
Territorial Strategy of Medical Units for Addressing the First Wave of the COVID-19 Pandemic in the Metropolitan Area of Mexico City: Analysis of Mobility, Accessibility and Marginalization

 , , ,
, , ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Area
2.2. Mexico’s Health Care System
2.3. Demographic and Population Mobility Data
2.4. Analytical and Statistical Methods
2.4.1. Identification of Infection Trends by Territory
2.4.2. Recognition of Patterns of Mobility toward Medical Units
2.4.3. Evaluation of the Hospital Strategy by Territory
2.4.4. Measurement of Accessibility to COVID Hospitals
3. Results
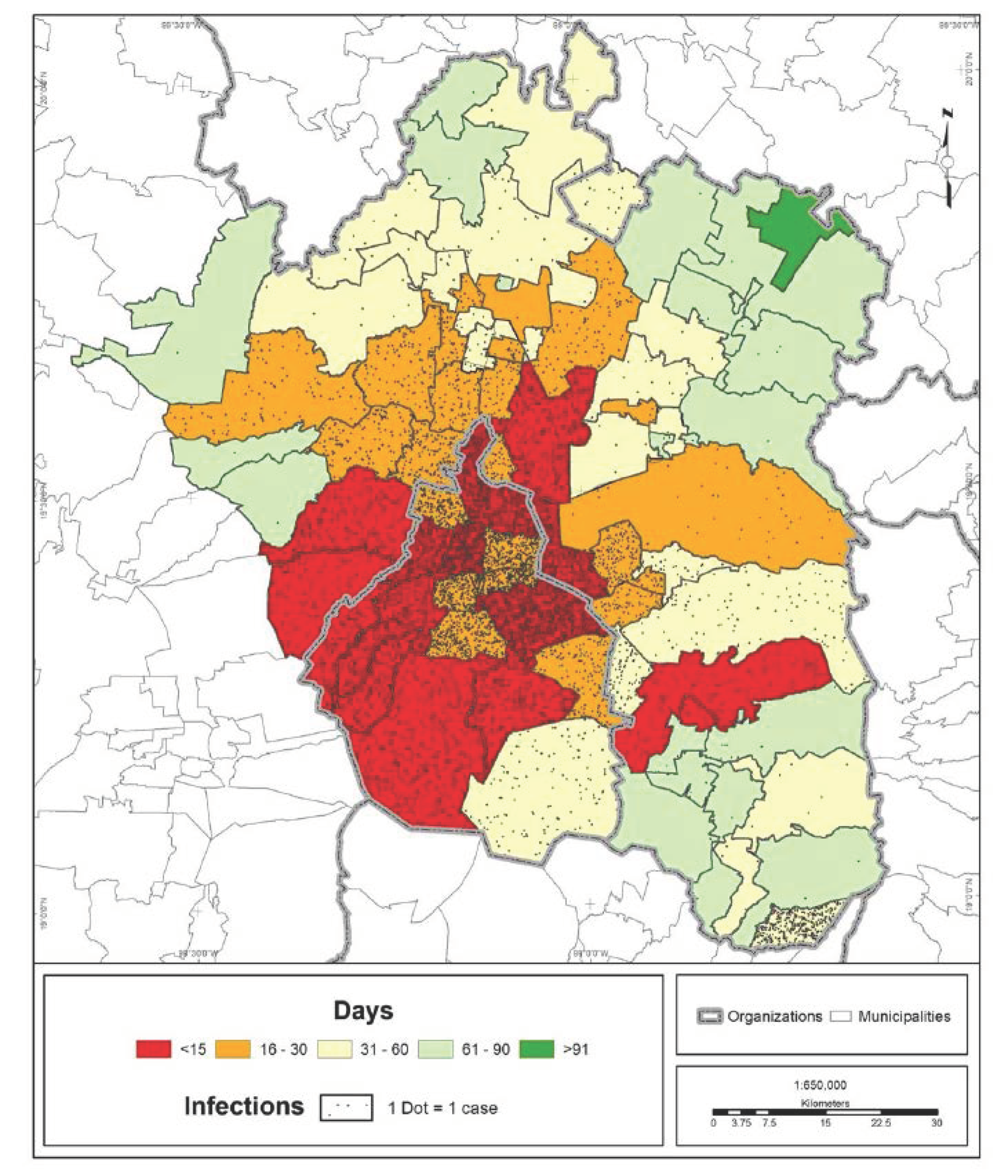
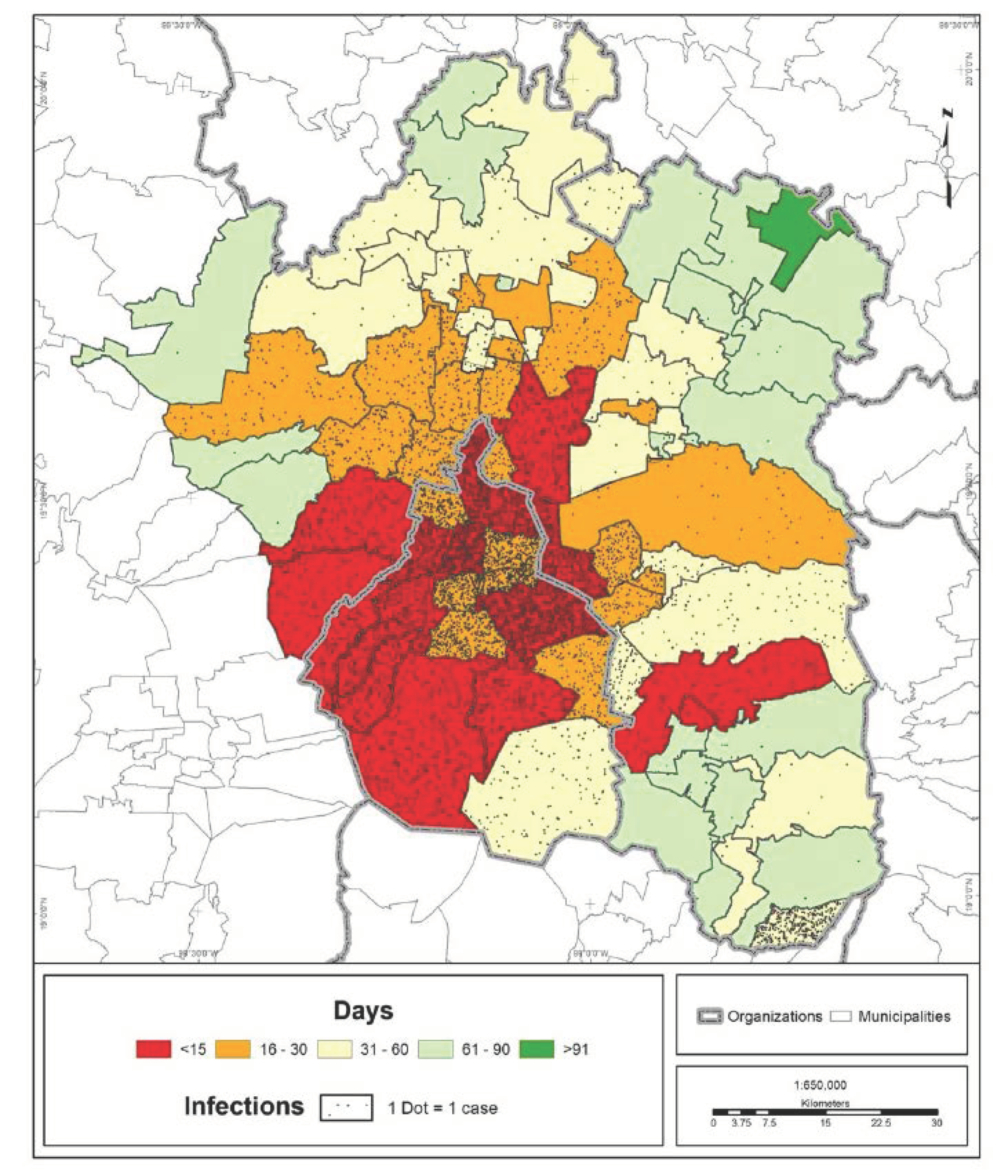
3.1. COVID-19 Infection Trend by Territory
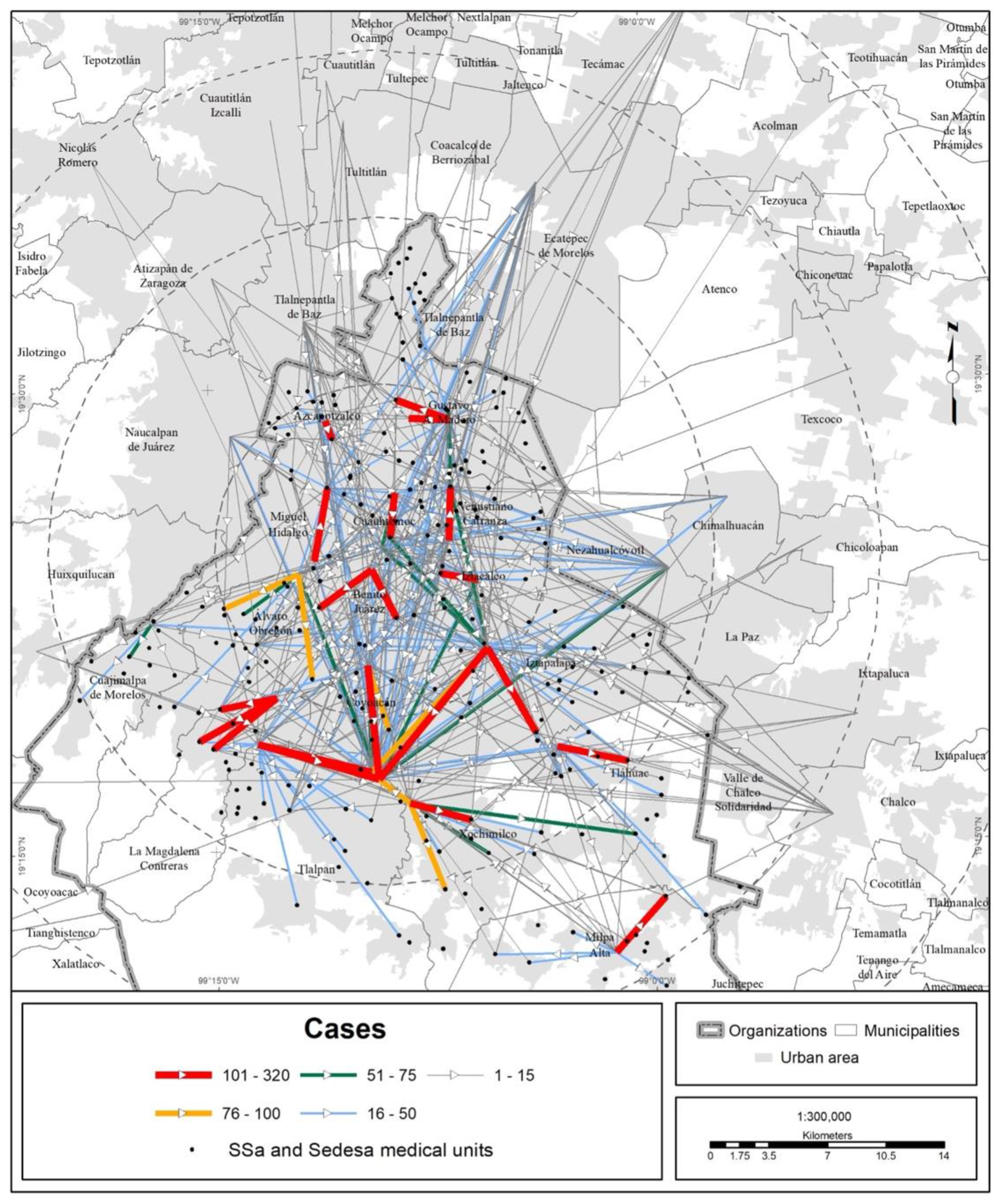
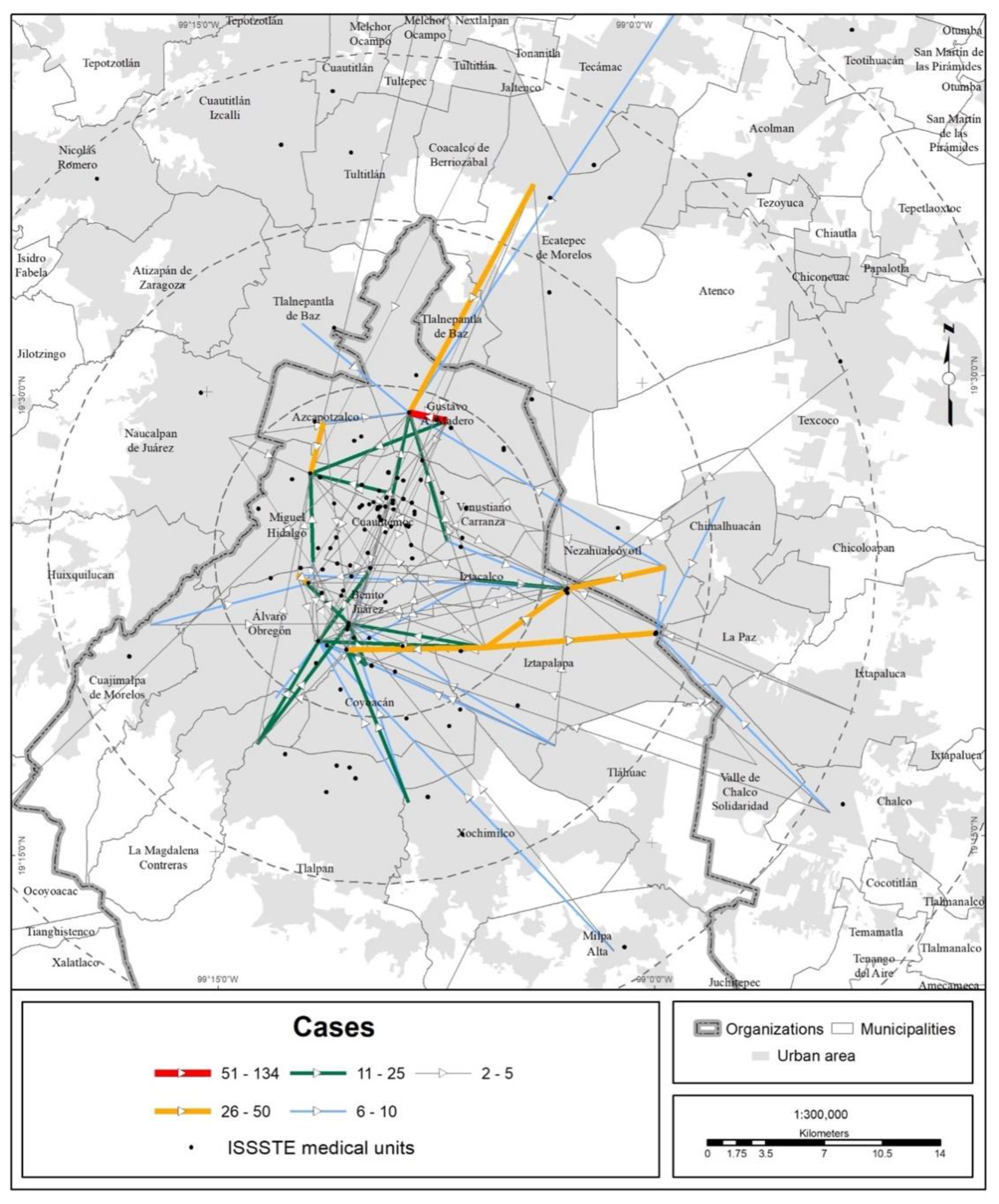
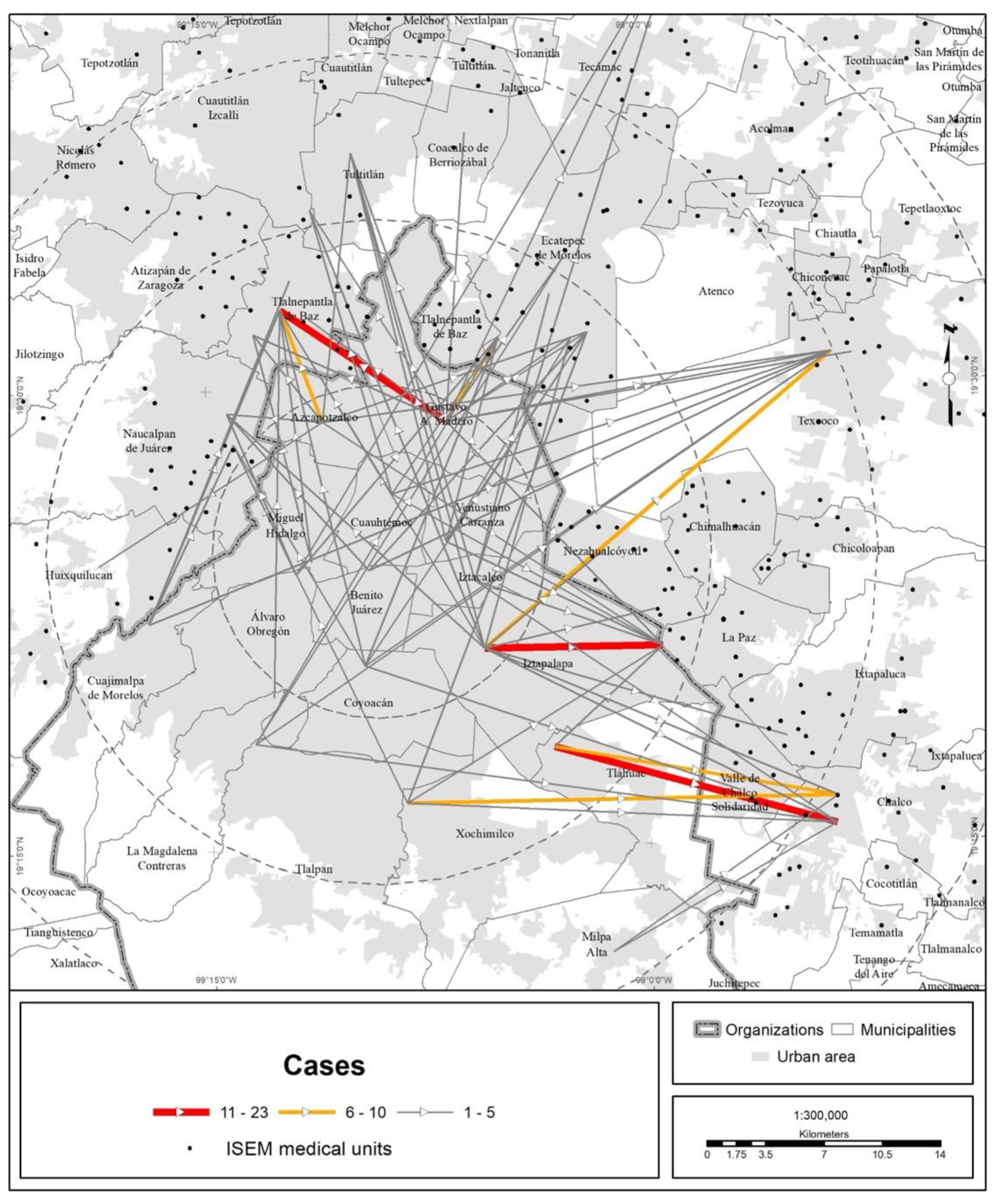
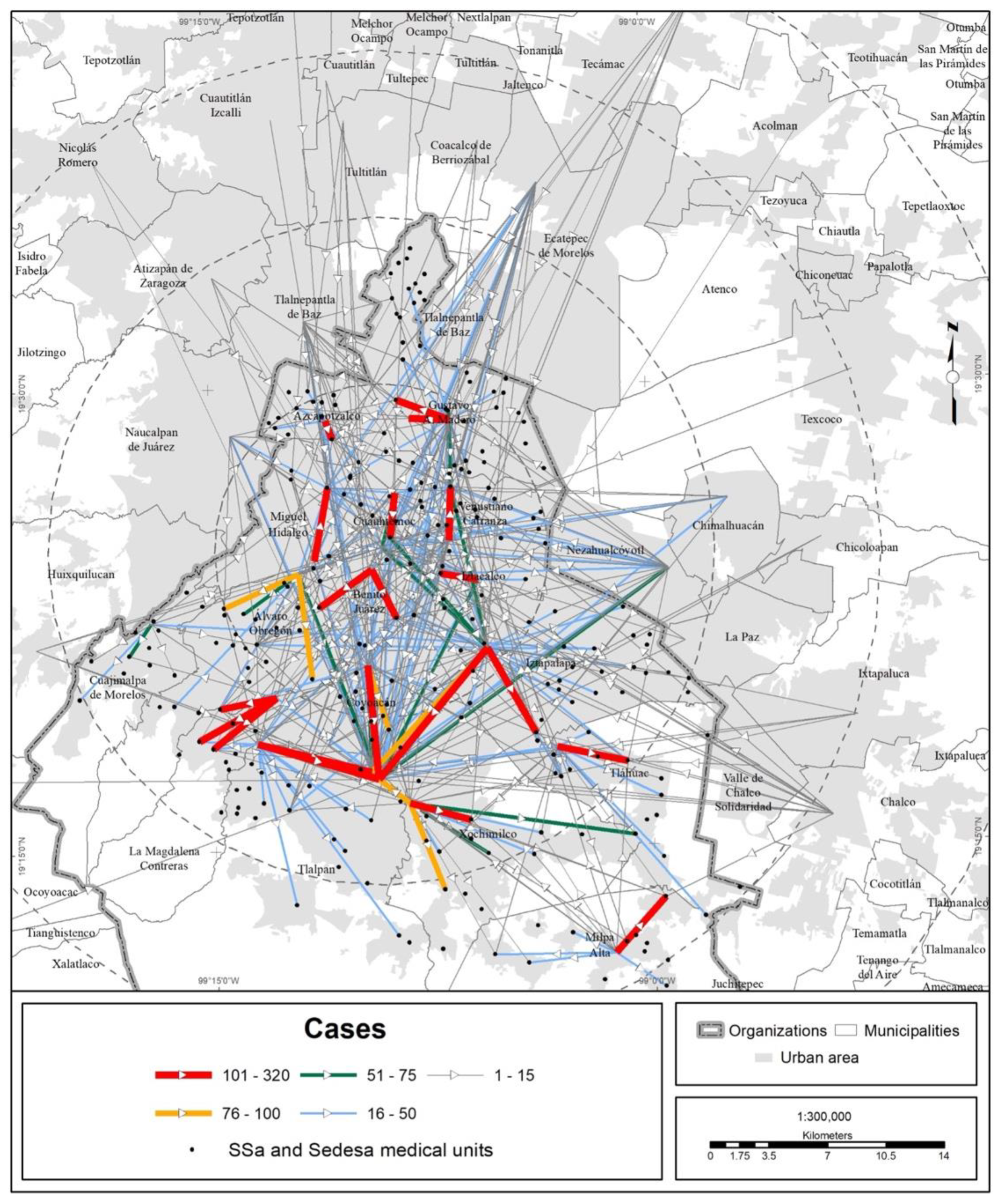
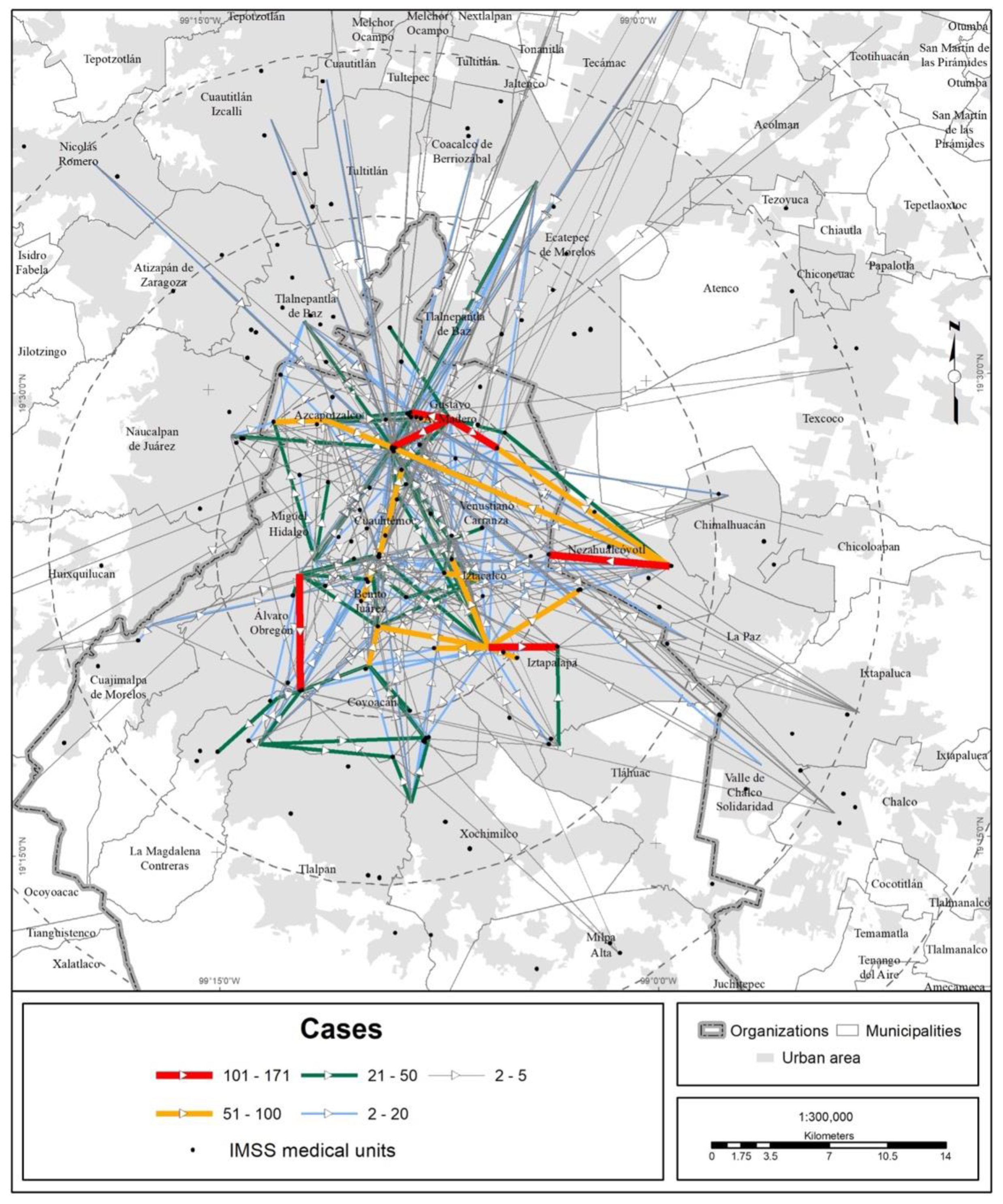
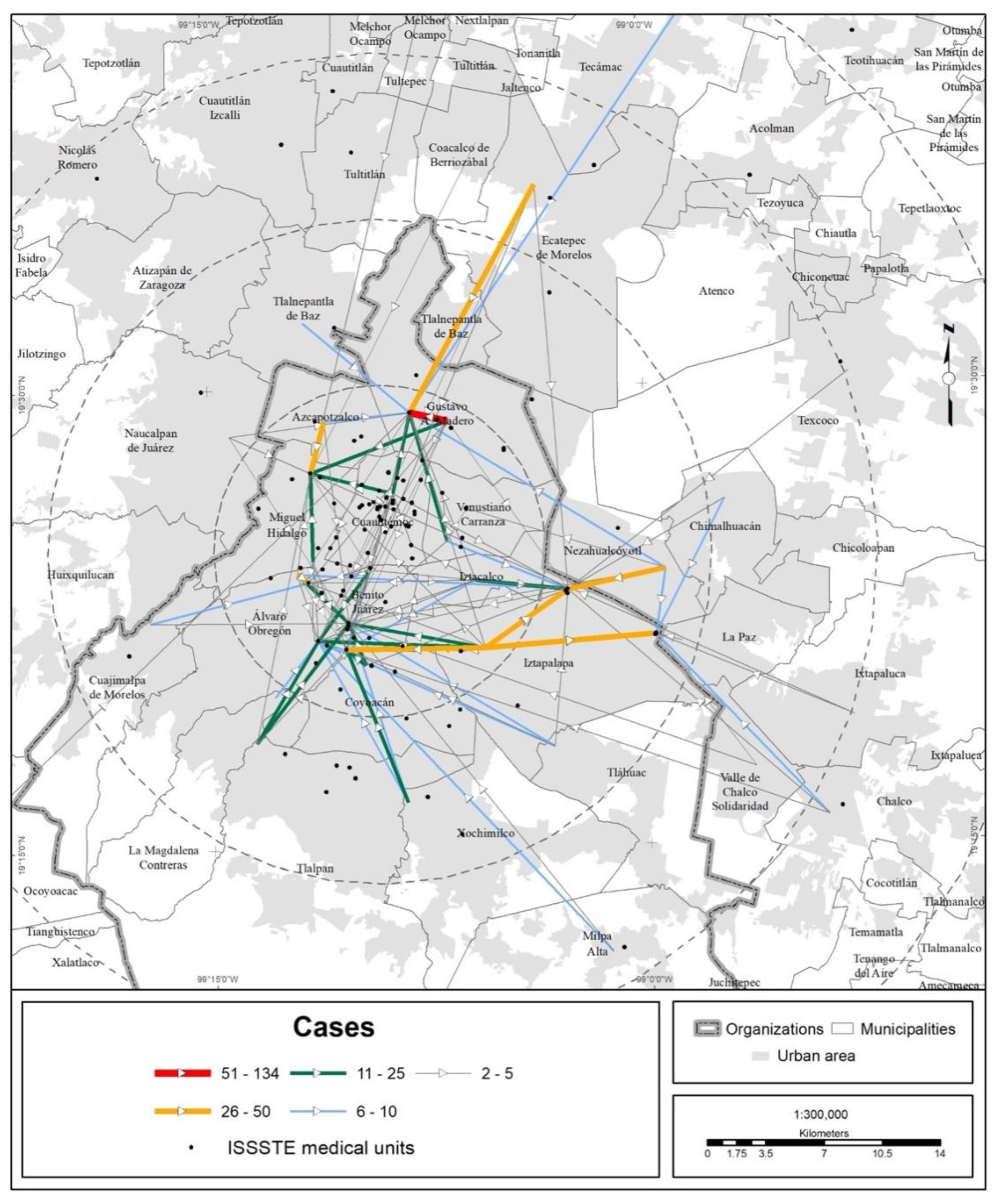
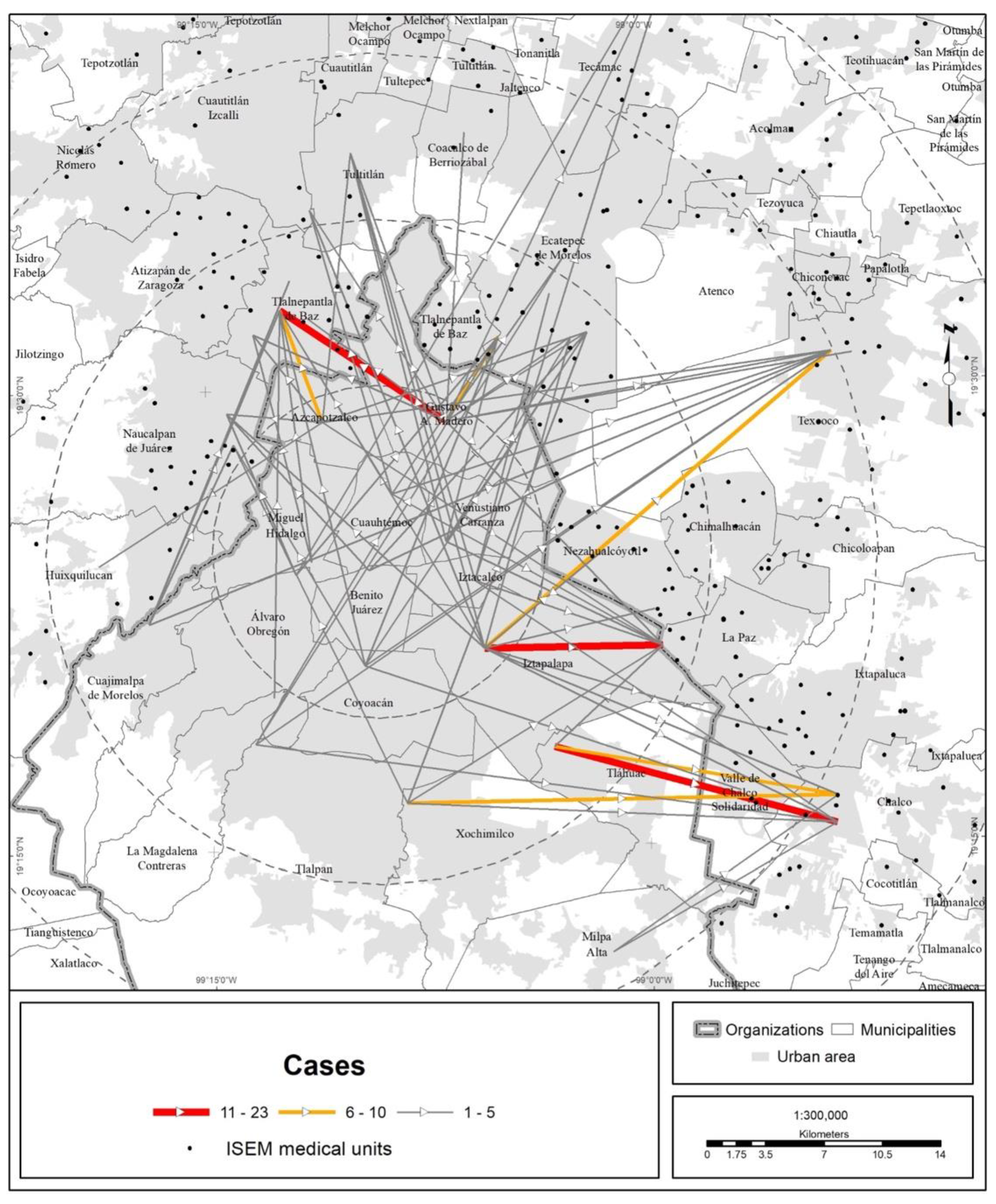
3.2. Mobility of the Population to Medical Units
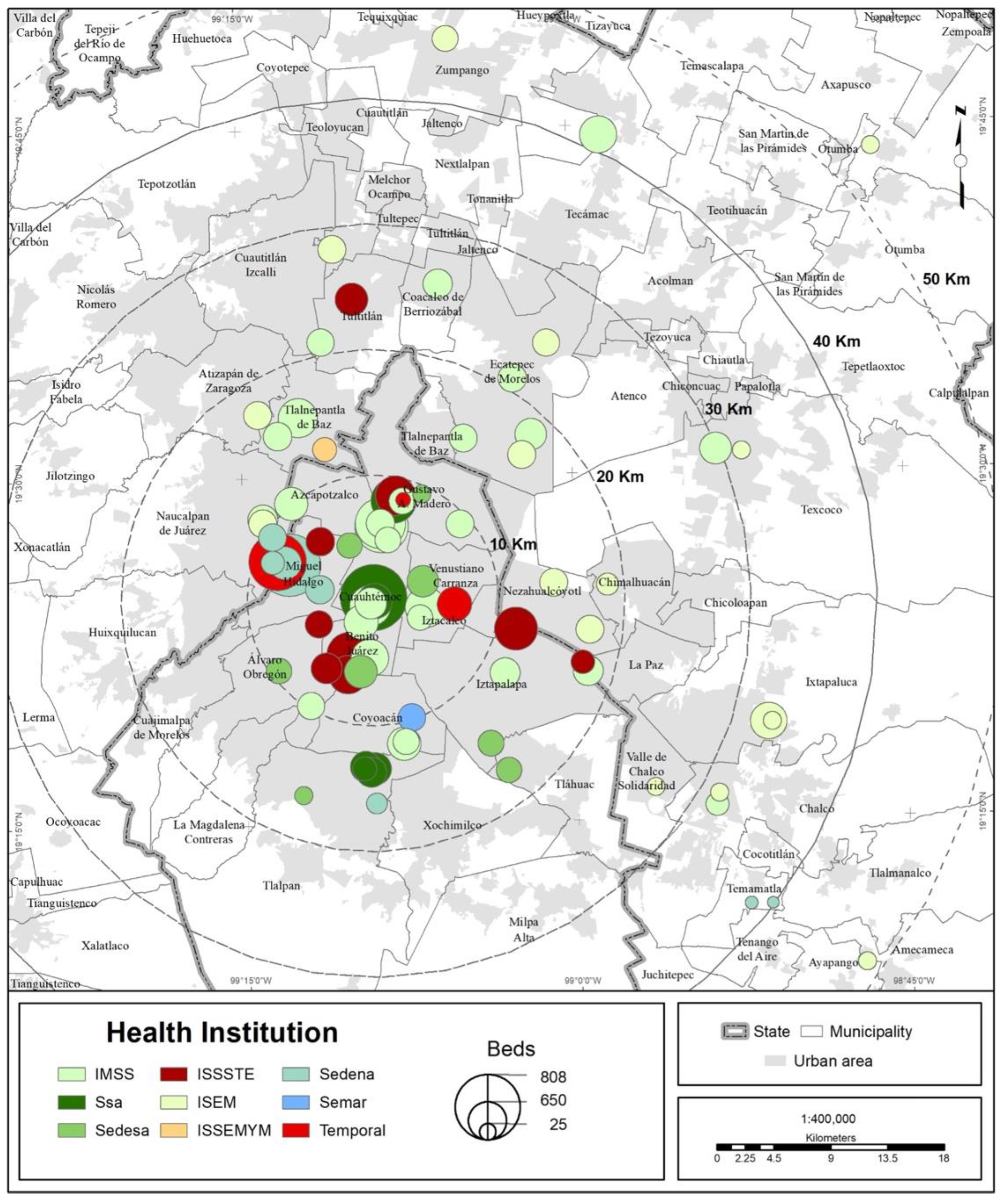
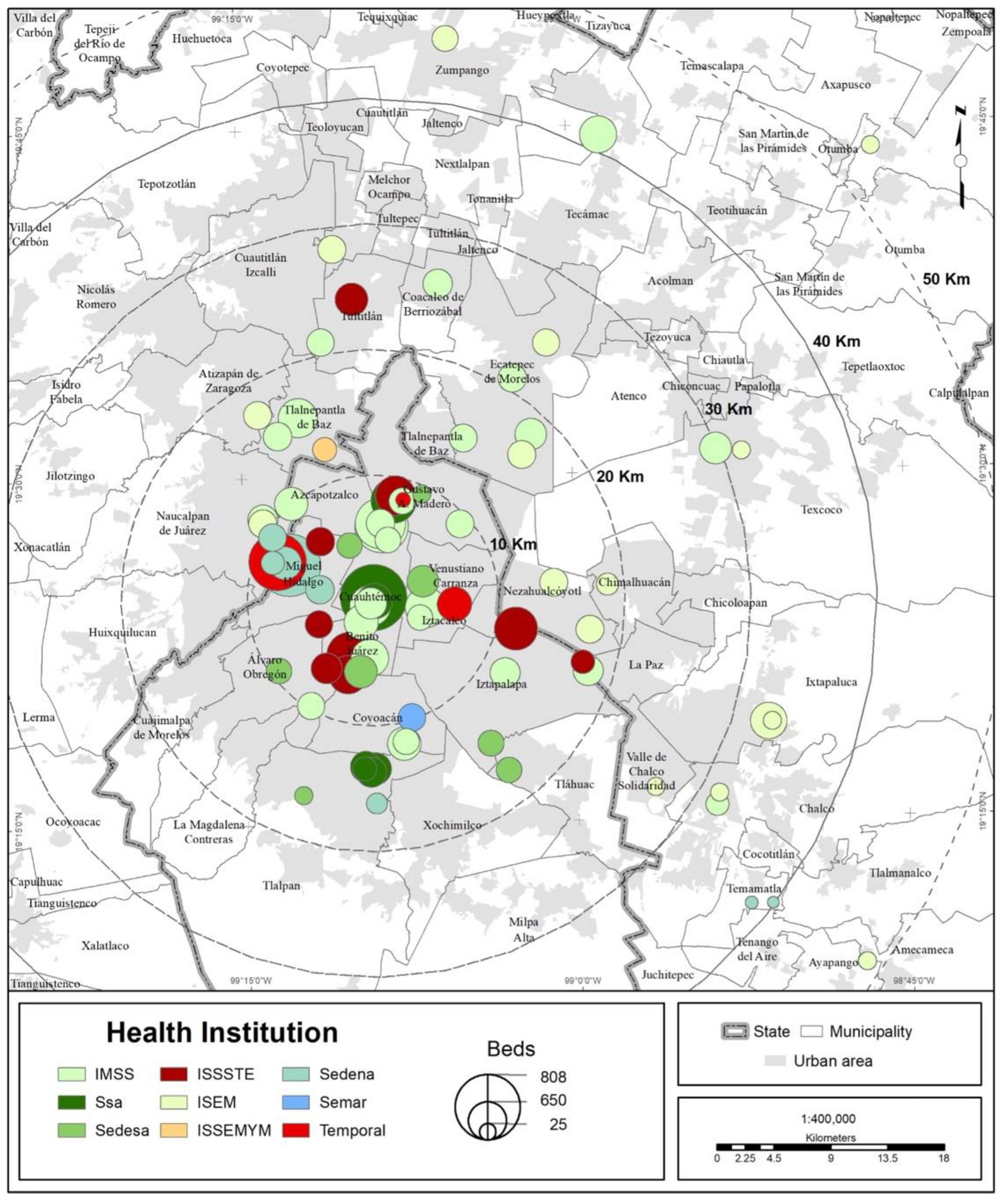
3.3. Territorial Evaluation of the COVID Hospital Strategy
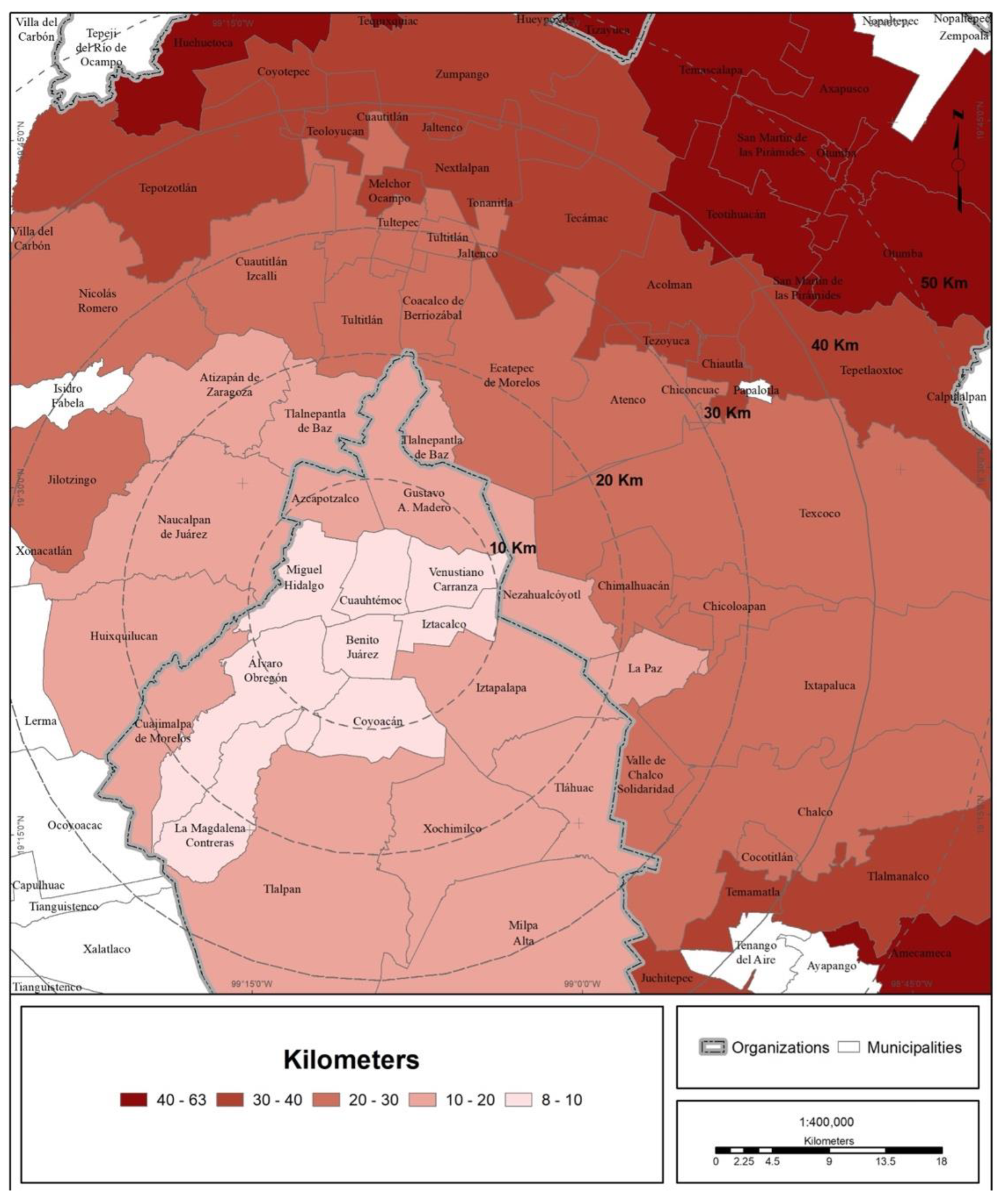
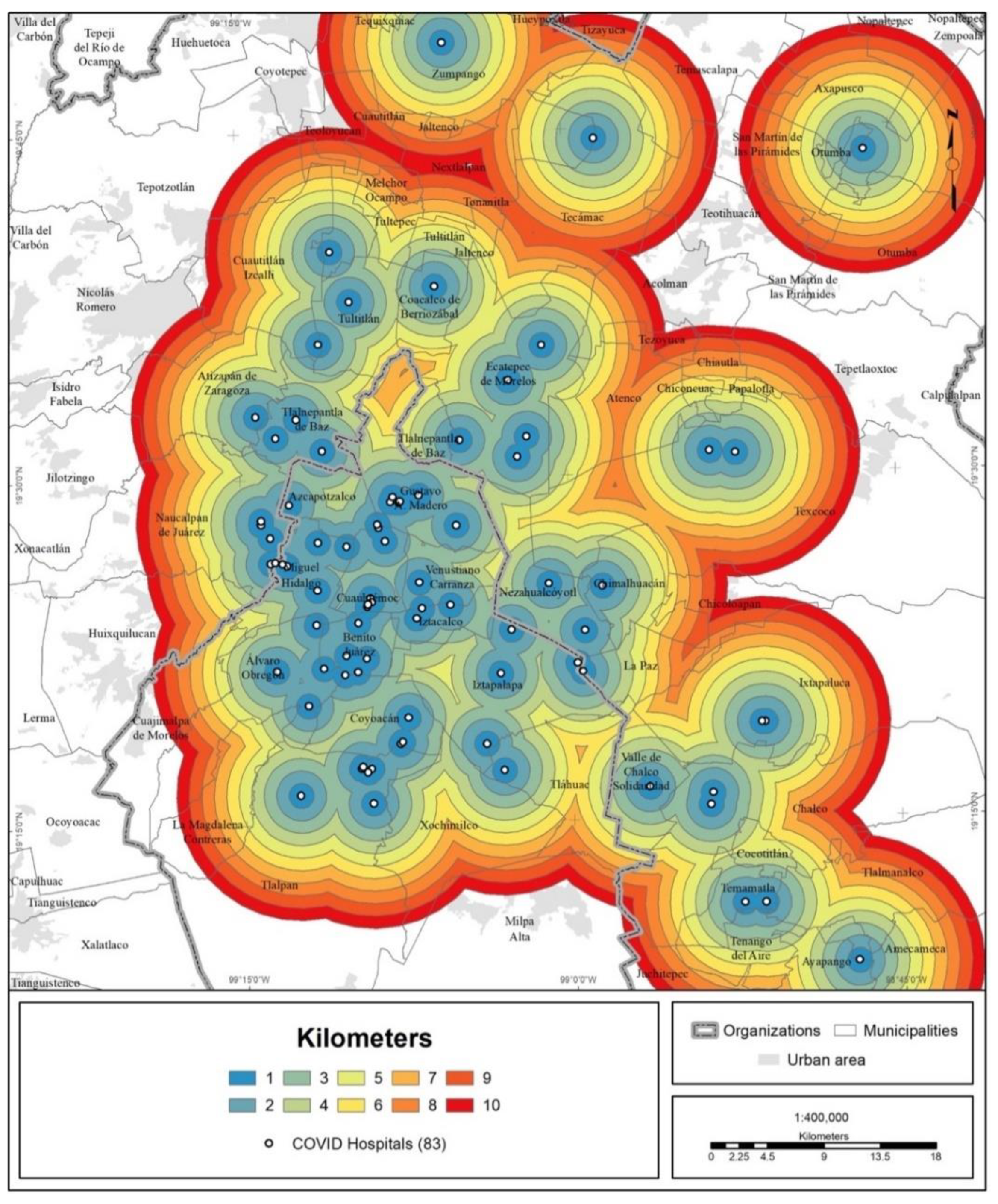
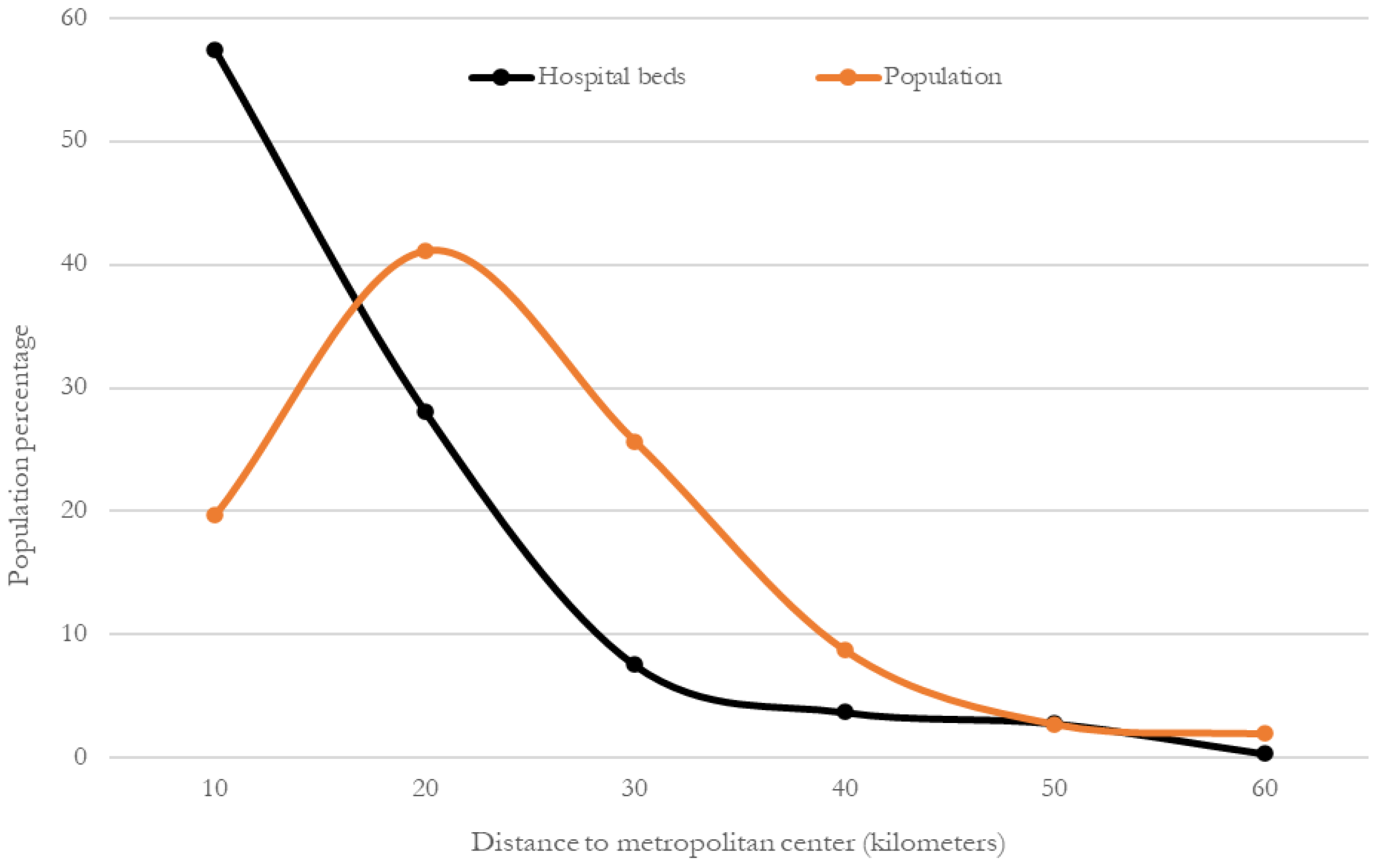
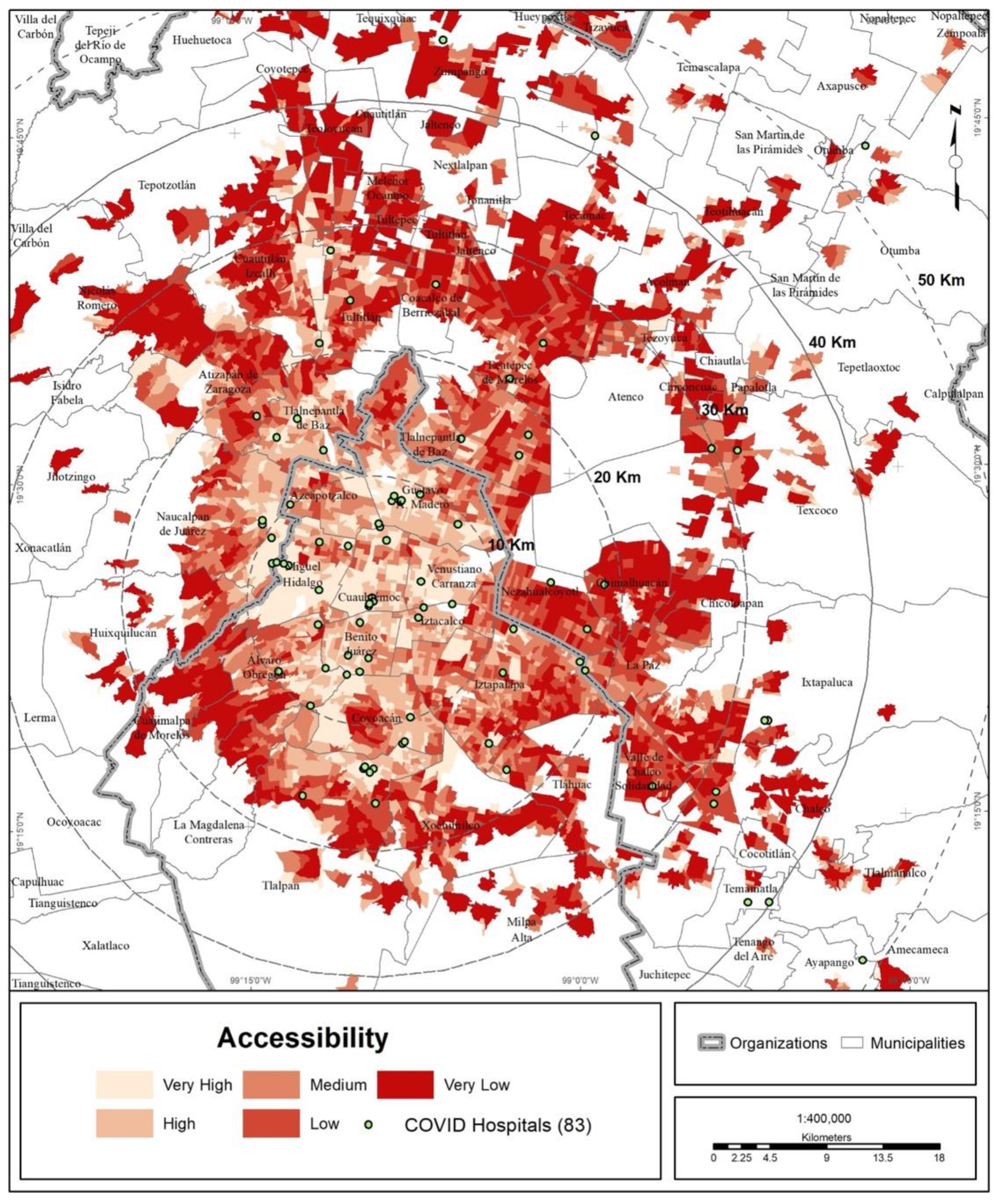
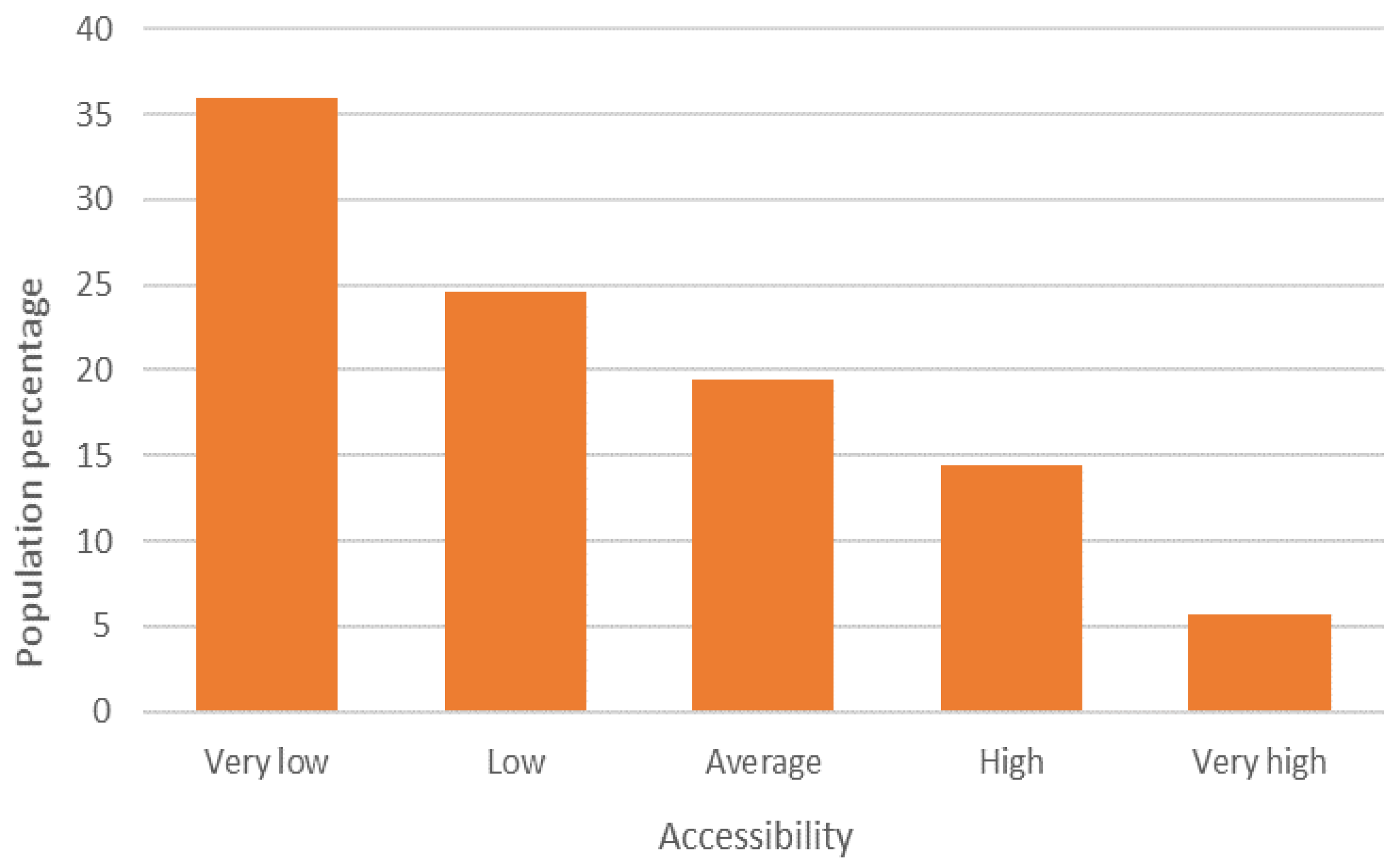
