
A Descriptive Cohort of Suicidal Cancer Patients: Analysis of the Autopsy Case Series from 1993 to 2019 in Milan (Italy)



Abstract
1. Introduction
2. Materials and Methods
3. Results
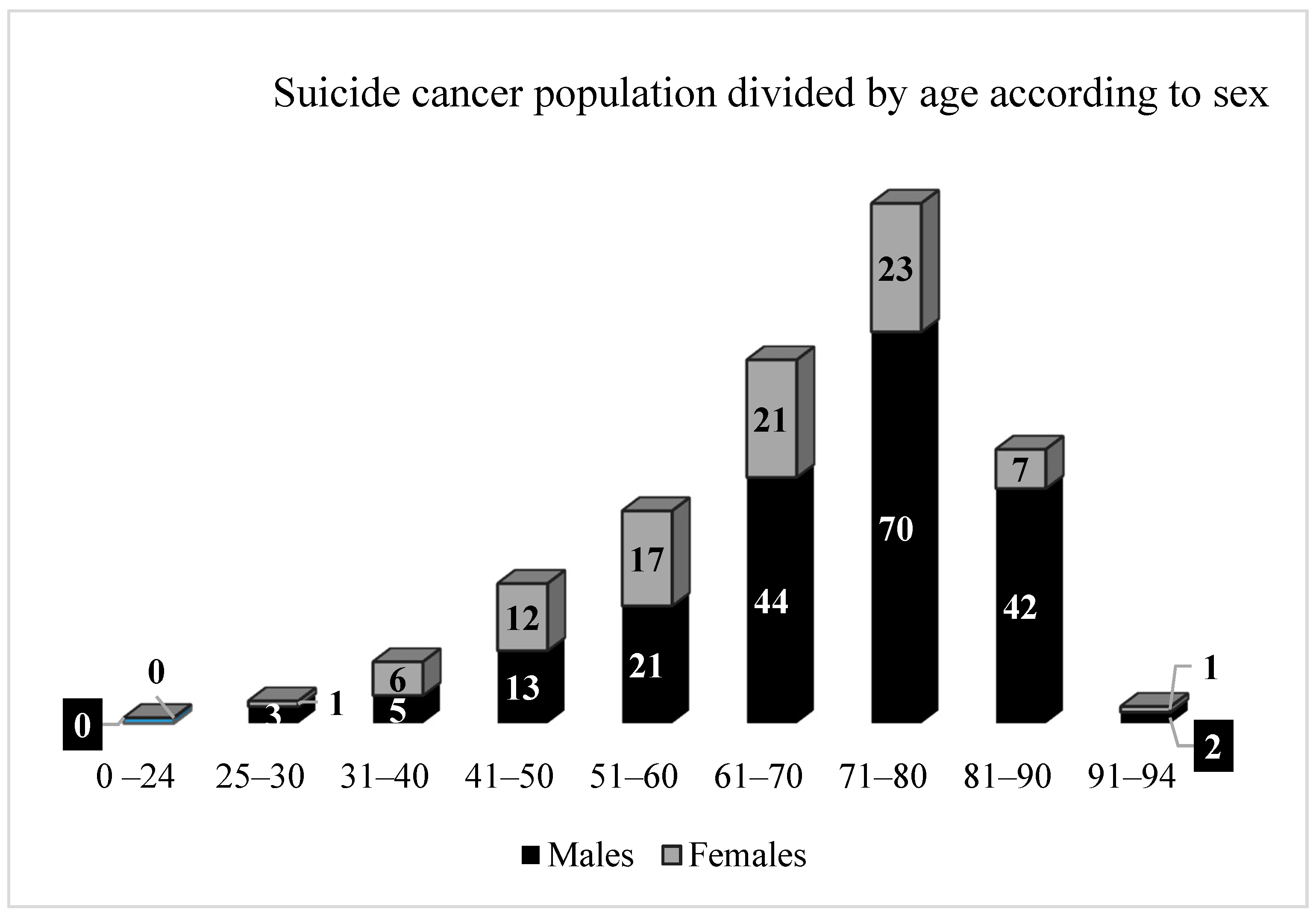
3.1. Socio-Demographic Features
3.2. Cancer-Related Features
3.3. Clinical Features
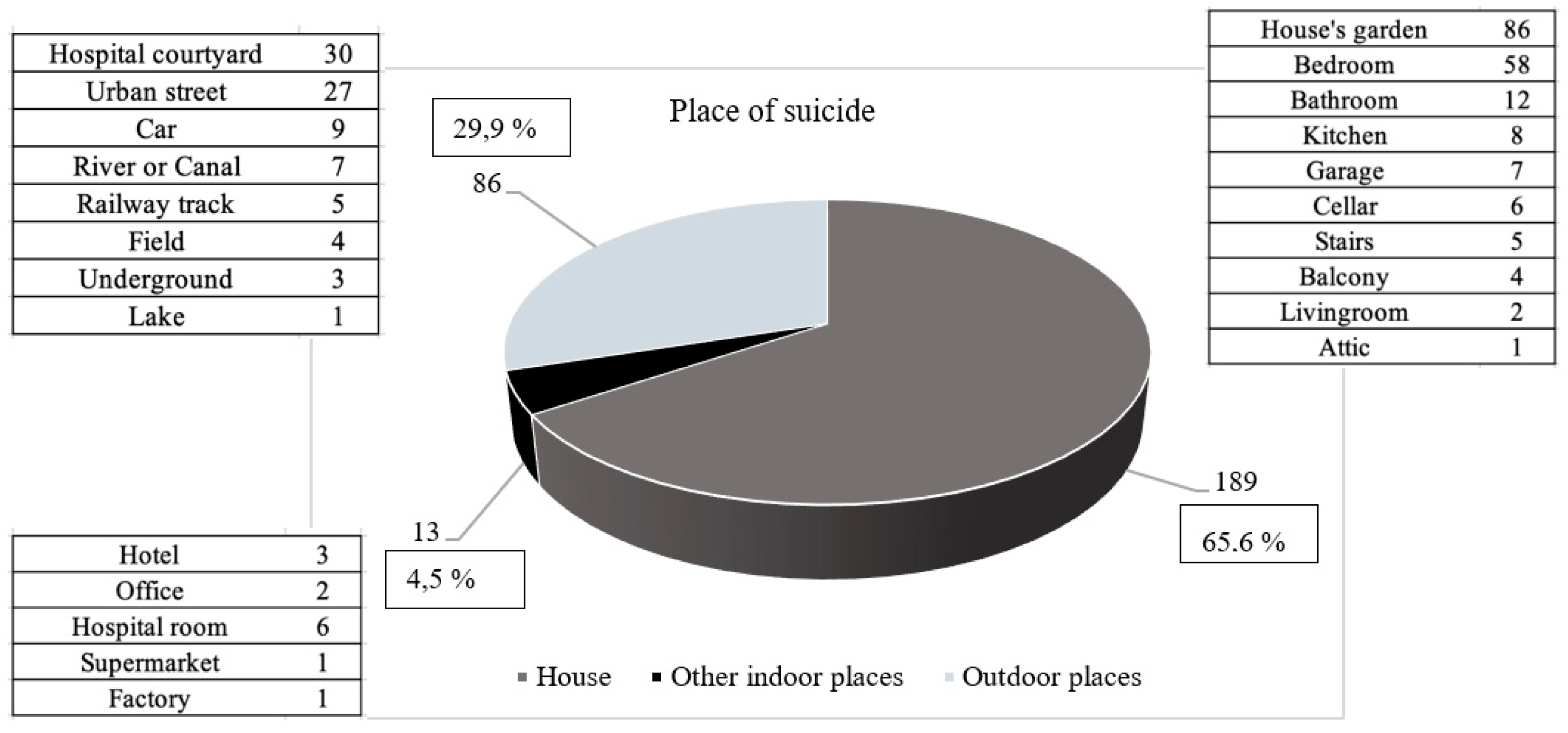
3.4. Suicide-Related Features
4. Discussion
5. Conclusions
Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Suicide Data. Available online: https://www.who.int/teams/mental-health-and-substance-use/suicide-data (accessed on 8 November 2021).
- World Health Organization. Cancer. Available online: https://www.who.int/news-room/fact-sheets/detail/cancer (accessed on 8 November 2021).
