Abstract
The aim of the study was to provide a systematic review and meta-analysis of studies examining the association between mortality risk and motor vehicle crashes (MVCs) in pregnant women compared with nonpregnant women. We used relevant MeSH terms to identify epidemiological studies of mortality risk in relation to MVCs from PubMed, Embase, and MEDLINE databases. The Newcastle–Ottawa Scale (NOS) was used for quality assessment. For comparison of mortality from MVCs between pregnant and nonpregnant women, the pooled odds ratios (OR) with 95% confidence intervals (CI) were calculated using a random effects model. The eight studies selected met all inclusion criteria. These studies included 14,120 injured victims who were pregnant at the time of the incident and 207,935 victims who were not pregnant. Compared with nonpregnant women, pregnant women had a moderate but insignificant decrease in mortality risk (pooled OR = 0.68, 95% CI = 0.38–1.22, I2 = 88.71%). Subgroup analysis revealed that the pooled OR significantly increased at 1.64 (95% CI = 1.16–2.33, I2 < 0.01%) for two studies with a similar difference in the mean injury severity score (ISS) between pregnant and nonpregnant women. Future studies should further explore the risk factors associated with MVCs in pregnant women to reduce maternal mortality.
1. Introduction
Pregnancy is a common condition that increases the risk of severe injuries and poor outcomes, including maternal and fetal morbidity and mortality, following trauma [1]. Pregnant women who experience trauma are at increased health risk because they tend to suffer complications caused by an increase in soft-tissue edema and fluid response, and interpreting their vital signs is difficult due to altered hemodynamics. Surgical interventions may also be impeded because of their altered anatomy. These factors make trauma during pregnancy challenging to treat, and they contribute to poor adverse outcomes [2].
Motor vehicle crashes (MVCs) account for the largest portion of reported trauma during pregnancy [1]. Involvement in MVCs during pregnancy might lead to preterm labor, placental abruption, and fetal demise [3,4]. Moreover, excess maternal and fetal mortality can be attributed to various injury-related mechanisms during the crash. Even minor injuries may still cause severe adverse pregnancy outcomes because of delayed recognition of pregnancy(especially involving injuries suffered during the first trimester), maternal morbid obesity, and critically injured pregnant women. As a precaution, a previous study suggested that all women of reproductive age should be considered pregnant until proven otherwise [2].
Although pregnancy could complicate the outcomes after MVCs, existing evidence on whether pregnancy may lead to increased risk of mortality following MVCs remains inconclusive [5,6,7,8,9,10,11]. Some studies have revealed that the better survival rates after trauma among pregnant women are largely attributable to their tendency to be more cautious and concerned with their babies’ safety, and thus they are more likely to seek medical attention than nonpregnant women [11,12]. To summarize the available information on this topic, we conducted this systematic review and meta-analysis to determine whether pregnant women experience an increased risk of mortality after MVCs.
2. Materials and Methods
This review was conducted following the guidelines of the Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement [13], the checklist of which has been included in Supplementary Checklist S1 (PROSPERO Review Protocol and Registration, CRD42020188698).
2.1. Eligibility Criteria
The inclusion criteria were as follows: (1) studies examined the mortality of MVCs, and (2) they were conducted on both pregnant women and nonpregnant women. The exclusion criteria were as follows: (1) case reports, qualitative reports, comments, simulation studies, and reviews; and (2) studies did not report information relevant for the key clinical questions, i.e., studies that reported fatalities of pregnant women due to MVCs but did not provide information about death following MVCs or traumatic injury.
2.2. Search Strategy
A comprehensive, systematic, electronic literature search was conducted using MEDLINE, PubMed, and Embase, regardless of publication timeline, in May 2021. References from the relevant literature were then manually searched and used as a basis for finding more relevant studies. The medical subject headings (MeSH) search terms used were ((Injured AND traffic injury OR accidents OR traffic OR motor vehicle) AND (pregnant or obstetric AND women) AND (mortality OR dead OR survival)) (Supplementary Table S1).
2.3. Risk of Bias Assessment
The revised version of the Newcastle–Ottawa Scale (NOS) for cohort studies was used to assess the quality of the included studies [14]. NOS contains eight items within three domains (selection, comparability, and outcomes). Studies that were assigned four stars for selection, two stars for comparability, and three stars for ascertainment of the outcome, were regarded as having a low risk of bias. Studies with two or three stars for selection, one star for comparability, and two stars for outcome ascertainment, were considered to have a medium risk of bias. Any study with a score of one star for selection or outcome ascertainment, or zero for any of the three domains, was deemed to have a high risk of bias [15]. Studies that were included in the review were assigned scores ranging from 0 to 9. Accepted standards were followed in the evaluation process to ensure objectivity in study selection. Two authors (YH and YY) independently performed all the data abstraction and then identified studies for inclusion or exclusion on the basis of NOS scores. Any discrepancy between the reviewers’ judgments regarding the scoring of a study’s quality was resolved by consensus with a third author (CY).
