
Knowledge, Attitudes, and Practices on Tick-Borne Encephalitis Virus and Tick-Borne Diseases within Professionally Tick-Exposed Persons, Health Care Workers, and General Population in Serbia: A Questionnaire-Based Study


 , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
- Entity characteristics: a place of residence (free entry); age (free entry); sex; educational level; having children under the age of 18; having dog(s); being a professionally tick-exposed person; experiencing a tick bite in a lifetime; having TBD(s); having a family member diagnosed with TBD(s); being a health care worker; and employment in primary health care in Serbia.
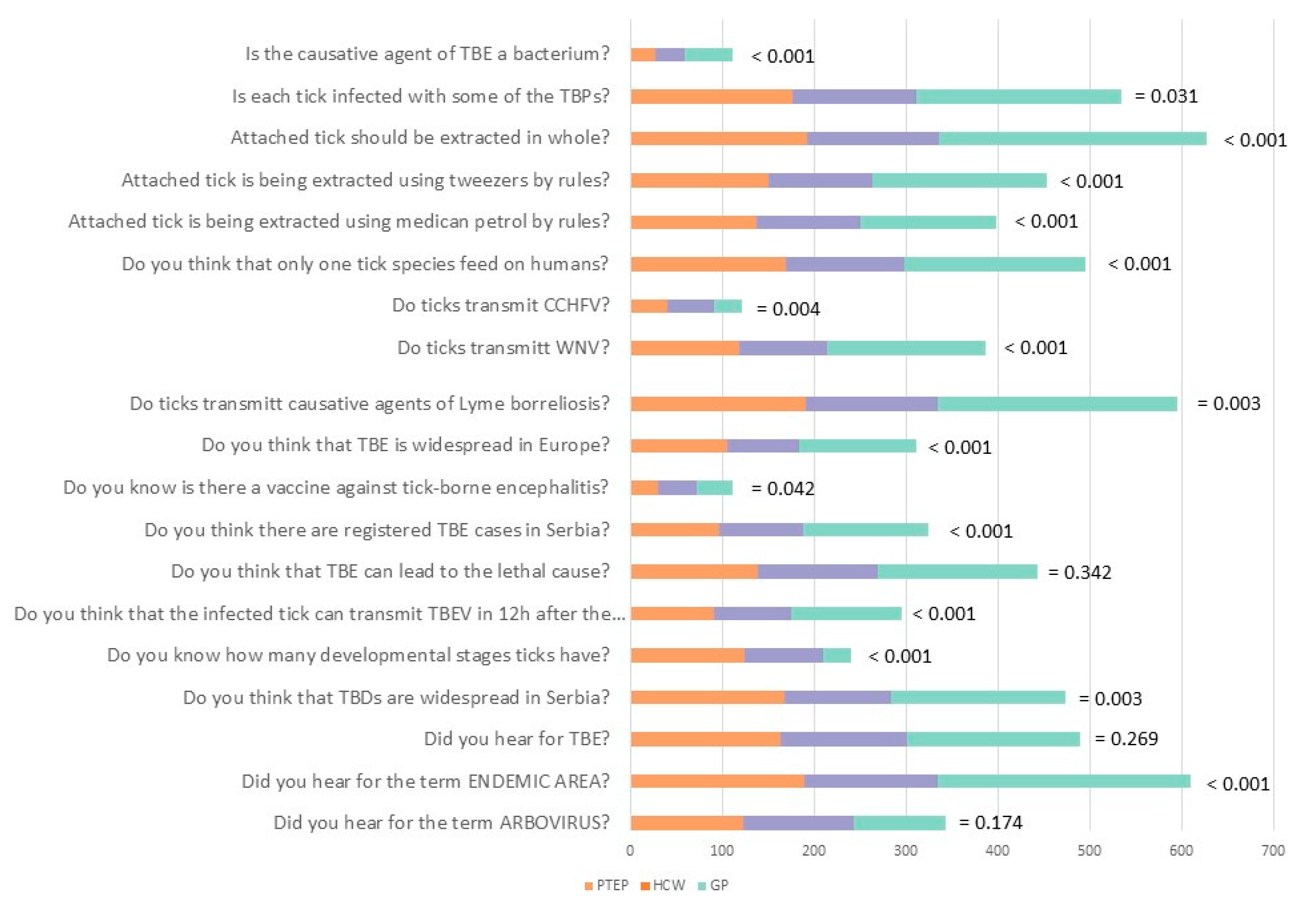
- Knowledge and opinion towards ticks and TBPs: familiarity with the term “arbovirus”; endemic area; TBE; frequency of TBDs in Serbia; number of developmental stages of ticks; time frame in which ticks could transmit a TBEV; the possible lethal outcome of TBE; registered cases of TBE in Serbia; availability of the vaccine against TBE in the world; the occurrence of TBE in Europe; whether ticks can transmit causative agents of