
The Sexual and Parenting Rights of People with Physical and Psychical Disabilities: Attitudes of Italians and Socio-Demographic Factors Involved in Recognition and Denial

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion/Exclusion Criteria for Study Participants
2.2. Study Design and General Description
2.3. Specific Contents of the Questionnaire
2.4. Data Collection
2.5. Statistical Analyses
3. Results
3.1. Descriptives
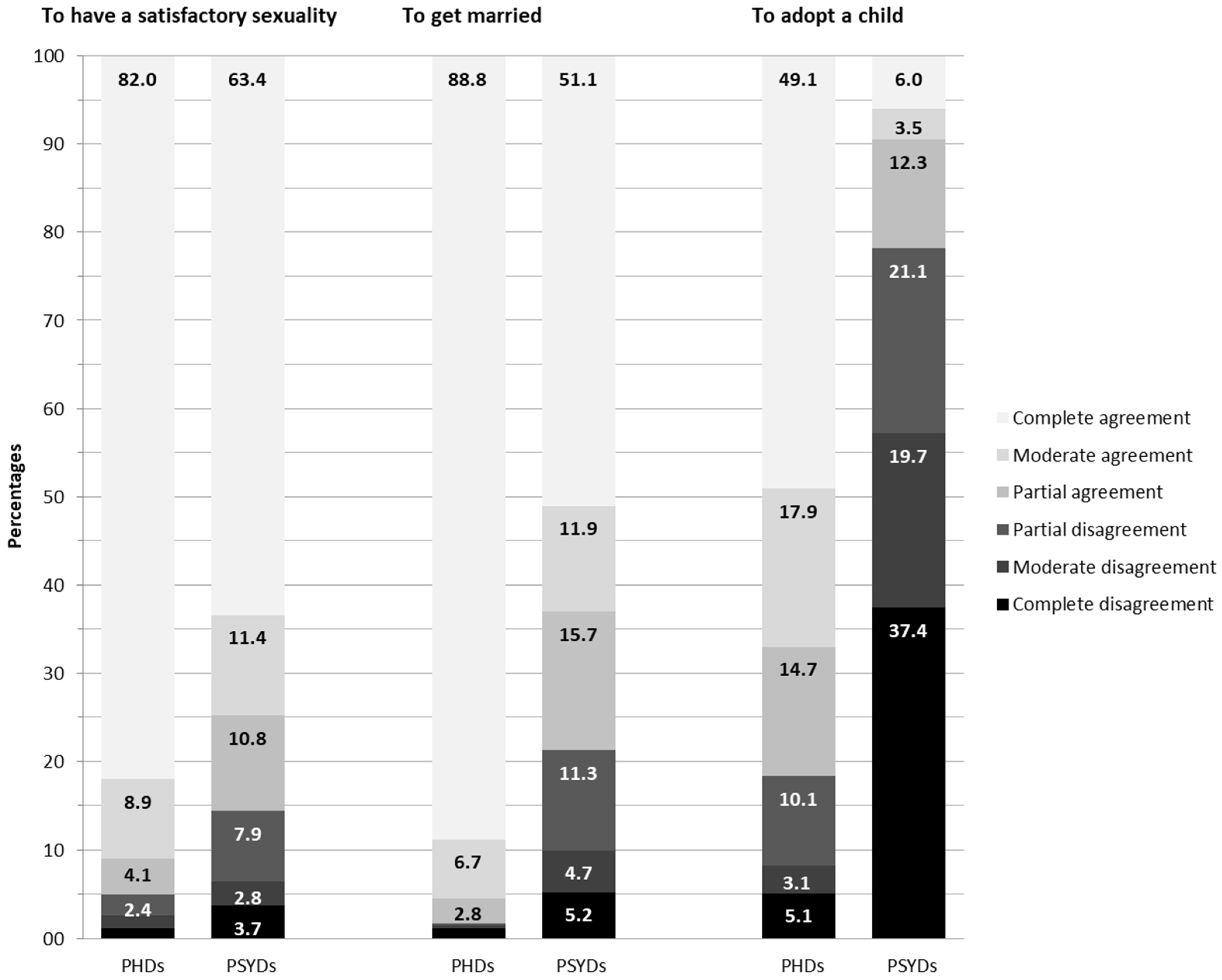
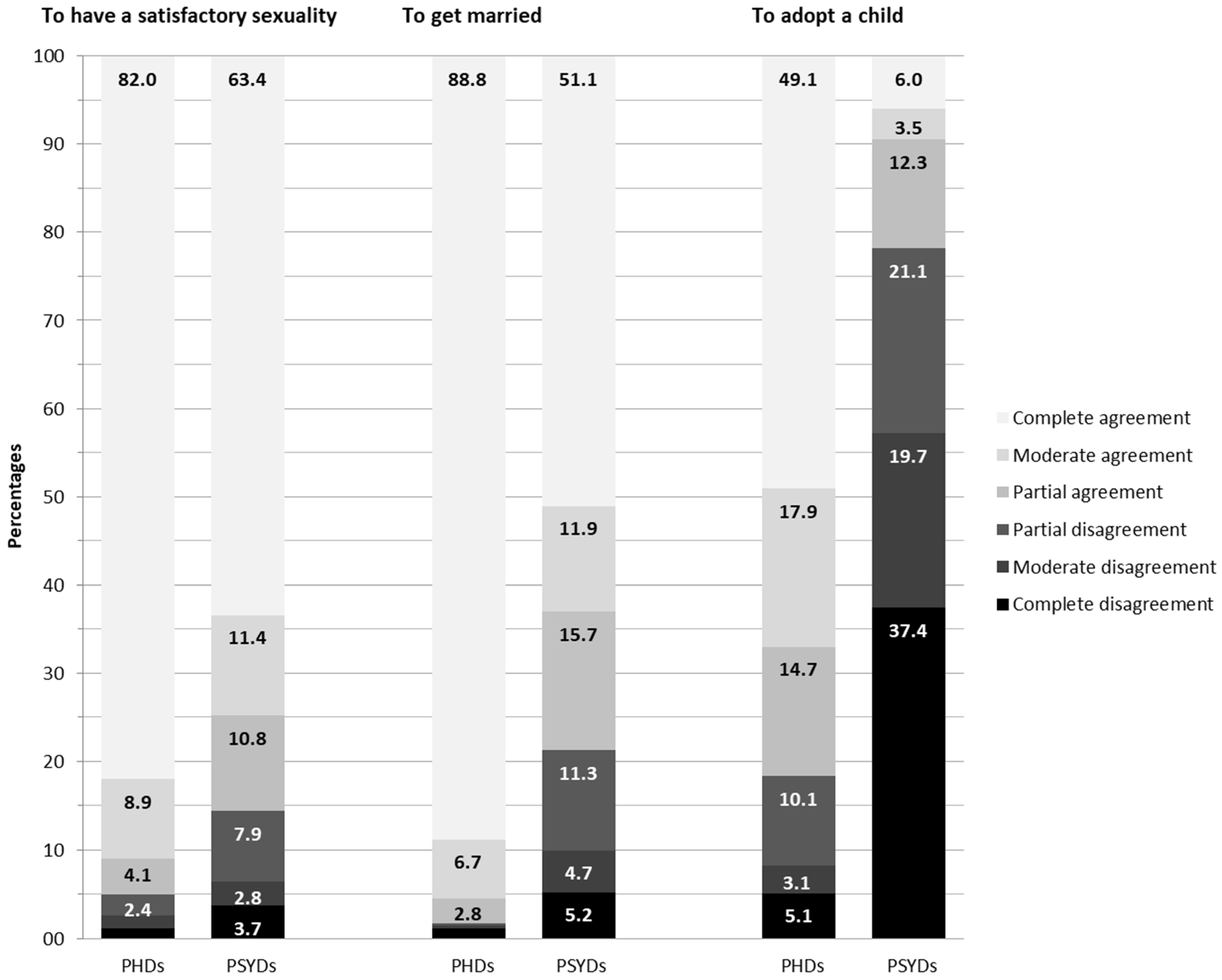
3.2. The Right of PwPHDs and PwPSYDs to Have Satisfactory Sexuality
3.2.1. Percentages of Agreement and Comparison between PwPHDs and PwPSYDs
3.2.2. Socio-Demographic Variables Associated with Agreement with PwPHDs’s Right to Have Satisfactory Sexuality
3.2.3. Socio-Demographic Variables Associated with Agreement with PwPSYDs’s Right to Have Satisfactory Sexuality
3.3. The Right of PwPHDs and PwPSYDs to Get Married
3.3.1. Percentages of Agreement and Comparison between PwPHDs and PwPSYDs
3.3.2. Socio-Demographic Variables Associated with Agreement with PwPHDs’s Right to Get Married
3.3.3. Socio-Demographic Variables Associated with Agreement with PwPSYDs’s Right to Get Married
3.4. The Right of PwPHDs and PwPSYDs to Adopt a Child
3.4.1. Percentages of Agreement and Comparison between PwPHDs and PwPSYDs
3.4.2. Socio-Demographic Variables Associated with Agreement with PwPHDs’s Right to Adopt a Child
3.4.3. Socio-Demographic Variables Associated with Agreement with PwPSYDs’s Right to Adopt a Child
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Carroll, A. World report on disability. Ir. Med. J. 2012, 105, 290. [Google Scholar] [CrossRef]
- United Nations. Convention on the Rights of Persons with Disabilities and Optional Protocol. 2006. Available online: https://www.un.org/disabilities/documents/convention/convoptprot-e.pdf (accessed on 28 September 2021).