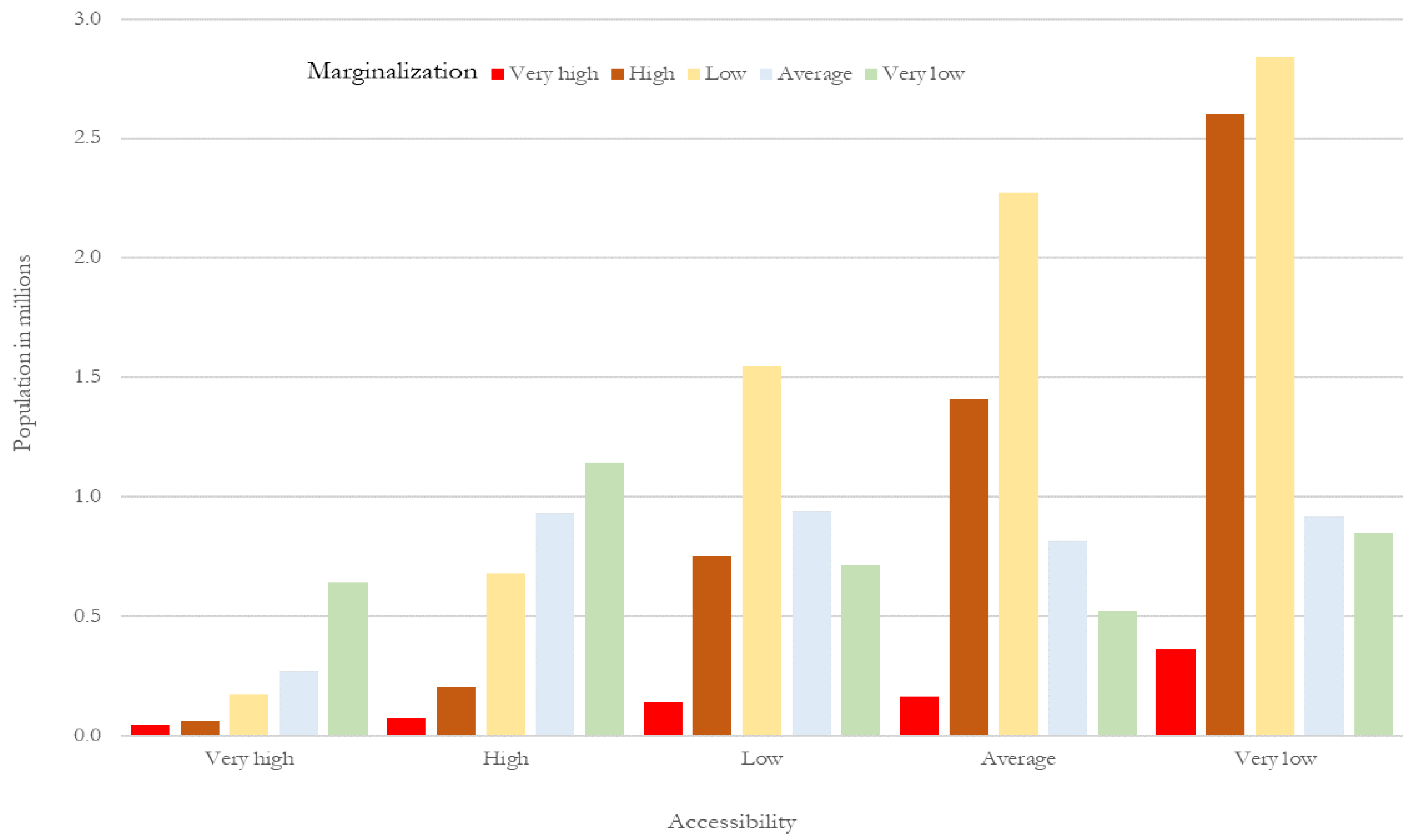
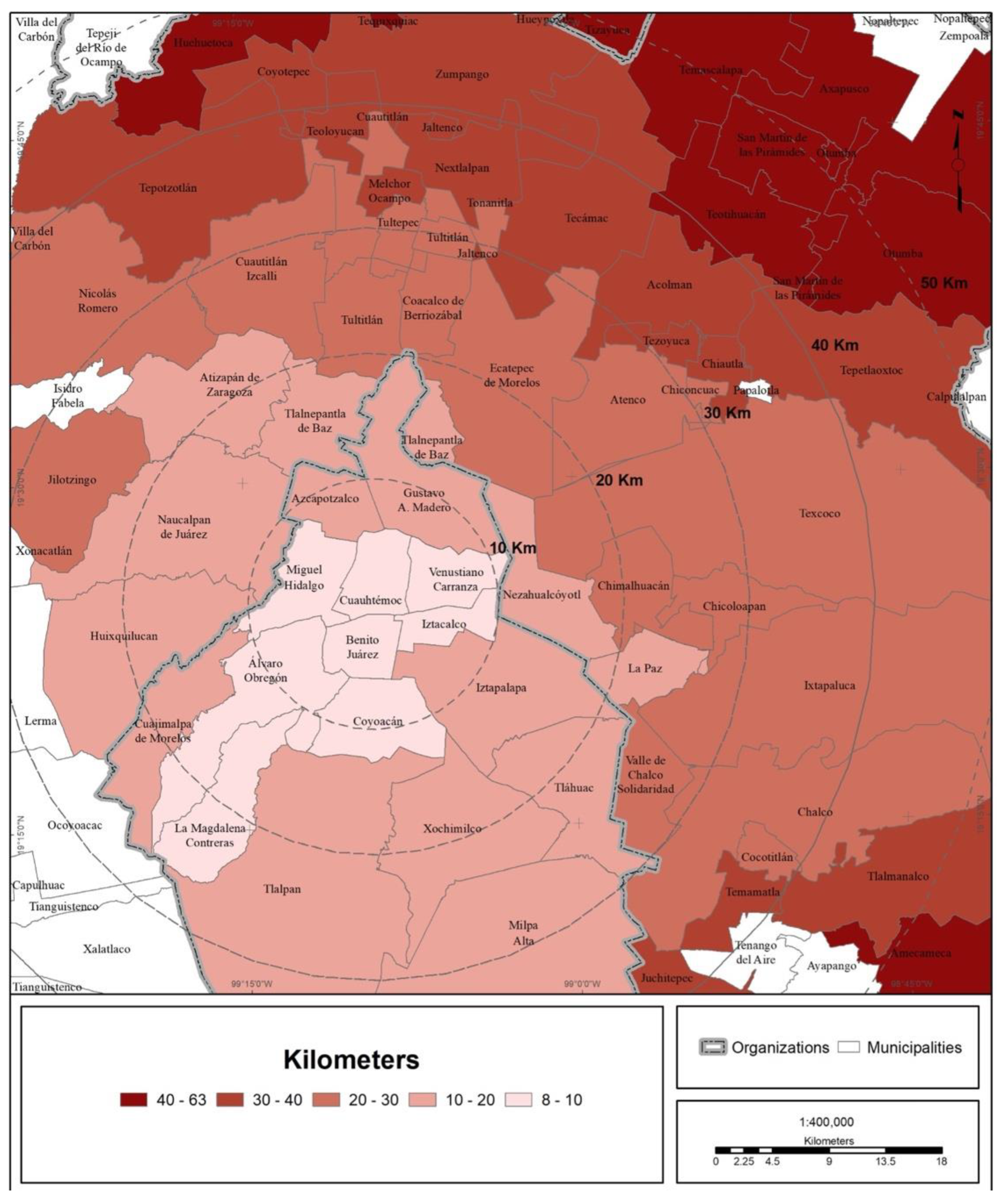
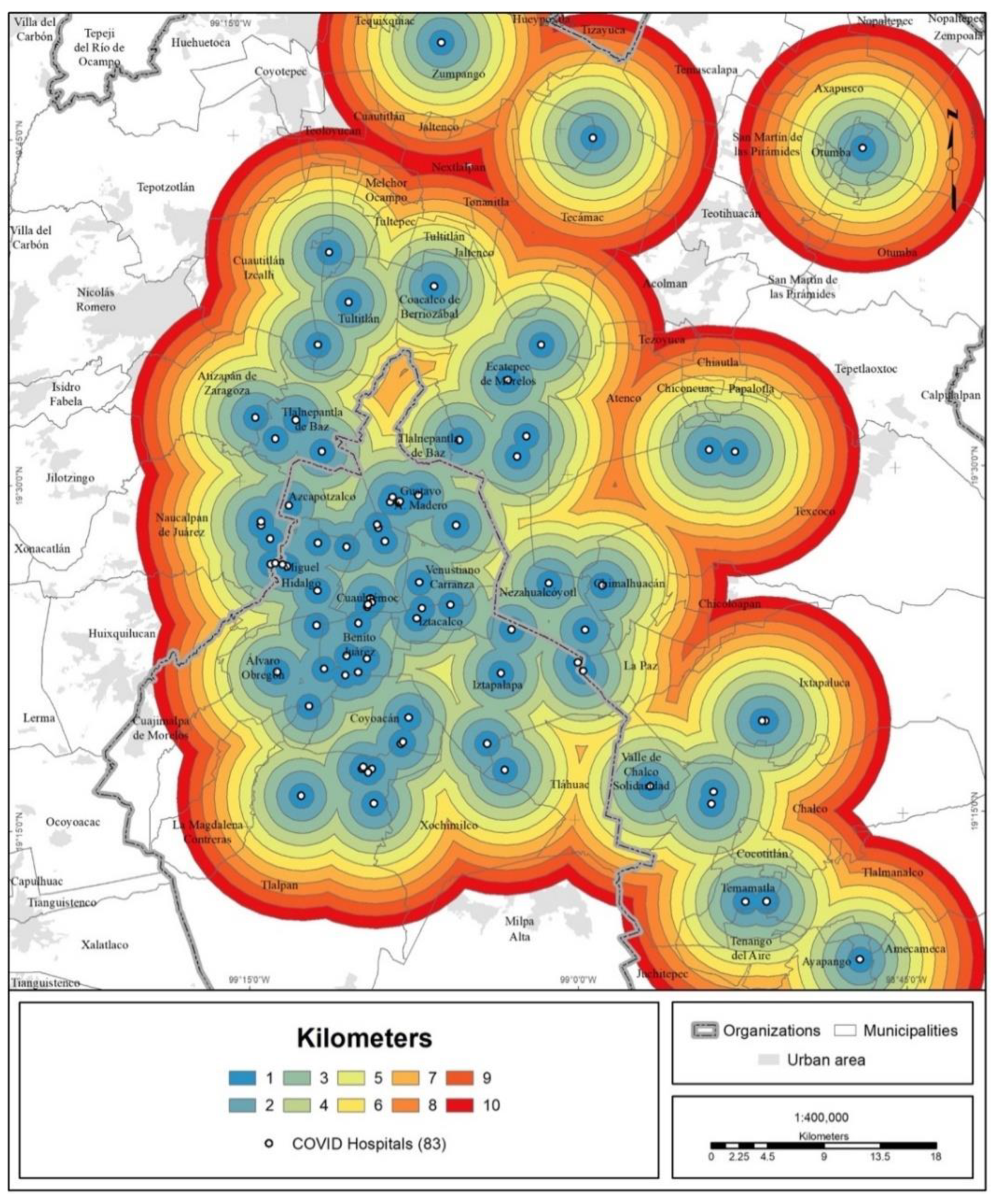
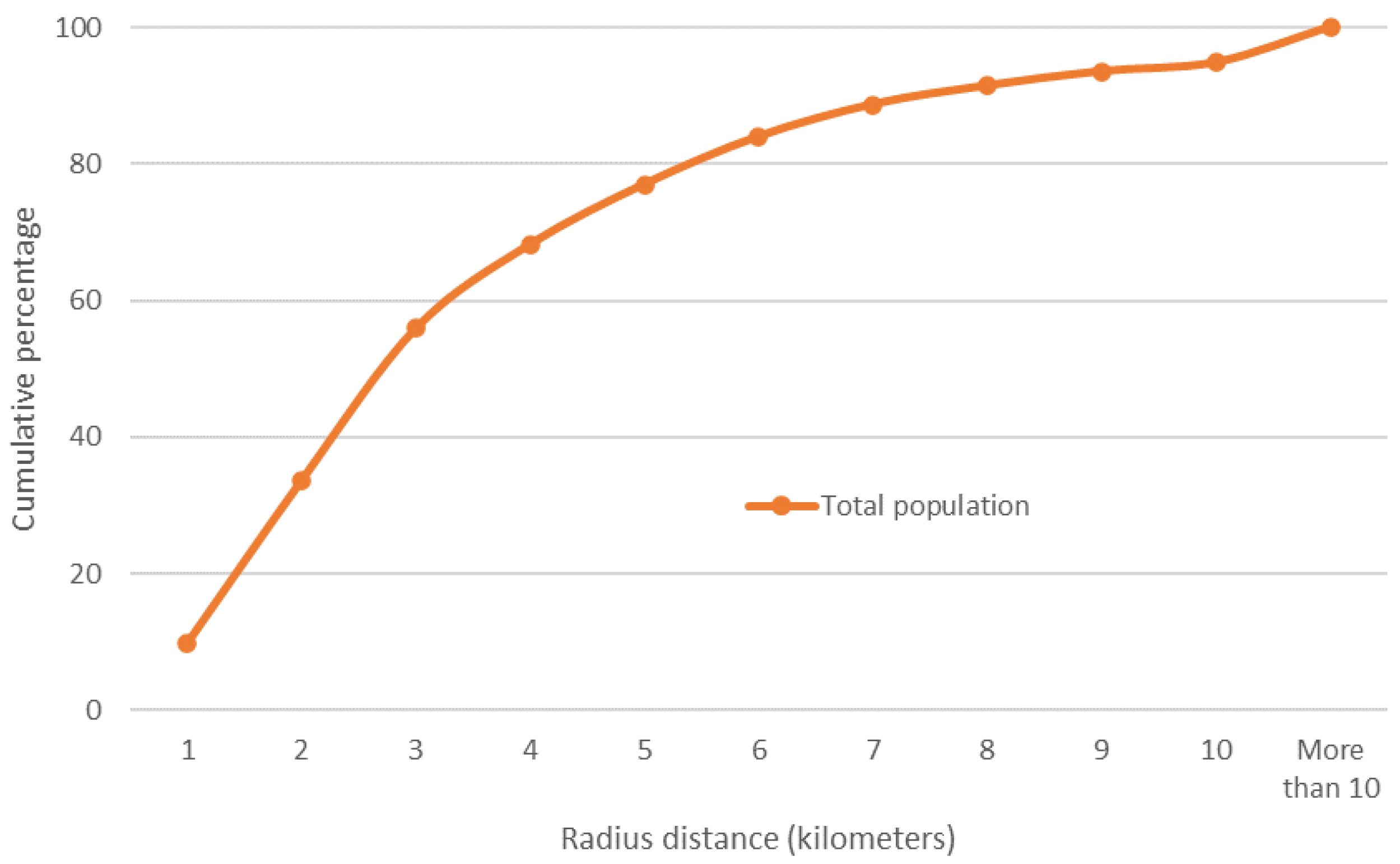
3.4. Accessibility to COVID Hospitals
4. Discussion
4.1. Reflections on the Findings
4.2. Potential of the Analysis and Future Work
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Li, Q.; Guan, X.; Wu, P.; Wang, X.; Zhou, L.; Tong, Y.; Ren, R.; Leung, K.S.M.; Lau, E.H.Y.; Wong, J.Y.; et al. Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia. N. Engl. J. Med. 2020, 382, 1199–1207. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Cai, W.; Watkins, D.; Glanz, J. How the Virus Got Out. The New York Times. Available online: https://www.nytimes.com/interactive/2020/03/22/world/coronavirusspread.html (accessed on 25 March 2020).
- Lutton, L. Coronavirus Case Numbers in the United States: MARCH 31 Update. Medical Economics. Available online: https://www.medicaleconomics.com/view/coronavirus-case-numbers-united-states-march-31-update (accessed on 25 March 2020).
- Jones, S. How Coronavirus Took Just Weeks to Overwhelm Spain. The Guardian. Available online: https://www.theguardian.com/world/2020/mar/25/how-spain-sat-on-its-hands-as-coronavirus-took-hold (accessed on 25 March 2020).
- Megna, R. First month of the epidemic caused by COVID-19 in Italy: Current status and real-time outbreak development forecast. Glob. Health Res. Policy 2020, 5, 43. [Google Scholar] [CrossRef] [PubMed]