2.4. Data Extraction
The studies were evaluated on the basis of all relevant information provided in each article. The criteria for study inclusion were based on the relevance of the study’s setting (hospitalized or population-based study), the participants (pregnant and nonpregnant women following MVCs), location (the country which conducted the study), study design (retrospective or cross-sectional design), and sample size (the number of participants). These components were evaluated by the authors and, after the preliminary screening, eight studies were selected for further analysis.
2.5. Data Analysis
We used the odds ratios (OR) as our primary outcome to estimate the magnitude of the effect of pregnancy on the associated risk of death after women are involved in traffic injury. Crude OR were calculated or the adjusted OR of adverse pregnancy outcomes in MVCs victims, with or without pregnancy, were captured for individual studies, both of which were pooled to obtain an overall estimate using random effects models, as heterogeneity between studies was anticipated. Although data were extracted from each original study, the likelihood that some residuals and unexplained factors may exist in each article was acknowledged. Therefore, we proposed that the random effects model was suitable for use under these circumstances. A weighted mean was computed and pooled using a random effects model. Heterogeneity between studies was assessed using the I2 test (0–40%: might not be important; 30–60%: may represent moderate heterogeneity; 50–90%: may represent substantial heterogeneity; and 75–100%: considerable heterogeneity) [16]. All data analyses were performed using the Comprehensive Meta-Analysis Software Version 2 (Biostat, Englewood, NJ, USA). Sensitivity analyses were conducted by removing the study with the largest effect size. Subgroup analyses were accomplished according to the injury severity score (ISS) pattern of the study participants. On the basis of these analyses, an inference was made regarding whether an estimate of mortality could be attributed to the severity levels of the injuries sustained by the participants in the included studies.
3. Results
3.1. Characteristics of Included Studies
Of the 297 articles, 251 were selected and reviewed, and eight observational studies proved eligible (Supplementary Figure S1). These eight studies evaluated and comparatively analyzed the association among retrospective cohort studies (Table 1). These studies included 14,120 pregnant injured victims and 207,935 nonpregnant victims. Most of the studies involved multiple centers and used nationwide data sources to compare pregnant women and nonpregnant women.

Table 1.
Characteristics of studies included herein.
According to the mechanism of injury, two articles enrolled only injured individuals from MVCs. Six articles enrolled trauma patients, of them 36.4–85.1% were due to MVCs (Table 1). Four studies used the age-matched method between pregnant and nonpregnant women (Table 1). The participants’ ages ranged from 12 years to 51 years. Many potential confounders were considered by the selected studies. However, the confounders they analyzed were diverse. Injury severity score was the most common potential factor they assessed.
3.2. Risk of Bias
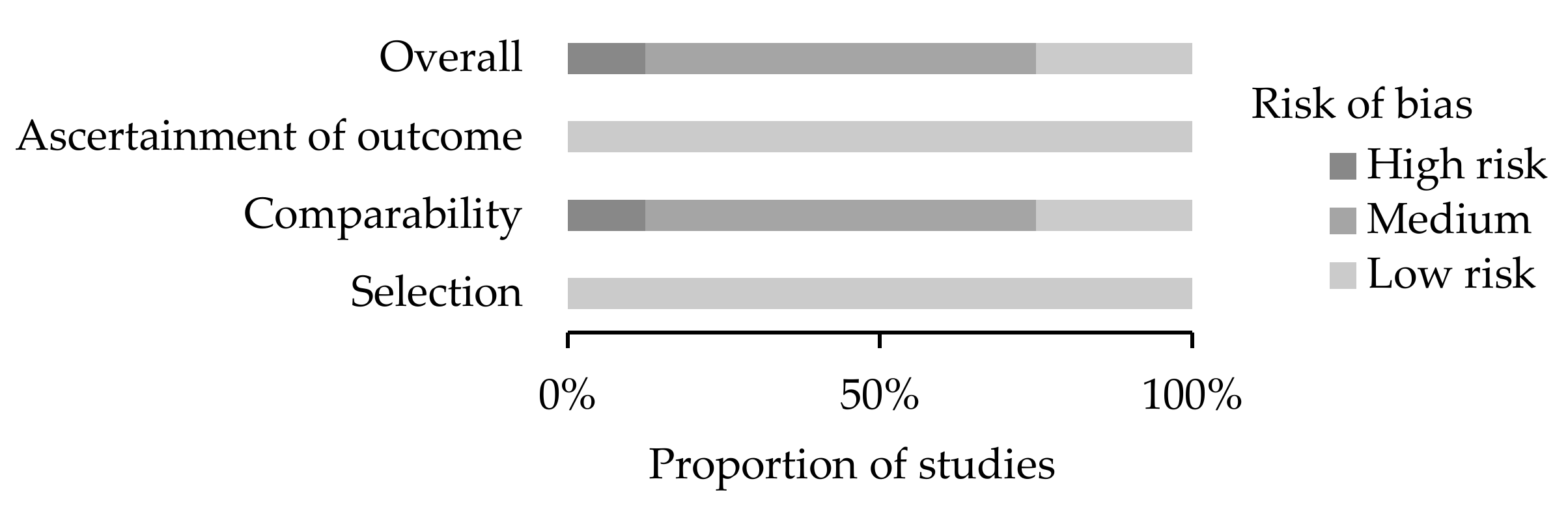
Seven studies were judged of medium/low overall risk of bias, and one study had a high overall risk of bias (Figure 1 and Supplementary Table S2). The main reason for downgrading was the lack of adequate comparability between groups, namely, limited adjustment for confounders between pregnant and nonpregnant women.
