
Addressing Challenges When Applying GRADE to Public Health Guidelines: A Scoping Review Protocol and Pilot Analysis

 , , ,
, , ,  , ,
, ,  , , ,
, , ,  , , , ,
, , , , 
 add
Show full author list
add
Show full author list
Abstract
:1. Introduction
2. Methods
2.1. Review Question
- How were previously identified challenges addressed within public health guidelines?
- What additional challenges have been identified within public health guidelines?
- Have any modifications been made to the GRADE approach within public health guidelines, and how were they justified?
2.2. Eligibility Criteria
2.2.1. Concept
2.2.2. Context
2.2.3. Types of Sources
2.3. Search
2.4. Evidence Selection
2.5. Data Extraction
- Title of the document;
- Date of publication;
- Source;
- The developing organization or author´s names;
- Characteristics of the guideline (de novo, adopted, living, an update, etc.);
- Purpose of the guideline, including a remit of the organization;
- Target audience;
- Country of origin (if applicable);
- Methods used for identifying different stakeholders and incorporating their perspectives;
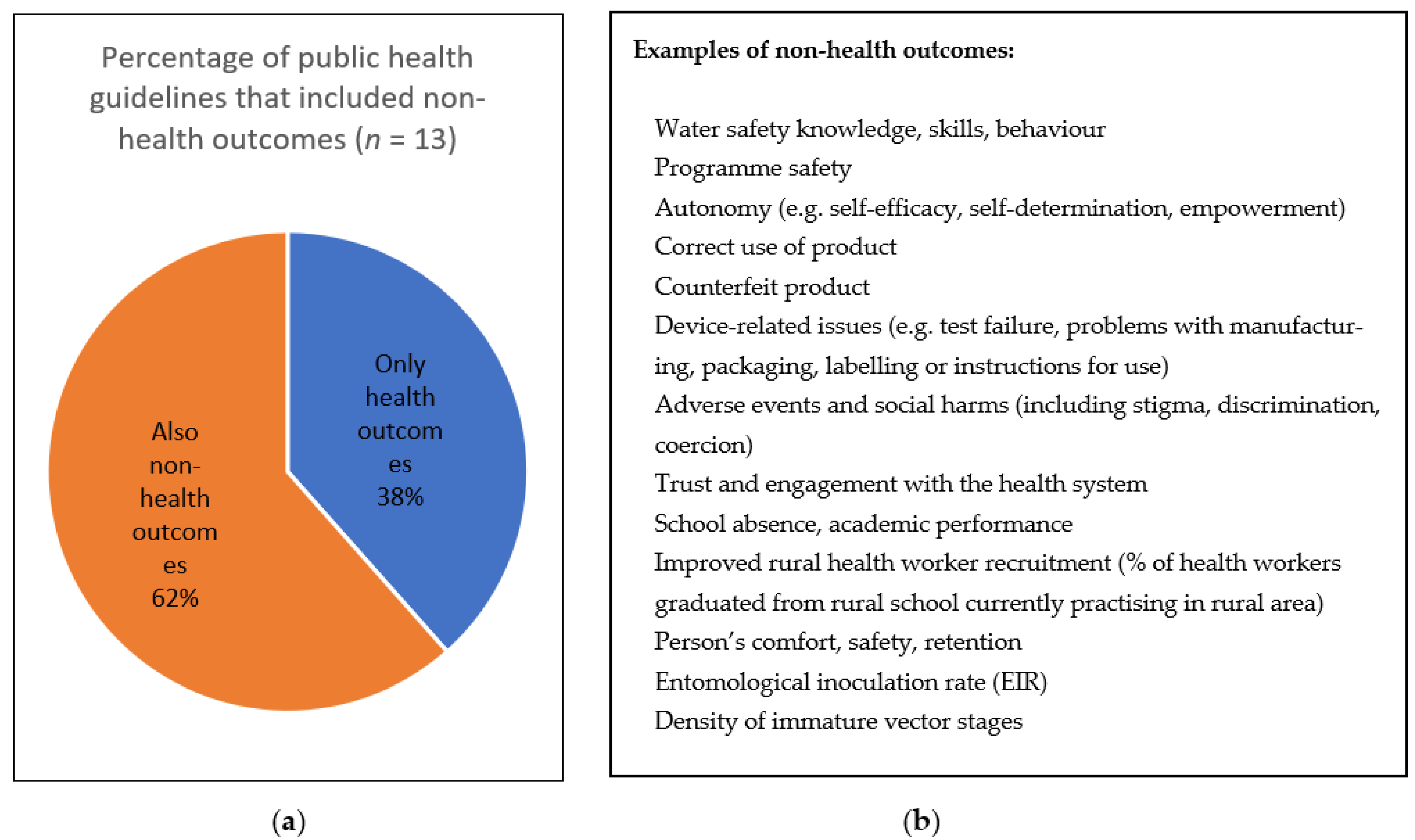
- Methods for identification and prioritization of any non-health outcomes;
- Methods for determining thresholds for decision-making;
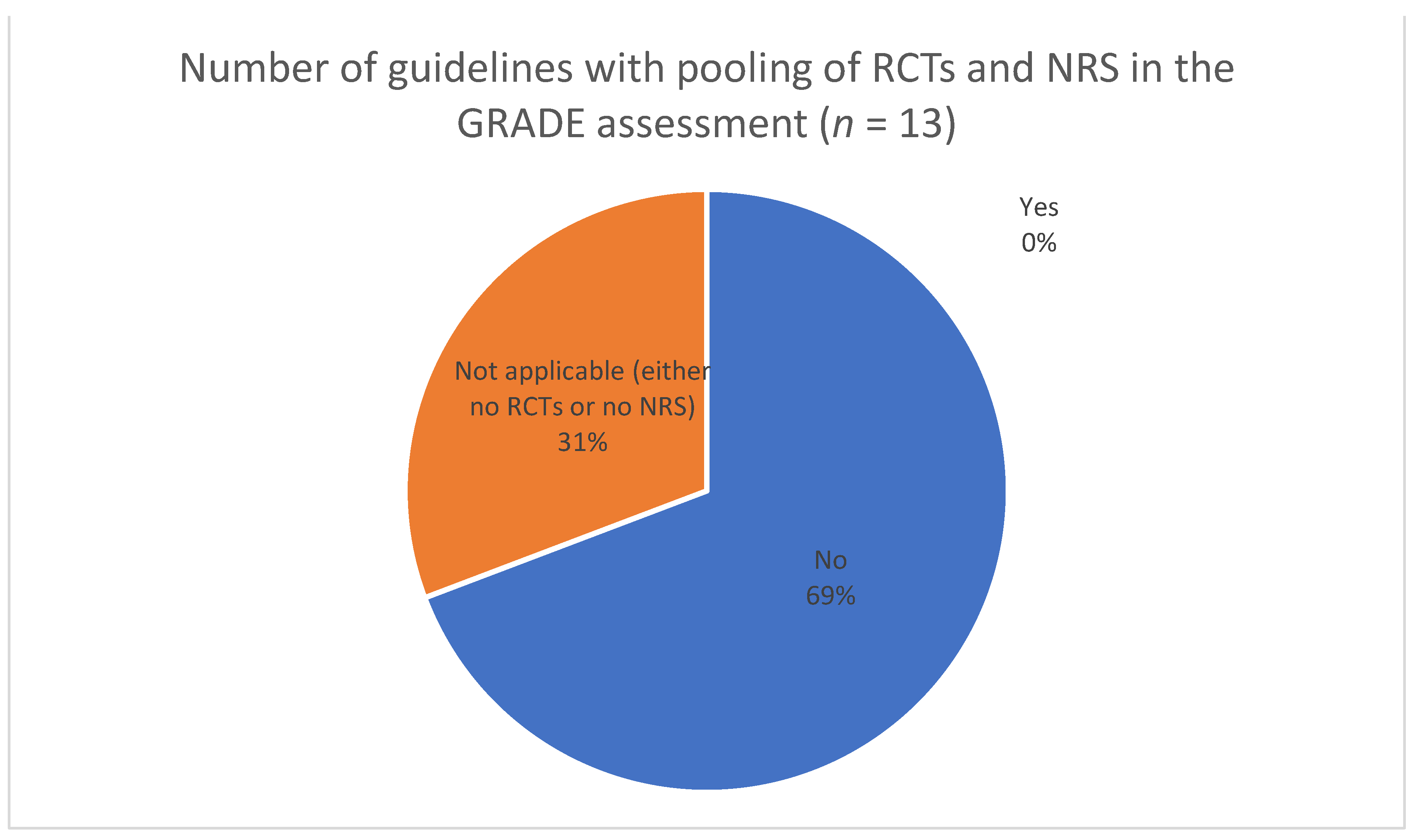
- Methods for incorporating and grading evidence from non-randomized studies;
- Methods for addressing concerns with conditional recommendations in public health;
- Methods for reaching consensus and the formal approval of recommendations;
- Additional methodological concerns and/or challenges noted by guideline authors;
- Any modifications made to GRADE and their justifications.
