
Correlation of Dengue Warning Signs during Febrile Phase with Rotational Thromboelastometry, Cortisol and Feritin


 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
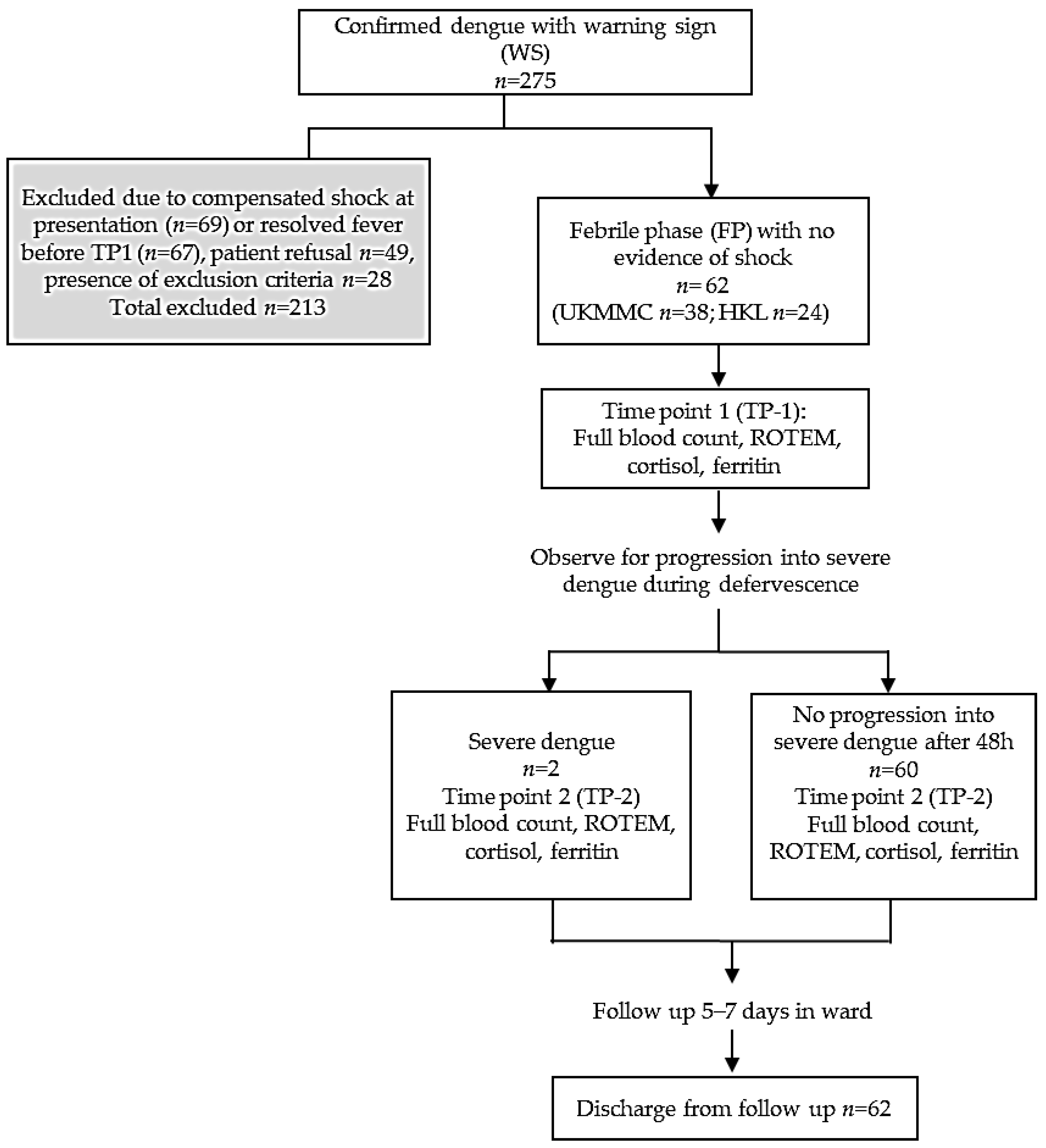
2.1. Recruitment
2.2. TP-1
2.3. TP-2
2.4. Hemostatic Parameters
2.5. Biochemical Markers
2.6. Clinical Assessments
2.7. Statistical Analysis
3. Results
3.1. Baseline Characteristics and Warning Signs at Febrile Phase (TP-1)
3.2. TP-1: Association of Warning Signs at Febrile Phase with ROTEM and Platelet Function
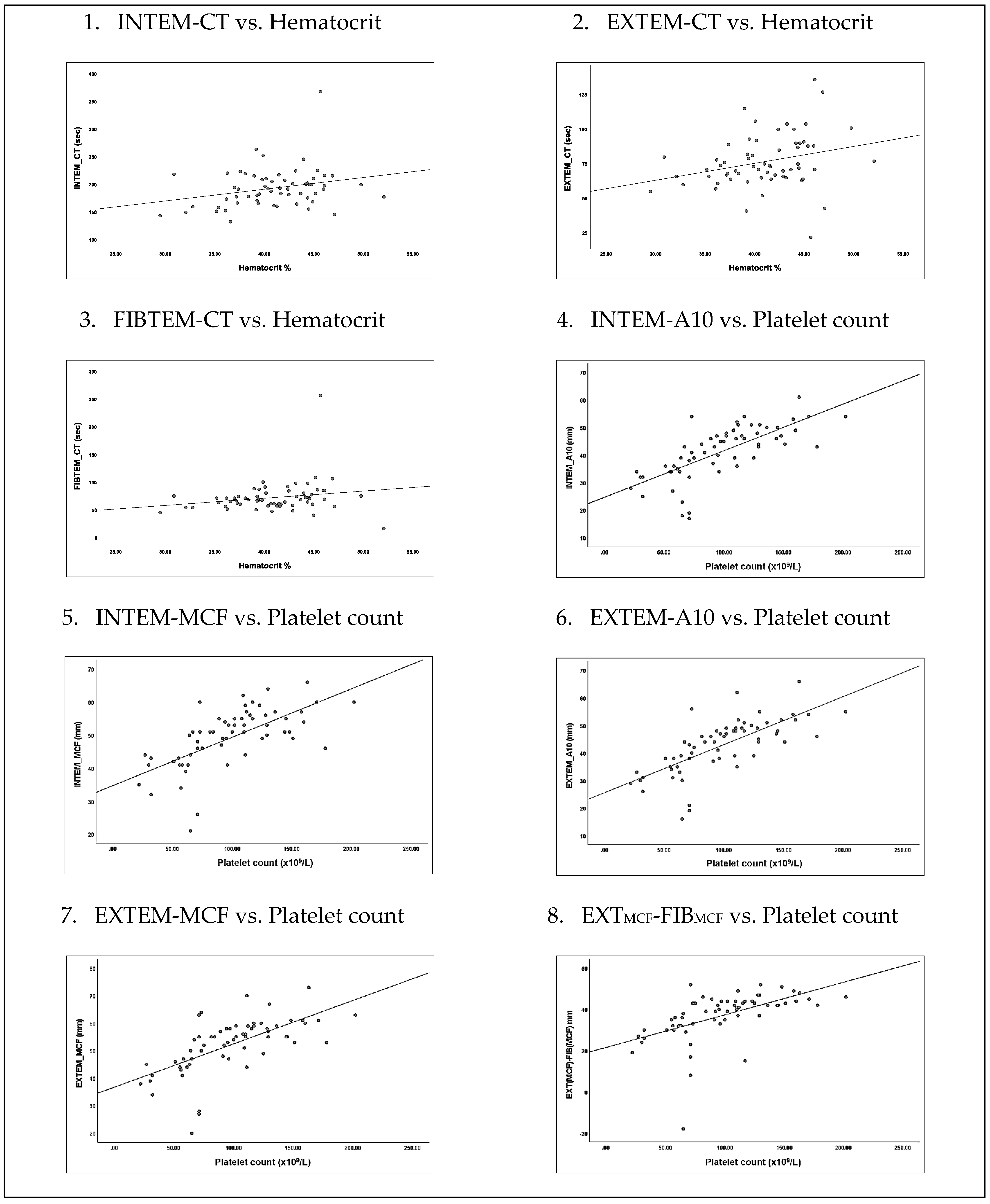
3.3. TP-1: Association of Warning Signs “Hematocrit Increase and Platelet Decrease” with ROTEM and Platelet Function
3.4. TP-1 to TP-2: Kinetics of Hemostatic and Biochemical Markers between Febrile Phase and Defervescence
3.5. TP-2: Association of Hemorrhage during Defervescence with ROTEM, Platelet Count & Conventional Coagulations
3.6. TP-2: Severity of Dengue
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Dengue and Severe Dengue. Available online: https://www.who.int/en/news-room/fact-sheets/detail/dengue-and-severe-dengue (accessed on 24 February 2019).
