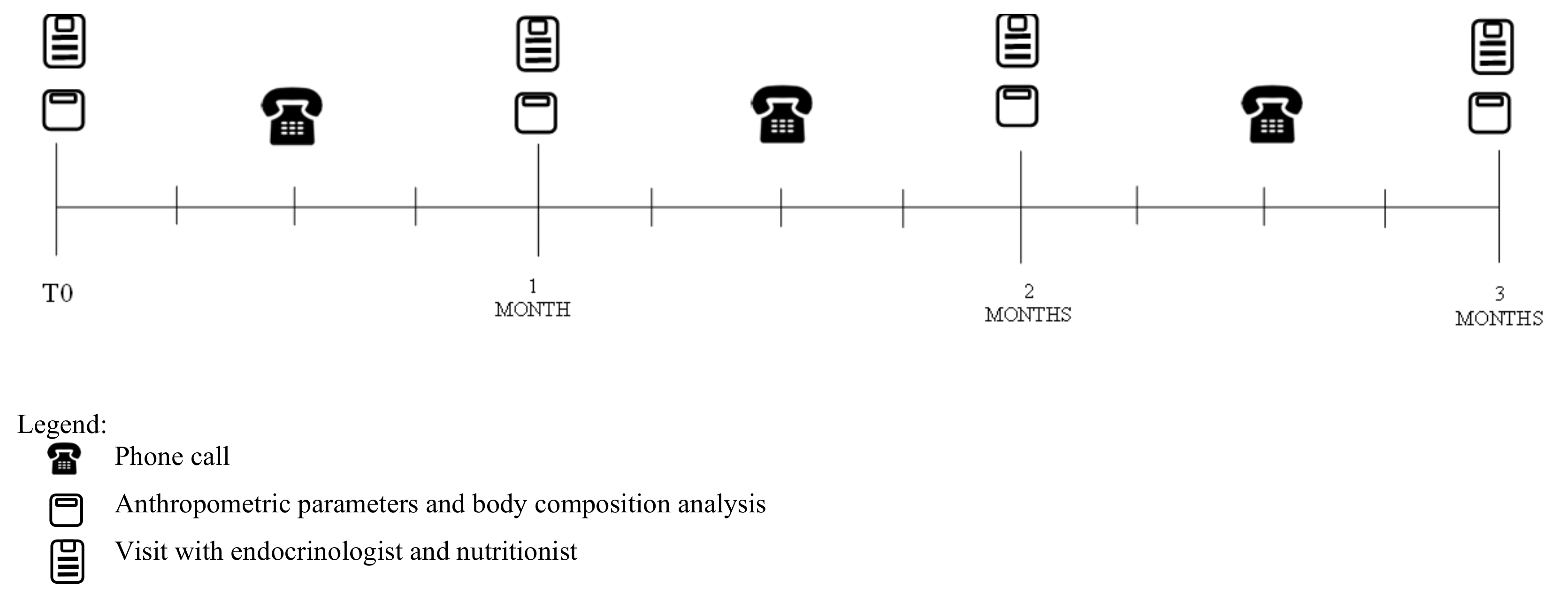
2.2. Study Protocol
2.3. Anthropometric Parameters
2.4. Body Composition Analysis
2.5. Nutritional Protocols
2.5.1. Mediterranean Diet
2.5.2. Very Low-Calorie Ketogenic Diet
2.6. Statistical Analysis
3. Results
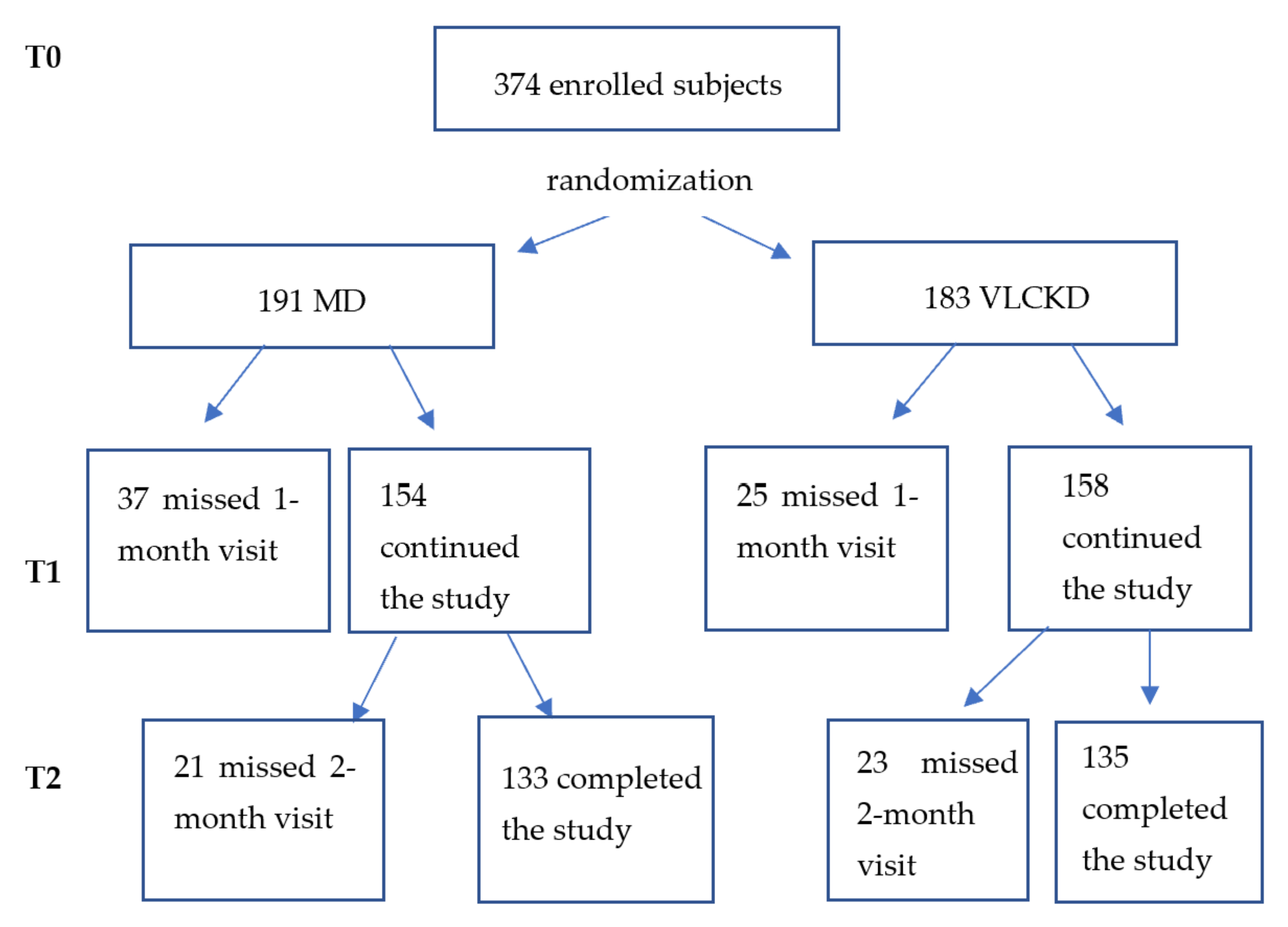
3.1. Study Population
3.2. Results on Anthropometric Parameters and Body Composition
3.3. Subgroups Evaluation: Age and BMI
3.3.1. Age
3.3.2. BMI
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Yu, W.; Rohli, K.E.; Yang, S.; Jia, P. Impact of obesity on COVID-19 patients. J. Diabetes Complicat. 2021, 35, 107817. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Obesity and Overweight Fact Sheet; WHO: Geneva, Switzerland, 2018. [Google Scholar]
- Batch, J.T.; Lamsal, S.P.; Adkins, M.; Sultan, S.; Ramirez, M.N. Advantages and Disadvantages of the Ketogenic Diet: A Review Article. Cureus 2020, 12, e9639. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. PASSI Surveillance System. 2019. Available online: https://www.epicentro.iss.it/passi/dati/sovrappeso?tab-container-1=tab1 (accessed on 9 March 2022).
- WHO Consultation on Obesity; World Health Organization. Obesity: Preventing and Managing the Global Epidemic: Report of a WHO Consultation; WHO Technical Report Series; World Health Organization: Geneva, Switzerland, 2000; Volume 894, 252. [Google Scholar]
- Varkevisser, R.D.M.; Van Stralen, M.M.; Kroeze, W.; Ket, J.C.F.; Steenhuis, H.M. Determinants of weight loss maintenance: A systematic review. Obes. Rev. 2019, 20, 171–211. [Google Scholar] [CrossRef] [PubMed]
- Magkos, F.; Fraterrigo, G.; Yoshino, J.; Luecking, C.; Kirbach, K.; Kelly, S.C.; de las Fuentes, L.; He, S.; Okunade, A.L.; Patterson, B.W.; et al. Effects of moderate and subsequent progressive weight loss on metabolic function and adipose tissue biology in humans with obesity. Cell Metab. 2016, 23, 591–601. [Google Scholar] [CrossRef]
- Standard Italiani per la Cura Dell’obesità SIO—ADI 2016–2017; Società Italiana dell’Obesità: Milan, Italy, 2017.
- Kushner, R. Obesity 2021: Current clinical management of a chronic serious disease. Supplement to the journal of family practice. J. Fam. Pract. 2021, 70, S35–S40. [Google Scholar]
- Wing, R.R.; Lang, W.; Wadden, T.A.; Safford, M.; Knowler, W.C.; Bertoni, A.G.; Hill, J.O.; Brancati, F.L.; Peters, A.; Wagenknecht, L.; et al. Benefit of modest weight loss in improving cardiovascular risk factors in overweight and obese individuals with type 2 diabetes. Diabetes Care 2011, 34, 1481–1486. [Google Scholar] [CrossRef]
- Paoli, A.; Bianco, A.; Grimaldi, K.A.; Lodi, A.; Bosco, G. Long term successful weight loss with a combination biphasic ketogenic Mediterranean diet and Mediterranean diet maintenance protocol. Nutrients 2013, 5, 5205–5217. [Google Scholar] [CrossRef]
- Di Rosa, C.; Lattanzi, G.; Taylor, S.F.; Manfrini, S.; Khazrai, Y.M. Very low—Calorie ketogenic diets in overweight and obesity treatment: Effects on anthropometric parameters, body composition, satiety, lipid profile and microbiota. Obes. Res. Clin. Pract. 2020, 14, 491–503. [Google Scholar] [CrossRef]