- Caul, S. Deaths Involving COVID-19 by Local Area and Socioeconomic Deprivation: Deaths Occurring between 1 March and 31 July 2020; Officer for National Statistics, Statistical Bulletin: UK. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/bulletins/deathsinvolvingcovid19bylocalareasanddeprivation/deathsoccurringbetween1marchand31july2020 (accessed on 30 August 2020).
- Secretaría de Salud. Datos Abiertos. Dirección General de Epidemiología, Secretaría de Salud, México. Available online: https://www.gob.mx/salud/documentos/datos-abiertos-152127 (accessed on 1 May 2020).
- Ribeiro, H.V.; Sunahara, A.S.; Sutton, J.; Perc, M.; Hanley, Q.S. City size and the spreading of COVID-19 in Brazil. PLoS ONE 2020, 15, e0239699. [Google Scholar] [CrossRef]
- Baser, O. Population density index and its use for distribution of COVID-19: A case study using Turkish data. Health Policy 2020, 125, 148–154. [Google Scholar] [CrossRef]
- Hamidi, S.; Sadegh, S.; Ewing, R. Does Density Aggravate the COVID-19 Pandemic? J. Am. Plan. Assoc. 2020, 86, 495–509. [Google Scholar] [CrossRef]
- Coşkun, H.; Yildirim, N.; Gündüz, S. The spread of COVID-19 virus through population density and wind in Turkey cities. Sci. Total Environ. 2021, 751, 141663. [Google Scholar] [CrossRef]
