
Comparative Study of Digital Breast Tomosynthesis (DBT) with and without Ultrasound versus Breast Magnetic Resonance Imaging (MRI) in Detecting Breast Lesion


Abstract
:1. Introduction
2. Materials and Methods
2.1. Imaging Protocols
2.2. Image Interpretation
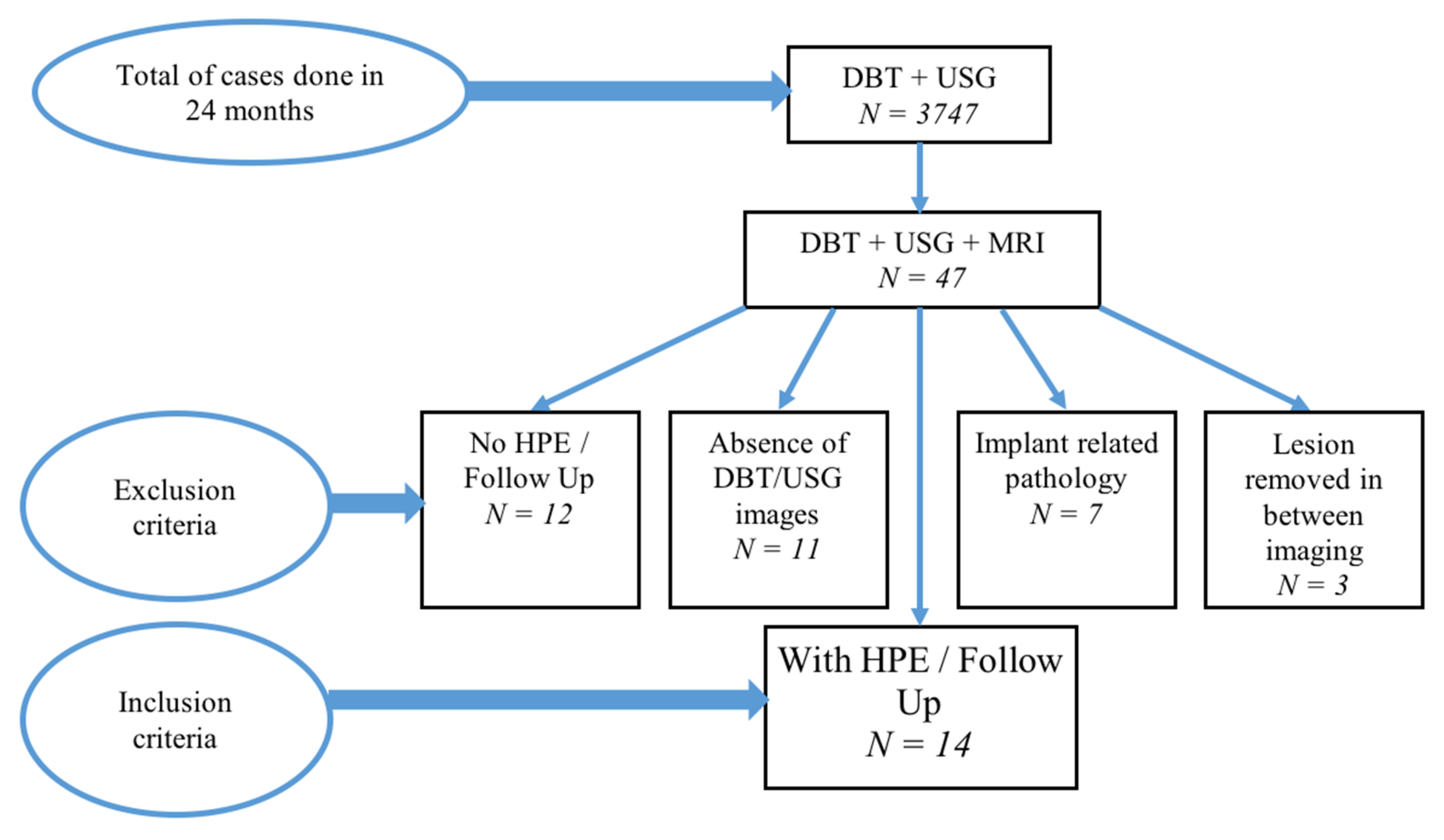
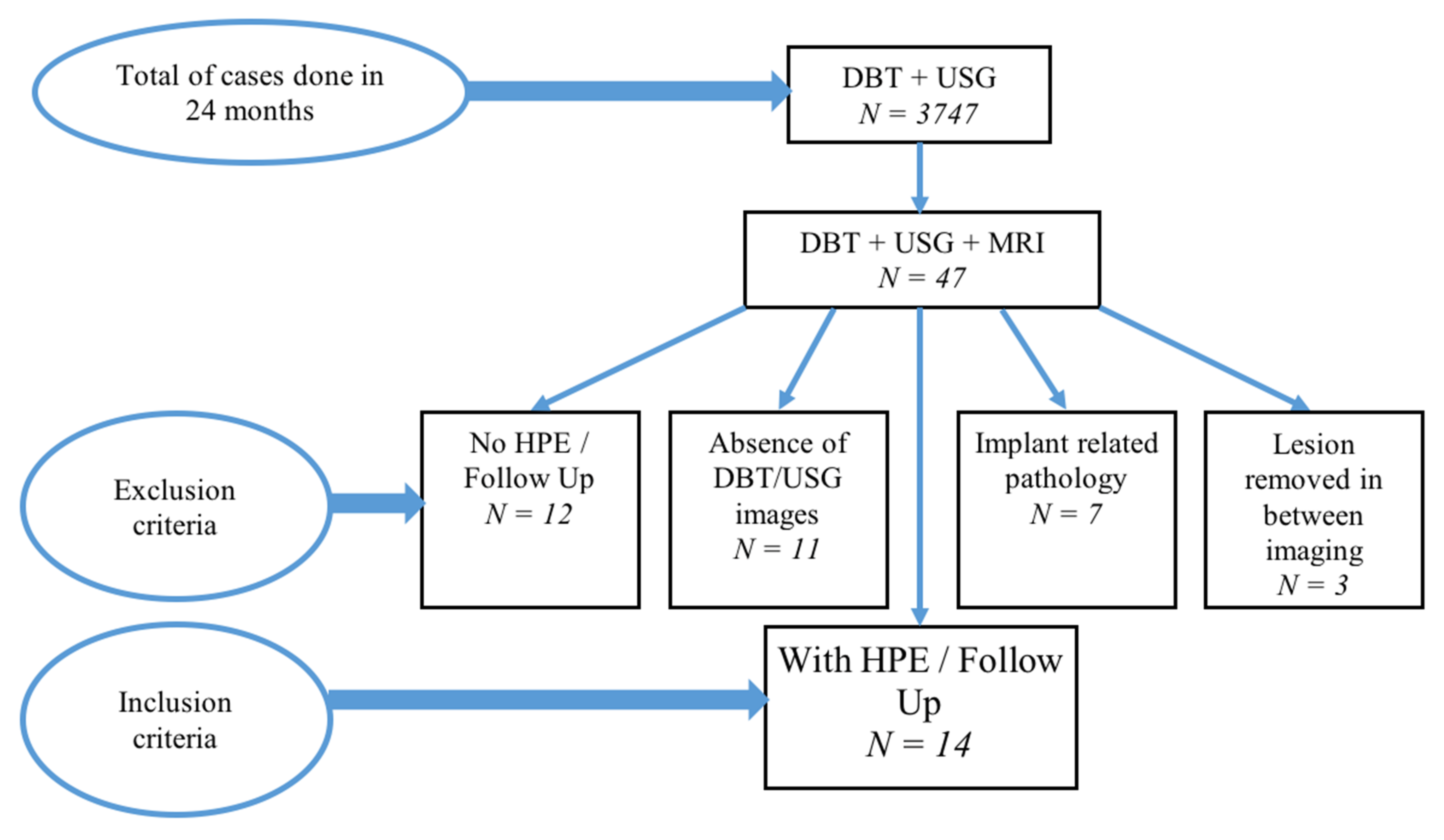
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sahran, S.; Qasem, A.; Omar, K.; Albashish, D.; Adam, A.; Abdullah, S.; Abdullah, A.; Hussain, R.; Ismail, F.; Norlia, A.; et al. Machine learning methods for breast cancer diagnostic. In Breast Cancer and Surgery; BoD—Books on Demand: Norderstedt, Germany, 2018. [Google Scholar] [CrossRef] [Green Version]
- Qasem, A.; Abdullah, S.; Sahran, S.; Ismail, F.; Hussain, R. An accurate rejection model for false positive reduction of mass localisation in mammogram. Pertanika J. Sci. Technol. 2017, 25, 49–62. [Google Scholar]
- Teoh, K.C.; Manan, H.A.; Mohd Norsuddin, N.; Rizuana, I.H. Comparison of mean glandular dose between full-field digital mammography and digital breast tomosynthesis. Healthcare 2021, 9, 1758. [Google Scholar] [CrossRef] [PubMed]
- Elmore, J.G.; Armstrong, K.; Lehman, C.D.; Fletcher, S.W. Screening for breast cancer. JAMA 2005, 293, 1245–1256. [Google Scholar] [CrossRef] [PubMed]
- Jochelson, M.S.; Pinker, K.; Dershaw, D.D.; Hughes, M.; Gibbons, G.F.; Rahbar, K.; Robson, M.E.; Mangino, D.A.; Goldman, D.; Moskowitz, C.S.; et al. Comparison of screening CEDM and MRI for women at increased risk for breast cancer: A pilot study. Eur. J. Radiol. 2017, 97, 37–43. [Google Scholar] [CrossRef]
- McDonald, E.S.; Oustimov, A.; Weinstein, S.P.; Synnestvedt, M.B.; Schnall, M.; Conant, E.F. Effectiveness of digital breast tomosynthesis compared with digital mammography: Outcomes analysis from 3 years of breast cancer screening. JAMA Oncol. 2016, 2, 737–743. [Google Scholar] [CrossRef] [Green Version]
- Zuckerman, S.P.; Conant, E.F.; Keller, B.M.; Maidment, A.D.; Barufaldi, B.; Weinstein, S.P.; Synnestvedt, M.; McDonald, E.S. Implementation of synthesized two-dimensional mammography in a population-based digital breast tomosynthesis screening program. Radiology 2016, 281, 730–736. [Google Scholar] [CrossRef] [Green Version]
