
COVID-19 Vaccination and Mental Stress within Diverse Sociodemographic Groups

 ,
,  ,
, 

Abstract
1. Introduction
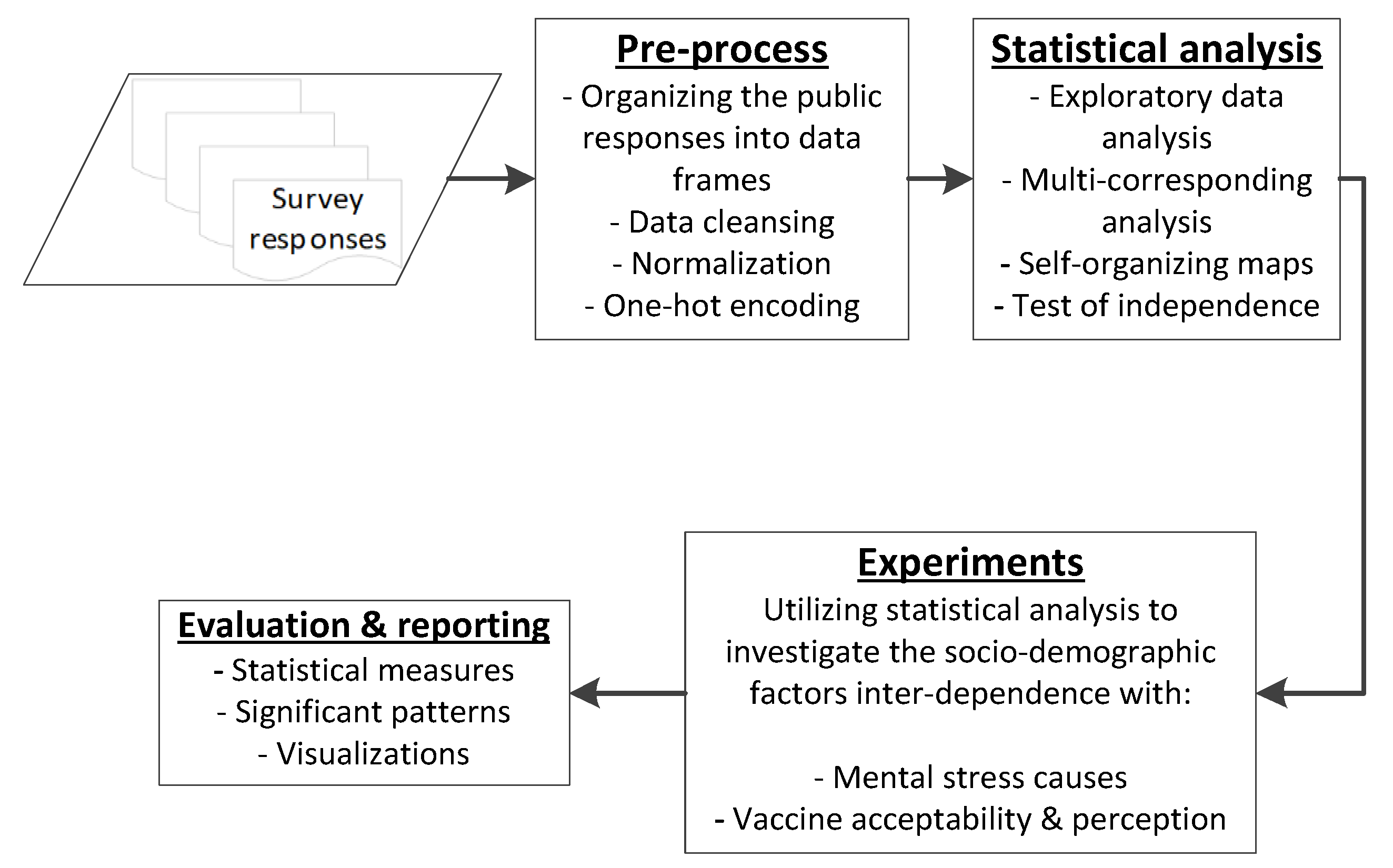
2. Materials and Methods
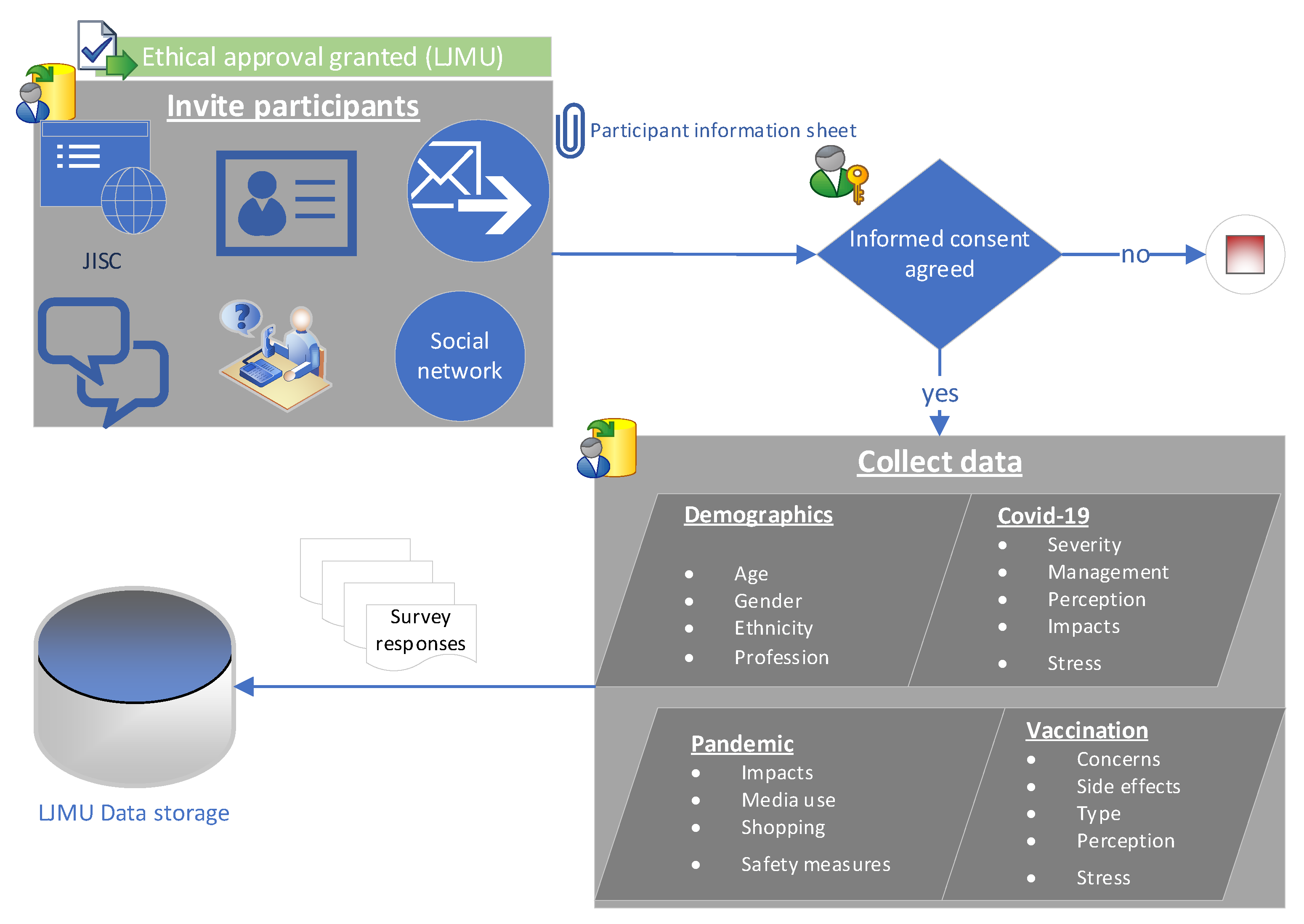
2.1. Primary Dataset Acquisition
