
Exploration of Estimated Emigration Trends of Polish Health Professionals



Abstract
1. Introduction
- -
- One of the lowest employment rates of medical professions per capita in Europe: 2.4 doctors/1000 inhabitants (EU average: 3.8/1000) and 5.1 nurses/1000 inhabitants (EU average: 8.2/1000). These indicators have not changed for many years, which makes the staff deficit extremely severe due to the care demand of the ageing Polish society [28].
- -
- An increasing age of health professionals and a systematic increase in the share of people of retirement age in the cohort. This results from a lack of generational replacement in the most numerous groups of medical professions. Currently, the average age of a doctor is 50.2 (specialists, over 54.2); the average age of a midwife is 50.4, and that of a nurse is 52.6 [22]. The latter is growing the fastest of them all.
- -
- Excessive workload and the need to take up employment in several places (over 60% of doctors and approximately 30–40% of nurses work in more than one healthcare unit) [22].
- -
- Low prestige and an unsatisfactory level of remuneration (especially among junior doctors, nurses, paramedics, and physiotherapists, whose wages in Poland are perceived as unsatisfactory). To improve the remuneration policy, in 2017 the Act on the method for determining the lowest basic salary for employees performing medical professions employed in healthcare entities was implemented, regulating the minimum basic salaries of medical staff employed in healthcare facilities [29].