- Roganovic, D.; Djilas, D.; Vujnovic, S.; Pavic, D.; Stojanov, D. Breast MRI, digital mammography and breast tomosynthesis: Comparison of three methods for early detection of breast cancer. Bosn. J. Basic Med. Sci. 2015, 15, 64–68. [Google Scholar] [CrossRef] [Green Version]
- Kamal, R.; Mansour, S.; ElMesidy, D.; Moussa, K.; Hussien, A. Detection and diagnosis of breast lesions: Performance evaluation of digital breast tomosynthesis and magnetic resonance mammography. Egypt. J. Radiol. Nucl. Med. 2016, 47, 1159–1172. [Google Scholar] [CrossRef] [Green Version]
- Saxena, S.; Meena, D.R.; Sharma, T.; Khokhar, H. Comparative evaluation of palpable breast lumps by digital breast tomosynthesis and MRI breast with its histopathological correlation. Int. J. Contemp. Med. Surg. Radiol. 2019, 4, B133–B139. [Google Scholar] [CrossRef]
- Comstock, C.E.; Gatsonis, C.; Newstead, G.M.; Snyder, B.S.; Gareen, I.F.; Bergin, J.T.; Rahbar, H.; Sung, J.S.; Jacobs, C.; Harvey, J.A.; et al. Comparison of abbreviated breast MRI vs digital breast tomosynthesis for breast cancer detection among women with dense breasts undergoing screening. JAMA 2020, 323, 746–756. [Google Scholar] [CrossRef]
- Ohuchi, N.; Suzuki, A.; Sobue, T.; Kawai, M.; Yamamoto, S.; Zheng, Y.F.; Shiono, Y.N.; Saito, H.; Kuriyama, S.; Tohno, E.; et al. Sensitivity and specificity of mammography and adjunctive ultrasonography to screen for breast cancer in the Japan Strategic Anti-cancer Randomized Trial (J-START): A randomised controlled trial. Lancet 2016, 387, 341–348. [Google Scholar] [CrossRef]
- Berg, W.A.; Blume, J.D.; Cormack, J.B.; Mendelson, E.B.; Lehrer, D.; Böhm-Vélez, M.; Pisano, E.D.; Jong, R.A.; Evans, W.P.; Morton, M.J.; et al. Combined screening with ultrasound and mammography vs mammography alone in women at elevated risk of breast cancer. JAMA 2008, 299, 2151–2163. [Google Scholar] [CrossRef]
- Sprague, B.L.; Stout, N.K.; Schechter, C.; van Ravesteyn, N.T.; Cevik, M.; Alagoz, O.; Lee, C.I.; van den Broek, J.J.; Miglioretti, D.L.; Mandelblatt, J.S.; et al. Benefits, harms, and cost-effectiveness of supplemental ultrasonography screening for women with dense breasts. Ann. Intern. Med. 2015, 162, 157–166. [Google Scholar] [CrossRef] [Green Version]