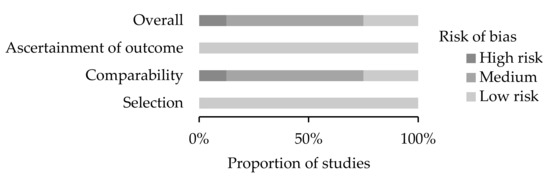
Figure 1.
Quality assessment using the Newcastle–Ottawa Scale of studies included in the present systematic review (n = 8).
3.3. Overall Effects
Eight studies reported the number of deaths among pregnant and nonpregnant women. The number of participants, number of deaths, and ORs in the included studies are summarized in Table 2. In-hospital death records from Deshpande et al. [6] were captured to ensure that the definition of outcome was consistent among the included studies.
Table 2.
Characteristics of studies included herein.
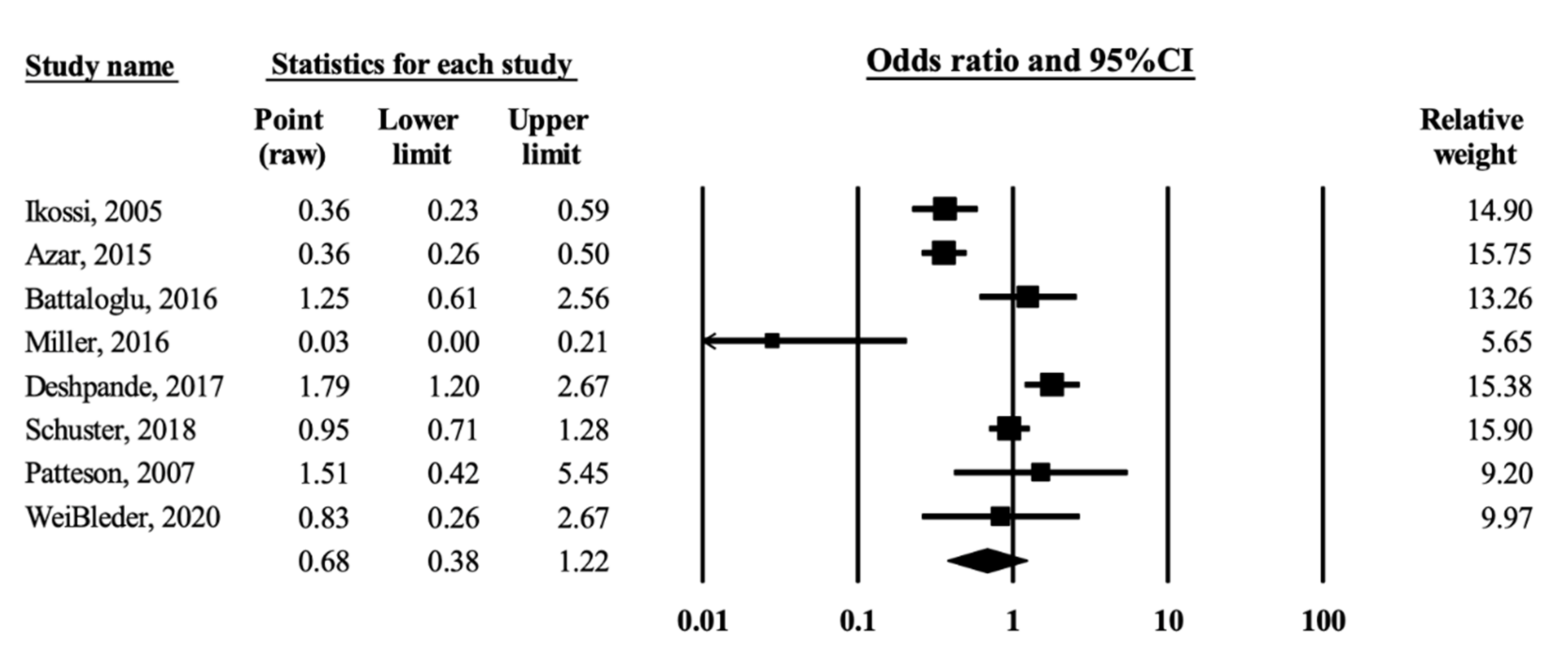
In-hospital mortality was then used as the primary study endpoint. Among the eight studies, injured pregnant women were shown to have a moderate but insignificant association with a lower risk of in-hospital mortality than nonpregnant women after MVCs (OR = 0.68, 95% CI = 0.38–1.22; heterogeneity, Q = 62.03, df = 7, I2 = 88.71%, Figure 2).