- -
- Recognition of physiotherapists as a medical profession (the third largest group), and the establishment of a chamber representing the interests of this important professional group [30].
2. Materials and Methods
2.1. Study Design and Participants
2.2. Data Sources and Variables
2.3. Statistical Analysis
3. Results
3.1. Estimated Emigration Trends of Polish Health Professionals in the Period of 2004–2020
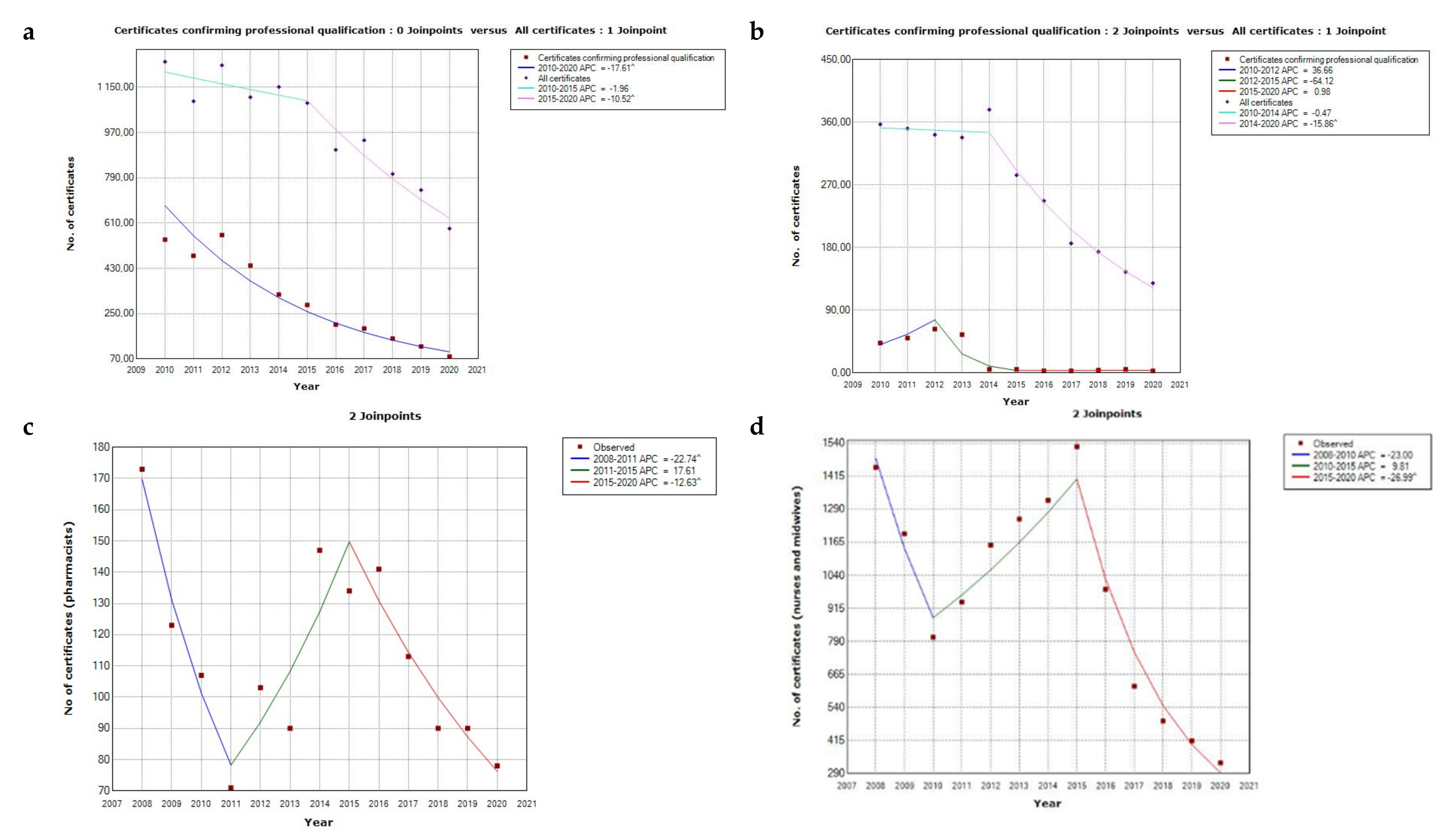
3.1.1. The National Chamber of Physicians Data
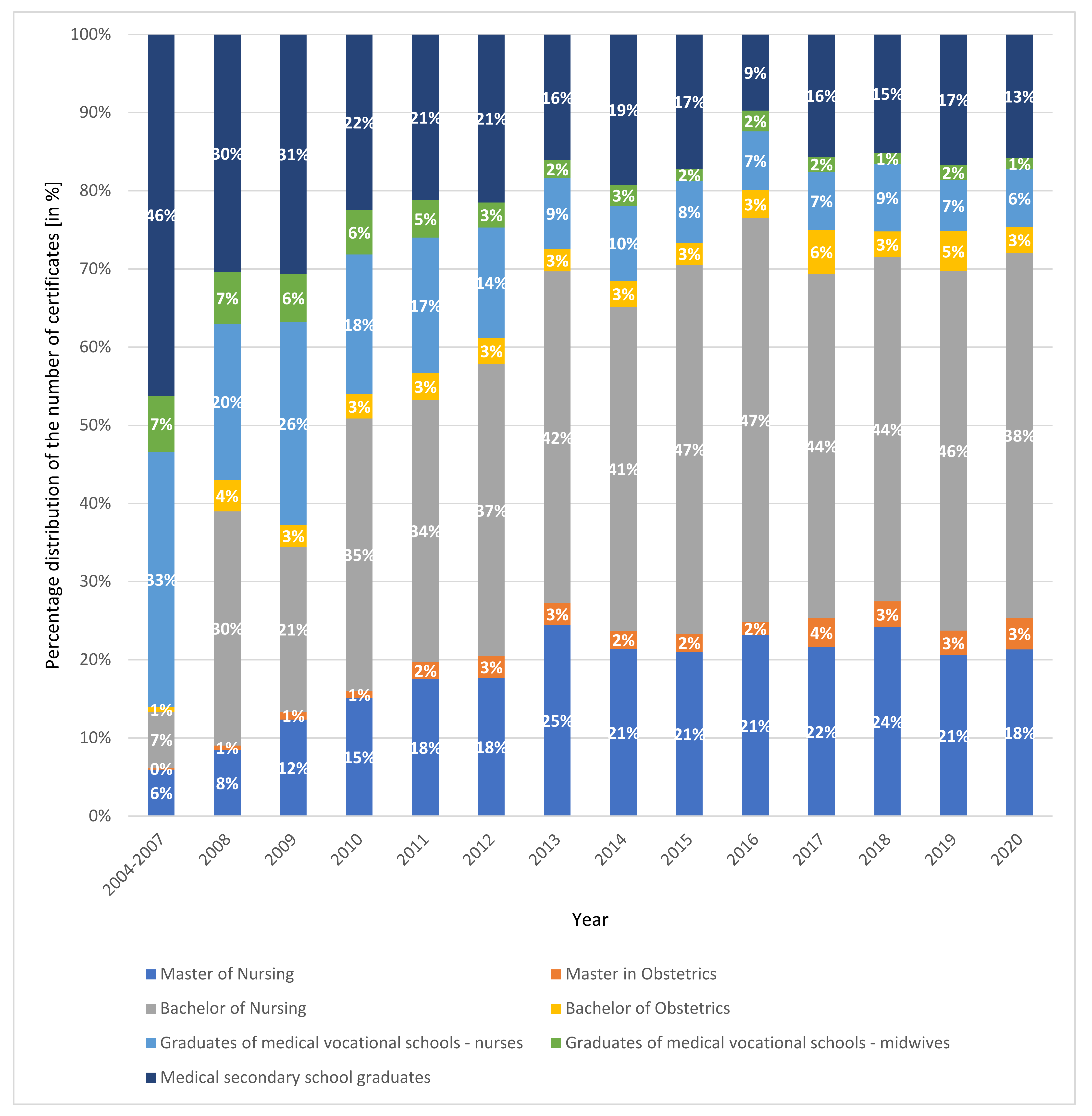
3.1.2. The National Chamber of Nurses and Midwives Data
3.1.3. The National Chamber of Physiotherapists Data
3.1.4. The Supreme Pharmaceutical Chamber and the Chamber of Laboratory Diagnosticians Data
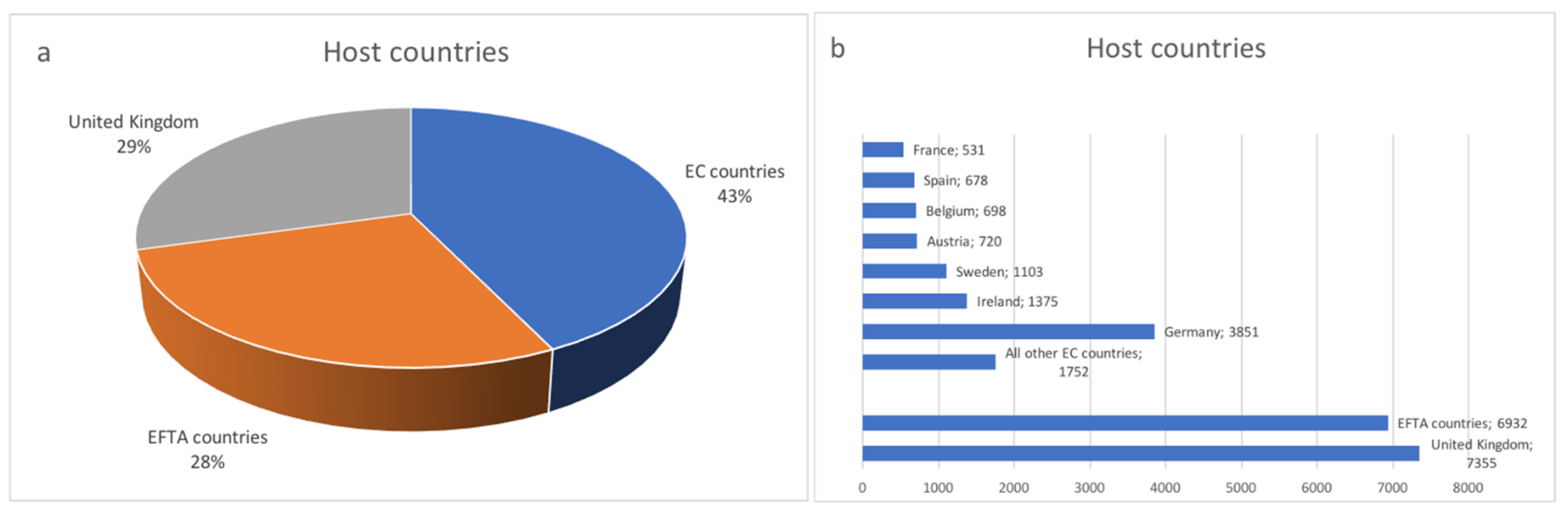
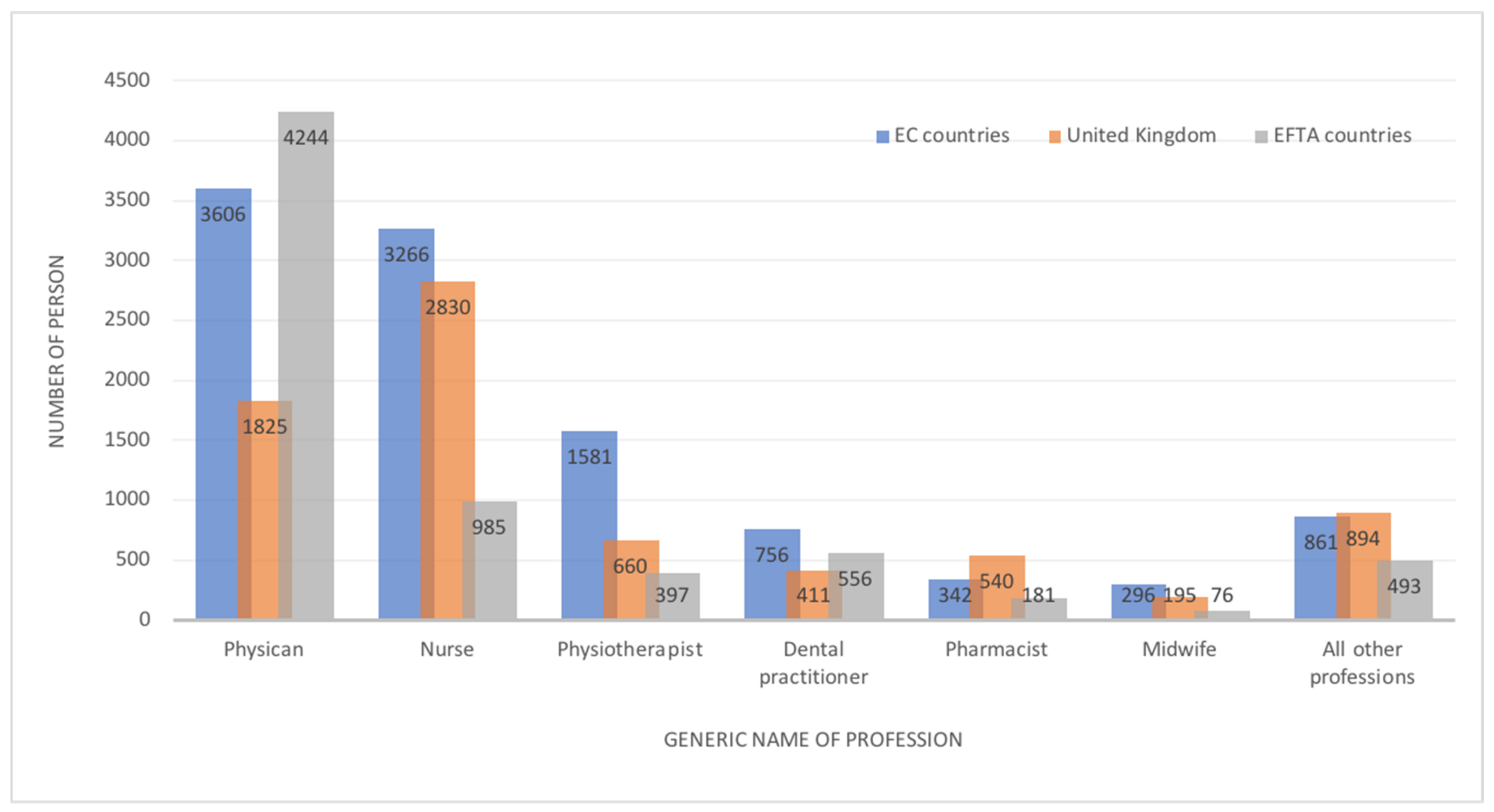
3.2. The Main Destinations of Polish Medical Staff—Analysis of the European Database
4. Discussion
4.1. Implications of the Study and Recommendations for Further Research
4.2. Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- European Union’s Directive. 2005/36/ec of the European Parliament and of the Council of 7 September 2005 on the Recognition of Professional Qualifications. Available online: http://eur-lex.europa.eu/legal-content/EN/TXT/?qid=1401715075231&uri=CELEX%3A32005L0036 (accessed on 18 June 2021).