- Kim, J.Y. Optimal Diet Strategies for Weight Loss and Weight Loss Maintenance. J. Obes. Metab. Syndr. 2021, 30, 20–31. [Google Scholar] [CrossRef]
- Muscogiuri, G.; El Goch, M.; Colao, A.; Hassapidou, M.; Yumuk, V.; Busetto, L. Obesity Management Task Force (OMTF) of the European Association for the study of Obesity (EASO) European Guidelines for Obesity Management in Adults with a Very Low-Calorie Ketogenic Diet: A Systematic Review and Meta-Analysis. Obes. Facts 2021, 14, 222–245. [Google Scholar] [CrossRef]
- Castellana, M.; Conte, E.; Cignarelli, A.; Perrini, S.; Giustina, A.; Giovanella, L.; Giorgino, F.; Trimboli, P. Efficacy and safety of very low—Calorie ketogenic diet (VLCKD) in patients with overweight and obesity: A systematic review and meta-analysis. Rev. Endocr. Metab. Disord. 2019, 21, 5–16. [Google Scholar] [CrossRef] [PubMed]
- Masood, W.; Annamaraju, P.; Uppaluri, K.R. Ketogenic Diet; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Serra-Majem, L.; Tomaino, L.; Dernini, S.; Berry, E.M.; Lairon, D.; de la Cruz, J.N.; Bach-Faig, A.; Donini, L.M.; Medina, F.X.; Belahsen, R.; et al. Updating the Mediterranean Diet Pyramid towards sustainability: Focus on environmental concerns. Int. J. Environ. Res. Public Health 2020, 17, 8758. [Google Scholar] [CrossRef] [PubMed]
- Landry, M.J.; Crimarco, A.; Perelman, D.; Lindsay, R.D.; Petlura, C.; Aronica, L.; Robinson, J.L.; Kim, S.H.; Gardner, D. Adherence to Ketogenic and Mediterranean Study Diets in a Crossover Trial: The Keto—Med Randomized Trial. Nutrients 2021, 13, 967. [Google Scholar] [CrossRef] [PubMed]
- Keys, A.B. How to Eat Well and Stay Well the Mediterranean Way; Doubleday: Garden City, NY, USA, 1975; p. 488. [Google Scholar]
- Bach-Faig, A.; Berry, E.M.; Lairon, D.; Reguant, J.; Trichopoulou, A.; Dernini, S.; Medina, F.X.; Battino, M.; Belahsen, R.; Miranda, G.; et al. Mediterranean diet pyramid today. Science and cultural updates. Public Health Nutr. 2011, 14, 2274–2284. [Google Scholar] [CrossRef]
- Diolintzi, A.; Panagiotakos, D.B.; Sidossis, L.S. From Mediterranean diet to Mediterranean lifestyle: A narrative review. Public Health Nutr. 2019, 22, 2703–2713. [Google Scholar] [CrossRef]
- Schroder, H. Protective mechanisms of the Mediterranean diet in obesity and type 2 diabetes. J. Nutr. Biochem. 2007, 18, 149–160. [Google Scholar] [CrossRef]
- Willett, W.C.; Leibel, R.L. Dietary fat is not a major determinant of body fat. Am. J. Med. 2002, 113 (Suppl. 9B), 47S–59S. [Google Scholar] [CrossRef]
- Mancini, J.G.; Filion, K.B.; Atallah, R.; Eisenberg, M.J. Systematic review of the Mediterranean diet for long-term weight loss. Am. J. Med. 2016, 129, 407–415. [Google Scholar] [CrossRef]
- Cheskin, L.J.; Kahan, S. Low-carbohydrate and Mediterranean diets led to greater weight loss than a low-fat diet in moderately obese adults. EBM 2008, 13, 6. [Google Scholar] [CrossRef]