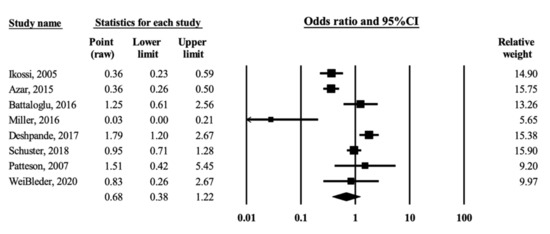
Figure 2.
Forest plot of odds ratio for mortality from motor vehicle crashes in association with pregnancy [5,6,7,8,9,11,17,18]. The black squares represent the odds ratios of the individual studies and the horizontal lines are their 95% CI. The area of the black squares and diamond respectively reflects the weight each trial contributes and the overall effect from the meta-analysis.
3.4. Sensitivity Analysis
One outlier was identified. Sensitivity analysis was performed by removing the study with the largest effect size [8]. The results of the remaining seven studies were insignificant for lower risk of in-hospital mortality among pregnant women than among nonpregnant women (OR = 0.82, 95% CI = 0.47–1.44) but with moderate heterogeneity (Q = 51.72, df = 6, I2 = 88.40%).
3.5. Subgroup Analysis
Although four studies did not explicitly provide the mean ISS for the comparison groups [7,8,9,17], the values from two studies were nevertheless estimated by recalculating the mean through capturing the median of the classified ISS scale and the number of women injured by each ISS stratum [7,8]. Two studies did not provide any ISS information [9,17]. Differences in the mean ISS (ISSD) between pregnant and nonpregnant women were calculated, and the ISSD was categorized into ≤2 and >2. Among the women admitted to hospitals after an MVC, the pregnant women tended to have sustained less severe injures than their nonpregnant age-matched controls [9,17]. Therefore, those studies were considered to be in the ISSD > 2 group.
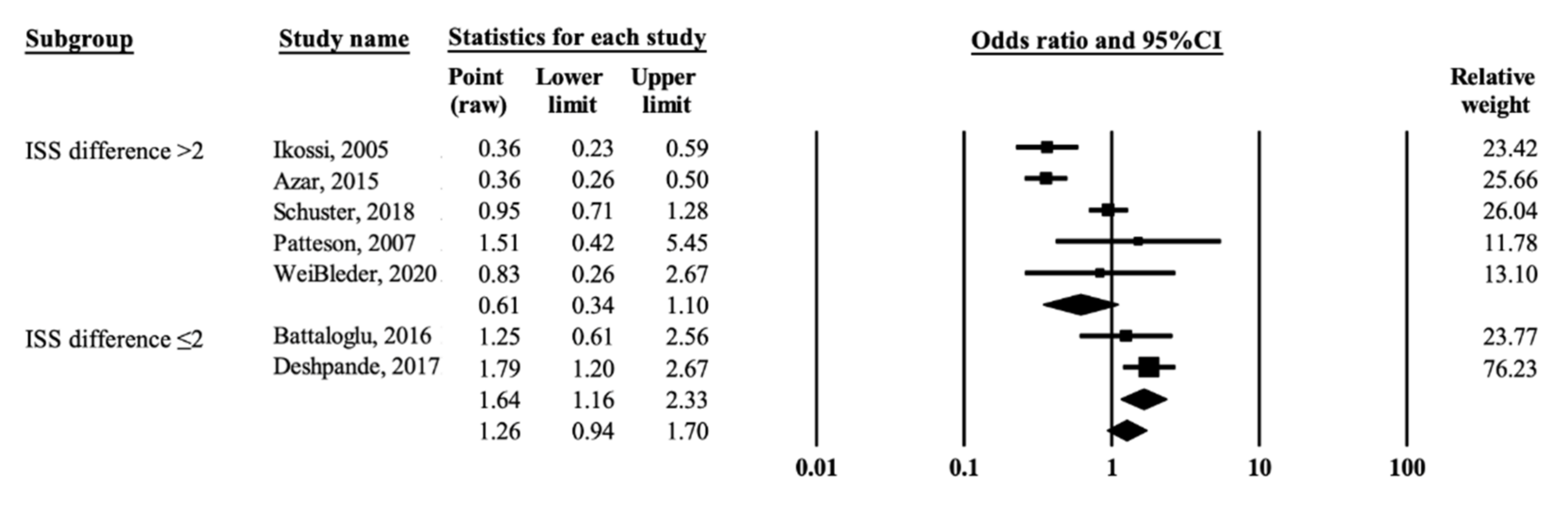
Figure 3 shows the results of subgroup analyses which were performed by removing the outlier [8]. The pooled estimates from the two studies with ISSD ≤ 2 showed a significantly higher risk of mortality in pregnant women than in nonpregnant women (OR = 1.64, 95% CI = 1.16–2.33, p = 0.005) with little heterogeneity (I2 = 0%, p = 0.392). By comparison, the pregnant women tended to have a lower risk of mortality from MVCs than nonpregnant women in the five studies with ISSD > 2 (OR = 0.61, 95% CI = 0.34–1.10, p = 0.099) with obvious heterogeneity (I2 = 83.93%, p ≤ 0.001).
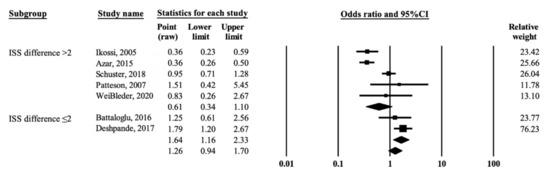
Figure 3.