- Glinos, I. Health professional mobility in the European Union: Exploring the ethics and efficiency of free movement. Health Policy 2015, 119, 1529–1536. [Google Scholar] [CrossRef] [PubMed]
- Eursostat. Statistic Explained. Migration and Migrant Population Statistics. 2021. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Migration_and_migrant_population_statistics (accessed on 2 December 2021).
- Simon, J.; Kiss, N.; Łaszewska, A.; Mayer, S. Public Health Aspects of Migrant Health: A Review of the Evidence on Health Status for Labour Migrants in the European Region; Health Evidence Network Synthesis Report 43; WHO Regional Office for Europe: Copenhagen, Denmark, 2015. [Google Scholar]
- Lebano, A.; Hamed, S.; Bradby, H.; Gil-Salmerón, A.; Durá-Ferrandis, E.; Garcés-Ferrer, J.; Azzedine, F.; Riza, E.; Karnaki, P.; Zota, D. Migrants’ and refugees’ health status and healthcare in Europe: A scoping literature review. BMC Public Health 2020, 20, 1039. [Google Scholar] [CrossRef] [PubMed]
- Titzmann, P.F.; Fuligni, A.J. Immigrants’ adaptation to different cultural settings: A contextual perspective on acculturation: Introduction for the special section on immigration. Int. J. Psychol. 2015, 50, 407–412. [Google Scholar] [CrossRef] [PubMed]
- Halikiopoulou, D.; Vlandas, T. When economic and cultural interests align: The anti-immigration voter coalitions driving far right party success in Europe. Eur. Political Sci. Rev. 2020, 12, 427–448. [Google Scholar] [CrossRef]