- Devkota, H.R.; Kett, M.; Groce, N. Societal attitude and behaviours towards women with disabilities in rural Nepal: Pregnancy, childbirth and motherhood. BMC Pregnancy Childbirth 2019, 19, 20. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Sexual Health, Human Rights and the Law. 2015. Available online: https://apps.who.int/iris/bitstream/handle/10665/175556/9789241564984_eng.pdf (accessed on 28 September 2021).
- Brodwin, M.G.; Frederick, P.C. Sexuality and societal beliefs regarding persons living with disabilities. J. Rehabil. 2010, 76, 37–41. [Google Scholar]
- Stone, S.D. The Myth of Bodily Perfection. Disabil. Soc. 1995, 10, 413–424. [Google Scholar] [CrossRef]
- Shakespeare, T.; Gillespie-Sells, K.; Davies, D. The Sexual Politics of Disability: Untold Desires; Ed Cassell: London, UK, 1996; pp. 16–43. [Google Scholar]
- Milligan, M.S.; Neufeldt, A.H. The myth of asexuality: A survey of social and empirical evidence. Sex. Disabil. 2001, 19, 91–109. [Google Scholar] [CrossRef]
- Ganle, J.K.; Baatiema, L.; Quansah, R.; Danso-Appiah, A. Barriers facing persons with disability in accessing sexual and reproductive health services in sub-Saharan Africa: A systematic review. PLoS ONE 2020, 15, e0238585. [Google Scholar] [CrossRef]
- Addlakha, R.; Price, J.; Heidari, S. Disability and sexuality: Claiming sexual and reproductive rights. Reprod. Health Matters 2017, 25, 4–9. [Google Scholar] [CrossRef] [Green Version]
- Hasson-Ohayon, I.; Hertz, I.; Vilchinsky, N.; Kravetz, S. Attitudes toward the sexuality of persons with physical versus psychiatric disabilities. Rehabil. Psychol. 2014, 59, 236–241. [Google Scholar] [CrossRef] [PubMed]
- McGuire, B.E.; Bayley, A.A. Relationships, sexuality and decision-making capacity in people with an intellectual disability. Curr. Opin. Psychiatry 2011, 24, 398–402. [Google Scholar] [CrossRef] [PubMed]
- Price, J. The Seeds of a Movement—Disabled Women and their Struggle to Organize. In Changing Their World, 2nd ed.; Batliwala, S., Ed.; Association for Women’s Rights in Development: Toronto, ON, Canada, 2011; pp. 1–15. Available online: https://www.awid.org/sites/default/files/atoms/files/changing_their_world_2_-_disabled_women_and_their_struggle_to_organize.pdf (accessed on 28 September 2021).
- Giami, A.; Humbert, C.; Laval, D. L’ange et la bête: Représentations de la Sexualité des Handicapés Mentaux chez Les Parents et Les Éducateurs; Editions de CTNERHI: Paris, France, 1983. [Google Scholar]
- Ditchman, N.; Kosyluk, K.; Lee, E.J.; Jones, N. How Stigma Affects the Lives of People with Intellectual Disabilities: An Overview. In Intellectual Disability and Stigma: Stepping Out from the Margins; Scior, K., Werner, S., Eds.; Palgrave Macmillan: London, UK, 2016; pp. 31–47. [Google Scholar] [CrossRef]
- Ditchman, N.; Easton, A.B.; Batchos, E.; Rafajko, S.; Shah, N. The Impact of Culture on Attitudes Toward the Sexuality of People with Intellectual Disabilities. Sex. Disabil. 2017, 35, 245–260. [Google Scholar] [CrossRef]
- World Health Organization. Eliminating Forced, Coercive and Otherwise Involuntary Sterilization. 2014. Available online: www.who.int/reproductivehealth (accessed on 29 September 2021).