- Hooley, R.J.; Greenberg, K.L.; Stackhouse, R.M.; Geisel, J.L.; Butler, R.S.; Philpotts, L.E. Screening US in patients with mammographically dense breasts: Initial experience with Connecticut Public Act 09-41. Radiology 2012, 265, 59–69. [Google Scholar] [CrossRef]
- Scheel, J.R.; Lee, J.M.; Sprague, B.L.; Lee, C.I.; Lehman, C.D. Screening ultrasound as an adjunct to mammography in women with mammographically dense breasts. Am. J. Obstet. Gynecol. 2015, 212, 9–17. [Google Scholar] [CrossRef] [Green Version]
- Chae, E.Y.; Kim, H.H.; Cha, J.H.; Shin, H.J.; Kim, H. Evaluation of screening whole-breast sonography as a supplemental tool in conjunction with mammography in women with dense breasts. J. Ultrasound Med. 2013, 32, 1573–1578. [Google Scholar] [CrossRef]
- Gartlehner, G.; Thaler, K.; Chapman, A.; Kaminski-Hartenthaler, A.; Berzaczy, D.; Van Noord, M.G.; Helbich, T.H. Mammography in combination with breast ultrasonography versus mammography for breast cancer screening in women at average risk. Cochrane Database Syst. Rev. 2013, 2013, CD009632. [Google Scholar] [CrossRef]
- Orel, S.G.; Schnall, M.D. MR Imaging of the breast for the detection, diagnosis, and staging of breast cancer. Radiology 2001, 220, 13–30. [Google Scholar] [CrossRef]
- Van Goethem, M.; Schelfout, K.; Dijckmans, L.; Van Der Auwera, J.C.; Weyler, J.; Verslegers, I.; Biltjes, I.; De Schepper, A. MR mammography in the pre-operative staging of breast cancer in patients with dense breast tissue: Comparison with mammography and ultra-sound. Eur. Radiol. 2004, 14, 809–816. [Google Scholar] [CrossRef]
- Lieske, B.; Ravichandran, D.; Alvi, A.; Lawrence, D.A.S.; Wright, D.J. Screen-detected breast lesions with an indeterminate (B3) core needle biopsy should be excised. Eur. J. Surg. Oncol. 2008, 34, 1293–1298. [Google Scholar] [CrossRef]
- Bianchi, S.; Caini, S.; Renne, G.; Cassano, E.; Ambrogetti, D.; Cattani, M.G.; Saguatti, G.; Chiaramondia, M.; Bellotti, E.; Bottiglieri, R.; et al. Positive predictive value for malignancy on surgical excision of breast lesions of uncertain malignant potential (B3) diagnosed by stereotactic vacuum-assisted needle core biopsy (VANCB): A large multi-institutional study in Italy. Breast 2011, 20, 264–270. [Google Scholar] [CrossRef]