Lyme borreliosis; West Nile fever (WNV); Crimean–Congo hemorrhagic fever (CCHF); whether only one tick species could transmit tick-borne pathogens; whether the tick should be removed from the skin by use of medical oil, tweezer and in whole; whether every tick is infected with TBP(s); and whether the causative agent of TBE is a bacterium. Each of the 19 items was presented as a binary forced-choice (Yes/No) response to statements with the “I don’t know” option.
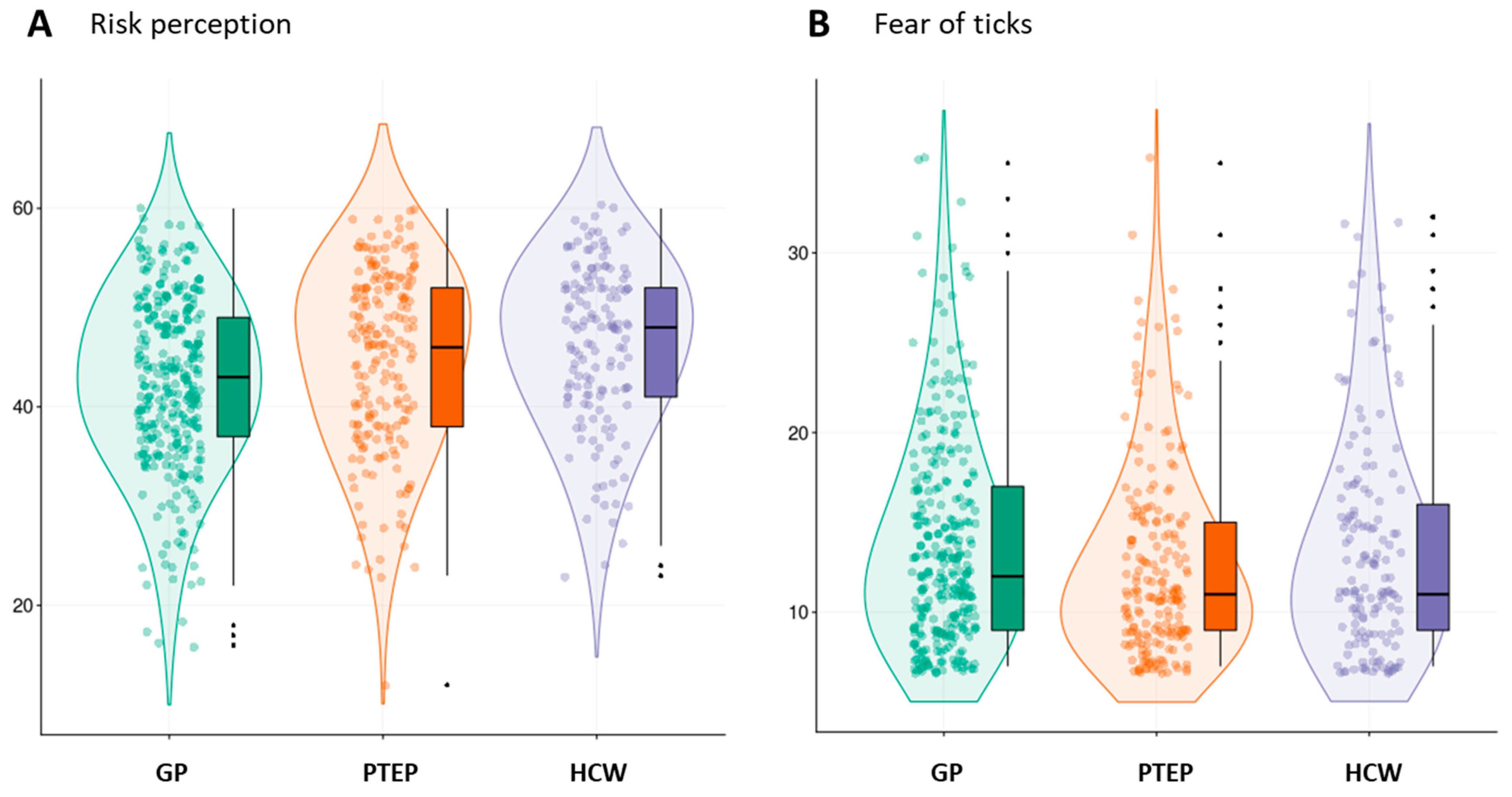
- Attitudes towards ticks and TBDs through the estimation of (a) risk and risk perception from ticks and TBDs: entering risky situations in general, being in nature and long-term being in nature as a risk of tick-bite, whether a tick bite could lead to the development of TBD(s), whether TBE could be deadly, whether the risk of TBE in Europe is increasing, whether vaccination could prevent TBE, walking through or on fields/woods/river banks/paths as a risk of a tick bite, whether ticks can pass from dog to human, whether tick bites are significant cause of concern; and (b) fear of ticks and TBDs: fear of ticks, TBDs, whether the fear of tick bite affects one’s desire towards spending time in nature, whether the fear of ticks repels people from grass areas, whether the fear of ticks prevents children playing in grass, whether the fear of ticks and TBPs influences everyday life, and whether the fear of TBE influences everyday life. The items were assessed through a 5-point Likert type scale (1—strongly disagree; 5—strongly agree).
- Protective behavior towards ticks and TBDs: use of repellents; wearing long sleeves; white clothes; socks; avoiding high grass; checking one’s skin after being in nature; protection against ticks; using tick repellent on dogs; vaccination against TBE and testing to TBDs; informing oneself through a chosen medical doctor with regard to what vaccinations are needed before trips abroad; protection in the workplace; acceptance of vaccination towards TBPs in general; informing about TBDs and tick control programs; and whether having a dog increases the risk of acquiring a TBD. Items were presented as a binary forced choice (Yes/No) response to statements in addition to the “I don’t know” option.