- Bieber, F. Is Nationalism on the Rise? Assessing Global Trends. Ethnopolitics 2018, 17, 519–540. [Google Scholar] [CrossRef]
- Cervi, L.; Tejedor, S.; Alencar Dornelles, M. When Populists Govern the Country: Strategies of Legitimization of Anti-Immigration Policies in Salvini’s Italy. Sustainability 2020, 12, 10225. [Google Scholar] [CrossRef]
- Cervi, L. Exclusionary Populism and Islamophobia: A Comparative Analysis of Italy and Spain. Religions 2020, 11, 516. [Google Scholar] [CrossRef]
- Brochmann, G. Controlling immigration in Europe. In Mechanisms of Immigration Control: A Comparative Analysis of European Regulation Policies; Routledge: London, UK, 2020; pp. 297–334. [Google Scholar]
- Bludau, H. Global Healthcare Worker Migration. Anthropology 2021. [Google Scholar] [CrossRef]
- OECD. Recent Trends in International Migration of Doctors, Nurses and Medical Students; OECD Publishing: Paris, France, 2019. [Google Scholar] [CrossRef]
- Wismar, M.; Maier, C.B.; Glinos, I.A.; Dussault, G.; Figueras, J. Health Professional Mobility and Health Systems: Evidence from 17 European Countries; Observatory Studies Series 23; WHO Regional Office for Europe on Behalf of the European Observatory on Health Systems and Policies: Copenhagen, Denmark, 2011; Available online: https://www.euro.who.int/__data/assets/pdf_file/0017/152324/Health-Professional-Mobility-Health-Systems.pdf (accessed on 9 August 2021).