- Forester, N.D.; Lowes, S.; Mitchell, E.; Twiddy, M. High risk (B3) breast lesions: What is the incidence of malignancy for individual lesion subtypes? A systematic review and meta-analysis. Eur. J. Surg. Oncol. 2019, 45, 519–527. [Google Scholar] [CrossRef]
- Sudhir, R.; Sannapareddy, K.; Potlapalli, A.; Krishnamurthy, P.B.; Buddha, S.; Koppula, V. Diagnostic accuracy of contrast-enhanced digital mammography in breast cancer detection in comparison to tomosynthesis, synthetic 2D mammography and tomosynthesis combined with ultrasound in women with dense breast. Br. J. Radiol. 2021, 94, 20201046. [Google Scholar] [CrossRef]
- Dibble, E.H.; Singer, T.M.; Jimoh, N.; Baird, G.L.; Lourenco, A.P. Dense Breast Ultrasound Screening After Digital Mammography Versus After Digital Breast Tomosynthesis. AJR Am. J. Roentgenol. 2019, 213, 1397–1402. [Google Scholar] [CrossRef] [PubMed]
- Cai, S.; Yan, J.; Cai, D.; Huang, M.; Lin, L. Comparative study on diagnosis efficacy of digital breast tomosynthesis and color Doppler ultrasound for breast lesions. Int. J. Clin. Exp. Med. 2018, 11, 3455–3461. [Google Scholar]
- Mariscotti, G.; Houssami, N.; Durando, M.; Bergamasco, L.; Campanino, P.P.; Ruggieri, C.; Regini, E.; Luparia, A.; Bussone, R.; Sapino, A.; et al. Accuracy of mammography, digital breast tomosynthesis, ultrasound and MR imaging in preoperative assessment of breast cancer. Anticancer Res. 2014, 34, 1219–1225. [Google Scholar]
- Bonnie, N.J.; Edward, A.S. The evolution of breast imaging: Past to present. Radiology 2014, 273, S23–S44. [Google Scholar] [CrossRef] [Green Version]
- Murakami, R.; Tani, H.; Kumita, S.; Uchiyama, N. Diagnostic performance of digital breast tomosynthesis for predicting response to neoadjuvant systemic therapy in breast cancer patients: A comparison with magnetic resonance imaging, ultrasound, and full-field digital mammography. Acta Radiol. Open 2021, 10, 1–8. [Google Scholar] [CrossRef]
- Förnvik, D.; Kataoka, M.; Iima, M.; Ohashi, A.; Kanao, S.; Toi, M.; Togashi, K. The role of breast tomosynthesis in a predominantly dense breast population at a tertiary breast centre: Breast density assessment and diagnostic performance in comparison with MRI. Eur. Radiol. 2018, 28, 3194–3203. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
| No. of Patient | Age (Year) | Ethnicity | Symptom | Duration Interval between Two Imaging Modalities |