3. Results
3.1. Knowledge about Ticks and TBDs in Serbia
3.2. Attitudes towards TBD
3.3. Protective Practices
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kernif, T.; Leulmi, H.; Raoult, D.; Parola, P. Emerging Tick-Borne Bacterial Pathogens. Microbiol. Spectr. 2016, 4. [Google Scholar] [CrossRef]
- Efstratiou, A.; Karanis, G.; Karanis, P. Tick-Borne Pathogens and Diseases in Greece. Microorganisms 2021, 9, 1732. [Google Scholar] [CrossRef]
- Van Den Wijngaard, C.C.; Hofhuis, A.; Wong, A.; Harms, M.G.; De Wit, G.A.; Lugnér, A.K.; Suijkerbuijk, A.W.M.; Mangen, M.J.J.; Van Pelt, W. The cost of Lyme borreliosis. Eur. J. Public Health 2017, 27, 538–547. [Google Scholar] [CrossRef]
- Müller, I.; Freitag, M.H.; Poggensee, G.; Scharnetzky, E.; Straube, E.; Schoerner, C.; Hlobil, H.; Hagedorn, H.J.; Stanek, G.; Schubert-Unkmeir, A.; et al. Evaluating frequency, diagnostic quality, and cost of lyme borreliosis testing in Germany: A retrospective model analysis. Clin. Dev. Immunol. 2012, 2012, 595427. [Google Scholar] [CrossRef]
- Beauté, J.; Spiteri, G.; Warns-Petit, E.; Zeller, H. Tick-borne encephalitis in europe, 2012 to 2016. Eurosurveillance 2018, 23, 1800201. [Google Scholar] [CrossRef]
- Bogovic, P.; Strle, F. Tick-borne encephalitis: A review of epidemiology, clinical characteristics, and management. World J. Clin. Cases 2015, 3, 430. [Google Scholar] [CrossRef]
- Frimmel, S.; Krienke, A.; Riebold, D.; Loebermann, M.; Littmann, M.; Fiedler, K.; Klaus, C.; Süss, J.; Reisinger, E.C. Tick-borne encephalitis virus habitats in north East Germany: Reemergence of TBEV in ticks after 15 years of inactivity. BioMed Res. Int. 2014, 2014, 8–11. [Google Scholar] [CrossRef]
- Amato-Gauci, A.J.; Zeller, H. Tick-borne encephalitis joins the diseases under surveillance in the European Union. Eurosurveillance 2012, 17, 20299. [Google Scholar] [CrossRef]
- Šmit, R.; Postma, M.J. Review of tick-borne encephalitis and vaccines: Clinical and economical aspects. Expert Rev. Vaccines 2015, 14, 737–747. [Google Scholar] [CrossRef]
- Taba, P.; Schmutzhard, E.; Forsberg, P.; Lutsar, I.; Ljøstad, U.; Mygland, Å.; Levchenko, I.; Strle, F.; Steiner, I. EAN consensus review on prevention, diagnosis and management of tick-borne encephalitis. Eur. J. Neurol. 2017, 24, 1214-e61. [Google Scholar] [CrossRef]
- Charrel, R.N.; Attoui, H.; Butenko, A.M.; Clegg, J.C.; Deubel, V.; Frolova, T.V.; Gould, E.A.; Gritsun, T.S.; Heinz, F.X.; Labuda, M.; et al. Tick-borne virus diseases of human interest in Europe. Clin. Microbiol. Infect. 2004, 10, 1040–1055. [Google Scholar] [CrossRef]
- Demina, T.V.; Dzhioev, Y.P.; Verkhozina, M.M.; Kozlova, I.V.; Tkachev, S.E.; Plyusnin, A.; Doroshchenko, E.K.; Lisak, O.V.; Zlobin, V.I. Genotyping and characterisation of the geographical distribution of tick-borne encephalitis virus variants with a set of molecular probes. J. Med. Virol. 2010, 82, 965–976. [Google Scholar] [CrossRef]
- Valeryevna, K.I.; Vasilievna, D.T.; Evgenyevich, T.S.; Konstantinovna, D.E.; Vasilievna, L.O.; Mihailovna, V.M.; Stanislavovna, K.L.; Pavlovich, D.Y.; Igorevich, P.A.; Vladimirovna, S.O.; et al. Characteristics of the baikal subtype of tick-borne encephalitis virus circulating in eastern siberia. Acta Biomed. Sci. 2018, 3, 53–60. [Google Scholar] [CrossRef]