2.6. Data Analysis and Presentation
3. Preliminary Results (Pilot Phase) and Discussion
Limitations and Strengths
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Guidelines for WHO Guidelines; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Qaseem, A.; Forland, F.; Macbeth, F.; Ollenschläger, G.; Phillips, S.; van der Wees, P. Guidelines International Network: Toward international standards for clinical practice guidelines. Ann. Intern. Med. 2012, 156, 525–531. [Google Scholar] [CrossRef] [PubMed]
- Schünemann, H.; Brożek, J.; Guyatt, G.; Oxman, A. (Eds.) GRADE Handbook. 2013. Available online: https://gdt.gradepro.org/app/handbook/handbook.html (accessed on 21 August 2021).
- Norris, S.L.; Rehfuess, E.A.; Smith, H.; Tunçalp, Ö.; Grimshaw, J.M.; Ford, N.P.; Portela, A. Complex health interventions in complex systems: Improving the process and methods for evidence-informed health decisions. BMJ Glob. Health 2019, 4 (Suppl. 1), e000963. [Google Scholar] [CrossRef] [PubMed]
- Hilton Boon, M.; Thomson, H. Challenges in applying the GRADE approach in public health guidelines and systematic reviews: A concept article from the GRADE Public Health Group. J. Clin. Epidemiol. 2021, 135, 42–53. [Google Scholar] [CrossRef] [PubMed]
- Munn, Z.; Peters, M.D.J. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med. Res. Methodol. 2018, 18, 143. [Google Scholar] [CrossRef] [PubMed]
- Peters, M.D.J.; Godfrey, C. Chapter 11: Scoping Reviews (2020 Version). In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; JBI: Adelaide, Australia, 2020. [Google Scholar] [CrossRef]
- Peters, M.D.J.; Marnie, C. Updated methodological guidance for the conduct of scoping reviews. JBI Evid. Synth. 2020, 18, 2119–2126. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Page, M.J.; McKenzie, J.E. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. J. Clin. Epidemiol. 2021, 134, 178–189. [Google Scholar] [CrossRef] [PubMed]
- Akl, E.A.; Kennedy, C. Using GRADE methodology for the development of public health guidelines for the prevention and treatment of HIV and other STIs among men who have sex with men and transgender people. BMC Public Health 2012, 12, 386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rehfuess, E.A.; Akl, E.A. Current experience with applying the GRADE approach to public health interventions: An empirical study. BMC Public Health 2013, 13, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burford, B.J.; Rehfuess, E. Assessing evidence in public health: The added value of GRADE. J. Public Health 2012, 34, 631–635. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, H.-F.; Shannon, S.E. Three Approaches to Qualitative Content Analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Antenatal Care Recommendations for a Positive Pregnancy Experience: Nutritional Interventions Update: Zinc Supplements during Pregnancy; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- World Health Organization. WHO guideline on the Prevention of Drowning through Provision of Day-Care and Basic Swimming and Water Safety Skills; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- World Health Organization. Consolidated Guidelines on HIV Prevention, Testing, Treatment, Service Delivery and Monitoring: Recommendations for a Public Health Approach; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- World Health Organization. Recommendations and Guidance on Hepatitis C Virus Self-Testing; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- World Health Organization. WHO Guideline on Self-Care Interventions for Health and Well-Being; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- World Health Organization. WHO Guideline on School Health Services; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- World Health Organization. Guideline: Infant Feeding in Areas of Zika Virus Transmission; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- World Health Organization. WHO Guideline on Health Workforce Development, Attraction, Recruitment and Retention in Rural and Remote Areas; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- World Health Organization. Updated Recommendations on Service Delivery for the Treatment and Care of People Living with HIV; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- World Health Organization. WHO Guideline on the Dairy Protein Content in Ready-to-Use Therapeutic Foods for Treatment of Uncomplicated Severe Acute Malnutrition; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Promoting 2SLGBTQI+ Health Equity (Registered Nurses’ Association of Ontario). Available online: https://rnao.ca/bpg/guidelines/promoting-2slgbtqi-health-equity (accessed on 6 August 2021).