- Keys, A.; Menotti, A.; Karvonen, M.J.; Aravanis, C.; Blackburn, H.; Buzina, R.; Djordjevic, B.S.; Dontas, A.S.; Fidanza, F.; Keys, M.H.; et al. The diet and 15-year death rate in the seven countries study. Am. J. Epidemiol. 1986, 124, 903–915. [Google Scholar] [CrossRef]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary prevention of cardiovascular disease with a Mediterranean diet. Supplemented with Extra-Virgin Olive Oil or Nuts. N. Engl. J. Med. 2018, 378, e34. [Google Scholar] [CrossRef]
- Dinu, M.; Pagliai, G.; Casini, A.; Sofi, F. Mediterranean diet and multiple health outcomes: An umbrella review of meta-analyses of observational studies and randomised trials. Eur. J. Clin. Nutr. 2018, 72, 30–43. [Google Scholar] [CrossRef]
- Muscogiuri, G.; Barrea, L.; Laudisio, D.; Pugliese, G.; Salzano, C.; Savastano, S.; Colao, A. The management of very low-calorie ketogenic diet in obesity outpatient clinic: A practical guide. J. Transl. Med. 2019, 17, 356. [Google Scholar] [CrossRef]
- Trimboli, P.; Castellana, M.; Bellido, D.; Casanueva, F.F. Confusion in the nomenclature of ketogenic diets blurs evidence. Rev. Endocr. Metab. Disord. 2020, 21, 1–3. [Google Scholar] [CrossRef]
- Krebs, H.A. The regulation of the release of ketone bodies by the liver. Adv. Enzym. Regul. 1966, 4, 339–354. [Google Scholar] [CrossRef]
- Caprio, M.; Infante, M.; Moriconi, E.; Armani, A.; Fabbri, A.; Mantovani, G.; Mariani, S.; Lubrano, C.; Poggiogalle, E.; Migliaccio, S.; et al. Very-low-calorie ketogenic diet (VLCKD) in the management of metabolic diseases: Systematic review and consensus statement from the Italian Society of Endocrinology (SIE). J. Endocrinol. Investig. 2019, 45, 1365–1386. [Google Scholar] [CrossRef]
- Spera, G.; Mariani, S. Diete chetogeniche: Ruolo nel trattamento di sovrappeso e obesità. L’endocrinologo 2017, 18, 285–290. [Google Scholar] [CrossRef]
- Moreno, B.; Bellido, D.; Sajoux, I.; Goday, A.; Saavedra, D.; Crujeiras, A.B.; Casanueva, F.F. Comparison of a very low-calorie-ketogenic diet with a standard low-calorie diet in the treatment of obesity. Endocrine 2014, 47, 793–805. [Google Scholar] [CrossRef]
- Moreno, B.; Crujeiras, A.B.; Bellido, D.; Sajoux, I.; Casanueva, F.F. Obesity treatment by very low-calorie-ketogenic diet at two years: Reduction in visceral fat and on the burden of disease. Endocrine 2016, 54, 681–690. [Google Scholar] [CrossRef]
- Castro, A.I.; Gomez-Arbelaez, D.; Crujeiras, A.B.; Granero, R.; Aguera, Z.; Jimenez-Murcia, S.; Sajoux, I.; Lopez-Jaramillo, P.; Fernandez-Aranda, F.; Casanueva, F.F. Effect of a very low-calorie ketogenic diet on food and alcohol cravings physical and sexual activity, sleep disturbances, and quality of life in obese patients. Nutrients 2018, 10, 1348. [Google Scholar] [CrossRef]
- Gomez-Arbelaez, D.; Bellido, D.; Castro, A.I.; Ordoñez-Mayan, L.; Carreira, J.; Galban, C.; Martinez-Olmos, M.A.; Crujeiras, A.B.; Sajoux, I.; Casanueva, F.F. Body composition changes after very low-calorie- ketogenic diet in obesity evaluated by three standardized methods. J. Clin. Endocrinol. Metab. 2016, 102, 488–498. [Google Scholar] [CrossRef]
- Waist Circumference and Waist-Hip Ratio: Report of a WHO Expert Consultation. 2008. Available online: https://www.who.int/publications/i/item/9789241501491 (accessed on 13 September 2022).