- Dai, X.; Shang, G.; Lu, S.; Yang, J.; Xu, J. A new subtype of eastern tick-borne encephalitis virus discovered in Qinghai-Tibet Plateau, China article. Emerg. Microbes Infect. 2018, 7, 1–9. [Google Scholar] [CrossRef]
- European Food Safety Authority (EFSA). Scientific Opinion on the public health risks related to the consumption of raw drinking milk. EFSA J. 2015, 13, 3940. [Google Scholar] [CrossRef]
- Michelitsch, A.; Wernike, K.; Klaus, C.; Dobler, G.; Beer, M. Exploring the reservoir hosts of tick-borne encephalitis virus. Viruses 2019, 11, 669. [Google Scholar] [CrossRef]
- Ličková, M.; Fumačová Havlíková, S.; Sláviková, M.; Slovák, M.; Drexler, J.F.; Klempa, B. Dermacentor reticulatus is a vector of tick-borne encephalitis virus. Ticks Tick-Borne Dis. 2020, 11, 101414. [Google Scholar] [CrossRef]
- Chitimia-Dobler, L.; Lemhöfer, G.; Król, N.; Bestehorn, M.; Dobler, G.; Pfeffer, M. Repeated isolation of tick-borne encephalitis virus from adult Dermacentor reticulatus ticks in an endemic area in Germany. Parasites Vectors 2019, 12, 1–8. [Google Scholar] [CrossRef]
- Bordjoški, M.; Gligić, A.; Bosković, R. [Arbovirus infections in Serbia]. Vojnosanit. Pregl. 1972, 29, 173–175. [Google Scholar]
- Hrnjaković-Cvjetković, I.; Cvjetković, D.; Patić, A.; Radovanov, J.; Kovačević, G.; Milošević, V. Tick-borne encephalitis virus infection in humans. Med. Pregl. 2016, 69, 93–98. [Google Scholar] [CrossRef][Green Version]
- Banović, P.; Budakov-Obradović, Z.; Grujić, J.; Cabezas-Cruz, A. Tick-Borne Encephalitis Virus Seropositivity among Tick Infested Individuals in Serbia. Pathogens 2021, 10, 301. [Google Scholar] [CrossRef]
- Poluga, J.; Barac, A.; Katanic, N.; Rubino, S.; Milosevic, B. Original Article Tick-borne encephalitis in Serbia: A case series. J. Infect. Dev. Ctries. 2019, 13, 510–515. [Google Scholar] [CrossRef]
- Potkonjak, A.; Savic, S. Molecular Detection and Serological Evidence. Vector-Borne Zoonotic Dis. 2017, 17, 813–820. [Google Scholar] [CrossRef]
- Dimitrijevic, D.; Drakulic, M.; Kanazir, M.; Loncarevic, G.; Milinkovic, M.; Milosavljevic, Z.; Plavsa, D.; Rakic, V.; Simic, D.; Stosic, M.; et al. Izvestaj o Zaraznim Bolestima u Republici Srbiji za 2019. Godinu; Institut za javno zdravlje Srbije Dr. Milan Jovanovic Batut: Belgrade, Serbia, 2020. [Google Scholar]
- Martin, V.; Chevalier, V.; Ceccato, P.; Anyamba, A.; De Simone, L.; Lubroth, J.; De La Rocque, S.; Domenech, J. The impact of climate change on the epidemiology and control of Rift Valley fever. Rev. Sci. Tech. 2008, 27, 413–426. [Google Scholar] [CrossRef]
- Schulte, P.A.; Chun, H. Climate Change and Occupational Safety and Health: Establishing a Preliminary Framework. J. Occup. Environ. Hyg. 2009, 9624, 542–554. [Google Scholar] [CrossRef]