- Behaviour Change: Digital and Mobile Health Interventions (National Institute for Heatlh and Care Excellence (NICE)). Available online: www.nice.org.uk/guidance/ng183 (accessed on 6 August 2021).
- World Health Organization. WHO Guidelines for Malaria; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Title and Reference | Publication Date | Organization | Purpose |
|---|---|---|---|
| WHO antenatal care recommendations for a positive pregnancy experience: nutritional interventions update: zinc supplements during pregnancy [15] | 12 August 2021 | WHO | To reflect and respond to issues surrounding antenatal care To prioritize person-centred health and well-being |
| WHO Guideline on the prevention of drowning through provision of day-care and basic swimming and water safety skills [16] | 23 July 2021 | WHO | To provide recommendations about appropriateness of day-care and basic swim skills and water safety among children (low- and middle-income countries) |
| Consolidated guidelines on HIV prevention, testing, treatment, service delivery and monitoring: recommendations for a public health approach [17] | 16 July 2021 | WHO | To provide recommendations about providing ARV drugs for HIV prevention and treatment (settings with limited health system capacity and resources); to increase HIV prevention, testing, and treatment access, strengthen the HIV care and integrate the provision of ARV drugs; to provide guidance on adapting, setting priorities for and implementing the clinical and operational recommendations, and monitoring their implementation and impact. |
| Recommendations and guidance on hepatitis C virus self-testing [18] | 15 July 2021 | WHO | To supplement the existing WHO guidelines on hepatitis testing services; to support countries and national programmes in reaching 2030 HCV elimination goals by helping them reach people who may not otherwise test. |
| WHO Guideline on self-care interventions for health and well-being [19] | 13 July 2021 | WHO | To provide guidance, to support individuals, communities, and countries with quality health services and self-care interventions good practice statements on key issues, to promote and increase safe and equitable access and the uptake and use of self-care interventions for health considerations for future research and guidelines processes. |
| WHO guideline on school health services [20] | 22 June 2021 | WHO | To provide guidance on effectiveness, acceptability, and content of SHS involving a health worker; to support national governments and partners to develop SHS programmes. |
| Guideline: infant feeding in areas of Zika virus transmission, 2nd edition [21] | 15 June 2021 | WHO | To provide recommendations on infant feeding in areas with Zika virus transmission. |
| WHO guideline on health workforce development, attraction, recruitment and retention in rural and remote areas [22] | 6 May 2021 | WHO | To support national authorities in strengthening the density and capacity of health workforce (rural and remote areas); to develop, attract, recruit, and retrain health workers; to identify relevant elements and implementation and evaluation considerations at policy and system levels. |