- Kyle, U.G.; Bosaeus, I.; De Lorenzo, A.D.; Deurenberg, P.; Elia, M.; Gomez, J.M.; Heitmann, B.L.; Kent-Smith, L.; Melchior, J.-C.; Pirlich, M.; et al. Bioelectrical impedance analysis-part I: Review of principles and methods. Clin. Nutr. 2004, 23, 1226–1243. [Google Scholar] [CrossRef]
- Livelli di Assunzione di Riferimento di Nutrienti ed Energia per la Popolazione Italiana, LARN; IV Revisione; Società Italiana di Nutrizione Umana (SINU): Milan, Italy, 2014.
- Yumuk, V.; Tsigos, C.; Fried, M.; Schndler, K.; Busetto, L.; Micic, D.; Toplak, H. European Guidelines for Obesity Management in adults. Obes. Facts 2015, 8, 402–424. [Google Scholar] [CrossRef]
- Esposito, K.; Marfella, R.; Ciotola, M.; Di Palo, C.; Giugliano, F.; Giugliano, G.; D’Armiento, M.; D’Andrea, F.; Giugliano, D. Effect of a mediterranean-style diet on endothelial dysfunction and markers of vascular inflammation in the metabolic syndrome: A randomized trial. JAMA 2004, 292, 1440–1446. [Google Scholar] [CrossRef]
- Bautista-Castaño, I.; Molina-Cabrillana, J.; Montoya-Alonso, J.A.; Serra-Majem, L. Variables predictive of adherence to diet and physical-activity recommendations in the treatment of obesity and overweight, in a group of Spanish Subjects. Int. J. Obes. Relat. Metab. Disord. 2004, 28, 697–705. [Google Scholar] [CrossRef][Green Version]
- Andreoli, A.; Lauro, S.; Di Daniele, N.; Sorge, R.; Celi, M.; Volpe, S.L. Effect of a moderately hypoenergetic Mediterranean diet and exercise program on body cell mass and cardiovascular risk factors in obese women. Eur. J. Clin. Nutr. 2008, 62, 892–897. [Google Scholar] [CrossRef]
- Martins, P.C.; Hansen, F.; Silva, A.M.; Silva, D.A.S. Fluid distribution and cell integrity indicators evaluated by bioelectrical impedance in university athletes: Comparison between team sports and individual sports. Physiol. Meas. 2019, 40, 015004. [Google Scholar] [CrossRef]
- Heymsfield, S.B.; Gonzalez, M.C.; Shen, W.; Redman, L.; Thomas, D. Weight loss composition is one-fourth fat-free mass: A critical review and critique of this widely cited rule. Obes. Rev. 2014, 15, 310–321. [Google Scholar] [CrossRef]
- Johannsen, D.L.; Knuth, N.D.; Huizenga, R.; Rood, J.C.; Ravussin, E.; Hall, K.D. Metabolic slowing with massive weight loss despite preservation of fat-free mass. J. Clin. Endocrinol. Metab. 2012, 97, 2489–2496. [Google Scholar] [CrossRef]
- Mongioì, L.M.; Cimino, L.; Condorelli, R.A.; Magagnini, M.C.; Barbagallo, F.; Cannarella, R.; La Vignera, S.; Calogero, A.E. Effectiveness of a Very Low Calorie Ketogenic Diet on Testicular Function in Overweight/Obese Men. Nutrients 2020, 12, 2967. [Google Scholar] [CrossRef]
- La Vignera, S.; Cannarella, R.; Galvano, F.; Grillo, A.; Aversa, A.; Cimino, L.; Magagnini, C.M.; Mongioì, L.M.; Condorelli, R.A.; Calogero, A.E. The ketogenic diet corrects metabolic hypogonadism and preserves pancreatic ß-cell function in overweight/obese men: A single-arm uncontrolled study. Endocrine 2021, 72, 392–399. [Google Scholar] [CrossRef]
- Carneiro-Barrera, A.; Amaro-Gahete, F.J.; Jurado-Fasoli, L.; Sáez-Roca, G.; Martín-Carrasco, C.; Tinahones, F.J.; Ruiz, J.R. Effect of a Weight Loss and Lifestyle Intervention on Dietary Behavior in Men with Obstructive Sleep Apnea: The INTERAPNEA Trial. Nutrients 2022, 14, 2731. [Google Scholar] [CrossRef]
- Rondanelli, M.; Perna, S.; Ilyas, Z.; Peroni, G.; Bazire, P.; Sajuox, I.; Maugeri, R.; Nichetti, M.; Gasparri, C. Effect of very low-calorie ketogenic diet in combination with omega-3 on inflammation, satiety hormones, body composition, and metabolic markers. A pilot study in class I obese subjects. Endocrine 2022, 75, 129–136. [Google Scholar] [CrossRef]