- Secretaría de Salud. Lineamientos de Reconversión Hospitalaria. Secretaría de Salud, México. 2020. Available online: https://coronavirus.gob.mx/wp-content/uploads/2020/04/Documentos-Lineamientos-Reconversion-Hospitalaria.pdf (accessed on 5 April 2020).
- Secretaría de Salud. Municipios de la Esperanza. Secretaría de Salud, México. 2020. Available online: https://coronavirus.gob.mx/wp-content/uploads/2020/05/Municipios_Esperanza_16052020.pdf (accessed on 16 May 2020).
- GobCdMx. Aporta Sedena y Marina 1,577 Camas y Centros de Aislamiento Voluntario Para Atender COVID-19 en la Ciudad de México. Gobierno de Ciudad de México. Available online: https://jefaturadegobierno.cdmx.gob.mx/comunicacion/nota/aporta-sedena-y-marina-1577-camas-y-centros-de-aislamiento-voluntario-para-atender-covid-19-en-la-ciudad-de-mexico (accessed on 4 May 2020).
- Hernández, E. Sheinbaum Inaugura Unidad Temporal de COVID-19. El Universal, México. 2020. Available online: https://www.eluniversal.com.mx/metropoli/cdmx/coronavirus-sheinbaum-inaugura-unidad-temporal-de-covid-19-en-centro-citibanamex (accessed on 22 April 2020).
- GobMex. IMSS Recibe Primeros Pacientes COVID-19 en Hospital de Expansión Autódromo Hermanos Rodríguez. Gobierno de México. Available online: http://www.imss.gob.mx/prensa/archivo/202005/290 (accessed on 14 May 2020).
- GobMex. IMSS Abre Centro de Atención Temporal Lindavista con 40 Camas Para la Ciudad de México. Gobierno de México. Available online: http://www.imss.gob.mx/prensa/archivo/202101/CCO05 (accessed on 28 January 2020).