| Updated recommendations on service delivery for the treatment and care of people living with HIV [23] | 28 April 2021 | WHO | To encourage improvement in access to ART; to simplify care delivery; to support return to care for those who have disengaged; to support reduction of people acquiring HIV and dying for associated causes; to contribute to achieving the Triple-Billion targets. |
| WHO guideline on the dairy protein content in ready-to-use therapeutic foods (RUTF) for treatment of uncomplicated severe acute malnutrition [24] | 8 April 2021 | WHO | To provide recommendation on whether reduced dairy or non-dairy RUTF should be used for treating malnutrition. |
| Promoting 2SLGBTQI+ Health Equity [25] | July 2021 | RNAO (CA) | To provide recommendations on care practices for 2SLGBTQI+ people; to enhance safety of organizations for 2SLGBTQI+ people; to optimize health outcomes for those people. |
| Behaviour change: digital and mobile health interventions [26] | 7 October 2020 1 | NICE (UK) | To cover interventions that use digital or mobile platforms to help people change behaviour. |
| WHO Guidelines for malaria [27] | 13 July 2021 | WHO | To reduce and ultimately eliminate malaria; to provide recommendations for malaria prevention; to support the development national malaria policies for prevention; to maximize the impact of available resources. |
| THEME 1 (Predefined): Incorporating Diverse Perspectives and Identifying Stakeholders | |
|---|---|
| CATEGORIES | CODES |
| Methods for identifying members of GDG | CODE: identifying members by searching the literature for researchers in the topic area CODE: identifying members through key informant interviews CODE: identifying members through established professional networks, associations, organizations, and advocacy bodies CODE: suggestions for membership came from previous guideline development group memberships CODE: identifying members in accordance with the organization´s Guideline development manual CODE: suggestions for membership came from the Guideline endorsing organization and its dedicated departments, expert advisory panels, country and regional offices and groups CODE: a group appointed by the endorsing organization identified experts for GDG |
| Characteristics of GDG members | CODE: GDG includes commissioners CODE: GDG includes health economist CODE: GDG includes local government CODE: members have expertise in guideline development methods CODE: members have collectively the necessary multidisciplinary expertise in the topic of interest CODE: members are among the intended end-users CODE: members have expertise in research CODE: members are representatives of civil society organizations CODE: members are from the target population (networks, lay members) CODE: representatives from national programmes to provide perspectives on the resource implications in their countries CODE: absence of significant conflicts of interest CODE: external (outside of the endorsing organization) CODE: geographically dispersed CODE: gender-balanced |
| Procedures of forming GDG | CODE: GDG membership list was posted for public review and comment and then finalized |
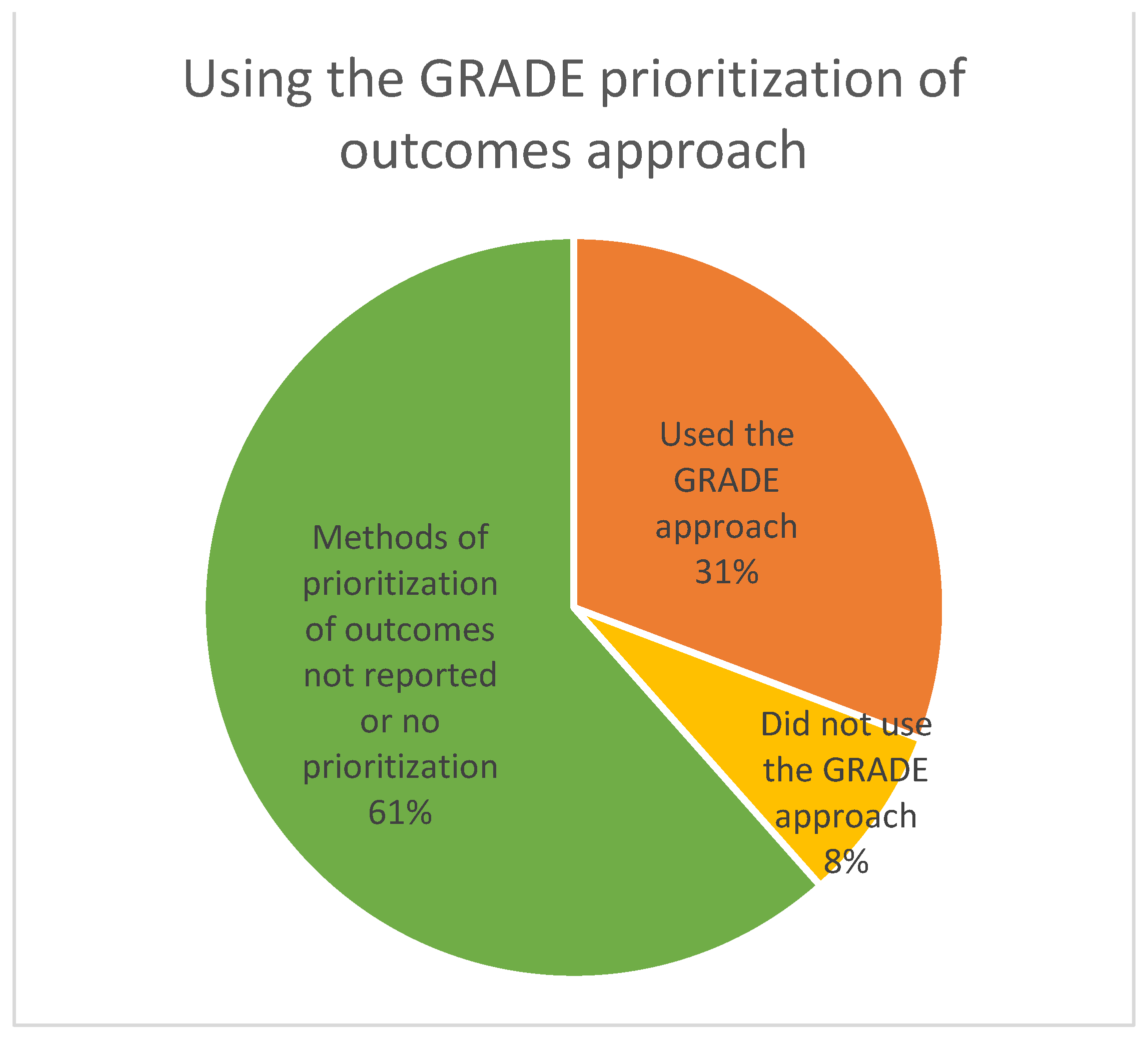
| THEME 2 (Predefined): Identifying and Prioritizing Outcomes | |