- Chakravorty, I.; Bamrah, J.S.; Mehta, R. Migration of healthcare professionals in post-Brexit Britain. Physician 2021, 6, 1–8. [Google Scholar] [CrossRef]
- OECD. Health Statistics 2020. Available online: https://stats.oecd.org/Index.aspx?ThemeTreeId=9 (accessed on 15 June 2021).
- Lekarska, N.I.; Ośrodek Studiów Analiz i Informacji. Ile Pracują Lekarze i Lekarze Dentyści w Polsce. 2018. Available online: https://nil.org.pl/uploaded_files/1575629852_mapy-2017-aneks-do-raportu-ogolnego-v1-0.pdf (accessed on 15 June 2021).
- European Commission. The European Working Time Directive (EWTD). Available online: https://ec.europa.eu/social/main.jsp?catId=706&langId=en&intPageId=205 (accessed on 9 August 2021).
- OECD Heath at a Glance 2019. OECD Indicators. 2019. Available online: https://www.oecd-isdlibrary.org/social-issues-migration-health/health-at-a-glance-2019_4dd50c09-en (accessed on 7 August 2021).
- International Health Data Comparison. 2020. Available online: https://www.aihw.gov.au/reports/phe/237/international-health-data-comparisons-2018/contents/remuneration-of-health-professionals (accessed on 7 August 2021).
- Brugha, R. Doctor retention in a COVID-world: An opportunity to reconfigure the health workforce, or “Plus ça change plus c’est la meme chose”? A response to the recent commentaries. Int. J. Health Policy Manag. 2021. [Google Scholar] [CrossRef]
- Bociąga-Jasik, M.; Domagała, A.; Gaciong, Z.; Golinowska, S.; Grodzicki, T.; Haber, M.; Karkowska, D.; Kózka, M.; Windak, A.; Włodarczyk, C. Alert Zdrowotny 4: Zawody Medyczne i Inne Zawody Ochrony Zdrowia w Świetle Pandemii COVID-19. In Proceedings of the Open Eyes Economy Summit, Krakow, Poland, 17–18 November 2020. [Google Scholar]
- Usher, K.; Durkin, J.; Bhullar, N. The COVID-19 pandemic and mental health impacts. Int. J. Ment. Health Nurs. 2020, 29, 315–318. [Google Scholar] [CrossRef]
- Vizheh, M.; Qorbani, M.; Arzaghi, S.M.; Muhidin, S.; Javanmard, Z.; Esmaeili, M. The mental health of healthcare workers in the COVID-19 pandemic: A systematic review. J. Diabetes Metab. Disord. 2020, 19, 1967–1978. [Google Scholar] [CrossRef]
- Lai, J.; Ma, S.; Wang, Y.; Cai, Z.; Hu, J.; Wei, N.; Wu, J.; Du, H.; Chen, T.; Li, R.; et al. Factors associated with mental health outcomes among health care workers exposed to coronavirus disease. JAMA Net. Open. 2020, 3, e203976. [Google Scholar] [CrossRef]
- Shaukat, N.; Ali, D.M.; Razzak, J. Physical and mental health impacts of COVID-19 on healthcare workers: A scoping review. Int. J. Emerg. Med. 2020, 13, 40. [Google Scholar] [CrossRef]
- World Health Organization. Health Workforce Policy and Management in the Context of the COVID-19 Pandemic Response. 2020. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-health_workforce-2020.1 (accessed on 24 June 2021).