2.2. Data Preparation
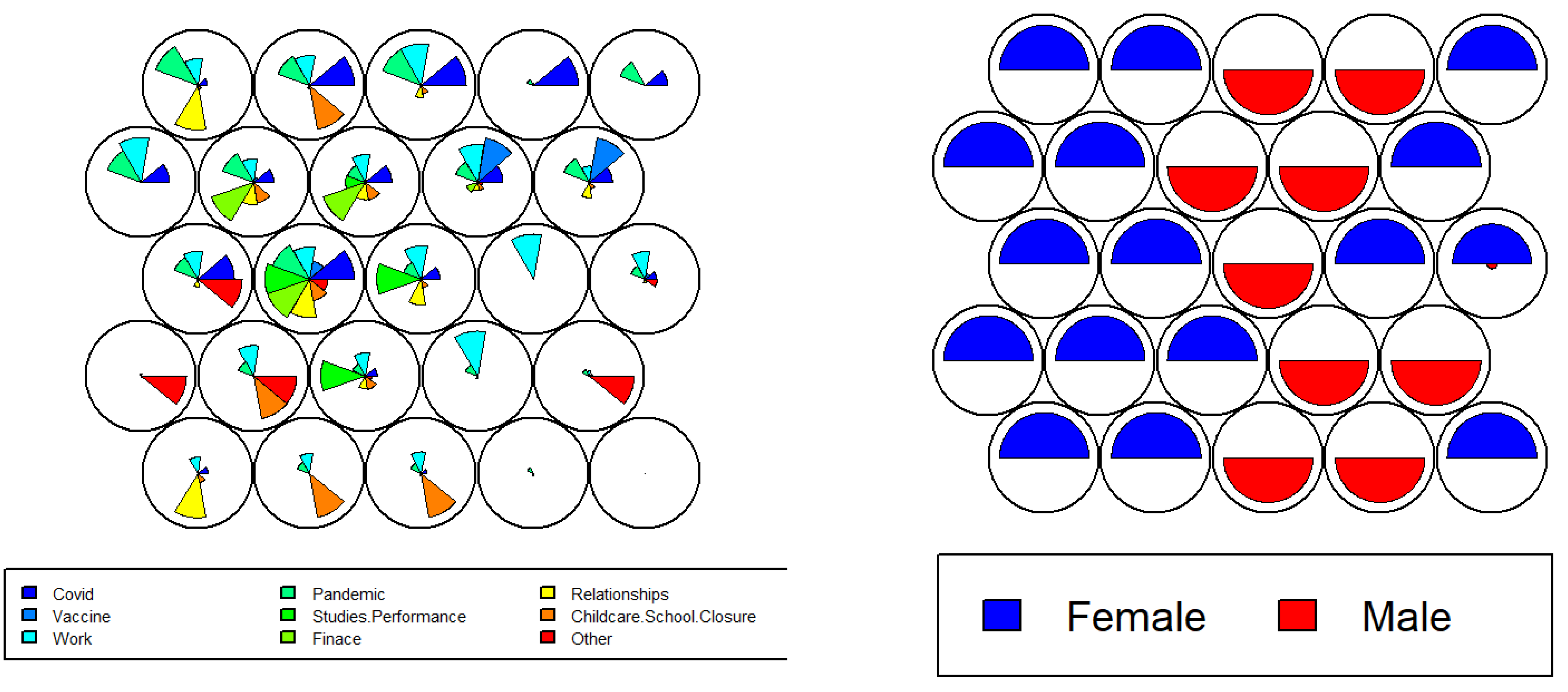
2.3. Statistical Analysis and Visualisations
3. Results and Discussions
3.1. Mental Stress Causes
3.1.1. Sex (Male, Female)
3.1.2. Age Groups
3.1.3. Ethnicity
3.1.4. Profession
3.2. Vaccination Acceptability and Perception
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gov.UK. Coronavirus (COVID-19) in the UK. 2021. Available online: https://coronavirus.data.gov.uk/ (accessed on 2 June 2021).