- Galindo Pérez, C. Localización de los servicios salud y subcentralidad urbana en la Ciudad de México. In Sentido y Formas del Cambio; Molina y Vedia, S.I., Sánchez Almanza, A., Eds.; FCPyS-UNAM: Mexico, 2017; pp. 219–236. Available online: https://www.researchgate.net/publication/325708691_Localizacion_de_los_servicios_salud_y_subcentralidad_urbana_en_la_Ciudad_de_Mexico (accessed on 1 May 2020).
- Infobae. Presentan Iniciativa “Juntos por la Salud” Para Hacer Frente al Coronavirus. Infobae, México. Available online: https://www.infobae.com/america/mexico/2020/04/30/en-vivo-lopez-obrador-presenta-nueva-proyeccion-para-el-coronavirus-en-mexico/ (accessed on 30 April 2020).
- Secretaría de Salud. 105. Sector Salud Suscribe Convenio Con Hospitales Privados Para Hacer Frente a la Pandemia de COVID-19. Secretaría de Salud, México. Available online: https://www.gob.mx/salud/prensa/105-sector-salud-suscribe-convenio-con-hospitales-privados-para-hacer-frente-a-la-pandemia-de-covid-19 (accessed on 13 April 2020).
- Suárez Lastra, M.; Valdés González, C.M.; Galindo Pérez, M.C.; Salvador Guzmán, L.E.; Ruiz-Rivera, N.; Alcántara-Ayala, I.; López-Cervantes, M.; Rosales Tapia, A.R.; Lee, W.H.; Benítez-Pérez, H.; et al. An index of vulnerability to COVID-19 in Mexico. Investig. Geográficas 2021, 104, e60140. [Google Scholar] [CrossRef]