Forest plot of odds ratio for mortality from motor vehicle crashes in association with pregnancy according to differences in ISS between comparison groups [5,6,7,9,11,17,18]. The black squares represent the odds ratios of the individual studies and the horizontal lines are their 95% CI. The area of the black squares and diamond respectively reflects the weight each trial contributes and the overall effect from the meta-analysis.
4. Discussion
According to the present systematic review, the issue of whether pregnancy increases the risk of mortality in victims involved in MVCs is controversial. This meta-analysis also found that, compared with nonpregnant women, pregnant women were found to have a moderate but insignificantly decreased mortality risk (pooled OR = 0.68, 95% CI = 0.38–1.22, I2 = 88.71%). To explore the sources of heterogeneity, we performed subgroup analyses according to differences in the ISS scale between pregnant and nonpregnant women. However, the pooled OR was significantly increased at 1.64 (95% CI = 1.16–2.33, I2 = 0.00%) for the studies with a similar difference in the mean ISS between pregnant and nonpregnant women. By contrast, the pooled OR tended to be reduced at 0.61 (95% CI = 0.34–1.10, I2 = 83.93%) in favor of pregnant women for the studies in which pregnant women had a lower mean ISS than their nonpregnant counterparts.
The mechanisms by which pregnancy might result in a low risk of mortality remain unclear. On the basis of our findings, we propose that when the inclusion criteria for maternal injury severity are considered, pregnant women have a higher risk of mortality than nonpregnant women due to pregnant women’s altered physiologic state, which in turn also affects their response to trauma [19,20,21]. Mothers obviously undergo physiological and anatomical changes during pregnancy, including increases in both plasma volume and cardiac output. These changes, combined with the shunting of blood away from the uteroplacental circulation after blood loss, may initially mask signs of hypovolemia [22]. Furthermore, pregnant women are at risk for aortocaval compression syndrome when in a supine position, and this may also confuse the interpretation of their vital signs [23]. These anatomical and physiological changes may affect the level of care extended to the injured trauma patient, thereby presenting a challenge to trauma surgeons. Moreover, these changes may explain the increase in mortality among women who sustain injury during pregnancy.