|---|---|
| CATEGORIES | CODES |
| Identifying and selecting outcomes | CODE: due to the variability of outcome reporting, decision rules for selecting outcomes were used CODE: outcomes identified via review of the literature CODE: outcomes identified via key informant interviews and discussion groups CODE: outcomes identified via expert panel survey prior to the in-person meeting CODE: outcomes identified via expert panel discussion at an in-person meeting CODE: primary outcomes were agreed upon by the GDG [seems after the relevant studies were identified, not a priori] CODE: scoping exercise of guidelines and systematic reviews of the Guideline topics informed the outcomes CODE: scoping review of target population´s values and preferences informed the outcomes |
| Prioritizing outcomes | CODE: outcomes were aligned with the Sustainable Development Goals CODE: priority outcomes were aligned with a previous (related) guideline CODE: Critical and important outcomes were agreed between the review team and the Steering Group and were endorsed by the GDG CODE: outcomes were prioritized via an online survey–members ranked the importance of each outcome on the GRADE rating scale of 1–9 (0–3: not important; 4–6: important; 7–9: critical). CODE: up to five priority outcomes were determined based on confidential voting by each member, and a subsequent facilitated discussion of the voting results CODE: online vote determined critical outcomes if 70% of the votes were ranked 7–9 on a 9-point Likert scale |
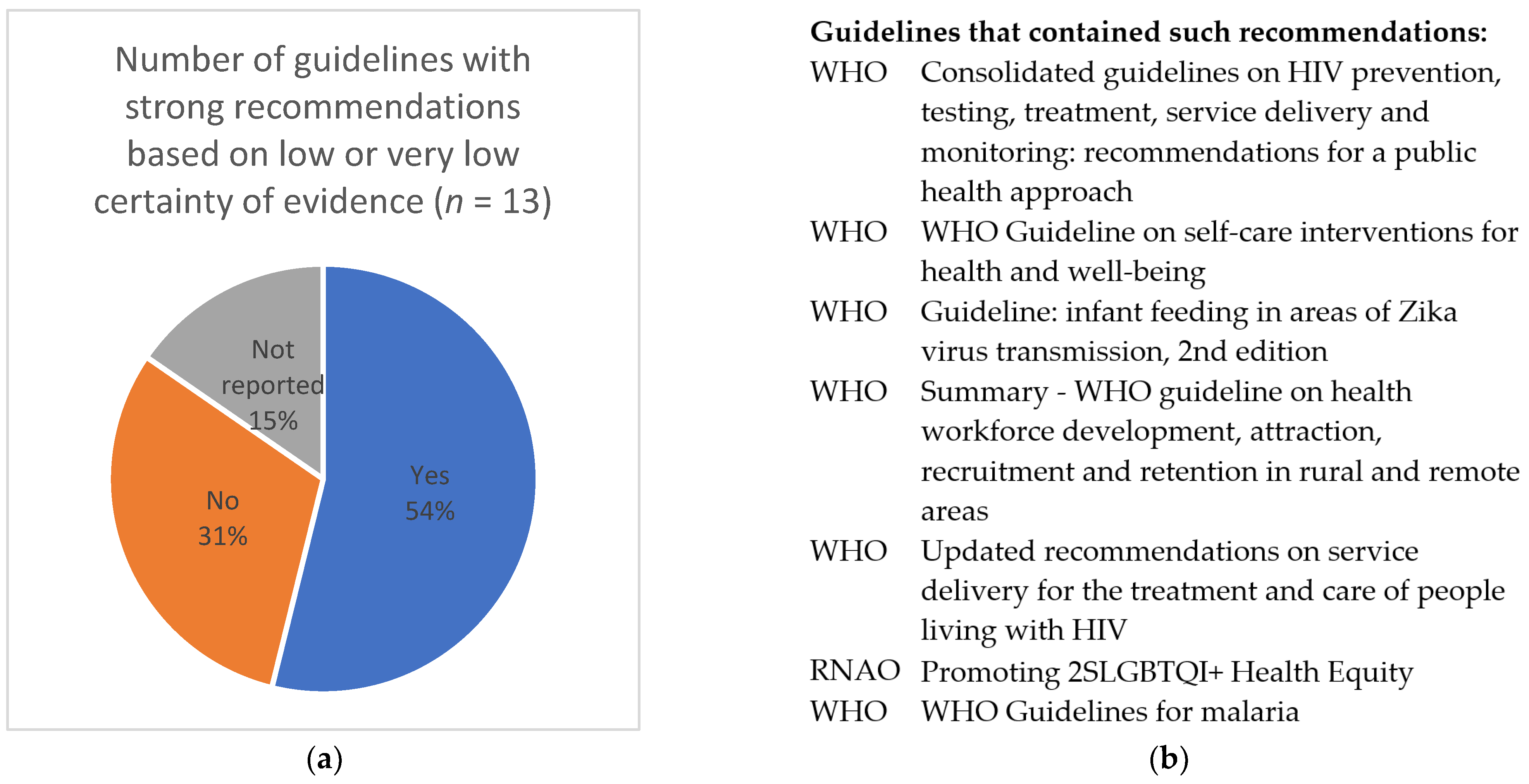
| THEME 5: Addressing Implications for Decision-Makers, Including Concerns about Conditional Recommendations Reasons for Developing Strong Recommendations Based on Low or Very Low Certainty of Evidence | ||
|---|---|---|
| Category | Explanation (by the Review Team) | Example Recommendation |
| There is a substantial experience of using the intervention (already widely implemented) and no harm. | The “intervention” is already implemented, seems effective, and this is causing the lack of research leading to low or very low certainty of evidence. | “WHO recommends making the self-management of folic acid supplements available as an additional option to health worker-led provision of folic acid supplements for individuals who are planning pregnancy within the next three months.” [19] |
| Greatly valued and/or needed by the target population and no known harm. | The target population is suffering greatly from a problem (or an intervention is needed), and any non-harmful intervention will be greatly valued and likely effective. Assessing effectiveness/costs and other aspects seems secondary. | “WHO recommends investing in rural infrastructure and services to ensure decent living conditions for health workers and their families.” [22] |
| Using other types of evidence with high confidence (indirect, pharmacokinetic modelling, programmatic data). | Various other-than scientific data (not experience or expert evidence) are available, and the panel has high confidence in them, or is confident that the identified indirect evidence can completely substitute the missing direct evidence (e.g., when one disease has much more evidence than another, but they are essentially the same, common for infectious diseases). | “Children weighing < 20 kg should receive a higher dose of artesunate (3 mg/kg bw per dose) than larger children and adults (2.4 mg/kg bw per dose) to ensure equivalent exposure to the drug.” (artesunate is recommended for adult populations with high certainty of the evidence) [27] |