- Lima, F.T.; Brown, N.C.; Duarte, J.P. Understanding the Impact of Walkability, Population Density, and Population Size on COVID-19 Spread: A Pilot Study of the Early Contagion in the United States. Entropy 2021, 23, 1512. [Google Scholar] [CrossRef]
- Cole, H.V.S.; Anguelovski, I.; Baró, F.; García-Lamarca, M.; Kotsila, P.; Pérez del Pulgar, C.; Shokry, G.; Triguero-Mas, M. The COVID-19 pandemic: Power and privilege, gentrification, and urban environmental justice in the global north. Cities Health 2020, 1–5. [Google Scholar] [CrossRef]
- Cave, B.; Kim, J.; Viliani, F.; Harris, P. Applying an equity lens to urban policy measures for COVID-19 in four cities. Cities Health 2020, 1–5. [Google Scholar] [CrossRef]
- Tampe, T. Potential impacts of COVID-19 in urban slums: Addressing challenges to protect the world’s most vulnerable. Cities Health 2020, 1–4. [Google Scholar] [CrossRef]
- Galindo Pérez, C.; Suárez Lastra, M. Health Services of ISSSTE in the Mexico City’s Metropolitan Area ¿What if we all Get Sick? Gestión Política Pública 2018, 27, 475–499. Available online: http://www.gestionypoliticapublica.cide.edu/ojscide/index.php/gypp/article/view/479/127 (accessed on 1 May 2020).
- Sedatu-Conapo-INEGI. Delimitación de Zonas Metropolitanas de México 2015. Sedatu-Conapo-INEGI, México. Available online: https://www.gob.mx/conapo/documentos/delimitacion-de-las-zonas-metropolitanas-de-mexico-2015 (accessed on 30 April 2020).