- Cuskelly, M.; Gilmore, L. Attitudes to Sexuality Questionnaire (Individuals with an Intellectual Disability): Scale development and community norms. J. Intellect. Dev. Disabil. 2007, 32, 214–221. [Google Scholar] [CrossRef]
- Cuskelly, M.; Bryde, R. Attitudes towards the sexuality of adults with an intellectual disability: Parents, support staff, and a community sample. J. Intellect. Dev. Disabil. 2004, 29, 255–264. [Google Scholar] [CrossRef]
- Meaney-Tavares, R.; Gavidia-Payne, S. Staff characteristics and attitudes towards the sexuality of people with intellectual disability. J. Intellect. Dev. Disabil. 2012, 37, 269–273. [Google Scholar] [CrossRef]
- Gilmore, L.; Chambers, B. Intellectual disability and sexuality: Attitudes of disability support staff and leisure industry employees. J. Intellect. Dev. Disabil. 2010, 35, 22–28. [Google Scholar] [CrossRef]
- Pebdani, R.N. Attitudes of Group Home Employees Towards the Sexuality of Individuals with Intellectual Disabilities. Sex. Disabil. 2016, 34, 329–339. [Google Scholar] [CrossRef]
- Hunt, X.; Carew, M.T.; Braathen, S.H.; Swartz, L.; Chiwaula, M.; Rohleder, P. The sexual and reproductive rights and benefit derived from sexual and reproductive health services of people with physical disabilities in South Africa: Beliefs of non-disabled people. Reprod. Health Matters 2017, 25, 66–79. [Google Scholar] [CrossRef] [Green Version]
- Trudel, G.; Desjardins, G. Staff reactions toward the sexual behaviors of people living in institutional settings. Sex. Disabil. 1992, 10, 173–188. [Google Scholar] [CrossRef]
- Saxe, A.; Flanagan, T. Factors that impact support workers’ perceptions of the sexuality of adults with developmental disabilities: A quantitative analysis. Sex. Disabil. 2014, 32, 45–63. [Google Scholar] [CrossRef]
- Bazzo, G.; Nota, L.; Soresi, S.; Ferrari, L.; Minnes, P. Attitudes of social service providers towards the sexuality of individuals with intellectual disability. J. Appl. Res. Intellect. Disabil. 2007, 20, 110–115. [Google Scholar] [CrossRef]
- Sankhla, D.; Theodore, K. British Attitudes Towards Sexuality in Men and Women with Intellectual Disabilities: A Comparison Between White Westerners and South Asians. Sex. Disabil. 2015, 33, 429–445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morales, G.E.M.; Ramirez, E.O.L.; Esterle, M.; Sastre, M.T.M.; Mullet, E. Judging the acceptability of sexual intercourse among people with learning DISABILities: A Mexico-france comparison. Sex. Disabil. 2010, 28, 81–91. [Google Scholar] [CrossRef]
- Carew, M.T.; Braathen, S.H.; Hunt, X.; Swartz, L.; Rohleder, P. Predictors of negative beliefs toward the sexual rights and perceived sexual healthcare needs of people with physical disabilities in South Africa. Disabil. Rehabil. 2020, 42, 3664–3672. [Google Scholar] [CrossRef] [PubMed]
- Camera dei Deputati XVIII Legislatura—Lavori—Progetti di Legge—Scheda del Progetto di Legge. Available online: https://www.camera.it/leg18/126?tab=&leg=18&idDocumento=0569 (accessed on 29 September 2021).
- Parlamento Italiano. Disegno di Legge S. 2005—18a Legislatura. 2021. Available online: https://www.senato.it/leg/18/BGT/Schede/Ddliter/53457.htm (accessed on 23 November 2021).
- Casadio, G. Oltre Trenta Piazze per Rilanciare il ddl Zan. Scintille tra Pd e IV. La Repubblica. Available online: https://www.repubblica.it/politica/2021/10/31/news/ddl_zan_pd_italia_viva-324413430/ (accessed on 23 November 2021).