| Potentially equivalent in benefits and harms, and doing intervention (vs. not doing) seems better in all other EtD domains (no reasons against). | When considering whether to perform an intervention or not, in the context of no obvious effects or harms, one option seems better in all other aspects, and there seems to be no reason not to perform the intervention. | “WHO recommends designing and enabling access to continuing education and professional development programmes that meet the needs of rural health workers to support their retention in rural areas.“ [22] |
| The intervention is ethically necessary (“sound”, “basic human right”). | “WHO recommends ensuring a safe and secure working environment for health workers in rural and remote areas.” [22] | |
| A perfect balance of effects, the only problem is low or very low certainty of evidence (lack of higher-certainty research) | Recommendation formulated in the context of lack of higher-certainty evidence (usually due to limited evidence, e.g., only observational studies downgraded by 0 or 1 level, or RCTs downgraded by 2–3 levels) when all other aspects are in favour of the intervention. | “People established on anti-retroviral therapy should be offered refills lasting 3–6 months, preferably six months if feasible.” [23] Rationale (from the guideline): “Some of the evidence supporting these recommendations came from observational studies with methodological limitations, and there was important variability (heterogeneity) in outcomes across studies.” |
| THEME 6 (Predefined): Formulating and Agreeing on Recommendations | |
|---|---|
| CATEGORIES | CODES |
| Prior to the meeting for agreeing on recommendations | CODE: PanelVoice was used to allow panelists to pre-vote on the EtD framework questions CODE: members could draw attention to any new evidence prior to the meeting CODE: recommendations were drafted a priori to the meeting CODE: members received detailed background documents prior to meetings CODE: reviewed the preliminary judgements and comments posted by all members in the online EtD form CODE: reviewed evidence summaries CODE: all members posted comments in an online form (EtD) CODE: members were provided with the EtD frameworks, evidence profiles, and full-text articles |
| The course of the meetings to agree on recommendations | CODE: discussion facilitated by the chair and/or methodologist CODE: the meeting was guided by a clear protocol CODE: process guided by the organization´s manual/handbook CODE: detailed background documents had been summarized in presentations during each GDG meeting CODE: methodologist facilitated discussions CODE: discussion was facilitated by co-chairs and methodologists CODE: formulate recommendations through a process of group discussion, engagement, and revision CODE: members were presented with a ‘neutral’ recommendation and decided on its direction and strength |