- Barrea, L.; Muscogiuri, G.; Aprano, S.; Vetrani, C.; de Alteriis, G.; Varcamonti, L.; Verde, L.; Colao, A.; Savastano, S. Phase angle as an easy diagnostic tool for the nutritionist in the evaluation of inflammatory changes during the active stage of a very low-calorie ketogenic diet. Int. J. Obes. 2022, 46, 1591–1597. [Google Scholar] [CrossRef]
- Tragni, E.; Vigna, L.; Ruscica, M.; Macchi, C.; Casula, M.; Santelia, A.; Catapano, A.L.; Magni, P. Reduction of Cardio-Metabolic Risk and Body Weight through a Multiphasic Very-Low Calorie Ketogenic Diet Program in Women with Overweight/Obesity: A Study in a Real-World Setting. Nutrients 2021, 13, 1804. [Google Scholar] [CrossRef]
- Keller, K.; Engelhardt, M. Strength and muscle mass loss with aging process. Age and strength loss. Muscles Ligaments Tendons J. 2014, 3, 346–350. [Google Scholar] [CrossRef]
- Wood, R.J.; Gregory, S.M.; Sawyer, J.; Milch, C.M.; Matthews, T.D.; Headley, S.A. Preservation of fat-free mass after two distinct weight loss diets with and without progressive resistance exercise. Metab. Syndr. Relat. Disord. 2012, 10, 167–174. [Google Scholar] [CrossRef]
- Silva, A.M.; Heymsfield, S.B.; Gallagher, D.; Albu, J.; Pi-Sunyer, X.-F.; Pierson, R.N.J.; Wang, J.; Heska, S.; Sardinha, L.B.; Wang, Z. Evaluation of between-methods agreement of extracellular water measurements in adults and children. Am. J. Clin. Nutr. 2008, 88, 315–323. [Google Scholar] [CrossRef][Green Version]
- Joshi, S.; Mohan, V. Pros & cons of some popular extreme weight-loss diets. Indian J. Med. Res. 2018, 148, 642–647. [Google Scholar]
- Whitton, C.; Ramos-Garcìa, C.; Kirkpatrick, S.I.; Healy, J.D.; Dhaliwal, S.S.; Boushey, C.J.; Collins, C.E.; Rollo, M.E.; Kerr, D.A. A Systematic Review Examining Contributors to Misestimation of Food and Beverage Intake Based on Short-Term Self-Report Dietary Assessment Instruments Administered to Adults. Adv. Nutr. 2022, nmac085. [Google Scholar] [CrossRef]
- Stern, L.; Iqbal, N.; Seshadri, P.; Chicano, K.L.; Daily, D.; McGrory, J.; Williams, M.; Gracely, E.J.; Samaha, F.F. The Effects of Low-Carbohydrate versus Conventional Weight Loss Diets in Severely Obese Adults: One-Year Follow-up of a Randomized Trial. Ann. Intern. Med. 2004, 140, 778–785. [Google Scholar] [CrossRef] [PubMed]
- Thom, G.; Lean, M. Is There an Optimal Diet for Weight Management and Metabolic Health? Gastroenterology 2017, 152, 1739–1751. [Google Scholar] [CrossRef] [PubMed]
- Hall, K.D.; Khan, S. Maintenance of Lost Weight and Long-Term Management of Obesity. Med. Clin. N. Am. 2018, 102, 183–197. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| MD Group (n = 133) | Trend of Variation | p-Value | VLCKD Group (n = 135) | Trend of Variation | p-Value | p–Value Intergroup | |||
|---|---|---|---|---|---|---|---|---|---|
| T0 | T3M | T0 | T1M | ||||||
| Weight (kg) | |||||||||
| General population | 88.61 ± 15.26 | 81.86 ± 14.54 | ↓ | <0.0001 | 91.81 ± 18.45 | 85.17 ± 17.07 | ↓ | <0.0001 | 0.6604 |
| Male | 98.67 ± 14.05 | 91.08 ± 13.43 | ↓ | <0.0001 | 107.99 ± 19.5 | 99.56 ± 18.07 | ↓ | <0.0001 | 0.1658 |
| Female | 84.73 ± 13.93 | 78.30 ± 13.40 | ↓ | <0.0001 | 86.36 ± 14.54 | 80.33 ± 13.73 | ↓ | <0.0001 | 0.1316 |
| Body Mass Index (BMI; kg/m2) | |||||||||
| General population | 32.14 ± 4.68 | 29.67 ± 4.53 | ↓ | <0.0001 | 33.54 ± 5.49 | 31.14 ± 5.15 | ↓ | <0.0001 | 0.4831 |
| Male | 32.44 ±3.8 | 29.94 ± 3.81 | ↓ | <0.0001 | 35.05 ± 5.81 | 32.33 ± 5.41 | ↓ | <0.0001 | 0.2778 |