- Silvaggi, M.; Eleuteri, S.; Colombo, M.; Fava, V.; Malandrino, C.; Simone, S.; Nanini, C.; Rossetto, C.; Di Santo, S.G. Attitudes towards the sexual rights of LGB people: Factors involved in recognition and denial. Sexologies 2019, 28, e72–e81. [Google Scholar] [CrossRef]
- Silvaggi, M.; Di Santo, S.G.; Artioli, C.; Colombo, M.; Fava, V.; Malandrino, C.; Melis, I.; Nanini, C.; Rossetto, C.; Simone, S.; et al. HP-02-005 Sexual rights of minorities in Italy: A snapshot of reality and sociodemographic characteristics involved in the recognition and denial. J. Sex. Med. 2017, 14, e146. [Google Scholar] [CrossRef]
- Franco, D.G.; Cardoso, J.; Neto, I. Attitudes towards affectivity and sexuality of people with intellectual disability. Sex. Disabil. 2012, 30, 261–287. [Google Scholar] [CrossRef]

{kind=link}
| Sample Characteristics | Variable Levels | Frequencies (%) |
|---|---|---|
| Sex | Male | 281 (28.9) |
| Female | 692 (71.1) | |
| Age | 18–29 | 348 (35.8) |
| 30–39 | 338 (34.7) | |
| 40 or more | 287 (29.5) | |
| Provenience | North | 390 (40.1) |
| Center | 314 (32.3) | |
| South and Islands | 269 (27.6) | |
| Education | Undergraduate | 332 (34.1) |
| Graduate | 391 (40.2) | |
| Post-graduate | 250 (25.7) | |
| Occupation | Student | 206 (21.2) |
| Employed | 620 (63.7) | |
| Unemployed or retired | 147 (15.1) | |
| Relational status | Single | 285 (29.3) |
| In a committed relationship | 260 (26.7) | |
| Cohabiting with partner | 190 (19.5) | |
| Married | 238 (24.5) | |
| Religiosity | Atheist/agnostic | 464 (47.7) |
| Believer | 361 (37.2) | |
| Churchgoer | 148 (15.2) | |
| Sexual orientation | Heterosexual | 730 (75.0) |
| Not-completely heterosexual, homosexual, bisexual or queer | 243 (25.0) |
| Agreement with the Right of People with Disabilities to Have Satisfactory Sexuality | People with Physical Disabilities | People with Psychical Disabilities | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Freq % | Univariate LR | Multiple LR | Freq % | Univariate LR | Multiple LR | ||||||
| OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | ||||
| Sex | Male | 92.5 | - | - | - | - | 81.9 | - | - | - | - |
| Female | 96.1 | 1.99 (1.11–3.58) | 0.022 | 2.11 (1.11–4.01) | 0.022 | 87.1 | 1.5 (1.03–2.19) | 0.034 | 1.55 (1.03–2.35) | 0.038 | |
| Age | 18–29 | 94.5 | - | - | - | - | 86.5 | - | - | - | - |
| 30–39 | 95.0 | 1.09 (0.55–2.13) | 0.801 | 0.76 (0.29–1.99) | 0.579 | 84.9 | 0.88 (0.57–1.35) | 0.554 | 0.84 (0.49–1.47) | 0.551 | |
| 40 or more | 95.8 | 1.32 (0.63–2.78) | 0.458 | 1.40 (0.48–4.13) | 0.538 | 85.4 | 0.91 (0.58–1.43) | 0.684 | 1.16 (0.63–2.12) | 0.642 | |
| Provenience | North | 96.2 | - | - | - | - | 88.2 | - | - | - | - |
| Center | 94.3 | 0.66 (0.33–1.33) | 0.242 | 0.59 (0.28–1.24) | 0.164 | 86.0 | 0.82 (0.53–1.28) | 0.382 | 0.74 (0.46–1.19) | 0.221 | |
| South and Islands | 94.4 | 0.68 (0.33–1.41) | 0.298 | 0.80 (0.37–2.01) | 0.584 | 81.4 | 0.59 (0.38–0.90) | 0.016 | 0.63 (0.39–1.00) | 0.051 | |
| Instruction | Undergraduate | 93.1 | - | - | - | - | 81.6 | - | - | - | - |
| Graduate | 96.9 | 2.35 (1.15–4.80) | 0.019 | 1.91 (0.89–4.08) | 0.096 | 88.5 | 1.73 (1.14–2.63) | 0.010 | 1.73 (1.1–2.72) | 0.019 | |