The inconsistency in the results of previous studies may be attributed to the potential for surveillance bias (also known as detection bias) [24]. Most studies reported that pregnant women are more likely to visit clinical institutions to confirm their baby’s safety after a crash than nonpregnant women, regardless of injury severity [11,25]. Furthermore, clinicians are prone to arrange admission for closer checkup or monitoring if a pregnant woman is hospitalized because of an MVC. Prior studies have demonstrated that nearly 60% of pregnant women were admitted to hospitals or emergency units after crashes, but only 34% of nonpregnant women were admitted [12,25]. Hence, well-monitored pregnant women had been observed to have a lesser injury severity than unmonitored nonpregnant women [11]. By contrast, among nonpregnant women, only those who sustained moderate injury severity were admitted to hospitals, leading to a misconception that nonpregnant women are associated with a higher risk of mortality after MVCs than pregnant women. This misconception was consistent with the present findings of a lower mortality risk in pregnant women than in nonpregnant women. However, a strong positive relationship between pregnancy and risk of mortality was observed after limiting the results to studies with differences in ISS of less than 2 between pregnant and nonpregnant women.
In general, the ISS scale is one of the most precise predictors of mortality in trauma patients. The ISS has been validated for predicting mortality after trauma in nonpregnant women [26]. However, Miller et al. [8] indicated that the ISS score might not be a useful predictive risk factor for pregnancy outcomes as they did not find a significant correlation between ISS and immediate adverse maternal–fetal pregnancy outcomes (p-value < 0.722). Schiff and Holt [3] also reiterated that the ISS is not accurate in predicting placental abruption in a study of hospitalized pregnant women following experiences of trauma. In fact, the relationship between the ISS and mortality risk in pregnant women is unclear due to the small number of maternal deaths reported in prior studies [3,12,27].
Apart from the potential confounding factor of the ISS, another possible confounder might have affected the results of previous studies. The possible dissimilarity in risk-taking behavior between pregnant and nonpregnant women, and its contribution to the low risk of mortality noted in previous studies cannot be discounted. Pregnant women may be more cautious in an effort to protect their babies. Previous studies show that pregnant women have better compliance with seatbelt use (66%) than nonpregnant women (50%) [11]. Therefore, pregnant women display behaviors that reduce risks, such as wearing a seat belt or being a passenger instead of the driver, and these behaviors may prevent pregnant women suffering a severe injury in a traumatic event. However, the possible risk reduction behaviors adopted by pregnant women were not considered in previous studies.
Selection bias is another possible source of bias in previous studies. Studies on the relationship between pregnancy and MVC-related mortality were conducted in various healthcare settings, including trauma centers or hospitals and clinic institutions. However, some injured victims might possibly have died at the scene and therefore, were not captured in data from clinical settings. Most medical institution-based studies enrolled trauma patients only when they visited or were transported to hospitals or trauma centers [5,7,8,9,11,17,18]. These patients’ conditions were likely to be categorized as moderate in relation to injury severity. A potential selection bias might arise if a study was based only on patients with MVC-related injuries seen in medical institutions [28]. The underrepresentation of out-of-hospital cardiac arrest (OCHA) cases might have also biased, at least to some extent, the results of previous studies. A population-based study design or patient enrollment that includes all pregnant women who experience MVCs may help reduce the potential selection bias (or survival bias) owing to the exclusion of OCHA cases or those cases where women did not seek clinical care after MVCs [6].
Strengths and Limitations
We conducted this review by using a prospectively registered protocol and reported it in accordance with international standards [29]. To the best of our knowledge, this review is the first meta-analysis to examine the potential role of pregnancy in the associations between mortality and victims involved in MVCs. We used established tools to assess outcome reporting quality for the risk of bias [13,14].
The weaknesses of this systematic review are as follows. Firstly, the mean ISS was not available in two studies. Secondly, the adverse outcomes following MVCs, including mortality, can be affected by various factors, such as adherence to seat belt use [30], type of vehicle [31], and quality of medical care [32]. Unfortunately, very few studies considered these safety features in their analysis, thus limiting the interpretation of the present results on the relationship between pregnancy and mortality following MVCs. Thirdly, we found only a limited number of relevant studies that compared mortality after MVCs between pregnant and nonpregnant women. Furthermore, almost all of the included studies were conducted in the US, and the most recent one was published in 2020. Given that road conditions and safety driving features have improved in recent years, this metal-analysis was unable to provide the most up-to-date information. Fourthly, only two of the included studies specifically assessed injury severity following MVCs. The other six studies involved participants with trauma due to various causes. Nevertheless, most of the included studies evaluated MVCs as the major cause of trauma. Finally, we did not consider the initial (baseline) health conditions of the women in both groups in our analysis, primarily because none of the included studies mentioned the medical history of the study participants before the MVCs.
5. Conclusions
After risk stratification (i.e., ISS), this meta-analysis observed a moderate but positive association between pregnancy and mortality in women after MVCs. Some previous studies that compared mortality risk after MVCs between pregnant and nonpregnant women might have been affected by potential confounding factors, due to dissimilarities in injury severity and safety features. Additionally, prior studies based on clinical settings were subject to selection bias arising from the exclusion of OCHA cases, uninjured cases, and mildly injured cases who did not require medical care.