- Mitchell, O.J.L.; Yuriditsky, E.; Johnson, N.J.; Doran, O.; Buckler, D.G.; Neefe, S.; Seethala, R.R.; Motov, S.; Moskowitz, A.; Lee, J.; et al. In-hospital cardiac arrest in patients with coronavirus 2019. Rescucitatio 2021, 160, 72–78. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Yu, Y.; Xu, J.; Shu, H.; Liu, H.; Wu, Y.; Zhang, L.; Yu, Z.; Fang, M.; Yu, T.; et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: A single-centered, retrospective, observational study. Lancet Respir. Med. 2020, 8, 475–481. [Google Scholar] [CrossRef]
- Walker, P.G.; Whittaker, C.; Watson, O.J.; Baguelin, M.; Winskill, P.; Hamlet, A.; Djafaara, B.A.; Cucunubá, Z.; Mesa, D.O.; Green, W.; et al. The global impact of COVID-19 and strategies for mitigation and suppression. Science 2020, 369, 413–422. [Google Scholar] [CrossRef] [PubMed]
- Maston, A.; Motti-Stefanidi, F. Multisystem Resilience for Children and Youth in Disaster: Reflections in the Context of COVID-19. Advers. Resil. Sci. 2020, 1, 95–106. [Google Scholar] [CrossRef]
- Duan, L.; Zhu, G. Psychological interventions for people affected by the COVID-19 epidemic. Lancet Psychiatry 2020, 7, 300–302. [Google Scholar] [CrossRef]
- Qiu, J.; Shen, B.; Zhao, M.; Wang, Z.; Xie, B.; Xu, Y. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: Implications and policy recommendations. Gen. Psychiatry 2020, 33, e100213. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate Psychological Responses and Associated Factors during the Initial Stage of the 2019 Coronavirus Disease (COVID-19) Epidemic among the General Population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef]
- Lima, C.K.T.; Carvalho, P.M.D.M.; Lima, I.D.A.A.S.; Nunes, J.V.A.D.O.; Saraiva, J.S.; de Souza, R.I.; da Silva, C.G.L.; Neto, M.L.R. The emotional impact of Coronavirus 2019-nCoV (new Coronavirus disease). Psychiatry Res. 2020, 287, 112915. [Google Scholar] [CrossRef]
- Bo, H.-X.; Li, W.; Yang, Y.; Wang, Y.; Zhang, Q.; Cheung, T.; Wu, X.; Xiang, Y.-T. Posttraumatic stress symptoms and attitude toward crisis mental health services among clinically stable patients with COVID-19 in China. Psychol. Med. 2020, 51, 1052–1053. [Google Scholar] [CrossRef]
- Taylor, S.; Landry, C.A.; Paluszek, M.M.; Fergus, T.A.; McKay, D.; Asmundson, G.J.G. Development and initial validation of the COVID Stress Scales. J. Anxiety Disord. 2020, 72, 102232. [Google Scholar] [CrossRef]
- Calvano, C.; Engelke, L.; Bella, J.D.; Kindermann, J.; Renneberg, B.; Winter, S.M. Families in the COVID-19 pandemic: Parental stress, parent mental health and the occurrence of adverse childhood experiences—Results of a representative survey in Germany. Eur. Child Adolesc. Psychiatry 2021, 31, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Prowse, R.; Sherratt, F.; Abizaid, A.; Gabrys, R.L.; Hellemans, K.G.C.; Patterson, Z.R.; McQuaid, R.J. Coping With the COVID-19 Pandemic: Examining Gender Differences in Stress and Mental Health Among University Students. Front. Psychiatry 2021, 12, 650759. [Google Scholar] [CrossRef] [PubMed]