- Clinical Practice Guidelines (CPG); MOH. Management of Dengue Infection in Adults. Available online: http://www.acadmed.org.my/index.cfm?menuid=67 (accessed on 24 February 2018).
- Bahagian Kawalan Penyakit Kebangsaan; KKM. Crisis Preparedness and Response Center Malaysia (CPRC). Dengue Statistic. 2017. Available online: http://idengue.remotesensing.gov.my/idengue/index.php (accessed on 24 February 2019).
- Selvarajoo, S.; Liew, J.W.K.; Tan, W.; Lim, X.Y.; Refai, W.F.; Zaki, R.A.; Sethi, N.; Sulaiman, W.Y.W.; Lim, Y.A.L.; Vadivelu, J. Knowledge, attitude and practice on dengue prevention and dengue seroprevalence in a dengue hotspot in Malaysia: A cross-sectional study. Sci. Rep. 2020, 10, 9534. [Google Scholar] [CrossRef]
- World Health Organization. Dengue Haemorrhagic Fever: Diagnosis, Treatment, Prevention and Control; World Health Organization: Geneva, Switzerland, 1997. [Google Scholar]
- Hadinegoro, S.R.S. The revised WHO dengue case classification: Does the system need to be modified? Paediatr. Int. Child Health 2012, 32, 33–38. [Google Scholar] [CrossRef] [Green Version]
- Alexander, N.; Balmaseda, A.; Coelho, I.C.; Dimaano, E.; Hien, T.T.; Hung, N.T.; Jänisch, T.; Kroeger, A.; Lum, L.C.; Martinez, E. Multicentre prospective study on dengue classification in four South-east Asian and three Latin American countries. Trop. Med. Int. Health 2011, 16, 936–948. [Google Scholar] [CrossRef]
- World Health Organization. Dengue Guidelines for Diagnosis, Treatment, Prevention and Control; New Edition; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Winearls, J.; Reade, M.; Miles, H.; Bulmer, A.; Campbell, D.; Görlinger, K.; Fraser, J.F. Targeted coagulation management in severe trauma: The controversies and the evidence. Anesth. Analg. 2016, 123, 910–924. [Google Scholar] [CrossRef]
- de Toledo Piza, F.M.; Corrêa, T.D.; Marra, A.R.; Guerra, J.C.C.; dos Reis Rodrigues, R.; Villarinho, A.A.R.; de Aranda, V.F.; Shiramizo, S.C.P.L.; de Lima, M.R.d.J.; Kallas, E.G. Thromboelastometry analysis of thrombocytopenic dengue patients: A cross-sectional study. BMC Infect. Dis. 2017, 17, 89. [Google Scholar]
- Sureshkumar, V.; Vijayan, D.; Kunhu, S.; Mohamed, Z.; Thomas, S.; Raman, M. Thromboelastographic analysis of hemostatic abnormalities in dengue patients admitted in a multidisciplinary intensive care unit: A cross-sectional study. Indian J. Crit. Care Med. 2018, 22, 238. [Google Scholar]
- Myo-Khin, D.C.H.; Soe-Thein, M.M.; Thein-Thein-Myint, F.R.C.P.; Than-Nu-Swe, M.M.; Tin-Tin-Saw, M.M.; Muya-Than, B.S. Serum cortisol levels in children with dengue haemorrhagic fever. J. Trop. Pediatr. 1995, 41, 295–297. [Google Scholar] [CrossRef]
- Joob, B.; Wiwanitkit, V. Serum cortisol in dengue and dengue hemorrhagic fever: Is there any clinical implication? Asian Pac. J. Trop. Dis. 2014, 4, 313–314. [Google Scholar] [CrossRef]
- Soundravally, R.; Agieshkumar, B.; Daisy, M.; Sherin, J.; Cleetus, C.C. Ferritin levels predict severe dengue. Infection 2015, 43, 13–19. [Google Scholar] [CrossRef]