- Tomao, P.; Ciceroni, L.; D’Ovidio, M.C.; De Rosa, M.; Vonesch, N.; Iavicoli, S.; Signorini, S.; Ciarrocchi, S.; Ciufolini, M.G.; Fiorentini, C.; et al. Prevalence and incidence of antibodies to Borrelia burgdorferi and to tick-borne encephalitis virus in agricultural and forestry workers from Tuscany, Italy. Eur. J. Clin. Microbiol. Infect. Dis. 2005, 24, 457–463. [Google Scholar] [CrossRef]
- Süss, J.; Kahl, O.; Aspöck, H.; Hartelt, K.; Vaheri, A.; Oehme, R.; Hasle, G.; Daute, H.; Kunz, C.; Kupreviciene, N.; et al. Tick-borne encephalitis in the age of general mobility. Wien. Med. Wochenschr. 2010, 160, 94–100. [Google Scholar] [CrossRef]
- Cisak, E.; Sroka, J.; Zwolinski, J.; Uminski, J. Seroepidemiological study on tick-borne encephalitis among forestry workers and farmers from the Lublin region (Eastern Poland). Ann. Agric. Environ. Med. 1998, 5, 177–181. [Google Scholar]
- Mowbray, F.; Amlôt, R.; James Rubin, G. Ticking all the boxes? A systematic review of education and communication interventions to prevent tick-borne disease. Vector-Borne Zoonotic Dis. 2012, 12, 817–825. [Google Scholar] [CrossRef]
- Stefanoff, P.; Zielicka-hardy, A.; Hlebowicz, M.; Konior, R.; Lipowski, D.; Szenborn, L.; Siennicka, J.; Orlikova, H. New endemic foci of tick-borne encephalitis (TBE) identified in districts where testing for TBE was not available before 2009 in Poland. Parasites Vectors 2013, 6, 180. [Google Scholar] [CrossRef]
- Hochbaum, G.; Rosenstock, I.; Kegels, S. Health Belief Model; United States Public Health Service: Washington, DC, USA, 1952. [Google Scholar]
- Donohoe, H.; Omodior, O.; Roe, J. Tick-borne disease occupational risks and behaviors of Florida Fish, Wildlife, and Parks Service employees—A health belief model perspective. J. Outdoor Recreat. Tour. 2018, 22, 9–17. [Google Scholar] [CrossRef]
- Rogers, R.W. A protection motivation theory of fear appeals and attitude change1. J. Psychol. 1975, 91, 93–114. [Google Scholar] [CrossRef]
- Rattay, P.; Michalski, N.; Domanska, O.M.; Kaltwasser, A.; De Bock, F.; Wieler, L.H.; Jordan, S. Differences in risk perception, knowledge and protective behaviour regarding COVID-19 by education level among women and men in Germany. Results from the COVID-19 Snapshot Monitoring (COSMO) study. PLoS ONE 2021, 16, e0251694. [Google Scholar] [CrossRef]
- Martin Haditsch, U.K. Tick-borne encephalitis: A disease neglected by travel medicine. Travel Med. Infect. Dis. 2013, 11, 295–300. [Google Scholar] [CrossRef]
- Zöldi, V.; Turunen, T.; Lyytikäinen, O.; Sane, J. Knowledge, attitudes, and practices regarding ticks and tick-borne diseases, Finland. Ticks Tick-Borne Dis. 2017, 8, 872–877. [Google Scholar] [CrossRef]
- Zielicka-Hardy, A.; Rosińska, M.; Kondrusik, M.; Konior, R.; Stefanoff, P.; Rosińska, M.; Kondrusik, M. Predictors for diagnosis of tick-borne encephalitis infection in Poland, 2009–2010. Infect. Dis. 2015, 47, 604–610. [Google Scholar] [CrossRef]
- Riccò, M.; Gualerzi, G.; Ranzieri, S.; Ferraro, P.; Bragazzi, N.L. Knowledge, Attitudes, Practices (KAP) of Italian Occupational Physicians towards Tick Borne Encephalitis. Trop. Med. Infect. Dis. 2020, 5, 117. [Google Scholar] [CrossRef]
- Vandererven, C.; Bellanger, A.P.; Faucher, J.F.; Marguet, P. Primary care physician management of tick bites in the Franche-Comté region (Eastern France, 2013). Med. Et Mal. Infect. 2017, 47, 261–265. [Google Scholar] [CrossRef]