- INEGI. Censo de Población y Vivienda 2020. Instituto Nacional de Estadística y Geografía, México. Available online: https://www.inegi.org.mx/programas/ccpv/2020/ (accessed on 30 April 2020).
- Kara, F.; Egresi, I. Accessibility of Health Care Institutions: A Case Study by Using GIS. Int. J. Sci. Knowl. 2013, 3, 16–27. [Google Scholar]
- Love, D.; Lindquist, P. The Geographical Accessibility of Hospitals to the Aged: A Geographic Information Systems Analysis within Illinois. Health Serv. Res. 1995, 29, 629–651. [Google Scholar]
- Baazeem, M.; Tennant, M.; Kruger, E. Determining Variations in Access to Public Hospitals in Makkah, Kingdom of Saudi Arabia: A GIS-Based Approach. Saudi J. Health Syst. Res. 2021, 1, 26–32. [Google Scholar] [CrossRef]
- Cervero, R.; Rood, T.; Appleyard, B. Job Accessibility as a Performance Indicator: An Analysis of Trends and Their Social Policy Implications in the San Francisco Bay Area. IURD-UCTC. Work. Pap. 1995, 366, 1–32. Available online: https://escholarship.org/uc/item/6mp941d9 (accessed on 1 May 2020).
- Cervero, R.; Rood, T.; Appleyard, B. Tracking Accessibility: Employment and Housing Opportunities in the San Francisco Bay Area. Environ. Plan. A 1999, 31, 1259–1278. Available online: https://journals.sagepub.com/doi/pdf/10.1068/a311259 (accessed on 4 May 2020). [CrossRef]
- Kang, J.Y.; Michels, A.; Lyu, F.; Wang, S.; Agbodo, N.; Freeman, V.L.; Wang, S. Rapidly measuring spatial accessibility of COVID-19 healthcare resources: A case study of Illinois, USA. Int. J. Health Geogr. 2020, 19, 36. [Google Scholar] [CrossRef]
- Hansen, W.G. How accessibility shapes land use. J. Am. Inst. Plan. 1959, 25, 73–76. [Google Scholar] [CrossRef]
- Morris, J.M.; Dumble, P.L.; Wigan, M.R. Accessibility indicators for transport planning. Transp. Rev. 1979, 13A, 91–109. [Google Scholar] [CrossRef]
- Geurs, K.T.; Van Wee, B. Accessibility evaluation of land-use and transport strategies: Review and research directions. J. Transp. Geogr. 2004, 12, 127–140. [Google Scholar] [CrossRef]
- Gao, F.; Kihal, W.; Le Meur, N.; Souris, M.; Deguen, S. Does the Edge effect impact on the measure of spatial accessibility to healthcare providers? Int. J. Health Geogr. 2017, 16, 46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guagliardo, M.F. Spatial accessibility of primary care: Concepts, methods and challenges. Int. J. Health Geogr. 2004, 3, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guagliardo, M.F.; Ronzio, C.R.; Cheung, I.; Chacko, E.; Joseph, J.G. Physician accessibility: An urban case study of pediatric providers. Health Place 2004, 10, 273–283. [Google Scholar] [CrossRef]
- Pearce, J.; Witten, K.; Bartie, P. Neighbourhoods and health: A GIS approach to measuring community resource accessibility. J. Epidemiol. Community Health 2006, 60, 389–395. [Google Scholar] [CrossRef] [Green Version]
- Conapo. Índice de Marginación Urbana 2010. Consejo Nacional de Población, México. Available online: http://www.conapo.gob.mx/es/CONAPO/Capitulo_1_Marginacion_Urbana_2010 (accessed on 30 April 2020).
- Álvarez, E. Colonias del Sur en la CDMX, de las Más Vulnerables al COVID-19. Forbes México. Available online: https://www.forbes.com.mx/noticias-colonias-sur-cdmx-vulnerables-covid19/ (accessed on 7 August 2020).
- Aday, L.A.; Andersen, R. A Framework for the Study of Access to Medical Care. Health Serv. Res. 1974, 9, 208–220. [Google Scholar] [PubMed]
- Penchansky, R.; Thomas, W. The concept of access. Definition and relationship to consumer satisfaction. Med. Care 1981, 29, 127–140. [Google Scholar] [CrossRef] [PubMed]
- Pereira, R.H.M.; Braga, C.K.V.; Servo, L.M.; Serra, B.; Amaral, P.; Gouveia, N. Mobilidade urbana e o acesso ao Sistema Único de Saúde para casos suspeitos e graves de COVID-19 nas 20 maiores cidades do Brasil. Nota Técnica 14, Instituto de Pesquisa Econômica Aplicada 2020. Available online: https://www.ipea.gov.br/portal/index.php?option=com_content&view=article&id=35442&Itemid=7 (accessed on 4 May 2020).
- Verhagen, M.D.; Brazel, D.M.; Dowd, J.B.; Kashnitsky, I.; Mills, M. March 21, Forecasting spatial, socioeconomic and demographic variation in COVID-19 health care demand in England and Wales. BMC Med. 2020, 18, 203. [Google Scholar] [CrossRef]
- Tavares, F.F.; Betti, G. The pandemic of poverty, vulnerability, and COVID-19: Evidence from a fuzzy multidimensional analysis of deprivations in Brazil. World Dev. 2021, 139, 105307. [Google Scholar] [CrossRef]
- Ramírez, I.J.; Lee, J. COVID-19 emergence and social and health determinants in Colorado: A rapid spatial analysis. Int. J. Environ. Res. Public Health 2020, 17, 3856. Available online: https://doi.org/10.3390/ijerph17113856 (accessed on 1 May 2020). [CrossRef]
- Reyes-Vega, M.F.; Soto-Cabezas, M.G.; Cárdenas, F.; Martel, K.S.; Valle, A.; Valverde, J.; Vidal-Anzardo, M.; Falcón, M.E.; Munayco, C.V. SARS-CoV-2 prevalence associated to low socioeconomic status and overcrowding in an LMIC megacity: A population-based seroepidemiological survey in Lima, Peru. EClinicalMedicine 2021, 34, 100801. [Google Scholar] [CrossRef] [PubMed]
- Sánchez Salazar, M.T.; Suárez Lastra, M. Zona Metropolitana de la Ciudad de México. In Atlas de Vulnerabilidad Urbana ante COVID-19 en las Zonas Metropolitanas de México; Suárez-Lastra, M., Galindo-Pérez, M.C., Salvador-Guzmán, L.E., Rosales-Tapia, A.R., Ruiz-Rivera, N., Alcántara-Ayala, I., Oropeza-Orozco, O., López-Cervantes, M., Sánchez-Salazar, M.T., Juárez-Gutiérrez, M.C., et al., Eds.; Instituto de Geografía, UNAM: Mexico, 2020; Available online: http://www.igg.unam.mx/covid-19/Vista/archivos/atlas/ZMValleMexico.pdf (accessed on 28 November 2020).
- Antonio-Villa, N.E.; Fernandez-Chirino, L.; Pisanty-Alatorre, J.; Mancilla-Galindo, J.; Kammar-García, A.; Vargas-Vázquez, A.; González-Díaz, A.; Fermín-Martínez, C.A.; Márquez-Salinas, A.; Guerra, E.C.; et al. Comprehensive evaluation of the impact of sociodemographic inequalities on adverse outcomes and excess mortality during the COVID-19 pandemic in Mexico City. medRxiv 2021. [Google Scholar] [CrossRef]
- Pengjun, Z.; Shengxiao, L.; Liu, D. Unequable spatial accessibility to hospitals in developing megacities: New evidence from Beijing. Health Place 2020, 65, 102406. [Google Scholar] [CrossRef]
- Karatas, M.; Yakici, E. An analysis of p-median location problem: Effects of backup service level and demand assignment policy. Eur. J. Oper. Res. 2019, 272, 207–218. [Google Scholar] [CrossRef]
- Daskin, M.S.; Stern, E.H. A Hierarchical Objective Set Covering Model for Emergency Medical Service Vehicle Deployment. Transp. Sci. 1981, 15, 137–152. [Google Scholar] [CrossRef]