| Post-graduate | 94.8 | 1.36 (0.68–2.74) | 0.393 | 0.89 (0.39–2.01) | 0.777 | 86.4 | 1.43 (0.91–2.26) | 0.124 | 1.42 (0.85–2.36) | 0.179 | |
| Occupation | Unemployed-retired | 92.5 | - | - | - | - | 76.9 | - | - | - | - |
| Employed | 96.3 | 2.10 (1.00–4.41) | 0.050 | 2.16 (0.97–4.78) | 0.058 | 86.8 | 1.97 (1.26–3.09) | 0.003 | 1.92 (1.18–3.11) | 0.008 | |
| Student | 93.2 | 1.11 (0.49–2.52) | 0.804 | 0.95 (0.34–2.67) | 0.924 | 88.3 | 2.28 (1.29–4.05) | 0.005 | 2.47 (1.27–4.81) | 0.008 | |
| Heterosexual | Yes | 94.9 | - | - | - | - | 84.5 | - | - | - | - |
| Not completely/no | 95.5 | 1.13 (0.57–2.24) | 0.736 | 1.44 (0.66–3.15) | 0.361 | 88.9 | 1.47 (0.94–2.29) | 0.094 | 1.35 (0.82–2.22) | 0.241 | |
| Relational status | Single/casual partners | 94.5 | - | - | - | - | 80.7 | - | - | - | - |
| In a committed relationship | 97.9 | 2.33 (1.05–5.16) | 0.037 | 2.64 (0.8–8.75) | 0.112 | 87.3 | 1.64 (1.03–2.63) | 0.037 | 1.52 (0.93–2.48) | 0.094 | |
| Cohabiting with partner | 96.5 | 3.89 (1.32–11.47) | 0.014 | 1.86 (0.69–5.04) | 0.220 | 90.0 | 2.15 (1.23–3.76) | 0.007 | 1.92 (1.06–3.48) | 0.032 | |
| Married | 92.3 | 1.45 (0.71–2.94) | 0.306 | 0.82 (0.36–1.87) | 0.637 | 86.1 | 1.49 (0.93–2.38) | 0.099 | 1.87 (1.11–3.17) | 0.019 | |
| Religiosity | Atheist/agnostic | 95.5 | - | - | - | - | 89.9 | - | - | - | - |
| Believer | 94.5 | 0.81 (0.43–1.51) | 0.808 | 0.77 (0.39–1.52) | 0.450 | 82.5 | 0.53 (0.36–0.8) | 0.002 | 0.55 (0.36–0.85) | 0.007 | |
| Churchgoer | 93.3 | 0.96 (0.40–2.30) | 0.918 | 0.97 (0.38–2.47) | 0.945 | 79.7 | 0.44 (0.27–0.73) | 0.001 | 0.44 (0.26–0.77) | 0.004 | |
| Agreement with the Right of People with Disabilities to Get Married | People with Physical Disabilities | People with Psychical Disabilities | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Freq % | Univariate LR | Multiple LR | Freq % | Univariate LR | Multiple LR | ||||||
| OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | ||||
| Sex | Male | 97.2 | - | - | - | - | 71.2 | - | - | - | |
| Female | 98.7 | 2.22 (0.85–5.82) | 0.104 | 2.05 (0.71–5.9) | 0.183 | 81.8 | 1.82 (1.32–2.51) | 0.000 | 1.83 (1.28–2.63) | 0.001 | |
| Age | 18–29 | 100.0 | - | - | - | - | 86.2 | - | - | - | - |
| 30–39 | 97.6 | - | - | - | - | 76.3 | 0.52 (0.35–0.77) | 0.001 | 0.62 (0.37–1.03) | 0.066 | |
| 40 or more | 96.9 | 0.36 (0.14–0.95) | 0.040 | 0.9 (0.28–2.85) | 0.852 | 72.5 | 0.42 (0.28–0.63) | 0.000 | 0.68 (0.39–1.16) | 0.152 | |
| Provenience | North | 97.9 | - | - | - | - | 78.7 | - | - | - | - |
| Center | 98.7 | 1.62 (0.48–5.44) | 0.433 | 1.13 (0.3–4.18) | 0.856 | 81.8 | 1.22 (0.84–1.77) | 0.302 | 1.03 (0.69–1.55) | 0.869 | |
| South and Islands | 98.1 | 1.11 (0.36–3.42) | 0.861 | 0.96 (0.28–3.27) | 0.952 | 75.1 | 0.82 (0.56–1.18) | 0.276 | 0.76 (0.51–1.14) | 0.182 | |
| Instruction | Undergraduate | 97.3 | - | - | - | - | 74.4 | - | - | - | - |
| Graduate | 98.7 | 2.15 (0.71–6.48) | 0.174 | 1.45 (0.42–4.99) | 0.557 | 80.6 | 1.43 (1–2.03) | 0.048 | 1.35 (0.91–1.99) | 0.134 | |
| Post-graduate | 98.8 | 2.29 (0.61–8.56) | 0.217 | 2.06 (0.49–8.6) | 0.321 | 81.6 | 1.53 (1.02–2.29) | 0.040 | 1.90 (1.21–2.98) | 0.005 | |