| Female | 32.03 ± 4.99 | 29.57 ± 4.8 | ↓ | <0.0001 | 33.03 ± 5.30 | 30.74 ± 5.02 | ↓ | <0.0001 | 0.1857 |
| Waist Circumference (cm) | |||||||||
| General population | 99.78 ± 14.14 | 92.92 ± 13.47 | ↓ | <0.0001 | 99.18 ± 15.46 | 93.44 ± 14.68 | ↓ | <0.0001 | 0.0010 |
| Male | 106.86 ± 12.71 | 99.85 ± 12.73 | ↓ | <0.0001 | 112.69 ± 14.28 | 106.33 ± 13.53 | ↓ | <0.0001 | 0.2760 |
| Female | 97.06 ± 13.78 | 90.26 ± 12.84 | ↓ | <0.0001 | 94.63 ± 13.04 | 89.09 ± 12.36 | ↓ | <0.0001 | 0.0020 |
| Phase angle (°) | |||||||||
| General population | 6.23 ± 0.81 | 6.17 ±0.8 | __ | 0.0812 | 6.41 ± 0.66 | 6.40 ± 0.73 | __ | 0.3067 | 0.3324 |
| Male | 6.84 ± 0.86 | 6.8 ± 0.84 | __ | 0.5593 | 6.88 ± 0.50 | 6.84 ± 0.47 | __ | 0.4831 | 0.9775 |
| Female | 5.99 ± 0.66 | 5.93 ± 0.64 | __ | 0.0873 | 6.25 ± 0.63 | 6.26 ± 0.74 | __ | 0.3182 | 0.3397 |
| Total Body Water (%) | |||||||||
| General population | 46.77 ± 5.46 | 49.04 ± 6.07 | ↑ | <0.0001 | 45.53 ± 5.32 | 47.11 ± 5.66 | ↑ | <0.0001 | 0.0017 |
| Male | 52.36 ± 4.76 | 54.27 ± 5.44 | ↑ | <0.0001 | 51.12 ± 4.24 | 52.27 ± 4.60 | ↑ | 0.0012 | 0.0676 |
| Female | 44.61 ± 4.00 | 47.02 ± 5.03 | ↑ | <0.0001 | 43.65 ± 4.21 | 45.37 ± 4.88 | ↑ | <0.0001 | 0.0076 |
| Extracellular Water (%) | |||||||||
| General population | 44.66 ± 3.7 | 44.82 ± 3.75 | __ | 0.3005 | 42.28 ± 7.29 | 41.96 ± 6.88 | __ | 0.1292 | 0.0659 |
| Male | 42.78 ± 4.38 | 42.85 ± 4.21 | __ | 0.7646 | 42.43 ± 3.43 | 41.95 ± 3.48 | __ | 0.0912 | 0.1342 |
| Female | 45.38 ± 3.13 | 45.58 ± 3.27 | __ | 0.3189 | 42.23 ± 8.20 | 41.97 ± 7.71 | __ | 0.3190 | 0.1656 |
| Intracellular Water (%) | |||||||||
| General population | 54.69 ± 5.45 | 54.50 ± 5.48 | __ | 0.2410 | 53.86 ± 9.03 | 54.19 ± 9.06 | __ | 0.3268 | 0.1655 |
| Male | 54.79 ± 9.3 | 54.74 ± 9.16 | __ | 0.8481 | 57.57 ± 3.43 | 57.25 ± 4.58 | __ | 0.6066 | 0.7454 |
| Female | 54.65 ± 3.15 | 54.41 ± 3.15 | __ | 0.2142 | 52.62 ± 9.95 | 53.16 ± 9.94 | __ | 0.1707 | 0.0797 |
| Fat-Free Mass (%) | |||||||||
| General population | 63.8 ± 7.4 | 66.68 ± 8.23 | ↑ | <0.0001 | 61.92 ± 6.97 | 64.15 ± 7.45 | ↑ | <0.0001 | 0.0373 |
| Male | 71.15 ± 6.4 | 73.58 ± 7.61 | ↑ | 0.0003 | 69.09 ± 5.27 | 71.07 ± 5.31 | ↑ | <0.0001 | 0.5024 |
| Female | 60.96 ± 5.6 | 64.03 ± 6.82 | ↑ | <0.0001 | 59.51 ± 5.71 | 61.82 ± 6.59 | ↑ | <0.0001 | 0.0251 |
| Fat Mass (%) | |||||||||
| General population | 36.16 ± 7.41 | 33.01 ± 8.26 | ↓ | <0.0001 | 38.29 ± 7.46 | 36.12 ± 8.12 | ↓ | <0.0001 | 0.0006 |
| Male | 28.77 ± 6.31 | 25.9 ± 7.11 | ↓ | <0.0001 | 30.89 ± 5.26 | 28.93 ± 5.31 | ↓ | <0.0001 | 0.0689 |
| Female | 39.01 ±5.63 | 35.75 ± 6.97 | ↓ | <0.0001 | 40.78 ± 6.37 | 38.54 ± 7.45 | ↓ | <0.0001 | 0.0034 |
| Body Cellular Mass (%) | |||||||||
| General population | 54.67 ± 4.17 | 54.12 ± 4.67 | __ | 0.0547 | 53.87 ± 7.54 | 53.90 ± 7.83 | __ | 0.8232 | 0.0756 |
| Male | 57.5 ± 3.8 | 57.21 ± 3.61 | __ | 0.3037 | 57.24 ± 2.28 | 56.88 ± 2.92 | __ | 0.2677 | 0.8884 |
| Female | 53.57 ± 3.79 | 52.93 ± 4.49 | __ | 0.0885 | 52.73 ± 8.32 | 52.90 ± 8.68 | __ | 0.3838 | 0.0518 |
| MD Group (n = 78) | Trend of Variation | p-Value | VLCKD Group (n = 78) | Trend of Variation | p-Value | p-Value Intergroup | |||
|---|---|---|---|---|---|---|---|---|---|
| T0 | T3M | T0 | T1M | ||||||
| Body weight (kg) | |||||||||
| Under 50 | 88.09 ± 16.23 | 81.28 ± 15.42 | ↓ | <0.0001 | 94.01 ± 19.69 | 87.19 ± 18.12 | ↓ | <0.0001 | 0.9892 |
| Over 50 | 89.35 ± 13.86 | 82.67 ± 13.29 | ↓ | <0.0001 | 88.79 ± 16.3 | 82.4 ± 15.23 | ↓ | <0.0001 | 0.4520 |
| Body Mass Index (BMI; kg/m2) | |||||||||