- Dwyer, J.; Hiscock, R.; O’Callaghan, C.; Taylor, K.; Ross, M.; Bugeja, L.; Philip, J. Characteristics of patients with cancer who die by suicide: Coronial case series in an Australian state. Psychooncology 2019, 28, 2195–2200. [Google Scholar] [CrossRef] [PubMed]
- Schneider, K.L.; Shenassa, E. Correlates of suicide ideation in a population-based sample of cancer patients. J. Psychosoc. Oncol. 2008, 26, 49–62. [Google Scholar] [CrossRef] [PubMed]
- Du, L.; Shi, H.Y.; Yu, H.R.; Liu, X.M.; Jin, X.H.; Qian, Y.; Fu, X.L.; Song, Y.P.; Cai, J.Y.; Chen, H.L. Incidence of suicide death in patients with cancer: A systematic review and meta-analysis. J. Affect. Disord. 2020, 276, 711–719. [Google Scholar] [CrossRef] [PubMed]
- Ravaioli, A.; Crocetti, E.; Mancini, S.; Baldacchini, F.; Giuliani, O.; Vattiato, R.; Bucchi, L.; Falcini, F. Suicide death among cancer patients: New data from northern Italy, systematic review of the last 22 years and meta-analysis. Eur. J. Cancer 2020, 125, 104–113. [Google Scholar] [CrossRef]
- Amiri, S.; Behnezhad, S. Cancer Diagnosis and Suicide Mortality: A Systematic Review and Meta-Analysis. Arch. Suicide Res. 2020, 24, S94–S112. [Google Scholar] [CrossRef]
- Semple, C.J.; Sullivan, K.; Dunwoody, L.; Kernohan, W.G. Psychosocial interventions for patients with head and neck cancer: Past, present, and future. Cancer Nurs. 2004, 27, 434–441. [Google Scholar] [CrossRef]
- Anderson, C.; Park, E.M.; Rosenstein, D.L.; Nichols, H.B. Suicide rates among patients with cancers of the digestive system. Psychooncology 2018, 27, 2274–2280. [Google Scholar] [CrossRef] [PubMed]
- Rahouma, M.; Kamel, M.; Abouarab, A.; Eldessouki, I.; Nasar, A.; Harrison, S.; Lee, B.; Shostak, E.; Morris, J.; Stiles, B.; et al. Lung cancer patients have the highest malignancy-associated suicide rate in USA: A population-based analysis. Ecancermedicalscience 2018, 12, 859. [Google Scholar] [CrossRef]
- Guo, Z.; Gan, S.; Li, Y.; Gu, C.; Xiang, S.; Zhou, J.; Gong, L.; Chan, F.L.; Wang, S. Incidence and risk factors of suicide after a prostate cancer diagnosis: A meta-analysis of observational studies. Prostate Cancer Prostatic Dis. 2018, 21, 499–508. [Google Scholar] [CrossRef]
- Fox, B.H.; Stanek III, E.J.; Boyd, S.C.; Flannery, J.T. Suicide rates among cancer patients in Connecticut. J. Chronic Dis. 1982, 35, 89–100. [Google Scholar] [CrossRef]
- Anguiano, L.; Mayer, D.K.; Piven, M.L.; Rosenstein, D. A literature review of suicide in cancer patients. Cancer Nurs. 2012, 35, E14–E26. [Google Scholar] [CrossRef] [PubMed]
- Fegg, M.; Kraus, S.; Graw, M.; Bausewein, C. Physical compared to mental diseases as reasons for committing suicide: A retrospective study. BMC Palliat. Care. 2016, 15, 14. [Google Scholar] [CrossRef]
- Lin, P.H.; Liao, S.C.; Chen, I.M.; Kuo, P.H.; Shan, J.C.; Lee, M.B.; Chen, W.L. Impact of universal health coverage on suicide risk in newly diagnosed cancer patients: Population-based cohort study from 1985 to 2007 in Taiwan. Psychooncology 2017, 26, 1852–1859. [Google Scholar] [CrossRef]
- Vyssoki, B.; Gleiss, A.; Rockett, I.R.; Hackl, M.; Leitner, B.; Sonneck, G.; Kapusta, N.D. Suicide among 915,303 Austrian cancer patients: Who is at risk? J. Affect. Disord. 2015, 175, 287–291. [Google Scholar] [CrossRef]
- Allebeck, P.; Bolund, C.; Ringbäck, G. Increased suicide rate in cancer patients. A cohort study based on the Swedish Cancer-Environment Register. J. Clin. Epidemiol. 1989, 42, 611–616. [Google Scholar] [CrossRef]
- Fang, F.; Fall, K.; Mittleman, M.A.; Sparén, P.; Ye, W.; Adami, H.O.; Valdimarsdóttir, U. Suicide and cardiovascular death after a cancer diagnosis. N. J. Med. 2012, 366, 1310–1318. [Google Scholar] [CrossRef]