| Facilitation methods | CODE: voting was used as a starting point to build consensus (not as a formal vote) CODE: members were asked to raise their hands in support of each separate option as a decision-making aid (not as a formal vote) CODE: in the online environment, close attention was paid to eliciting responses from all members CODE: regular straw-polling and chat function were used to gain an initial indication of members’ views |
| Methods for agreeing on recommendations | CODE: consensus—unanimous agreement (on the direction, strength, and wording of a recommendation) after a facilitated discussion CODE: voting only in case of disagreement CODE: forming recommendations without explicitly considering those from a previous version of the guideline CODE: no member expressed opposition to the recommendations CODE: at an in-person meeting CODE: at an online meeting CODE: online vote (after the meeting) CODE: if consensus could not be reached, more time was given for deliberations CODE: the GDG reached an agreement (method not specified) CODE: voting was anonymous (“In some cases, anonymous voting was used for judging the different criteria and developing the final recommendation to reduce peer pressure.”) CODE: every member was asked to express their decision verbally |
| Voting thresholds | CODE: voting, 60% of the cast votes CODE: voting, 70% of the cast votes CODE: voting, two thirds of the cast votes |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kantorová, L.; Friessová, T.; Slezáková, S.; Langaufová, A.; Kantor, J.; Munn, Z.; Barker, T.H.; Katikireddi, S.V.; Mustafa, R.A.; Žuljević, M.F.; et al. Addressing Challenges When Applying GRADE to Public Health Guidelines: A Scoping Review Protocol and Pilot Analysis. Int. J. Environ. Res. Public Health 2022, 19, 992. https://doi.org/10.3390/ijerph19020992
Kantorová L, Friessová T, Slezáková S, Langaufová A, Kantor J, Munn Z, Barker TH, Katikireddi SV, Mustafa RA, Žuljević MF, et al. Addressing Challenges When Applying GRADE to Public Health Guidelines: A Scoping Review Protocol and Pilot Analysis. International Journal of Environmental Research and Public Health. 2022; 19(2):992. https://doi.org/10.3390/ijerph19020992
Chicago/Turabian StyleKantorová, Lucia, Tereza Friessová, Simona Slezáková, Alena Langaufová, Jiří Kantor, Zachary Munn, Timothy Hugh Barker, Srinivasa Vittal Katikireddi, Reem A. Mustafa, Marija Franka Žuljević, and et al. 2022. "Addressing Challenges When Applying GRADE to Public Health Guidelines: A Scoping Review Protocol and Pilot Analysis" International Journal of Environmental Research and Public Health 19, no. 2: 992. https://doi.org/10.3390/ijerph19020992
APA StyleKantorová, L., Friessová, T., Slezáková, S., Langaufová, A., Kantor, J., Munn, Z., Barker, T. H., Katikireddi, S. V., Mustafa, R. A., Žuljević, M. F., Lukežić, M., Klugarová, J., Riad, A., Vrbová, T., Pokorná, A., Búřilová, P., Búřil, J., Kirkovski, A., Ćaćić, N., ... Klugar, M. (2022). Addressing Challenges When Applying GRADE to Public Health Guidelines: A Scoping Review Protocol and Pilot Analysis. International Journal of Environmental Research and Public Health, 19(2), 992. https://doi.org/10.3390/ijerph19020992