- OECD/European Union. Health at a Glance: Europe 2020: State of Health in the EU Cycle; OECD Publishing: Paris, France, 2020. [Google Scholar] [CrossRef]
- Act on the Method for Determining the Lowest Basic Salary 8 June 2017 for Employees Performing Medical Professions Employed in Item 1 473 Healthcare Entities Ustawa z Dnia 8 Czerwca 2017 r. o Sposobie Ustalania Najniższego Wynagrodzenia Zasadniczego Pracowników Wykonujących Zawody Medyczne Zatrudnionych w Podmiotach Leczniczych. Available online: https://isap.sejm.gov.pl/isap.nsf/DocDetails.xsp?id=WDU20170001473 (accessed on 15 June 2021).
- Act on Profession of Physicoterapists, Ustawa z Dnia 25 Września 2015 r. o Zawodzie Fizjoterapeuty, 2015 Dz. U. 2015 Poz. 1994. Available online: https://isap.sejm.gov.pl/isap.nsf/DocDetails.xsp?id=WDU20150001994 (accessed on 15 June 2021).
- The Polish Supreme Audit Office (NIK). Kształcenie i Przygotowanie Zawodowe Kadr Medycznych. Report Dedicated to Training of Medical Staff. 2016. Available online: https://www.nik.gov.pl/plik/id,10242,vp,12565.pdf (accessed on 15 June 2021).
- Żuk, P.; Żuk, P.; Lisiewicz-Jakubaszko, J. Labour migration of doctors and nurses and the impact on the quality of health care in Eastern European countries: The case of Poland. Econ. Labour Relat. Rev. 2019, 30, 307–320. [Google Scholar] [CrossRef]
- European Commission. The EU single market. In Regulated Profession Database; European Commission; Available online: https://ec.europa.eu/growth/tools-databases/regprof (accessed on 15 June 2021).
- Szpakowski, R.; Zajac, P.W.; Dykowska, G.; Sienkiewicz, Z.; Augustynowicz, A.; Czerw, A. Labour migration of Polish nurses: A questionnaire survey conducted with the Computer Assisted Web Interview technique. Hum. Resour. Health 2016, 14, 79–88. [Google Scholar] [CrossRef]
- Szpakowski, R.; Dykowska, G.; Fronczak, A.; Zając, P.; Czerw, A. Migrations of nurses and doctors from Poland: Data for the years 2014–2020 based on the sample of the capital city of Warsaw. Arch. Med. Sci. 2019, 15, 811–820. [Google Scholar] [CrossRef]
- Domagała, A.; Dubas-Jakóbczyk, K. Migration intentions among physicians working in Polish hospitals—Insights from survey research. Health Policy 2019, 23, 782–789. [Google Scholar] [CrossRef]
- Kalinowski, P. Wyszarpnięte pensje. Med. Trib. 2008, 3, 4. [Google Scholar]
- National Chamber of Physicans. NIL, Zestawienie Liczbowe wg Liczby Wydanych Zaświadczeń Województwa Miejsca Zameldowania i Okresu Wydania Zaświadczenia. Available online: https://old.nil.org.pl/__data/assets/pdf_file/0009/141849/za-grudzien-2019_Zestawienie-nr-05.pdf (accessed on 30 June 2021).
- Goštautaitė, B.; Bučiūnienė, I.; Milašauskienė, Ž.; Bareikis, K.; Bertašiūtė, E.; Mikelionienė, G. Migration intentions of Lithuanian physicians, nurses, residents and medical students. Health Policy 2018, 122, 1126–1131. [Google Scholar] [CrossRef]
- Filippidis, F.T. Emigrating young physicians leave Greece with an aging health workforce. J. Public Health 2015, 38, e587. [Google Scholar] [CrossRef][Green Version]
- Győrff, Z.; Dweik, D.; Girasek, E. Willingness to migrate—A potential effect of burnout? A survey of Hungarian physicians. Hum. Resour. Health 2018, 16, 36. [Google Scholar] [CrossRef]
- Domagała, A.; Peña-Sánchez, J.N.; Dubas-Jakóbczyk, K. Satisfaction of Physicians Working in Polish Hospitals—A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2018, 15, 2640. [Google Scholar] [CrossRef]
- Merçay, C.; Dumont, J.C.; Lafortune, G. Trends and policies affecting the international migration of doctors and nurses to OECD countries. In Health Workforce Policies in OECD Countries: Right Jobs, Right Kills, Right Places; OECD Health Policy Studies; OECD Publishing: Paris, France, 2016; pp. 103–124. [Google Scholar]
- POLITICO, The EU exodus: When Doctors and Nurses Follow the Money Doctors and Nurses Flow. By Hervey, G. 30 September 2017. Available online: https://www.politico.eu/article/doctors-nurses-migration-health-care-crisis-workers-follow-the-money-european-commission-data (accessed on 18 June 2021).
- Buchan, J.; Campbell, J.; Dhillon, I.; Charlesworth, A. Labour Market Change and the International Mobility of Health Workers. The health Foundation, Working Paper Number 5 March 2019. Available online: https://www.health.org.uk/publications/labour-market-change-and-the-international-mobility-of-health-workers (accessed on 18 June 2021).