- Wan Jamaludin, W.F.; Periyasamy, P.; Mat, W.R.W.; Wahid, S.F.A. Dengue infection associated hemophagocytic syndrome: Therapeutic interventions and outcome. J. Clin. Virol. 2015, 69, 91–95. [Google Scholar] [CrossRef]
- National Cancer Institute. Common Terminology Criteria for Adverse Events (CTCAE); Version 4.0; National Cancer Institute Enterprise Vocabulary Services Website; National Cancer Institute: Bethesda, MD, USA, 2010. [Google Scholar]
- Wills, B.A.; Oragui, E.E.; Stephens, A.C.; Daramola, O.A.; Dung, N.M.; Loan, H.T.; Chau, N.V.; Chambers, M.; Stepniewska, K.; Farrar, J.J. Coagulation abnormalities in dengue hemorrhagic fever: Serial investigations in 167 Vietnamese children with dengue shock syndrome. Clin. Infect. Dis. 2002, 35, 277–285. [Google Scholar] [CrossRef]
- Mitrakul, C.; Poshyachinda, M.; Futrakul, P.; Sangkawibha, N.; Ahandrik, S. Hemostatic and platelet kinetic studies in dengue hemorrhagic fever. Am. J. Trop. Med. Hyg. 1977, 26, 975–984. [Google Scholar] [CrossRef]
- Isarangkura, P.; Pongpanich, B.; Pintadit, P.; Phanichyakarn, P.; Valyasevi, A. Hemostatic derangement in dengue haemorrhagic fever. Southeast Asian J. Trop. Med. Public Health 1987, 18, 331–339. [Google Scholar]
- Funahara, Y.; Shirahata, A.; Setiabudy-Dharma, R. DHF characterized by acute type DIC with increased vascular permeability. Southeast Asian J. Trop. Med. Public Health 1987, 18, 346–350. [Google Scholar]
- Bain, B.J.; Bates, I.; Laffan, M.A.; Lewis, S.M. Dacie and Lewis Practical Haematology: Expert Consult; Online and Print; Elsevier Health Sciences: Amsterdam, The Netherlands, 2016. [Google Scholar]
- Lang, T.; Bauters, A.; Braun, S.L.; Pötzsch, B.; von Pape, K.-W.; Kolde, H.-J.; Lakner, M. Multi-centre investigation on reference ranges for ROTEM thromboelastometry. Blood Coagul. Fibrinolysis 2005, 16, 301–310. [Google Scholar] [CrossRef]
- Srichaikul, T.; Nimmannitya, S.; Sripaisarn, T.; Kamolsilpa, M.; Pulgate, C. Platelet function during the acute phase of dengue hemorrhagic fever. Southeast Asian J. Trop. Med. Public Health 1989, 20, 19–25. [Google Scholar]
- Boonpucknavig, S.; Vuttiviroj, O.; Bunnag, C.; Bhamarapravati, N.; Nimmanitya, S. Demonstration of dengue antibody complexes on the surface of platelets from patients with dengue hemorrhagic fever. Am. J. Trop. Med. Hyg. 1979, 28, 881–884. [Google Scholar] [CrossRef]
- Mariappan, V.; Adikari, S.; Shanmugam, L.; Easow, J.M.; Balakrishna Pillai, A. Expression dynamics of vascular endothelial markers: Endoglin and syndecan-1 in predicting dengue disease outcome. Transl. Res. 2021, 232, 121–141. [Google Scholar] [CrossRef]
- Sellahewa, K.H. Pathogenesis of dengue haemorrhagic fever and its impact on case management. ISRN Infect. Dis. 2012, 2013, 571646. [Google Scholar] [CrossRef] [Green Version]