- Crocetti, E.; Arniani, S.; Acciai, S.; Barchielli, A.; Buiatti, E. High suicide mortality soon after diagnosis among cancer patients in central Italy. Br. J. Cancer 1998, 77, 1194–1196. [Google Scholar] [CrossRef]
- Nasseri, K.; Mills, P.K.; Mirshahidi, H.R.; Moulton, L.H. Suicide in cancer patients in California, 1997–2006. Arch. Suicide Res. 2012, 16, 324–333. [Google Scholar] [CrossRef]
- Ward, K.K.; Roncancio, A.M.; Plaxe, S.C. Women with gynecologic malignancies have a greater incidence of suicide than women with other cancer types. Suicide Life Threat. Behav. 2013, 43, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Misono, S.; Weiss, N.S.; Fann, J.R.; Redman, M.; Yueh, B. Incidence of suicide in persons with cancer. J. Clin. Oncol. 2008, 26, 4731–4738. [Google Scholar] [CrossRef] [PubMed]
- Harris, E.C.; Barraclough, B. Suicide as an outcome for mental disorders. A meta-analysis. Br. J. Psychiatry 1997, 170, 205–228. [Google Scholar] [CrossRef]
- Ullman, K. Cancer survivorship gains importance. J. Natl. Cancer Inst. 2014, 106, djt450. [Google Scholar] [CrossRef][Green Version]
- Bellini, M.; Capannini, D. Increased suicide risk in cancer patients. Minerva Psichiatr. 1994, 35, 175–186. [Google Scholar]
- Allemani, C.; Weir, H.K.; Carreira, H.; Harewood, R.; Spika, D.; Wang, X.S.; Bannon, F.; Ahn, J.V.; Johnson, C.J.; Bonaventure, A.; et al. Global surveillance of cancer survival 1995-2009: Analysis of individual data for 25,676,887 patients from 279 population-based registries in 67 countries (CONCORD-2). Lancet 2015, 385, 977–1010. [Google Scholar] [CrossRef]
- Breitbart, W.; Rosenfeld, B.; Pessin, H.; Kaim, M.; Funesti-Esch, J.; Galietta, M.; Nelson, C.J.; Brescia, R. Depression, hopelessness, and desire for hastened death in terminally ill patients with cancer. JAMA 2000, 284, 2907–2911. [Google Scholar] [CrossRef]
- Louhivuori, K.A.; Hakama, M. Risk of suicide among cancer patients. Am. J. Epidemiol. 1979, 109, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Diaz-Frutos, D.; Baca-Garcia, E.; Mahillo-Fernandez, I.; Garcia-Foncillas, J.; Lopez-Castroman, J. Suicide ideation among oncologic patients in a Spanish ward. Psychol. Health Med. 2016, 21, 261–271. [Google Scholar] [CrossRef] [PubMed]
- Sperner-Unterweger, B. Depression in cancer patients. Wien Med. Wochenschr. 2015, 165, 297–303. [Google Scholar] [CrossRef]
- Brunckhorst, O.; Hashemi, S.; Martin, A.; George, G.; Van Hemelrijck, M.; Dasgupta, P.; Stewart, R.; Ahmed, K. Depression, anxiety, and suicidality in patients with prostate cancer: A systematic review and meta-analysis of observational studies. Prostate Cancer Prostatic Dis. 2021, 24, 281–289. [Google Scholar] [CrossRef]
- De la Grandmaison, G.L.; Watier, L.; Cavard, S.; Charlier, P. Are suicide rates higher in the cancer population? An investigation using forensic autopsy data. Med. Hypotheses 2014, 82, 16–19. [Google Scholar] [CrossRef]
- Juurlink, D.N.; Herrmann, N.; Szalai, J.P.; Kopp, A.; Redelmeier, D.A. Medical illness and the risk of suicide in the elderly. Arch. Intern. Med. 2004, 164, 1179–1184. [Google Scholar] [CrossRef] [PubMed]
- Llorente, M.D.; Burke, M.; Gregory, G.R.; Bosworth, H.B.; Grambow, S.C.; Horner, R.D.; Golden, A.; Olsen, E.J. Prostate cancer: A significant risk factor for late-life suicide. Am. J. Geriatr. Psychiatry 2005, 13, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Conwell, Y.; Duberstein, P.R.; Hirsch, J.K.; Conner, K.R.; Eberly, S.; Caine, E.D. Health status and suicide in the second half of life. Int. J. Geriatr. Psychiatry 2010, 25, 371–379. [Google Scholar] [CrossRef] [PubMed]