| Under 50 | 31.34 ± 4.07 | 28.95 ± 3.93 | ↓ | <0.0001 | 33.86 ± 5.79 | 31.44 ± 5.42 | ↓ | <0.0001 | 0.8271 |
| Over 50 | 33.29 ± 5.27 | 30.71 ± 5.14 | ↓ | <0.0001 | 33.1 ± 5.05 | 30.73 ± 4.77 | ↓ | <0.0001 | 0.2167 |
| Waist circumference (cm) | |||||||||
| Under 50 | 96.54 ± 13.38 | 89.58 ± 12.48 | ↓ | <0.0001 | 98.53 ± 17.32 | 92.78 ±16.47 | ↓ | <0.0001 | 0.0076 |
| Over 50 | 104.39 ± 14.04 | 97.67 ± 13.51 | ↓ | <0.0001 | 100.07 ± 12.58 | 94.34 ±11.89 | ↓ | <0.0001 | 0.0577 |
| Phase angle (°) | |||||||||
| Under 50 | 6.43 ± 0.74 | 6.36 ± 0.74 | __ | 0.0949 | 6.55 ± 0.62 | 6.53 ±0.72 | __ | 0.3021 | 0.4144 |
| Over 50 | 5.95 ± 0.84 | 5.90 ± 0.80 | __ | 0.4307 | 6.22 ± 0.67 | 6.23 ± 0.71 | __ | 0.8538 | 0.6885 |
| Total Body Water (%) | |||||||||
| Under 50 | 47.26 ± 4.87 | 49.65 ± 5.53 | ↑ | <0.0001 | 45.03 ± 5.23 | 46.58 ± 5.39 | ↑ | <0.0001 | 0.0040 |
| Over 50 | 46.06 ± 6.19 | 48.17 ± 6.72 | ↑ | <0.0001 | 46.20 ±5.4 | 47.83 ± 5.99 | ↑ | <0.0001 | 0.1547 |
| Extracellular Water (%) | |||||||||
| Under 50 | 43.94 ± 3.42 | 44.15 ± 3.66 | __ | 0.2615 | 40.27 ±8.49 | 40.21 ± 8.16 | __ | 0.7691 | 0.3320 |
| Over 50 | 45.68 ± 3.86 | 45.77 ± 3.7 | __ | 0.7318 | 45.03 ± 3.82 | 44.36 ± 3.4 | __ | 0.1018 | 0.1189 |
| Intracellular Water (%) | |||||||||
| Under 50 | 55.30 ± 5.90 | 55.08 ± 5.73 | __ | 0.2455 | 52.61 ± 11.11 | 52.91 ± 10.87 | __ | 0.0595 | 0.0347 |
| Over 50 | 53.82 ± 4.92 | 53.69 ± 5.06 | __ | 0.6270 | 55.59 ± 4.47 | 55.94 ± 5.34 | __ | 0.6459 | 0.5549 |
| Fat-Free Mass (%) | |||||||||
| Under 50 | 64.57 ± 6.55 | 67.69 ± 7.42 | ↑ | <0.0001 | 61.7 ±6.53 | 64.01 ± 6.72 | ↑ | <0.0001 | 0.0326 |
| Over 50 | 62.69 ± 8.4 | 65.25 ± 9.14 | ↑ | <0.0001 | 62.24 ± 7.58 | 64.34 ± 8.41 | ↑ | <0.0001 | 0.4098 |
| Fat Mass (%) | |||||||||
| Under 50 | 35.36 ± 6.57 | 32.03 ± 7.46 | ↓ | <0.0001 | 38.77 ± 7.33 | 36.62 ± 7.91 | ↓ | <0.0001 | 0.0019 |
| Over 50 | 37.3 ±8.40 | 34.4 ± 9.19 | ↓ | <0.0001 | 37.64 ± 7.66 | 35.44 ±8.41 | ↓ | <0.0001 | 0.1122 |
| Body Cellular Mass (%) | |||||||||
| Under 50 | 55.72 ± 3.88 | 54.94 ± 5.04 | __ | 0.0760 | 53.14 ± 8.86 | 53.02 ± 9.04 | __ | 0.5689 | 0.1667 |
| Over 50 | 53.17 ± 4.14 | 52.95 ± 3.83 | __ | 0.4667 | 54.86 ±5.13 | 55.11 ± 5.65 | __ | 0.3944 | 0.2631 |
| MD Group (n = 46) | Trend of Variation | p-Value | VLCKD Group (n = 38) | Trend of Variation | p-Value | p-Value Intergroup | |||
|---|---|---|---|---|---|---|---|---|---|
| T0 | T3M | T0 | T1M | ||||||
| Body Weight (kg) | |||||||||
| Subjects with overweight | 75.21 ± 8.58 | 69.06 ± 8.21 | ↓ | <0.0001 | 75.76 ± 6.94 | 70.26 ± 6.49 | ↓ | <0.0001 | 0.1254 |
| Subjects with obesity | 95.7 ± 13.11 | 88.62 ± 12.47 | ↓ | <0.0001 | 98.09 ± 17.74 | 91.01 ± 16.37 | ↓ | <0.0001 | 0.9878 |
| Body Mass Index (BMI; kg/m2) | |||||||||
| Subjects with overweight | 27.55 ± 1.56 | 25.35 ± 1.73 | ↓ | <0.0001 | 27.67 ± 1.37 | 25.70 ± 1.31 | ↓ | <0.0001 | 0.1740 |
| Subjects with obesity | 34.57 ± 3.89 | 31.96 ±3.83 | ↓ | <0.0001 | 35.84 ± 4.72 | 33.27 ± 4.48 | ↓ | <0.0001 | 0.7133 |
| Waist Circumference (cm) | |||||||||
| Subjects with overweight | 88.74 ± 9.10 | 81.83 ± 8.52 | ↓ | <0.0001 | 87.06 ± 11.72 | 82.05 ± 11.11 | ↓ | <0.0001 | 0.0020 |
| Subjects with obesity | 105.77 ± 12.62 | 98.79 ± 11.83 | ↓ | <0.0001 | 103.93 ± 14.13 | 97.89 ± 13.49 | ↓ | <0.0001 | 0.0289 |
| Phase angle (°) | |||||||||
| Subjects with overweight | 6.29 ± 0.70 | 6.21 ± 0.67 | __ | 0.0812 | 6.30 ± 0.63 | 6.21 ± 0.66 | __ | 0.0818 | 0.9077 |
| Subjects with obesity | 6.2 ± 0.87 | 6.15 ± 0.86 | __ | 0.2534 | 6.45 ± 0.67 | 6.48 ± 0.74 | __ | 0.5072 | 0.9390 |
| Total Body Water (%) | |||||||||