- Hilgard, P.; Stockert, R. Heparan sulfate proteoglycans initiate dengue virus infection of hepatocytes. Hepatology 2000, 32, 1069–1077. [Google Scholar] [CrossRef]
- Sosothikul, D.; Seksarn, P.; Pongsewalak, S.; Lusher, J. Activation of endothelial cells, coagulation and fibrinolysis in children with Dengue virus infection. Thromb. Haemost. 2007, 97, 627–634. [Google Scholar] [CrossRef] [PubMed]
- Min, M.; Aye, M.; Shwe, T.; Swe, T. Hydrocortisone in the management of dengue shock syndrome. Southeast Asian J. Trop. Med. Public Health 1975, 6, 573–579. [Google Scholar] [PubMed]
- Pongpanich, B.; Bhanchet, P.; Phanichyakarn, P.; Valyasevi, A. Studies on dengue hemorrhagic fever. Clinical study: An evaluation of steroids as a treatment. J. Med. Assoc. Thail. 1973, 56, 6–14. [Google Scholar]
- Sumarmo; Talogo, W.; Asrin, A.; Isnuhandojo, B.; Sahudi, A. Failure of hydrocortisone to affect outcome in dengue shock syndrome. Pediatrics 1982, 69, 45–49. [Google Scholar] [CrossRef]
- Panpanich, R.; Sornchai, P.; Kanjanaratanakorn, K. Corticosteroids for treating dengue shock syndrome. Cochrane Database Syst. Rev. 2006, 3, CD003488. [Google Scholar] [CrossRef] [Green Version]
- Chaiyaratana, W.; Chuansumrit, A.; Atamasirikul, K.; Tangnararatchakit, K. Serum ferritin levels in children with dengue infection. Southeast Asian J. Trop. Med. Public Health 2008, 39, 832–836. [Google Scholar]
- Leo, Y.S.; Gan, V.C.; Ng, E.L.; Hao, Y.; Ng, L.C.; Pok, K.Y.; Dimatatac, F.; Go, C.J.; Lye, D.C. Utility of warning signs in guiding admission and predicting severe disease in adult dengue. BMC Infect. Dis. 2013, 13, 498. [Google Scholar] [CrossRef] [Green Version]
- Lei, H.Y.; Yeh, T.M.; Liu, H.S.; Lin, Y.S.; Chen, S.H.; Liu, C.C. Immunopathogenesis of dengue virus infection. J. Biomed. Sci. 2001, 8, 377–388. [Google Scholar] [CrossRef]
- Simmons, C.P.; Farrar, J.J.; Nguyen v, V.; Wills, B. Dengue. N. Engl. J. Med. 2012, 366, 1423–1432. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Characteristic | Median (IQR Q1–Q3) or n/62 (%) |
|---|---|
| Age, years | 25.1 (20–35.25) |
| Male | 23 (19–32) |
| Female | 29 (22–45.5) |
| Gender | |
| male | 37 (59.7%) |
| female | 25 (40.3%) |
| BMI (kg/m2) | |
| Male | 24.45 (21.59–28.78) |
| Female | 24.03 (20.68–27.54) |
| Day of fever | 5 (4–5) |
| Confirmed dengue fever | |
| NS 1 positivity | 48 (77.4%) |
| IgM positivity | 8 (12.9%) |
| IgG positivity | 2 (3.2%) |
| IgM & IgG positivity | 4 (6.5%) |
| Warning sign present | |
| Abdominal pain | 34 (54.8%) |
| Vomiting >3/24 h | 39 (62.9%) |
| Loose stool >3/24 h | 28 (45.2%) |
| Mucosal bleeding | 7 (11.3%) |
| Lethargy, confusion | 26 (41.9%) |
| Tender liver | 0 |
| Clinical fluid accumulations | 0 |
| HCT increase with platelet decrease | 27 (44%) |
| Blood parameters during febrile phase | |
| Platelet count (×109/L) | 96.5 (65–125.75) |
| Mean platelet volume, MPV (fL) | 11.06 (10.45–11.73) |
| Plateletcrit (%) | 0.11 (0.08–0.13) |
| Hematocrit % | |
| Male | 43.2 (40.05–45.2) |