- Buczek, A.; Pilch, J.; Buczek, W. Tick Preventive Behaviors and Practices Adopted by Medical Students from Poland, Germany, and Thailand in Relation to Socio-Demographic Conditions and Their Knowledge of Ticks and Tick-Borne Diseases. Insects 2020, 11, 863. [Google Scholar] [CrossRef]
- Thorin, C.; Rigaud, E.; Capek, I.; André-Fontaine, G.; Oster, B.; Gastinger, G.; Abadia, G. Séroprévalence de la borréliose de Lyme et de l’encéphalite à tiques chez des professionnels exposés dans le Grand Est de la France. Med. Mal. Infect. 2008, 38, 533–542. [Google Scholar] [CrossRef]
- Jones, C.L.; Jensen, J.D.; Scherr, C.L.; Brown, N.R.; Christy, K.; Weaver, J. The Health Belief Model as an explanatory framework in communication research: Exploring parallel, serial, and moderated mediation. Health Commun. 2015, 30, 566–576. [Google Scholar] [CrossRef]
- Becker, M.H. The Health Belief Model and personal health behaviour. Health Educ. Monographs. 1974, 2, 324–508. [Google Scholar] [CrossRef]
- Wesołowski, R.; Woźniak, A.; Mila-Kierzenkowska, C. The importance of tick-borne diseases in public health. Med. Biol. Sci. 2014, 28, 51. [Google Scholar] [CrossRef]
- Slunge, D.; Jore, S.; Krogfelt, K.A.; Jepsen, M.T.; Boman, A. Who is afraid of ticks and tick-borne diseases? Results from a cross-sectional survey in Scandinavia. BMC Public Health 2019, 19, 1666. [Google Scholar] [CrossRef]
- Prokop, P.; Fančovičová, J.; Fedor, P. Health Is Associated With Antiparasite Behavior and Fear of Disease-Relevant Animals in Humans. Ecol. Psychol. 2010, 23, 222–237. [Google Scholar] [CrossRef]
- Gierlach, E.; Belsher, B.E.; Beutler, L.E. Cross-cultural differences in risk perceptions of disasters. Risk Anal. 2010, 30, 1539–1549. [Google Scholar] [CrossRef]
- Weinstein, N.D.; Lyon, J.E. Mindset, optimistic bias about personal risk and health-protective behaviour. Br. J. Health Psychol. 1999, 4, 289–300. [Google Scholar] [CrossRef]
- Herrington, J.E.; Campbell, G.L.; Bailey, R.E.; Cortter, M.L.; Adams, M.; Frazier, E.L.; Damrow, T.A.; Gensheimer, K.F. Predisposing factors for individuals’ Lyme disease prevention practices: Connecticut, Maine, and Montana. Am. J. Public Health 1997, 87, 2035–2038. [Google Scholar] [CrossRef]
- Mawby, T.V.; Lovett, A.A. The public health risks of Lyme disease in Breckland, UK.: An investigation of environmental and social factors. Soc. Sci. Med. 1998, 46, 719–727. [Google Scholar] [CrossRef]
- Jones, T.F.; Garman, R.L.; LaFleur, B.; Stephan, S.J.; Schaffner, W. Risk factors for tick exposure and suboptimal adherence to preventive recommendations. Am. J. Prev. Med. 2002, 23, 47–50. [Google Scholar] [CrossRef]
- Omodior, O.; Anderson, K.R.; Clark, W.; Eze, P.; Donohoe, H. Preventing tick-bites among children in Indiana, USA: An analysis of factors associated with parental protective behaviors. Ticks Tick-Borne Dis. 2021, 12, 101647. [Google Scholar] [CrossRef]