|---|---|---|---|---|
| 1. | 72 | Indian | X | ≤1 month |
| 2. | 56 | Malay | X | ≤1 month |
| 3. | 65 | Malay | √ | ≤1 month |
| 4. | 58 | Chinese | X | >3 months |
| 5. | 58 | Malay | X | >3 months |
| 6. | 60 | Malay | √ | >3 months |
| 7. | 54 | Malay | X | >3 months |
| 8. | 78 | Chinese | √ | >1 month to ≤3 months |
| 9. | 42 | Malay | √ | Same day |
| 10. | 36 | Malay | √ | >1 month to ≤3 months |
| 11. | 40 | Chinese | √ | >1 month to ≤3 months |
| 12. | 65 | Malay | X | ≤1 month |
| 13. | 42 | Malay | √ | >3 months |
| 14. | 46 | Malay | √ | ≤1 month |
| No. | Age | Breast Composition (BI-RADS) | BI-RADS Category | Follow Up DBT (BI-RADS) | CONCLUSION (BIOPSY/FOLLOW UP) | ||
|---|---|---|---|---|---|---|---|
| DBT | DBT + USG | MRI | |||||
| 1. | 72 | b | 4 | 4 | 4 | N/A | ILC |
| 2. | 56 | b | 5 | 5 | 5 | N/A | IDC |
| 3. | 56 | b | 1 | 1 | 5 | N/A | IDC |
| 4. | 65 | c | 4 | 5 | 5 | N/A | IDC |
| 5. | 65 | c | 1 | 1 | 2 | 1 | Stable lesion |
| 6. | 65 | c | 1 | 1 | 2 | 1 | Stable lesion |
| 7. | 65 | c | 1 | 1 | 2 | 1 | Stable lesion |
| 8. | 65 | c | 3 | 2 | 2 | 2 | Benign breast tissue |
| 9. | 58 | c | 1 | 2 | 2 | 1 | Stable lesion |
| 10. | 58 | c | 1 | 2 | 2 | 1 | Stable lesion |
| 11. | 58 | c | 1 | 1 | 2 | 1 | Fibroglandular tissue |
| 12. | 58 | c | 3 | 2 | 2 | 2 | Scar |
| 13. | 58 | c | 4 | 4 | 2 | 2 | Radiotherapy changes |
| 14. | 60 | c | 2 | 2 | 2 | 2 | Stable lesion |
| 15. | 54 | a | 4 | 5 | 5 | N/A | IDC |
| 16. | 78 | c | 1 | 3 | 4 | N/A | Benign breast tissue |
| 17. | 42 | c | 4 | 4 | 4 | N/A | Benign breast tissue |
| 18. | 36 | d | 5 | 5 | 5 | N/A | IDC |
| 19. | 36 | d | 1 | 2 | 3 | N/A | Benign breast tissue |
| 20. | 40 | c | 4 | 5 | 5 | N/A | ILC |
| 21. | 65 | c | 5 | 5 | 5 | N/A | ILC |
| 22. | 65 | c | 1 | 1 | 2 | 1 | Resolved |
| 23. | 42 | c | 2 | 2 | 2 | N/A | Fibroadenoma |
| 24. | 46 | c | 4 | 5 | 5 | N/A | ILC |
| Type of Lesion | Histopathology/Follow Up DBT | TOTAL | |
|---|---|---|---|
| Benign | Malignant | ||
| DBT | |||
| Benign | 11 | 1 | 12 |
| Malignant | 4 | 8 | 12 |
| DBT + USG | |||
| Benign | 12 | 1 | 13 |
| Malignant | 3 | 8 | 11 |
| MRI breast | |||
| Benign | 10 | 0 | 10 |
| Malignant | 5 | 9 | 14 |
| TOTAL | 15 | 9 | 24 |