| Female | 38.9 (35.65–41.05) |
| Cortisol (nmol/L) | 321.85 (256.68–409.35) |
| Ferritin (µg/L) | 2508.87 (798.30–5217.25) |
| ROTEM Parameters (n = 62) | Median (IQR Q1–Q3) | Laboratory Normal Range |
|---|---|---|
| INTEM | ||
| CT (s) | 192.5 (170.5–211) | 100–240 |
| A10 (mm) | 43 (34.75–48) | 44–66 |
| MCF (mm) | 51 (43.75–55) | 50–72 |
| EXTEM | ||
| CT (s) | 73 (65.75–88.25) | 38–79 |
| A10 (mm) | 44 (36.5–49) | 43–65 |
| MCF (mm) | 55 (46.75–59) | 50–72 |
| FIBTEM | ||
| CT (s) | 69 (60.5–81) | n. d |
| A10 (mm) | 13 (10–15.25) | 7–23 |
| MCF (mm) | 14 (11–17) | 8–24 |
| EXTMCF-FIBMCF (mm) | 40.5 (32–44) | 41–48 |
| Conventional coagulation tests (n = 38) | ||
| INR | 1.030 (0.98–1.10) | 0.8–1.1 |
| PT (s) | 13.4 (12.8–14.32) | 11.8–14.5 |
| APTT (s) | 48.85 (43.68–52.28) * | 30–44.5 |
| Fibrinogen (g/L) | 2.7 (2.28–3.0) | 2–4 |
| Warning Signs | INTEM Median (IQR) | EXTEM Median (IQR) | FIBTEM Median (IQR) | Platelet Function (EXTMCF-FIBMCF) Median (IQR) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| n = 62 | CT (s) | A10 (mm) | MCF (mm) | CT (s) | A10 (mm) | MCF (mm) | CT (s) | A10 (mm) | MCF (mm) | |
| Abdominal pain | ||||||||||
| Yes, n = 34 | 192 (168.25–217.5) | 43.5 (35.5–48.5) | 51 (45.5–56.25) | 72 (64–90) | 45 (38–55) | 55 (47.75–59) | 68.5 (58.75–81) | 13 (10–15) | 14.5 (11–16.25) | 41.5 (33–44.25) |
| No, n = 28 | 194.5 (176–205) | 43 (34–46.75) | 50 (41.5–53.75) | 73.5 (68–87.75) | 44 (35–48) | 53.5(44–58) | 69.5 (61.25–83.25) | 13 (9.25–16) | 14 (10.25–17.75) | 37 (29.75–43) |
| p value | 0.72 | 0.53 | 0.24 | 0.63 | 0.41 | 0.25 | 0.99 | 0.84 | 0.98 | 0.17 |
| Vomiting >3/24 h | ||||||||||
| Yes, n = 39 | 184 (165–200) * | 43 (36–49) | 50 (43–55) | 73 (67–88) | 44 (38–50) | 53 (47–59) | 69 (62–75) | 13(10–16) | 14(11–17) | 41 (33–44) |
| No, n = 23 | 203 (184–224) | 44 (32–47) | 51 (44–55) | 73 (57–93) | 44 (33–49) | 55 (45–58) | 73 (57–93) | 13 (10–15) | 15 (11–16) | 40 (30–44) |
| p value | 0.01 | 0.43 | 0.93 | 0.64 | 0.71 | 0.74 | 0.73 | 0.74 | 0.68 | 0.94 |
| Diarrhea >3/24 h | ||||||||||
| Yes, n = 28 | 200 (179.75–214.75) | 43.5 (34–46.75) | 51 (42.25–55) | 73.5 (65.5–84) | 45 (34.25–48) | 55 (44.25–58) | 70.5 (58–77.5) | 12.5 (10–15.75) | 13.5 (11–17.5) | 40 (30–44) |
| No, n = 34 | 184 (165.75–205) | 43 (36–49.25) | 50.5 (45.5–57) | 72 (65.75–89.25) | 44 (38–50.25) | 54 (47.75–59) | 67.5 (60.5–82.25) | 13 (10–15.25) | 14.5 (11–17) | 40.5(34.5–44) |
| p value | 0.18 | 0.51 | 0.48 | 0.85 | 0.51 | 0.83 | 1 | 0.99 | 0.95 | 0.5 |
| Mucosal bleeding | ||||||||||
| Yes, n = 7 | 201 (156–221) | 37 (28–49) | 47 (35–60) | 73 (61–81) | 37 (29–52) | 48 (38–60) | 68 (52–73) | 12 (8–15) | 13 (7–19) | 37 (19–44) |
| No, n = 55 | 192(171–211) | 44 (35–48) | 51 (44–55) | 73 (66–89) | 45 (38–49) | 55 (47–49) | 69 (61–81) | 13 (10–16) | 14 (11–17) | 41 (32–44) |
| p value | 0.87 | 0.35 | 0.77 | 0.67 | 0.3 | 0.27 | 0.68 | 0.48 | 0.55 | 0.5 |
| Lethargy, confusion | ||||||||||