- Fall, K.; Fang, F.; Mucci, L.A.; Ye, W.; Andrén, O.; Johansson, J.E.; Andersson, S.O.; Sparén, P.; Klein, G.; Stampfer, M.; et al. Immediate risk for cardiovascular events and suicide following a prostate cancer diagnosis: Prospective cohort study. PLoS Med. 2009, 6, e1000197. [Google Scholar] [CrossRef] [PubMed]
- Träskman, L.; Asberg, M.; Bertilsson, L.; Sjöstrand, L. Monoamine metabolites in CSF and suicidal behavior. Arch. Gen. Psychiatry 1981, 38, 631–636. [Google Scholar] [CrossRef]
- Ludwig, B.; Dwivedi, Y. The concept of violent suicide, its underlying trait and neurobiology: A critical perspective. Eur. Neuropsychopharmacol. 2018, 28, 243–251. [Google Scholar] [CrossRef] [PubMed]
- Gentile, G.; Galante, N.; Tambuzzi, S.; Zoja, R. A forensic analysis on 53 cases of complex suicides and one complicated assessed at the Bureau of Legal Medicine of Milan (Italy). Forensic Sci. Int. 2021, 319, 110662. [Google Scholar] [CrossRef]
- Altun, G. Planned complex suicide: Report of three cases. Forensic Sci. Int. 2006, 157, 83–86. [Google Scholar] [CrossRef]
- Racette, S.; Sauvageau, A. Planned and unplanned complex suicides: A 5-year retrospective study. J. Forensic Sci. 2007, 52, 449–452. [Google Scholar] [CrossRef]
- Gentile, G.; Bianchi, M.; Boracchi, M.; Goj, C.; Tambuzzi, S.; Zoja, R. Forensic pathological considerations of a unique case of “complicated suicide”. J. Forensic Sci. 2020, 65, 2184–2187. [Google Scholar] [CrossRef]
- Töro, K.; Pollak, S. Complex suicide versus complicated suicide. Forensic Sci. Int. 2009, 184, 6–9. [Google Scholar] [CrossRef]
- Saukko, P.; Knight, B. Burns and scalds. In Knight’s Forensic Pathology; Saukko, P., Knight, B., Eds.; Hodder Arnold: London, UK, 2004; pp. 312–323. [Google Scholar]
- Calati, R.; Filipponi, C.; Mansi, W.; Casu, D.; Peviani, G.; Gentile, G.; Tambuzzi, S.; Zoja, R.; Fornaro, M.; Lopez-Castroman, J.; et al. Cancer diagnosis and suicide outcomes: Umbrella review and methodological considerations. J. Affect. Disord. 2021, 295, 1201–1214. [Google Scholar] [CrossRef]
- Upadhyaya, S.A.; Ghazwani, Y.; Wu, S.; Broniscer, A.; Boop, F.A.; Gajjar, A.; Qaddoumi, I. Mortality in children with low-grade glioma or glioneuronal tumors: A single-institution study. Pediatr. Blood Cancer. 2018, 65, e26717. [Google Scholar] [CrossRef]
- Sauvageau, A.; Racette, S. Child and adolescent victims in forensic autopsy: A 5-year retrospective study. J. Forensic Sci. 2008, 53, 699–702. [Google Scholar] [CrossRef]
- Zaorsky, N.G.; Zhang, Y.; Tuanquin, L.; Bluethmann, S.M.; Park, H.S.; Chinchilli, V.M. Suicide among cancer patients. Nat. Commun. 2019, 10, 207. [Google Scholar] [CrossRef] [PubMed]
- Akechi, T.; Kugaya, A.; Okamura, H.; Nakano, T.; Okuyama, T.; Mikami, I.; Shima, Y.; Yamawaki, S.; Uchitomi, Y. Suicidal thoughts in cancer patients: Clinical experience in psycho-oncology. Psychiatry Clin. Neurosci. 1999, 53, 569–573. [Google Scholar] [CrossRef] [PubMed]
- AIOM. I Numeri del Cancro in Italia 2021; Intermedia Editore: Brescia, Italy, 2021; pp. 1–177. [Google Scholar]
- Akechi, T. Suicide prevention among patients with cancer. Gen. Hosp. Psychiatry 2020, 64, 119–120. [Google Scholar] [CrossRef]
- Henriksson, M.M.; Isometsä, E.T.; Hietanen, P.S.; Aro, H.M.; Lönnqvist, J.K. Mental disorders in cancer suicides. J. Affect. Disord. 1995, 36, 11–20. [Google Scholar] [CrossRef]
- Akechi, T.; Okamura, H.; Yamawaki, S.; Uchitomi, Y. Why do some cancer patients with depression desire an early death and others do not? Psychosomatics 2001, 42, 141–145. [Google Scholar] [CrossRef] [PubMed]