This review suggests a need for additional original research with improved methodology to provide better quantitative evidence concerning mortality risk in relation to pregnancy after MVCs. Understanding how pregnancy may be associated with the risk of death in the context of traffic incidents has the potential to lead to improved treatments, including both emergency medical and prenatal care.
Supplementary Materials
The following are available online at https://www.mdpi.com/article/10.3390/ijerph19020911/s1, Checklist S1: PRISMA Checklist of the study, Figure S1: PRISMA flow chart describing the inclusion and exclusion processes, Table S1: Searching strategy, Table S2: Quality score of the included studies.
Author Contributions
Conceptualization, Software, Formal Analysis, Validation, Data Curation, Writing–Original Draft, Y.-H.C. and Y.-Y.C.; Conceptualization, Supervision, Y.-W.C., C.-H.C., P.-L.C., T.-H.L. and L.Y.H.; Conceptualization, Methodology, Data Curation, Writing–Reviewing and Editing, Supervision, Project Administration, C.-Y.L., W.-H.H. and N.-P.F. All authors have read and agree to the published version of manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Petrone, P.; Jiménez-Morillas, P.; Axelrad, A.; Marini, C.P. Traumatic injuries to the pregnant patient: A critical literature review. Eur. J. Trauma Emerg. Surg. 2019, 45, 383–392. [Google Scholar] [CrossRef] [PubMed]
- Sakamoto, J.; Michels, C.; Eisfelder, B.; Joshi, N. Trauma in pregnancy. Emerg. Med. Clin. N. Am. 2019, 37, 317–338. [Google Scholar] [CrossRef] [PubMed]
- Schiff, M.A.; Holt, V.L. The injury severity score in pregnant trauma patients: Predicting placental abruption and fetal death. J. Trauma 2002, 53, 946–949. [Google Scholar] [CrossRef] [PubMed]
- Vladutiu, C.J.; Weiss, H.B. Motor vehicle safety during pregnancy. Am. J. Lifestyle Med. 2012, 6, 241–249. [Google Scholar] [CrossRef]
- Schuster, M.; Becker, N.; Young, A.; Paglia, M.J.; Mackeen, A.D. Trauma in pregnancy: A review of the Pennsylvania Trauma Systems Foundation database. Trauma 2018, 20, 30–37. [Google Scholar] [CrossRef] [Green Version]
- Deshpande, N.A.; Kucirka, L.M.; Smith, R.N.; Oxford, C.M. Pregnant trauma victims experience nearly 2-fold higher mortality compared to their nonpregnant counterparts. Am. J. Obstet. Gynecol. 2017, 217, 590.e1–590.e9. [Google Scholar] [CrossRef]
- Battaloglu, E.; McDonnell, D.; Chu, J.; Lecky, F.; Porter, K. Epidemiology and outcomes of pregnancy and obstetric complications in trauma in the United Kingdom. Injury 2016, 47, 184–187. [Google Scholar] [CrossRef]
- Miller, N.; Biron-Shental, T.; Peleg, K.; Fishman, A.; Olsha, O.; Givon, A.; Kessel, B. Are pregnant women safer in motor vehicle accidents? J. Perinat. Med. 2016, 44, 329–332. [Google Scholar] [CrossRef]
- Azar, T.; Longo, C.; Oddy, L.; Abenhaim, H.A. Motor vehicle collision-related accidents in pregnancy. J. Obstet. Gynaecol. Res. 2015, 41, 1370–1376. [Google Scholar] [CrossRef]
- Kvarnstrand, L.; Milsom, I.; Lekander, T.; Druid, H.; Jacobsson, B. Maternal fatalities, fetal and neonatal deaths related to motor vehicle crashes during pregnancy: A national population-based study. Acta Obstet. Gynecol. Scand. 2008, 87, 946–952. [Google Scholar] [CrossRef]
- Ikossi, D.G.; Lazar, A.A.; Morabito, D.; Fildes, J.; Knudson, M.M. Profile of mothers at risk: An analysis of injury and pregnancy loss in 1,195 trauma patients. J. Am. Coll. Surg. 2005, 200, 49–56. [Google Scholar] [CrossRef]
- Aboutanos, M.B.; Aboutanos, S.Z.; Dompkowski, D.; Duane, T.M.; Malhotra, A.K.; Ivatury, R.R. Significance of motor vehicle crashes and pelvic injury on fetal mortality: A five-year insititutional review. J. Trauma 2008, 65, 616–620. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle–Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses [Article Online]. Ottawa Hospital Research Institute Web site. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 13 April 2021).