| Yes, n = 26 | 200 (173.25–20.5) | 43 (34–48.25) | 50.5 (41–55) | 74.5 (66–90.25) | 44 (34–49.5) | 54.5 (43.75–59) | 70 (63.5–79.75) | 12.5 (10–15.25) | 13.5 (11–17.25) | 39 (31.5–43.25) |
| No, n = 36 | 192 (169.5–218.75) | 44 (36–47.75) | 51 (46–55.75) | 72 (64.25–81.5) | 45 (38–48.75) | 55 (48.25–58.75) | 68.5 (58–81) | 13(10–15.75) | 14.5 (11–16.75) | 41 (33.5–44) |
| p value | 0.88 | 0.53 | 0.27 | 0.26 | 0.66 | 0.42 | 0.75 | 0.87 | 0.99 | 0.46 |
| “HCT increase” with “platelet decrease” | ||||||||||
| Yes, n = 27 | 200 (180–208) | 41 (34–46) ** | 49 (41–53) ** | 73 (66–90) | 42 (33–47) ** | 52 (44–56) ** | 70 (58–85) | 13 (10–15) | 14 (11–17) | 38 (30–42) ** |
| No, n = 35 | 184 (165–216) | 45 (38–51) | 51 (47–57) | 73 (65–82) | 46 (39–52) | 55 (50–61) | 68 (61–76) | 13 (10–16) | 14 (11–17) | 42 (35–46) |
| p value | 0.19 | 0.02 | 0.03 | 0.64 | 0.01 | 0.01 | 0.89 | 0.94 | 0.98 | 0.02 |
| Parameters | Hematocrit Level, Spearman’s Rho (p-Value) | Platelet Count, Spearman’s Rho (p-Value) |
|---|---|---|
| INTEM | ||
| CT (s) | 0.26 (p = 0.04) * | −0.23 (p = 0.07) |
| A10 (mm) | −0.21 (p = 0.10) | 0.77 (p < 0.001) * |
| MCF (mm) | −0.20 (p = 0.11) | 0.71 (p < 0.001) * |
| EXTEM | ||
| CT (s) | 0.31 (p = 0.02) * | −0.06 (p = 0.62) |
| A10 (mm) | −0.19 (p = 0.15) | 0.78 (p < 0.001) * |
| MCF (mm) | −0.22 (p = 0.09) | 0.71 (p < 0.001) * |
| FIBTEM | ||
| CT (s) | 0.27 (p = 0.04) * | −0.06 (p = 0.62) |
| A10 (mm) | −0.21 (p = 0.11) | 0.11 (p = 0.40) |
| MCF (mm) | −0.22 (p = 0.09) | 0.06 (p = 0.65) |
| EXTMCF-FIBMCF (mm) | −0.1 (p = 0.44) | 0.70 (p < 0.001) * |
| Parameters n = 62 | Febrile Phase, TP-1 Median (IQR) | Defervescence, TP-2 Median (IQR) | p-Value | Laboratory Normal Range |
|---|---|---|---|---|
| Hematocrit (%) | 41.05 (37.88–44.33) | 43.05 (38.98–46.45) * | <0.001 | 38–46 |
| Platelet (109/L) | 96.50 (65–125.8) | 65.50 (37.5–104.25) * | <0.001 | 150–400 |
| INTEM | ||||
| CT (s) | 192.50 (170.5–211) | 205 (178.5–224) * | 0.03 | 100–240 |
| A10 (mm) | 43 (34.75–48) | 40.5 (33–48.25) | 0.11 | 44–66 |
| MCF (mm) | 51 (43.75–55) | 50.0 (43–59) | 0.99 | 50–72 |
| EXTEM | ||||
| CT (s) | 73 (65.75–88.25) | 70 (63.75–75.25) * | 0.01 | 38–79 |
| A10 (mm) | 44 (36.5–49) | 40.28 (32.75–51) | 0.08 | 43–65 |
| MCF (mm) | 55 (46.75–59) | 52.18 (44–61.25) | 0.74 | 50–72 |
| FIBTEM | ||||
| CT (s) | 69 (60.5–81) | 67.63 (59.75–73.25) | 0.27 | n. d |
| A10 (mm) | 13 (10–15.25) | 13.02 (10–16) | 0.79 | 7–23 |
| MCF (mm) | 14 (11–17) | 15.68 (12–18.25) | 0.27 | 8–24 |
| EXTMCF-FIBMCF (mm) | 40.5 (32–44) | 36.75 (31.75–42) | 0.3 | 41–48 |
| Conventional coagulation, (UKMMC subjects n = 38) | ||||
| INR | 1.03 (0.98–1.10) | 0.95 (0.92–0.98) * | <0.001 | 0.8–1.1 |
| PT (s) | 13.4 (12.78–14.35) | 12.5 (12.18–12.9) * | <0.001 | 11.8–14.5 s |
| APTT (s) | 48.85 (43.55–55.3) | 43.75 (39.2–54.35) * | 0.025 | 30–44.5 s |
| Fibrinogen g/L | 2.7 (2.28–3.0) | 2.75 (2.5–3.1) | 0.18 | 2–4 g/L |
| Cortisol (nmol/L) | 321.85 (256.68–409.35) | 254.35 (202.98–366.25) * | 0.01 | >50 |