| Subjects with overweight | 49.74 ± 4.87 | 52.53 ± 5.49 | ↑ | <0.0001 | 48.24 ± 3.89 | 50.23 ± 3.57 | ↑ | <0.0001 | 0.0340 |
| Subjects with obesity | 45.19 ± 5.12 | 47.2 ± 5.55 | ↑ | <0.0001 | 44.46 ± 5.44 | 45.88 ± 5.87 | ↑ | <0.0001 | 0.0301 |
| Extracellular Water (%) | |||||||||
| Subjects with overweight | 55.82 ± 3.16 | 55.46 ± 2.93 | __ | 0.3005 | 42.64 ± 7.75 | 42.53 ± 7.26 | __ | 0.8379 | 0.6403 |
| Subjects with obesity | 44.87 ± 3.95 | 45.03 ± 4.10 | __ | 0.4031 | 42.14 ± 7.13 | 41.74 ± 6.75 | __ | 0.0423 | 0.0409 |
| Intracellular Water (%) | |||||||||
| Subjects with overweight | 44.26 ± 3.15 | 44.41 ± 2.97 | __ | 0.2410 | 54.01 ± 9.74 | 53.22 ± 8.43 | __ | 0.1883 | 0.4870 |
| Subjects with obesity | 54.09 ± 6.4 | 53.99 ± 6.4 | __ | 0.6229 | 53.81 ± 8.78 | 54.57 ± 9.30 | __ | 0.0547 | 0.0589 |
| Fat-Free Mass (%) | |||||||||
| Subjects with overweight | 67.96 ± 6.57 | 71.13 ± 7.57 | ↑ | <0.0001 | 65.58 ± 6.59 | 68.16 ± 6.80 | ↑ | <0.0001 | 0.4078 |
| Subjects with obesity | 61.59 ± 6.87 | 64.33 ± 7.61 | ↑ | <0.0001 | 60.49 ±6.61 | 62.58 ± 7.13 | ↑ | <0.0001 | 0.0516 |
| Fat Mass (%) | |||||||||
| Subjects with overweight | 32.03 ± 6.57 | 28.2 ± 7.32 | ↓ | <0.0001 | 34.32 ± 6.59 | 31.84 ± 6.80 | ↓ | <0.0001 | 0.0126 |
| Subjects with obesity | 38.35 ± 6.92 | 35.55 ± 7.61 | ↓ | <0.0001 | 39.81 ± 7.26 | 37.8 ± 8.00 | ↓ | <0.0001 | 0.0237 |
| Body Cellular Mass (%) | |||||||||
| Subjects with overweight | 54.94 ± 3.39 | 53.81 ± 5.47 | __ | 0.0547 | 54.28 ± 8.61 | 53.91 ± 8.86 | __ | 0.1665 | 0.3538 |
| Subjects with obesity | 54.52 ± 4.54 | 54.28 ± 4.21 | __ | 0.2471 | 53.7 ± 7.12 | 53.9 ± 7.44 | __ | 0.3534 | 0.1436 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Rosa, C.; Lattanzi, G.; Spiezia, C.; Imperia, E.; Piccirilli, S.; Beato, I.; Gaspa, G.; Micheli, V.; De Joannon, F.; Vallecorsa, N.; et al. Mediterranean Diet versus Very Low-Calorie Ketogenic Diet: Effects of Reaching 5% Body Weight Loss on Body Composition in Subjects with Overweight and with Obesity—A Cohort Study. Int. J. Environ. Res. Public Health 2022, 19, 13040. https://doi.org/10.3390/ijerph192013040
Di Rosa C, Lattanzi G, Spiezia C, Imperia E, Piccirilli S, Beato I, Gaspa G, Micheli V, De Joannon F, Vallecorsa N, et al. Mediterranean Diet versus Very Low-Calorie Ketogenic Diet: Effects of Reaching 5% Body Weight Loss on Body Composition in Subjects with Overweight and with Obesity—A Cohort Study. International Journal of Environmental Research and Public Health. 2022; 19(20):13040. https://doi.org/10.3390/ijerph192013040
Chicago/Turabian StyleDi Rosa, Claudia, Greta Lattanzi, Chiara Spiezia, Elena Imperia, Sara Piccirilli, Ivan Beato, Gianluigi Gaspa, Vanessa Micheli, Federica De Joannon, Noemi Vallecorsa, and et al. 2022. "Mediterranean Diet versus Very Low-Calorie Ketogenic Diet: Effects of Reaching 5% Body Weight Loss on Body Composition in Subjects with Overweight and with Obesity—A Cohort Study" International Journal of Environmental Research and Public Health 19, no. 20: 13040. https://doi.org/10.3390/ijerph192013040
APA StyleDi Rosa, C., Lattanzi, G., Spiezia, C., Imperia, E., Piccirilli, S., Beato, I., Gaspa, G., Micheli, V., De Joannon, F., Vallecorsa, N., Ciccozzi, M., Defeudis, G., Manfrini, S., & Khazrai, Y. M. (2022). Mediterranean Diet versus Very Low-Calorie Ketogenic Diet: Effects of Reaching 5% Body Weight Loss on Body Composition in Subjects with Overweight and with Obesity—A Cohort Study. International Journal of Environmental Research and Public Health, 19(20), 13040. https://doi.org/10.3390/ijerph192013040