- Dussault, G.; Fronteira, I.; Cabral, J. Migration of Health Personnel in the WHO European Region; WHO Regional Office for Europe: Cepenhagen, Denmark, 2009; Available online: http://www.euro.who.int/__data/assets/pdf_file/0010/95689/E93039.pdf (accessed on 18 June 2021).
- Ustawa z Dnia 27 Listopada 2020 r. o Zmianie Niektórych Ustaw w Celu Zapewnienia w Okresie Ogłoszenia Stanu Zagrożenia Epidemicznego lub Stanu Epidemii Kadr Medycznych, Dz.U.2020.2401. Available online: https://sip.lex.pl/akty-prawne/dzu-dziennik-ustaw/zmiana-niektorych-ustaw-w-celu-zapewnienia-w-okresie-ogloszenia-stanu-19064770 (accessed on 24 June 2021).
- Barriball, L.; Bremner, J.; Buchan, J.; Craveiro, I.; Dieleman, M.; Dix, O.; Dussault, G.; Jansen, C.; Kroezen, M.; Rafferty, A.M.; et al. Recruitment and Retention of the Health Workforce in Europe Final Report; European Commission: Brussels, Belgium, 2015. [Google Scholar]
- Skucha, E.; Domagała, A. Problem migracji ratowników medycznych. Polityka Społeczna 2018, 2, 24–29. [Google Scholar]
- Jośko, J.; Kasperczyk, J.; Grzybowski, A.; Ejsmont, J.; Karwat, D.; Zarzeczna-Baran, M.; Jethon, Z. Career plans of Polish medical university students. Probl. Hig. Epidemiol. 2011, 92, 199–203. [Google Scholar]
- Krajewski-Siuda, K.; Romaniuk, P.; Madaj, B.; Forbes, J.; Hubicki, L. Brain drain threat-Polish students are not satisfied with labor market options for health professionals in Poland. J. Public Health 2008, 16, 347–351. [Google Scholar] [CrossRef]
- Krajewski-Siuda, K.; Szromek, A.; Romaniuk, P.; Gericke, C.A.; Szpak, A.; Kaczmarek, K. Emigration preferences and plans among medical students in Poland. Hum. Resour. Health 2012, 10, 8. [Google Scholar] [CrossRef]
- Szostek, Ł.; Leńczuk-Gruba, A.; Kobos, E.; Imiela, J. Nursing students’ professional plans regarding migration. Pol. Nurs. 2017, 3, 481–486. [Google Scholar] [CrossRef][Green Version]
- Szczepańska, B.; Szady-Grad, M.; Klawe, J.; Kołodziejska, K.; Złotowska, A. Professional plans of students of physiotherapy and medical rescue at the Collegium Medicum in Bydgoszcz. Probl. Hig. Epidemiol. 2010, 91, 708–709. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Physicians | Dentists | Nurses and Midwives | Physiotherapists | Pharmacists | Total | |
|---|---|---|---|---|---|---|
| 2004–2009 * | 7805 | 810 | 11,963 | n/d | 296 | 20,578 (3430 -annually) |
| 2010 | 544 | 43 | 806 | n/d | 107 | 1500 |
| 2011 | 480 | 50 | 939 | n/d | 71 | 1540 |
| 2012 | 562 | 63 | 1154 | n/d | 103 | 1882 |
| 2013 | 441 | 55 | 1253 | n/d | 90 | 1839 |
| 2014 | 326 | 5 | 1324 | n/d | 147 | 1802 |
| 2015 | 249 | 5 | 1527 | n/d | 134 | 1915 |
| 2016 | 206 | 3 | 987 | n/d | 141 | 1337 |
| 2017 | 191 | 3 | 620 | 295 | 113 | 1222 |
| 2018 | 151 | 4 | 488 | 376 | 90 | 1109 |
| 2019 | 119 | 5 | 413 | 304 | 90 | 931 |
| 2020 | 79 | 3 | 330 | 239 | 78 | 729 |
| Total | 11,153 | 1049 | 21,804 | 1214 | 1460 | 36,680 |
| Certificates Confirming Professional Qualification Issued to the Doctors | |||
| Period | APC | 95% CI | p value |
| 2010–2020 | −17.605 | (−20.225; −14.900) | <0.001 |
| Certificates confirming professional qualification issued to the dentists | |||
| Period | APC | 95% CI | p value |
| 2010–2012 | 36.664 | (−55.981; 324.294) | 0.445 |
| 2012–2015 | −64.124 | (−88.445; 11.381) | 0.064 |
| 2015–2020 | 0.976 | (−21.620; 30.088) | 0.911 |
| All certificates issued to the doctors (including certificates of good standing) | |||
| Period | APC | 95% CI | p value |
| 2010–2015 | −1.962 | (−7.383; 3.777) | 0.427 |
| 2015–2020 | −10.517 | (−15.465; −5.280) | 0.003 |