| Ferritin (µg/L) | 2508.87 (798.30–5217.25) | 3765.37 (1431.83–6393.40) | 0.06 | 4.63–204 |
| INTEM Median (IQR) | EXTEM Median (IQR) | FIBTEM Median (IQR) | Platelet Function (mm) (EXTMCF-FIBMCF) | Platelet Count (109/L) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| CT (s) | A10 (mm) | MCF (mm) | CT (s) | A10 (mm) | MCF (mm) | CT (s) | A10 (mm) | MCF (mm) | |||
| No hemorrhage, n = 45 | 205 (174–223) | 41 (37–48) | 51 (45.5–60) | 70.6 (64–76) | 41 (37–48) | 55 (47.5–62) | 67.63 (59–72) | 14 (12–16) | 15.68 (13–19) | 39 (32.5–43) | 76.5 (36.35–124) |
| Hemorrhage n = 17 | 207 (193–236.5) | 36 (21–45) | 46 (29.5–56.5) | 69.5 (64–74) | 35.5 * (25.5–42) | 47 * (34–67.3) | 66.5 (69–76) | 10.5 * (8–15) | 12 * (10–19.6) | 34.5 (22–42) | 46 (20–82) |
| p value | 0.44 | 0.18 | 0.18 | 0.41 | 0.03 | 0.046 | 0.61 | 0.049 | 0.04 | 0.34 | 0.13 |
| INR Median (IQR) | PT (sec) Median (IQR) | APTT (sec) Median (IQR) | Fibrinogen g/L Median (IQR) | |
|---|---|---|---|---|
| No hemorrhage n = 27 | 0.94 (0.88–0.98) | 12.5 (11.9–13.05) | 43.3 (38.9–49.8) | 2.85 (2.5–3.18) |
| Hemorrhage n = 11 | 0.95 (0.92–1.0) | 12.6 (12.3–13.1) | 56.3 (42.1–64.9) * | 2.6 (2.5–3) |
| p value | 0.17 | 0.12 | 0.01 | 0.43 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Syed Abas, S.S.; Abdul Karim, N.; Periyasamy, P.; Yusof, N.; Shah, S.A.; Leong, T.T.; Md Sani, S.S.; Othman, H.; Salleh, S.A.; Mohd Zaidi, N.N.; et al. Correlation of Dengue Warning Signs during Febrile Phase with Rotational Thromboelastometry, Cortisol and Feritin. Int. J. Environ. Res. Public Health 2022, 19, 807. https://doi.org/10.3390/ijerph19020807
Syed Abas SS, Abdul Karim N, Periyasamy P, Yusof N, Shah SA, Leong TT, Md Sani SS, Othman H, Salleh SA, Mohd Zaidi NN, et al. Correlation of Dengue Warning Signs during Febrile Phase with Rotational Thromboelastometry, Cortisol and Feritin. International Journal of Environmental Research and Public Health. 2022; 19(2):807. https://doi.org/10.3390/ijerph19020807
Chicago/Turabian StyleSyed Abas, Syarifah Syahirah, Noralisa Abdul Karim, Petrick Periyasamy, Nurasyikin Yusof, Shamsul Azhar Shah, Tan Toh Leong, Saiful Safuan Md Sani, Hanita Othman, Sharifah Azura Salleh, Nurul Nadiah Mohd Zaidi, and et al. 2022. "Correlation of Dengue Warning Signs during Febrile Phase with Rotational Thromboelastometry, Cortisol and Feritin" International Journal of Environmental Research and Public Health 19, no. 2: 807. https://doi.org/10.3390/ijerph19020807
APA StyleSyed Abas, S. S., Abdul Karim, N., Periyasamy, P., Yusof, N., Shah, S. A., Leong, T. T., Md Sani, S. S., Othman, H., Salleh, S. A., Mohd Zaidi, N. N., Abdul Wahid, S. F., & Wan Jamaludin, W. F. (2022). Correlation of Dengue Warning Signs during Febrile Phase with Rotational Thromboelastometry, Cortisol and Feritin. International Journal of Environmental Research and Public Health, 19(2), 807. https://doi.org/10.3390/ijerph19020807