- Filiberti, A.; Ripamonti, C.; Totis, A.; Ventafridda, V.; De Conno, F.; Contiero, P.; Tamburini, M. Characteristics of terminal cancer patients who committed suicide during a home palliative care program. J. Pain Symptom Manag. 2001, 22, 544–553. [Google Scholar] [CrossRef]
- Smith, M.T.; Edwards, R.R.; Robinson, R.C.; Dworkin, R.H. Suicidal ideation, plans, and attempts in chronic pain patients: Factors associated with increased risk. Pain 2004, 111, 201–208. [Google Scholar] [CrossRef] [PubMed]
- Walker, J.; Waters, R.A.; Murray, G.; Swanson, H.; Hibberd, C.J.; Rush, R.W.; Storey, D.L.; Strong, V.A.; Fallon, M.T.; Wall, L.R.; et al. Better off dead: Suicidal thoughts in cancer patients. J. Clin. Oncol. 2008, 26, 4725–4730. [Google Scholar] [CrossRef]
- Sinyor, M.; Howlett, A.; Cheung, A.H.; Schaffer, A. Substances used in completed suicide by overdose in Toronto: An observational study of coroner’s data. Can. J. Psychiatry 2012, 57, 184–191. [Google Scholar] [CrossRef] [PubMed]
- Fornasari, D.; Gerra, G.; Maione, S.; Mannaioni, G.; Mugelli, A.; Parolaro, D.; Romualdi, P.; Sacerdote, P. Trattamento del dolore cronico in Italia: Appropriatezza terapeutica con oppiacei e timore di addiction: Situazione italiana vs USA. Quotidianosanità 2019, I, 1–20. [Google Scholar]



{kind=link}
{kind=link}
| Body Area | Site | Total (%) | Sex | |
|---|---|---|---|---|
| M (%) | F (%) | |||
| Head 14 (4.9%) | Brain | 9 (64.3) | 5 (55.5) | 4 (44.5) |
| Ear | 1 (7.1) | 1 (100) | ||
| Tongue | 4 (28.6) | 3 (75) | 1 (25) | |
| Neck 23 (8%) | Pharynx | 2 (8.8) | 2 (100) | |
| Thyroid | 6 (26) | 2 (33.3) | 4 (66.7) | |
| Larynx | 15 (65.2) | 14 (93.3) | 1 (6.7) | |
| Chest 73 (25.3%) | Esophagus | 4 (5.5) | 4 (100) | |
| Breast | 29 (39.7) | 29 (100) | ||
| Lung | 40 (54.8) | 36 (90) | 4 (10) | |
| Abdomen 78 (27.1%) | Liver | 11 (14.1) | 7 (63.6) | 4 (36.4) |
| Biliary tract | 4 (5.1) | 4 (100) | ||
| Pancreas | 13 (16.7) | 10 (77) | 3 (33) | |
| Stomach | 12 (15.3) | 11 (91.6) | 1 (8.4) | |
| Duodenum | 1 (1.4) | 1 (100) | ||
| Colon | 26 (33.3) | 16 (61.5) | 10 (38.4) | |
| Rectum | 9 (11.6) | 6 (66.6) | 3 (33.4) | |
| Peritoneum | 2 (2.5) | 2 (100) | ||
| Reproductive system 56 (19.4%) | Testicle | 5 (8.9) | 5 (100) | |
| Prostate | 36 (64.3) | 36 (100) | ||
| Ovary | 3 (5.3) | 3 (100) | ||
| Uterus | 12 (21.5) | 12 (100) | ||
| Urinary system 22 (7.7%) | Kidney | 10 (45.5) | 7 (70) | 3 (30) |
| Bladder | 12 (54.5) | 11 (91.6) | 1 (8.4) | |
| Immune system 16 (5.5%) | Lymphocytes | 16 (100) | 12 (75) | 4 (25) |
| Integumentary system 5 (1.7%) | Skin | 5 (100) | 5 (100) | |
| Skeletal system 1 (0.3%) | Bone | 1 (100) | 1 (100) | |
| Type of Pathology | Disease 1 | Disease 2 | N of Cases | % | |
|---|---|---|---|---|---|
| Single disease—139 | Psychiatric 111 (79.8%) | Depression | 109 | 98.1 | |
| Psychosis | 2 | 1.9 | |||
| Organic 28 (20.2%) | Hypertension | 9 | 32.1 | ||
| Myocardial infarction | 8 | 28.5 | |||
| Coronary artery disease | 2 | 7.2 | |||
| Diabetes | 7 | 25 | |||
| Hepatitis c virus (HCV) | 2 | 7.2 | |||
| Multiple diseases—46 | Psychiatric 37 (80.4%) | Depression 37 (100%) | Alcoholism | 8 | 21.7 |
| HCV | 4 | 10.8 | |||
| Myocardial infarction | 4 | 10.8 | |||
| Hypertension | 4 | 10.8 | |||
| Diabetes | 3 | 8.1 | |||
| Arrhythmia | 3 | 8.1 | |||
| Bronchial asthma | 2 | 5.4 | |||
| Kidney failure | 2 | 5.4 | |||
| Maculopathy | 2 | 5.4 | |||
| Epilepsy | 1 | 2.7 | |||
| Cerebral stroke | 1 | 2.7 | |||
| Parkinson disease | 1 | 2.7 | |||
| Pulmonary emphysema | 1 | 2.7 | |||
| Sarcoidosis | 1 | 2.7 | |||
| Organic 9 (19.6) | COPD (chronic obstructive pulmonary disease) 4 (44.4%) | Hypertension | 2 | 50 | |