- Pirkul, H.; Schilling, D.A. The Siting of Emergency Service Facilities with Workload Capacities and Backup Service. Manag. Sci. 1988, 34, 896–908. [Google Scholar] [CrossRef]
- Jánošíková, L.; Gábrišová, L.; Ježek, B. Load balancing location of emergency medical service stations. E+M Ekon. Manag. 2015, 18, 30–41. Available online: https://dspace.tul.cz/handle/15240/13239 (accessed on 4 May 2020). [CrossRef]
- Stettin, C. CDMX crea Hospital Virtual para Disminuir Ocupación por COVID-19. Milenio Diario, México. Available online: https://www.milenio.com/ciencia-y-salud/cdmx-crea-hospital-virtual-disminuir-ocupacion-covid-19 (accessed on 11 February 2021).



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Institution | Hospitals | Beds |
|---|---|---|
| IMSS | 30 | 6002 |
| Ssa | 7 | 2050 |
| ISSSTE | 9 | 2044 |
| Sedena | 8 | 1448 |
| Semar | 1 | 140 |
| Sedesa | 8 | 984 |
| ISEM | 16 | 1820 |
| ISSEMyM | 1 | 107 |
| Temporary centers | 3 | 865 |
| Total | 83 | 15,460 |
| Estimate | Std. Error | t Value | Pr (>|t|) | |
|---|---|---|---|---|
| (Intercept) | 5.533308 | 0.841046 | 6.579 | 6.54 × 10−9 *** |
| (NL) Days elapsed between the metropolitan index case and the first case in the municipality | −0.643523 | 0.16859 | −3.817 | 0.000283 *** |
| Road distance to the metropolitan center (km) | −0.037074 | 0.011311 | −3.278 | 0.001613 ** |
| Urban population density (population/Ha) | 0.016093 | 0.004587 | 3.509 | 0.000781 *** |
| Institution | Cases | |
|---|---|---|
| Total | % | |
| Ssa and Sedesa | 13,878 | 56.6 |
| IMSS | 6878 | 28 |
| Private institutions | 2108 | 8.6 |
| ISSSTE | 1056 | 4.3 |
| Pemex | 237 | 1 |
| Semar | 226 | 0.9 |
| Sedena | 115 | 0.5 |
| ISSEMyM | 16 | 0.1 |
| Red Cross | 5 | 0.02 |
| IMSS-Opportunities | 3 | 0.01 |
| Other | 1 | 0.004 |
| Total | 24,523 | 100 |
| Institution | Average Distance Traveled (Linear Kilometers) |
|---|---|
| Ssa and Sedesa | 16.7 |
| IMSS | 14.7 |
| ISSSTE | 14.2 |
| ISEM | 19.7 |
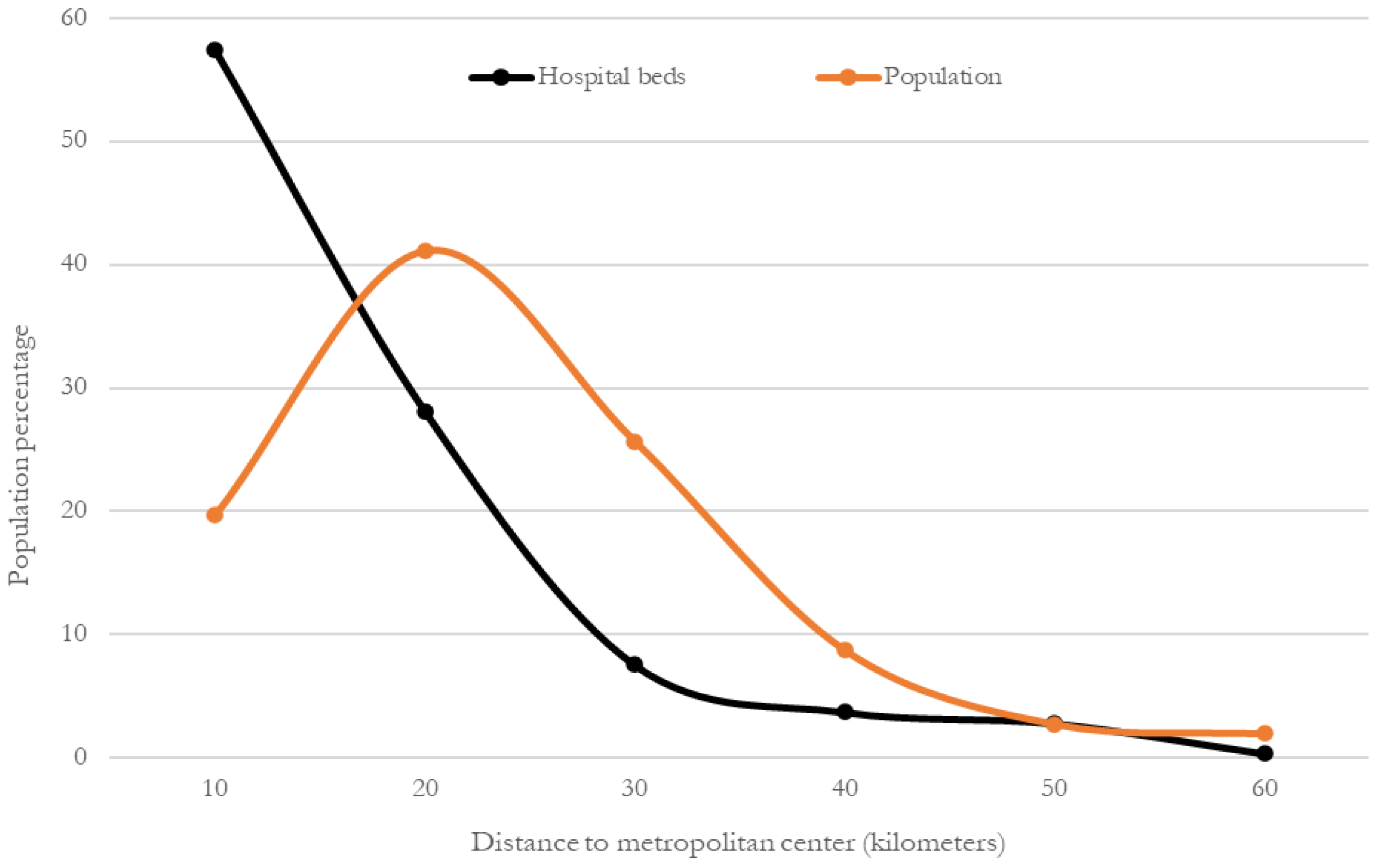
| Radius (Kilometers) | Total Hospitals | Hospital Beds | 2020 Population | ||
|---|---|---|---|---|---|
| Total | % | Total | % | ||
| 10 | 36 | 8869 | 57.4 | 4,100,074 | 19.7 |
| 20 | 28 | 4345 | 28.1 | 8,545,588 | 41.1 |
| 30 | 8 | 1170 | 7.6 | 5,339,309 | 25.7 |
| 40 | 7 | 578 | 3.7 | 1,823,406 | 8.8 |
| 50 | 3 | 438 | 2.8 | 575,747 | 2.8 |
| 60 | 1 | 60 | 0.4 | 409,742 | 2 |
| Total | 83 | 15,460 | 100 | 21,088,201 | 100 |
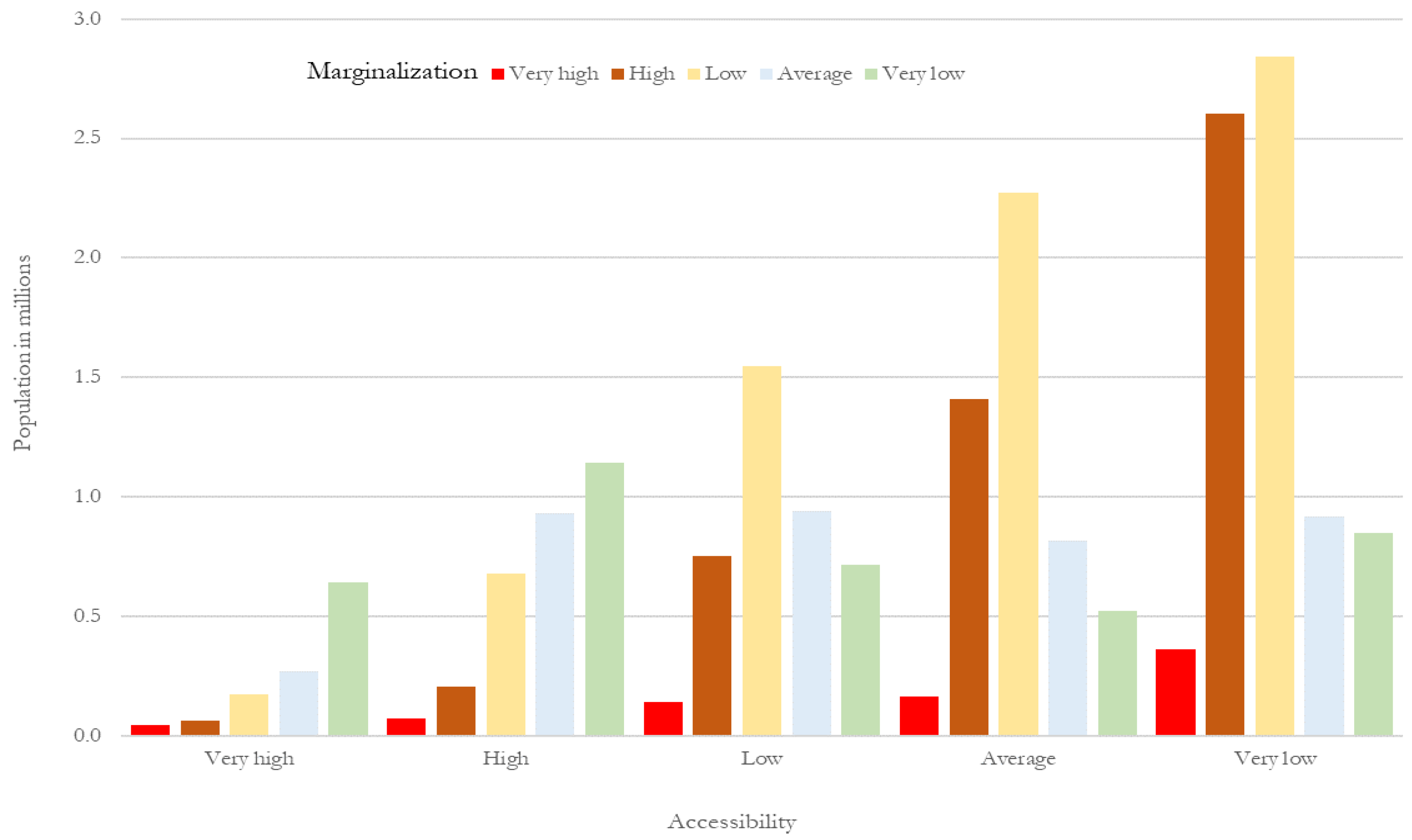
| Marginalization | |||||||
|---|---|---|---|---|---|---|---|
| Very High | High | Average | Low | Very Low | Total | ||
| Accessibility (frequency) | Very high | 42,557 | 64,271 | 174,556 | 270,705 | 641,583 | 1,193,672 |
| High | 71,191 | 207,516 | 679,357 | 931,892 | 1,144,483 | 3,034,437 | |
| Average | 140,828 | 752,870 | 1,549,083 | 941,651 | 716,434 | 4,100,866 | |
| Low | 163,767 | 1,407,775 | 2,272,995 | 816,578 | 521,055 | 5,182,168 | |
| Very low | 360,166 | 2,605,597 | 2,842,277 | 918,298 | 850,719 | 7,577,058 | |
| Total | 778,508 | 5,038,028 | 7,518,267 | 3,879,123 | 3,874,273 | 21,088,201 | |
| Very high | High | Average | Low | Very low | Total | ||
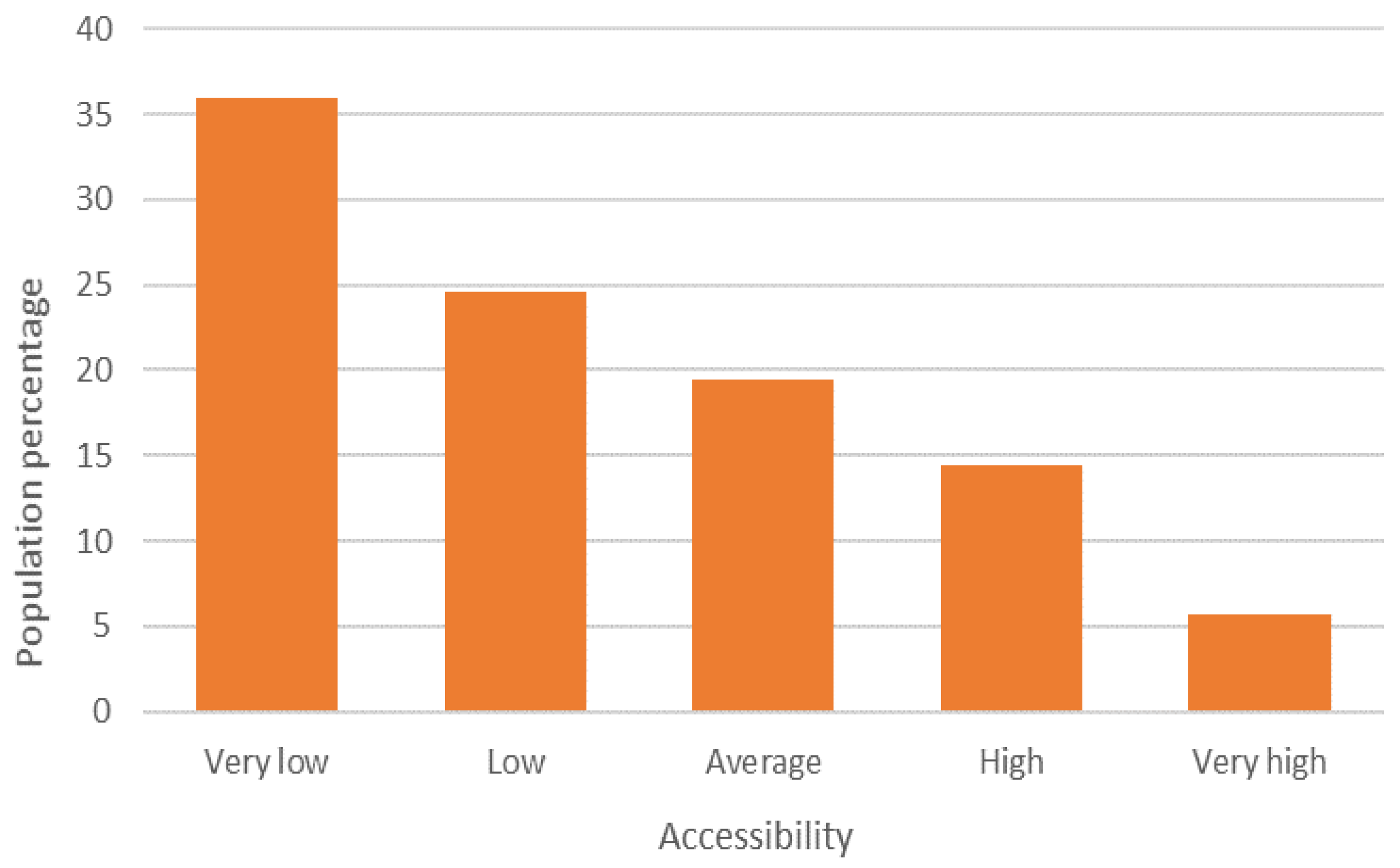
| Accessibility (percentage) | Very high | 5.5 | 1.3 | 2.3 | 7 | 16.6 | 5.7 |
| High | 9.1 | 4.1 | 9 | 24 | 29.5 | 14.4 | |
| Average | 18.1 | 14.9 | 20.6 | 24.3 | 18.5 | 19.4 | |
| Low | 21 | 27.9 | 30.2 | 21.1 | 13.4 | 24.6 | |
| Very low | 46.3 | 51.7 | 37.8 | 23.7 | 22 | 35.9 | |
| Total | 100 | 100 | 100 | 100 | 100 | 100 | |
| Range | Average Distance in Kilometers | |||
|---|---|---|---|---|
| To the Nearest COVID Hospital | To the Urban Health Sub Center | |||
| Accessibility | Marginalization | Accessibility | Marginalization | |
| Very high | 3.7 | 7.5 | 18.5 | 32.6 |
| High | 3.1 | 5.6 | 16.4 | 27.2 |
| Average | 3.8 | 3.7 | 19.7 | 19.4 |
| Low | 4.3 | 2.9 | 23 | 16.3 |
| Very low | 5.8 | 2.3 | 28.5 | 13 |
| Estimate | Std. Error | t Value | Pr (>|t|) | |
|---|---|---|---|---|
| (Intercept) | 2.26736 | 1.71959 | 1.319 | 0.191619 |
| Urban marginalization index | −2.27127 | 0.48127 | −4.719 | 1.18 × 10−5 *** |
| % population with some disability | 0.82066 | 0.2287 | 3.588 | 0.000613 *** |
| % economically dependent population | −0.98423 | 0.32194 | −3.057 | 0.003162 ** |
| Road distance to the metropolitan center (kms) | −0.07428 | 0.01187 | −6.259 | 2.72 × 10−5 *** |
| COVID hospital accessibility index | −1.78524 | 1.06106 | −1.683 | 0.096923. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Galindo-Pérez, M.C.; Suárez, M.; Rosales-Tapia, A.R.; Sifuentes-Osornio, J.; Angulo-Guerrero, O.; Benítez-Pérez, H.; de Anda-Jauregui, G.; Díaz-de-León-Santiago, J.L.; Hernández-Lemus, E.; Alonso Herrera, L.; et al. Territorial Strategy of Medical Units for Addressing the First Wave of the COVID-19 Pandemic in the Metropolitan Area of Mexico City: Analysis of Mobility, Accessibility and Marginalization. Int. J. Environ. Res. Public Health 2022, 19, 665. https://doi.org/10.3390/ijerph19020665
Galindo-Pérez MC, Suárez M, Rosales-Tapia AR, Sifuentes-Osornio J, Angulo-Guerrero O, Benítez-Pérez H, de Anda-Jauregui G, Díaz-de-León-Santiago JL, Hernández-Lemus E, Alonso Herrera L, et al. Territorial Strategy of Medical Units for Addressing the First Wave of the COVID-19 Pandemic in the Metropolitan Area of Mexico City: Analysis of Mobility, Accessibility and Marginalization. International Journal of Environmental Research and Public Health. 2022; 19(2):665. https://doi.org/10.3390/ijerph19020665
Chicago/Turabian StyleGalindo-Pérez, Mateo Carlos, Manuel Suárez, Ana Rosa Rosales-Tapia, José Sifuentes-Osornio, Ofelia Angulo-Guerrero, Héctor Benítez-Pérez, Guillermo de Anda-Jauregui, Juan Luis Díaz-de-León-Santiago, Enrique Hernández-Lemus, Luis Alonso Herrera, and et al. 2022. "Territorial Strategy of Medical Units for Addressing the First Wave of the COVID-19 Pandemic in the Metropolitan Area of Mexico City: Analysis of Mobility, Accessibility and Marginalization" International Journal of Environmental Research and Public Health 19, no. 2: 665. https://doi.org/10.3390/ijerph19020665
APA StyleGalindo-Pérez, M. C., Suárez, M., Rosales-Tapia, A. R., Sifuentes-Osornio, J., Angulo-Guerrero, O., Benítez-Pérez, H., de Anda-Jauregui, G., Díaz-de-León-Santiago, J. L., Hernández-Lemus, E., Alonso Herrera, L., López-Arellano, O., Revuelta-Herrera, A., Ruiz-Gutiérrez, R., Sheinbaum-Pardo, C., & Kershenobich-Stalnikowitz, D. (2022). Territorial Strategy of Medical Units for Addressing the First Wave of the COVID-19 Pandemic in the Metropolitan Area of Mexico City: Analysis of Mobility, Accessibility and Marginalization. International Journal of Environmental Research and Public Health, 19(2), 665. https://doi.org/10.3390/ijerph19020665