| All certificates issued to the dentists (including certificates of good standing) | |||
| Period | APC | 95% CI | p value |
| 2010–2014 | −0.468 | (−4.857; 4.123) | 0.807 |
| 2014–2015 | −15.857 | (−17.861; −13.804) | <0.001 |
| Certificates issued for the recognition of professional qualifications of pharmacist | |||
| Period | APC | 95% CI | p value |
| 2008–2011 | −22.742 | (−37.388; −4.671) | 0.025 |
| 2011–2015 | 17.610 | (−5.675; 46.645) | 0.117 |
| 2015–2020 | −12.633 | (−21.511; −2.750) | 0.023 |
| Certificates issued for the recognition of professional qualifications of nurses and midwives | |||
| 2008–2010 | −23.000 | (−43.460; 4.864) | 0.082 |
| 2010–2015 | 9.812 | (−0.406; 21.079) | 0.057 |
| 2015–2020 | −26.988 | (−31.860; −21.767) | <0.001 |
| Generic Name of Profession | Recognition in EC Countries | Recognition in the United Kingdom | Recognition in EFTA Countries | Recognition TOTAL |
|---|---|---|---|---|
| Doctor of medicine | 3606 | 1825 | 4244 * | 9675 |
| Nurse | 3266 | 2830 | 985 | 4534 |
| Physiotherapist | 1581 | 660 | 397 | 2638 |
| Dental practitioner | 756 | 411 | 556 | 1723 |
| Pharmacist | 342 | 540 | 181 | 1063 |
| Midwife | 296 | 195 | 76 | 567 |
| Nursing assistant and health care assistant | 208 | 2 | 198 | 408 |
| Psychologist | 155 | 78 | 82 | 315 |
| Masseur/massage therapist/SPA therapist | 82 | 0 | 0 | 82 |
| Radiographer/radiotherapist | 79 | 98 | 18 | 195 |
| Medical/biomedical laboratory technician | 75 | 122 | 24 | 221 |
| Pharmaceutical technician/pharmaceutical assistant | 57 | 52 | 59 | 168 |
| Paramedic/ambulance nurse/other ambulance professionals | 41 | 248 | 48 | 337 |
| Dental technician | 26 | 107 | 32 | 165 |
| Dietician | 24 | 19 | 2 | 45 |
| Speech and language therapist | 21 | 1 | 1 | 23 |
| Optometrist (ophthalmic optician) | 20 | 10 | 19 | 49 |
| Geriatric nurse/carer for the aged | 18 | 0 | 0 | 18 |
| Chiropodist (podiatrist) | 13 | 0 | 0 | 13 |
| Dental hygienist | 11 | 98 | 6 | 115 |
| Bio-medical analyst | 11 | 0 | 0 | 11 |
| Dental assistant/dental nurse | 5 | 52 | 0 | 57 |
| Optician (dispensing optician) | 4 | 1 | 0 | 5 |
| Clinical psychologist | 4 | 0 | 0 | 4 |
| Hearing aid dispenser/audiometric technician/audiometric technician | 2 | 5 | 3 | 10 |
| Nutritionist/Clinical nutritionist | 2 | 0 | 1 | 3 |
| Nursery nurse | 1 | 0 | 0 | 1 |
| Surgical assistant | 1 | 1 | 0 | 2 |
| Psychomotor therapist | 1 | 0 | 0 | 1 |
| Total | 10,708 | 7355 | 6932 | 22,448 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Domagała, A.; Kautsch, M.; Kulbat, A.; Parzonka, K. Exploration of Estimated Emigration Trends of Polish Health Professionals. Int. J. Environ. Res. Public Health 2022, 19, 940. https://doi.org/10.3390/ijerph19020940
Domagała A, Kautsch M, Kulbat A, Parzonka K. Exploration of Estimated Emigration Trends of Polish Health Professionals. International Journal of Environmental Research and Public Health. 2022; 19(2):940. https://doi.org/10.3390/ijerph19020940
Chicago/Turabian StyleDomagała, Alicja, Marcin Kautsch, Aleksandra Kulbat, and Kamila Parzonka. 2022. "Exploration of Estimated Emigration Trends of Polish Health Professionals" International Journal of Environmental Research and Public Health 19, no. 2: 940. https://doi.org/10.3390/ijerph19020940
APA StyleDomagała, A., Kautsch, M., Kulbat, A., & Parzonka, K. (2022). Exploration of Estimated Emigration Trends of Polish Health Professionals. International Journal of Environmental Research and Public Health, 19(2), 940. https://doi.org/10.3390/ijerph19020940