- Sobhy, S.; Babiker, Z.; Zamora, J.; Khan, K.; Kunst, H. Maternal and perinatal mortality and morbidity associated with tuberculosis during pregnancy and the postpartum period: A systematic review and meta-analysis. BJOG Int. J. Obstet. Gynaecol. 2017, 124, 727–733. [Google Scholar] [CrossRef]
- Deeks, J.J.; Higgins, J.P.T.; Altman, D.G. Chapter 10: Analysing data and undertaking meta-analyses. In Cochrane Handbook for Systematic Reviews of Interventions Version 6.2 (Updated 2021); Higgins, J.P.T., Green, S., Eds.; The Cochrane Collaboration: Chichester, UK, 2021; Available online: https://training.cochrane.org/handbook/current/chapter-10 (accessed on 13 April 2021).
- Patteson, S.K.; Snider, C.C.; Meyer, D.S.; Enderson, B.L.; Armstrong, J.E.; Whitaker, G.L.; Carroll, R.C. The consequences of high-risk behaviors: Trauma during pregnancy. J. Trauma Acute Care Surg. 2007, 62, 1015–1020. [Google Scholar] [CrossRef]
- Weißleder, A.; Kulla, M.; Annecke, T.; Beese, A.; Lang, P. Akutbehandlung schwangerer Patientinnen nach schwerem trauma—eine retrospektive multicenteranalyse. Der Unf. 2020, 123, 944–953. (In German) [Google Scholar] [CrossRef]
- Rodriguez, A.; Bohlin, G.; Lindmark, G. Symptoms across pregnancy in relation to psychosocial and biomedical factors. Acta Obstet. Gynecol. Scand. 2001, 80, 213–223. [Google Scholar] [CrossRef]
- Taylor, A.H.; Dorn, L. Stress, fatigue, health, and risk of road traffic accidents among professional drivers: The contribution of physical inactivity. Annu. Rev. Public Health 2006, 27, 371–391. [Google Scholar] [CrossRef] [Green Version]
- McCall, S.J.; Bhattacharya, S. High risk of traffic crashes in pregnancy: Are there any explanations? Can. Med Assoc. J. 2014, 186, 733–734. [Google Scholar] [CrossRef] [Green Version]
- Esposito, T.J. Trauma during pregnancy. Emerg. Med. Clin. N. Am. 1994, 12, 167–199. [Google Scholar] [CrossRef]
- Shah, K.H.; Simons, R.K.; Holbrook, T.; Fortlage, D.; Winchell, R.J.; Hoyt, D.B. Trauma in pregnancy: Maternal and fetal outcomes. J. Trauma 1998, 45, 83–86. [Google Scholar] [CrossRef]
- Haut, E.R.; Pronovost, P.J. Surveillance bias in outcomes reporting. JAMA 2011, 305, 2462–2463. [Google Scholar] [CrossRef]
- Weiss, H.B.; Strotmeyer, S. Characteristics of pregnant women in motor vehicle crashes. Inj. Prev. 2002, 8, 207–210. [Google Scholar] [CrossRef]
- Baker, S.P.; O’Neill, B.; Haddon, W.; Long, W.B. The injury severity score: A method for describing patients with multiple injures and evaluating emergency care. J. Trauma 1974, 14, 187–196. [Google Scholar] [CrossRef]
- Baerga-Varela, Y.; Zietlow, S.P.; Bannon, M.P.; Harmsen, W.S.; Ilstrup, D.M. Trauma in pregnancy. Mayo Clin. Proc. 2000, 75, 1243–1248. [Google Scholar] [CrossRef]
- Schiff, M.A.; Holt, V.L. Pregnancy outcomes following hospitalization for motor vehicle crashes in Washington state from 1989 to 2001. Am. J. Epidemiol. 2005, 161, 503–510. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. Ann. Intern. Med. 2009, 151, W65–W94. [Google Scholar] [CrossRef] [Green Version]
- Wolf, M.E.; Alexander, B.H.; Rivara, F.P.; Hickok, D.E.; Maier, R.V.; Starzyk, P.M. A retrospective cohort study of seatbelt use and pregnancy outcome after a motor vehicle crash. J. Trauma 1993, 34, 116–119. [Google Scholar] [CrossRef] [PubMed]
- Xiong, L.; Li, L. Single-vehicle and multi-vehicle accidents involving motorcycles in a small city in China: Characteristics and injury patterns. AIMS Public Health 2015, 2, 75–85. [Google Scholar] [CrossRef]
- Distelhorst, J.T.; Krishnamoorthy, V.; Schiff, M.A. Association between hospital trauma designation and maternal and neonatal outcomes after injury among pregnant women in Washington State. J. Am. Coll. Surg. 2016, 222, 296–302. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).