- Sgroi, G.; Iatta, R.; Lia, R.P.; Napoli, E.; Buono, F.; Bezerra-Santos, M.A.; Veneziano, V.; Otranto, D. Tick exposure and risk of tick-borne pathogens infection in hunters and hunting dogs: A citizen science approach. Transbound. Emerg. Dis. 2021, 1–8. [Google Scholar] [CrossRef]
- Daltroy, L.H.; Phillips, C.; Lew, R.; Wright, E.; Shadick, N.A.; Liang, M.H. A controlled trial of a novel primary prevention program for Lyme disease and other tick-borne illnesses. Health Educ. Behav. 2007, 34, 531–542. [Google Scholar] [CrossRef]
- Weidinger, P.; Kolodziejek, J.; Bakonyi, T.; Brunthaler, R.; Erdélyi, K.; Weissenböck, H.; Nowotny, N. Different dynamics of Usutu virus infections in Austria and Hungary, 2017–2018. Transbound. Emerg. Dis. 2020, 67, 298–307. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Group | Participants (No.) | Mean Age of Participants (Years (CI)/Minimum–Maximum) | Sex (Male/Female/Other) | Having Children under 18 Years | Having Dogs | Tick Bite during the Lifetime | TBDs | TBDs—Family Members |
|---|---|---|---|---|---|---|---|---|
| PTEPs | 199 | 42.9 (30.3–55.5)/20–74 | 101/97/1 | 72 | 97 | 146 | 8 | 14 |
| HCWs | 147 | 43.2 (30.6–55.7)/19–75 | 59/88/0 | 66 | 79 | 82 | 6 | 12 |
| GP | 296 | 39.7 (28.4–50.9)/18–76 | 80/215/1 | 129 | 108 | 165 | 3 | 24 |
| Total | 642 | 41.9/18–76 | 240/400/2 | 267 | 284 | 393 | 17 | 50 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vasić, A.; Bjekić, J.; Veinović, G.; Mihaljica, D.; Sukara, R.; Poluga, J.; Filipović, S.R.; Tomanović, S. Knowledge, Attitudes, and Practices on Tick-Borne Encephalitis Virus and Tick-Borne Diseases within Professionally Tick-Exposed Persons, Health Care Workers, and General Population in Serbia: A Questionnaire-Based Study. Int. J. Environ. Res. Public Health 2022, 19, 867. https://doi.org/10.3390/ijerph19020867
Vasić A, Bjekić J, Veinović G, Mihaljica D, Sukara R, Poluga J, Filipović SR, Tomanović S. Knowledge, Attitudes, and Practices on Tick-Borne Encephalitis Virus and Tick-Borne Diseases within Professionally Tick-Exposed Persons, Health Care Workers, and General Population in Serbia: A Questionnaire-Based Study. International Journal of Environmental Research and Public Health. 2022; 19(2):867. https://doi.org/10.3390/ijerph19020867
Chicago/Turabian StyleVasić, Ana, Jovana Bjekić, Gorana Veinović, Darko Mihaljica, Ratko Sukara, Jasmina Poluga, Saša R. Filipović, and Snežana Tomanović. 2022. "Knowledge, Attitudes, and Practices on Tick-Borne Encephalitis Virus and Tick-Borne Diseases within Professionally Tick-Exposed Persons, Health Care Workers, and General Population in Serbia: A Questionnaire-Based Study" International Journal of Environmental Research and Public Health 19, no. 2: 867. https://doi.org/10.3390/ijerph19020867
APA StyleVasić, A., Bjekić, J., Veinović, G., Mihaljica, D., Sukara, R., Poluga, J., Filipović, S. R., & Tomanović, S. (2022). Knowledge, Attitudes, and Practices on Tick-Borne Encephalitis Virus and Tick-Borne Diseases within Professionally Tick-Exposed Persons, Health Care Workers, and General Population in Serbia: A Questionnaire-Based Study. International Journal of Environmental Research and Public Health, 19(2), 867. https://doi.org/10.3390/ijerph19020867