| Accuracy (%) | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) | |
|---|---|---|---|---|---|
| DBT | 79.1 | 88.9 | 73.3 | 66.7 | 91.6 |
| DBT + USG | 83.3 | 88.9 | 80 | 72.7 | 92.3 |
| MRI | 79.1 | 100 | 66.7 | 64.3 | 100 |
| Modalities | Ch2 | df | p-Value |
|---|---|---|---|
| DBT | 8.711 | 1 | 0.003 * |
| DBT + USG | 10.752 | 1 | 0.001 * |
| MRI | 10.286 | 1 | 0.001 * |
| Data Source | Year | No. of Lesion/Patient | DBT | DBT + USG | DM + DBT + USG | MRI |
|---|---|---|---|---|---|---|
| Present study | 2021 | 24 lesions | √ | √ | √ | |
| Sudhir et al. | 2021 | 166 lesions | √ | √ | ||
| Comstock et al. | 2020 | 1444 patients | √ | √ | ||
| Dibble et al. | 2019 | 3183 breasts | √ | |||
| Saxena et al. | 2019 | 50 patients | √ | √ | ||
| Kamal et al. | 2016 | 103 lesions | √ | √ | ||
| Roganovic et al. | 2015 | 57 lesions | √ | √ | ||
| Mariscotti et al. | 2014 | 200 patients | √ | √ | √ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goh, J.H.L.; Tan, T.L.; Aziz, S.; Rizuana, I.H. Comparative Study of Digital Breast Tomosynthesis (DBT) with and without Ultrasound versus Breast Magnetic Resonance Imaging (MRI) in Detecting Breast Lesion. Int. J. Environ. Res. Public Health 2022, 19, 759. https://doi.org/10.3390/ijerph19020759
Goh JHL, Tan TL, Aziz S, Rizuana IH. Comparative Study of Digital Breast Tomosynthesis (DBT) with and without Ultrasound versus Breast Magnetic Resonance Imaging (MRI) in Detecting Breast Lesion. International Journal of Environmental Research and Public Health. 2022; 19(2):759. https://doi.org/10.3390/ijerph19020759
Chicago/Turabian StyleGoh, Janice Hui Ling, Toh Leong Tan, Suraya Aziz, and Iqbal Hussain Rizuana. 2022. "Comparative Study of Digital Breast Tomosynthesis (DBT) with and without Ultrasound versus Breast Magnetic Resonance Imaging (MRI) in Detecting Breast Lesion" International Journal of Environmental Research and Public Health 19, no. 2: 759. https://doi.org/10.3390/ijerph19020759
APA StyleGoh, J. H. L., Tan, T. L., Aziz, S., & Rizuana, I. H. (2022). Comparative Study of Digital Breast Tomosynthesis (DBT) with and without Ultrasound versus Breast Magnetic Resonance Imaging (MRI) in Detecting Breast Lesion. International Journal of Environmental Research and Public Health, 19(2), 759. https://doi.org/10.3390/ijerph19020759