| HCV | 1 | 25 | |||
| Heart failure | 1 | 25 | |||
| Hypertension 5 (55.6) | Aortic aneurysm | 1 | 20 | ||
| Diabetes | 1 | 20 | |||
| Epilepsy | 1 | 20 | |||
| Glaucoma | 1 | 20 | |||
| Neuropathy | 1 | 20 | |||
| (A) | |||
| Medication | N of Cases (%) | ||
| Single-drug therapy—133–66% | Chemotherapy | 44 (33) | |
| Antidepressants | 38 (28.7) | ||
| Anxiolytics | 12 (9) | ||
| Antihypertensive | 5 (3.8) | ||
| Analgesic | 8 (6) | ||
| Antiepileptic | 2 (1.5) | ||
| Oxygen therapy | 1 (0.7) | ||
| Antipsychotics | 4 (3) | ||
| Proton-pump inhibitor | 2 (1.5) | ||
| Antithyroid | 3 (2.3) | ||
| Antiparkinsonian | 1 (0.7) | ||
| Antiplatelets agents | 3 (2.3) | ||
| Oral hypoglycemic agents | 3 (2.3) | ||
| Anti-inflammatory | 4 (3) | ||
| Diuretics | 2 (1.5) | ||
| Blood products | 1 (0.7) | ||
| (B) | |||
| Medication | N of Cases (%) | ||
| Multi-drug therapy—68–34% | Antidepressants 29 (42.7%) | Chemotherapy | 6 (20.6) |
| Anxiolytics | 13 (44.8) | ||
| Antihypertensive | 4 (13.8) | ||
| Morphine | 3 (10.3) | ||
| Immunosuppressants | 1 (3.5) | ||
| Antiarrhythmic | 1 (3.5) | ||
| Antiepileptic | 1 (3.5) | ||
| Chemotherapy 18 (26.5%) | Morphine | 5 (27.7) | |
| Antihypertensive | 4 (22.2) | ||
| Insulin | 2 (11.2) | ||
| Cortisone | 2 (11.2) | ||
| Diuretics | 1 (5.5) | ||
| Antiemetics | 2 (11.2) | ||
| Interferon | 1 (5.5) | ||
| Oral hypoglycemic agents | 1 (5.5) | ||
| Analgesic 8 (11.8%) | Antiplatelets agents | 3 (37.5) | |
| Cortisone | 2 (25) | ||
| Diuretics | 2 (25) | ||
| Proton-pump inhibitor | 1 (12.5) | ||
| Diuretics 6 (8.8%) | Cardiotonic | 2 (33.6) | |
| Oral hypoglycemic agents | 1 (16.6) | ||
| Antiepileptic | 1 (16.6) | ||
| Anxiolytics | 1 (16.6) | ||
| Antiplatelets agents | 1 (16.6) | ||
| Anxiolytics 5 (7.3%) | Cortisone | 1 (20) | |
| Sedative-hypnotic | 4 (80) | ||
| Antihypertensive 2 (2.9%) | Antiplatelets agents | 1 (50) | |
| Cortisone | 1 (50) | ||
| Detrimental Modalities and Applied Means According to Victims’ Sex and Cause of Death in Simple (Nor Complex, Complicated) Suicides | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Detrimental Modality | Applied Mean | Total | % | Sex | Cause of Death | Total | % | ||||
| M | % | F | % | ||||||||
| Violent suicides—246 cases 85.5% | Falling from a height (3–27 m) | 145 | 94.8 | 87 | 60 | 58 | 40 | Skeletal-visceral injuries | 138 | 95.1 | |
| Brain injuries | 7 | 4.9 | |||||||||
| Pedestrian running over | Train (5 cases—62.5%) | 8 | 5.2 | 7 | 87.5 | 1 | 12.5 | Body disruption | 6 | 75 | |
| Subway (3 cases—37.5%) | Brain disruption | 2 | 25 | ||||||||
| Gunshot | Gun (46 cases—88.5%) | 52 | 18 | 48 | 92.3 | 4 | 7.7 | Brain injuries | 46 | 88.4 | |
| Shotgun (6 cases—11.5%) | Cardio-pulmonary injuries | 5 | 9.6 | ||||||||
| Acute bleeding due to vascular lesions | 1 | 2 | |||||||||
| Hanging | Rope (17 cases—50%) | 34 | 12 | 30 | 88.2 | 4 | 11.8 | Hanging mechanical asphyxia | 34 | 100 | |
| Electric cable (6 cases—17.5%) | |||||||||||
| Roller shutter belt (1 case—3%) | |||||||||||
| Mountaineer rope (1 case—3%) | |||||||||||
| Clothing (7 cases—20.5%) | |||||||||||
| Scarf (1 case—3%) | |||||||||||
| Shoelaces (1 case—3%) | |||||||||||
| Sharp force trauma | Knife (5 cases—71.4%) | 7 | 2.5 | 4 | 57.1 | 3 | 42.9 | Acute bleeding due to vascular lesions | 4 | 57.1 | |
| Internal submersion | 1 | 14.3 | |||||||||
| Razor (1 case—14.3%) | Cardio-pericardial injuries | 1 | 14.3 | ||||||||
| Scalpel (1 case—14.3%) | Lung injuries | 1 | 14.3 | ||||||||
| Non-violent suicides—37 cases 14.5% | Chemical | Antidepressants (9 cases—39%) | 23 | 8 | 11 | 48.2 | 12 | 51.8 | Acute drug poisoning | 14 | 60.8 |