| Occupation | Unemployed-retired | 96.6 | - | - | - | - | 73.5 | - | - | - | - |
| Employed | 98.2 | 1.95 (0.67–5.7) | 0.223 | 1.9 (0.6–5.98) | 0.272 | 76.6 | 1.18 (0.78–1.78) | 0.423 | 1.32 (0.84–2.07) | 0.224 | |
| Student | 99.5 | 7.22 (0.83–62.45) | 0.073 | 4.49 (0.42–47.69) | 0.213 | 88.8 | 2.87 (1.63–5.07) | 0.000 | 2.31 (1.2–4.43) | 0.012 | |
| Heterosexual | Yes | 97.8 | - | - | - | - | 75.5 | - | - | - | - |
| Not completely/no | 99.6 | 5.42 (0.72–41.11) | 0.102 | 2.37 (0.27–20.54) | 0.434 | 88.5 | 2.49 (1.63–3.83) | 0.000 | 1.81 (1.13–2.88) | 0.013 | |
| Relational status | Single/casual partners | 97.5 | - | - | - | - | 80.0 | - | - | - | - |
| In a committed relationship | 99.6 | 6.52 (0.8–53.37) | 0.080 | 4.96 (0.58–42.2) | 0.143 | 80.4 | 1.02 (0.67–1.56) | 0.910 | 0.81 (0.52–1.28) | 0.373 | |
| Cohabiting with partner | 99.5 | 4.76 (0.58–39) | 0.146 | 3.39 (0.38–29.87) | 0.271 | 83.7 | 1.28 (0.79–2.08) | 0.312 | 1.12 (0.66–1.88) | 0.680 | |
| Married | 96.6 | 0.72 (0.26–2.03) | 0.538 | 1.18 (0.39–3.63) | 0.768 | 71.4 | 0.63 (0.42–0.94) | 0.023 | 0.93 (0.59–1.47) | 0.765 | |
| Religiosity | Atheist/agnostic | 99.6 | - | - | - | - | 84.9 | - | - | - | - |
| Believer | 97.5 | 0.17 (0.04–0.79) | 0.024 | 0.22 (0.04–1.08) | 0.062 | 76.7 | 0.59 (0.41–0.83) | 0.003 | 0.68 (0.46–0.99) | 0.046 | |
| Churchgoer | 95.9 | 0.1 (0.02–0.51) | 0.006 | 0.14 (0.03–0.76) | 0.023 | 64.2 | 0.32 (0.21–0.49) | 0.000 | 0.38 (0.24–0.61) | 0.000 | |
| Agreement with the Right of People with Disabilities to Adopt a Child | People with Physical Disabilities | People with Psychical Disabilities | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Freq % | Univariate LR | Multiple LR | Freq % | Univariate LR | Multiple LR | ||||||
| OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | ||||
| Sex | Male | 81.1 | - | - | - | - | 19.9 | - | - | - | - |
| Female | 81.9 | 1.05 (0.74–1.51) | 0.771 | 0.99 (0.67–1.46) | 0.949 | 22.5 | 1.17 (0.83–1.65) | 0.371 | 1.05 (0.73–1.52) | 0.800 | |
| Age | 18–29 | 81.6 | - | - | - | - | 25.9 | - | - | - | - |
| 30–39 | 84.0 | 1.19 (0.8–1.76) | 0.402 | 1.29 (0.77–2.14) | 0.332 | 20.7 | 0.75 (0.52–1.07) | 0.111 | 0.84 (0.53–1.34) | 0.465 | |
| 40 or more | 79.1 | 0.85 (0.58–1.26) | 0.426 | 1.17 (0.68–2.00) | 0.576 | 18.1 | 0.63 (0.43–0.93) | 0.020 | 0.83 (0.49–1.40 | 0.486 | |
| Provenience | North | 82.6 | - | - | - | - | 21.8 | - | - | - | - |
| Center | 84.1 | 1.12 (0.75–1.66) | 0.593 | 1.04 (0.68–1.58) | 0.853 | 23.9 | 1.13 (0.79–1.6) | 0.511 | 1.07 (0.74–1.55) | 0.712 | |
| South and Islands | 77.7 | 0.74 (0.5–1.08) | 0.121 | 0.74 (0.49–1.11) | 0.144 | 19.3 | 0.86 (0.58–1.27) | 0.444 | 0.86 (0.58–1.29) | 0.479 | |
| Instruction | Undergraduate | 77.4 | - | - | - | - | 17.8 | - | - | - | - |
| Graduate | 82.6 | 1.39 (0.96–2) | 0.081 | 1.37 (0.92–2.04) | 0.118 | 22.8 | 1.36 (0.94–1.97) | 0.098 | 1.43 (0.97–2.11) | 0.074 | |
| Post-graduate | 86.0 | 1.79 (1.15–2.78) | 0.009 | 1.84 (1.14–2.98) | 0.013 | 25.6 | 1.59 (1.07–2.37) | 0.023 | 1.97 (1.26–3.08) | 0.003 | |
| Occupation | Unemployed-retired | 77.6 | - | - | - | - | 21.8 | - | - | - | - |
| Employed | 82.1 | 1.33 (0.86–2.06) | 0.206 | 1.14 (0.71–1.81) | 0.590 | 19.5 | 0.87 (0.56–1.35) | 0.539 | 0.82 (0.51–1.30) | 0.395 | |
| Student | 83.5 | 1.46 (0.86–2.5) | 0.162 | 1.51 (0.82–2.78) | 0.186 | 28.6 | 1.44 (0.88–2.37) | 0.147 | 1.51 (0.87–2.65) | 0.146 | |
| Heterosexual | Yes | 79.2 | - | - | - | - | 20.3 | - | - | - | - |
| Not completely/no | 89.3 | 2.19 (1.41–3.42) | 0.001 | 2.03 (1.26–3.27) | 0.004 | 26.3 | 1.41 (1–1.97) | 0.048 | 1.16 (0.8–1.68) | 0.430 | |
| Relational status | Single/casual partners | 79.3 | - | - | - | - | 20.4 | - | - | - | - |
| In a committed relationship | 83.1 | 1.28 (0.83–1.98) | 0.261 | 1.28 (0.82–2.01) | 0.280 | 21.9 | 1.1 (0.73–1.66) | 0.653 | 0.98 (0.64–1.50) | 0.917 | |
| Cohabiting with partner | 87.9 | 1.90 (1.13–3.19) | 0.016 | 1.7 (0.98–2.96) | 0.061 | 26.8 | 1.44 (0.93–2.21) | 0.100 | 1.42 (0.89–2.26) | 0.145 | |
| Married | 78.2 | 0.93 (0.61–1.42) | 0.749 | 1.05 (0.66–1.68) | 0.835 | 19.3 | 0.94 (0.61–1.44) | 0.770 | 1.29 (0.79–2.10) | 0.314 | |
| Religiosity | Atheist/agnostic | 85.6 | - | - | - | - | 26.1 | - | - | - | - |
| Believer | 77.6 | 0.58 (0.41–0.83) | 0.003 | 0.72 (0.49–1.05) | 0.089 | 20.2 | 0.72 (0.52–1) | 0.050 | 0.79 (0.55–1.12) | 0.181 | |
| Churchgoer | 79.7 | 0.66 (0.41–1.07) | 0.092 | 0.88 (0.53–1.47) | 0.623 | 12.2 | 0.39 (0.23–0.67) | 0.001 | 0.44 (0.25–0.77) | 0.004 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Santo, S.G.; Colombo, M.; Silvaggi, M.; Gammino, G.R.; Fava, V.; Malandrino, C.; Nanini, C.; Rossetto, C.; Simone, S.; Eleuteri, S. The Sexual and Parenting Rights of People with Physical and Psychical Disabilities: Attitudes of Italians and Socio-Demographic Factors Involved in Recognition and Denial. Int. J. Environ. Res. Public Health 2022, 19, 1017. https://doi.org/10.3390/ijerph19021017
Di Santo SG, Colombo M, Silvaggi M, Gammino GR, Fava V, Malandrino C, Nanini C, Rossetto C, Simone S, Eleuteri S. The Sexual and Parenting Rights of People with Physical and Psychical Disabilities: Attitudes of Italians and Socio-Demographic Factors Involved in Recognition and Denial. International Journal of Environmental Research and Public Health. 2022; 19(2):1017. https://doi.org/10.3390/ijerph19021017
Chicago/Turabian StyleDi Santo, Simona Gabriella, Margherita Colombo, Marco Silvaggi, Giorgia Rosamaria Gammino, Valentina Fava, Chiara Malandrino, Chiara Nanini, Cristina Rossetto, Sara Simone, and Stefano Eleuteri. 2022. "The Sexual and Parenting Rights of People with Physical and Psychical Disabilities: Attitudes of Italians and Socio-Demographic Factors Involved in Recognition and Denial" International Journal of Environmental Research and Public Health 19, no. 2: 1017. https://doi.org/10.3390/ijerph19021017
APA StyleDi Santo, S. G., Colombo, M., Silvaggi, M., Gammino, G. R., Fava, V., Malandrino, C., Nanini, C., Rossetto, C., Simone, S., & Eleuteri, S. (2022). The Sexual and Parenting Rights of People with Physical and Psychical Disabilities: Attitudes of Italians and Socio-Demographic Factors Involved in Recognition and Denial. International Journal of Environmental Research and Public Health, 19(2), 1017. https://doi.org/10.3390/ijerph19021017