| Anxiolytics (3 cases—13%) | |||||||||||
| Insulin (2 cases—8.8%) | |||||||||||
| Acid caustic substances (2 cases—8.8%) | Esophagus-gastric perforation | 3 | 13.2 | ||||||||
| Acid caustic substances (1 case—4.4%) | |||||||||||
| Carbon monoxide (CO) (6 cases—26%) | Acute carbon monoxide intoxication | 6 | 26 | ||||||||
| Drowning | River (7 cases—87.5%) | 8 | 3 | 4 | 50 | 4 | 50 | Asphyxia by drowning | 8 | 100 | |
| Lake (1 case—12.5%) | |||||||||||
| Plastic bag suffocation | Plastic bag (6 cases—100%) | 6 | 2 | 4 | 66.6 | 2 | 33.4 | Plastic bag suffocation | 6 | 100 | |
| Violent Suicide | Non-Violent Suicide | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Body Area | Site | Falling from a Height | Pedestrian Run over | Gunshot | Hanging | Sharp Force Trauma | Chemical | Drowning | Plastic Bag Suffocation | Complex Suicide | Complicated Suicide | ||||||||||
| M | F | M | F | M | F | M | F | M | F | M | F | M | F | M | F | M | F | M | F | ||
| Head | Brain | 2 | 3 | 2 | 1 | 1 | |||||||||||||||
| Ear | 1 | ||||||||||||||||||||
| Tongue | 1 | 1 | 1 | 1 | |||||||||||||||||
| Neck | Pharynx | 2 | |||||||||||||||||||
| Thyroid | 1 | 3 | 1 | 1 | |||||||||||||||||
| Larynx | 6 | 1 | 4 | 2 | 2 | ||||||||||||||||
| Chest | Esophagus | 2 | 2 | ||||||||||||||||||
| Breast | 18 | 1 | 3 | 4 | 1 | 2 | |||||||||||||||
| Lung | 18 | 3 | 1 | 9 | 5 | 2 | 1 | 1 | |||||||||||||
| Abdomen | Liver | 6 | 2 | 1 | 1 | 1 | |||||||||||||||
| Biliary tract | 4 | ||||||||||||||||||||
| Pancreas | 6 | 1 | 2 | 2 | 2 | ||||||||||||||||
| Stomach | 7 | 1 | 1 | 2 | 1 | ||||||||||||||||
| Duodenum | 1 | ||||||||||||||||||||
| Colon | 7 | 9 | 1 | 5 | 1 | 2 | 1 | ||||||||||||||
| Rectum | 1 | 2 | 1 | 1 | 1 | 3 | |||||||||||||||
| Peritoneum | 2 | ||||||||||||||||||||
| Reproductive System | Testicle | 1 | 1 | 1 | 2 | ||||||||||||||||
| Prostate | 11 | 2 | 12 | 4 | 2 | 2 | 2 | 1 | |||||||||||||
| Ovary | 3 | ||||||||||||||||||||
| Uterus | 9 | 2 | 1 | ||||||||||||||||||
| Urinary System | Kidney | 3 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | ||||||||||||
| Bladder | 4 | 1 | 1 | 3 | 2 | 1 | |||||||||||||||
| Immune System | Lymphocytes | 4 | 1 | 1 | 5 | 1 | 1 | 2 | 1 | ||||||||||||
| Integumentary System | Skin | 2 | 1 | 2 | |||||||||||||||||
| Skeletal System | Bone | 1 | |||||||||||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gentile, G.; Tambuzzi, S.; Calati, R.; Zoja, R. A Descriptive Cohort of Suicidal Cancer Patients: Analysis of the Autopsy Case Series from 1993 to 2019 in Milan (Italy). Int. J. Environ. Res. Public Health 2022, 19, 829. https://doi.org/10.3390/ijerph19020829
Gentile G, Tambuzzi S, Calati R, Zoja R. A Descriptive Cohort of Suicidal Cancer Patients: Analysis of the Autopsy Case Series from 1993 to 2019 in Milan (Italy). International Journal of Environmental Research and Public Health. 2022; 19(2):829. https://doi.org/10.3390/ijerph19020829
Chicago/Turabian StyleGentile, Guendalina, Stefano Tambuzzi, Raffaella Calati, and Riccardo Zoja. 2022. "A Descriptive Cohort of Suicidal Cancer Patients: Analysis of the Autopsy Case Series from 1993 to 2019 in Milan (Italy)" International Journal of Environmental Research and Public Health 19, no. 2: 829. https://doi.org/10.3390/ijerph19020829
APA StyleGentile, G., Tambuzzi, S., Calati, R., & Zoja, R. (2022). A Descriptive Cohort of Suicidal Cancer Patients: Analysis of the Autopsy Case Series from 1993 to 2019 in Milan (Italy). International Journal of Environmental Research and Public Health, 19(2), 829. https://doi.org/10.3390/ijerph19020829