- Alnazly, E.; Khraisat, O.M.; Al-Bashaireh, A.M.; Bryant, C.L. Anxiety, depression, stress, fear and social support during COVID-19 pandemic among Jordanian healthcare workers. PLoS ONE 2021, 16, e0247679. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.B.; Sun, J.; Liu, L.; Zhao, Y.M.; Yan, W.; Yuan, K.; Su, S.; Lu, Z.; Huang, Y.; Liu, L.; et al. COVID-19 Vaccine-Related Psychological Stress Among General Public in China. Front. Psychiatry 2021, 12, 774504. [Google Scholar] [CrossRef] [PubMed]
- De Roo, S.S.; Pudalov, N.J.; Fu, L.Y. Planning for a COVID-19 Vaccination Program. JAMA 2020, 323, 2458. [Google Scholar] [CrossRef]
- Coe, A.B.; Elliott, M.H.; Gatewood, S.B.; Goode, J.-V.R.; Moczygemba, L.R. Perceptions and predictors of intention to receive the COVID-19 vaccine. Res. Soc. Adm. Pharm. 2021, 18, 2593–2599. [Google Scholar] [CrossRef]
- Reiter, P.L.; Pennell, M.L.; Katz, M.L. Acceptability of a COVID-19 vaccine among adults in the United States: How many people would get vaccinated? Vaccine 2020, 38, 6500–6507. [Google Scholar] [CrossRef]
- Kreps, S.; Prasad, S.; Brownstein, J.S.; Hswen, Y.; Garibaldi, B.T.; Zhang, B.; Kriner, D.L. Factors Associated With US Adults’ Likelihood of Accepting COVID-19 Vaccination. JAMA Netw. Open 2020, 3, e2025594. [Google Scholar] [CrossRef]
- Malik, A.A.; McFadden, S.M.; Elharake, J.; Omer, S.B. Determinants of COVID-19 vaccine acceptance in the US. eClinicalMedicine 2020, 26, 100495. [Google Scholar] [CrossRef]
- Kumari, A.; Ranjan, P.; Chopra, S.; Kaur, D.; Kaur, T.; Kalanidhi, K.B.; Goel, A.; Singh, A.; Baitha, U.; Prakash, B.; et al. What Indians Think of the COVID-19 vaccine: A qualitative study comprising focus group discussions and thematic analysis. Diabetes Metab. Syndr. Clin. Res. Rev. 2021, 15, 679–682. [Google Scholar] [CrossRef]
- Maraqa, B.; Nazzal, Z.; Rabi, R.; Sarhan, N.; Al-Shakhra, K.; Al-Kaila, M. COVID-19 vaccine hesitancy among health care workers in Palestine: A call for action. Prev. Med. 2021, 149, 106618. [Google Scholar] [CrossRef]
- Dryhurst, S.; Schneider, C.R.; Kerr, J.; Freeman, A.L.; Recchia, G.; Van Der Bles, A.M.; Spiegelhalter, D.; van der Linden, S. Risk perceptions of COVID-19 around the world. J. Risk Res. 2020, 23, 994–1006. [Google Scholar] [CrossRef]
- Glöckner, A.; Dorrough, A.R.; Wingen, T.; Dohle, S. The Perception of Infection Risks during the Early and Later Outbreak of COVID-19 in Germany: Consequences and Recommendations. arXiv 2020. [Google Scholar]
- Adams, S.H.; Schaub, J.P.; Nagata, J.M.; Park, M.J.; Brindis, C.D.; Irwin, C., Jr. Young Adult Perspectives on COVID-19 Vaccinations. J. Adolesc. Health 2021, 69, 511–514. [Google Scholar] [CrossRef]
- Menni, C.; Klaser, K.; May, A.; Polidori, L.; Capdevila, J.; Louca, P.; Sudre, C.H.; Nguyen, L.H.; David, A.; Drew, J.M.; et al. Vaccine side-effects and SARS-CoV-2 infection after vaccination in users of the COVID Symptom Study app in the UK: A prospective observational study. Lancet Infect. Dis. 2021, 21, 939–949. [Google Scholar] [CrossRef]
- Quiroga, B.; Sánchez-Álvarez, E.; Goicoechea, M.; de Sequera, P. COVID-19 vaccination among Spanish nephrologists: Acceptance and side effectsVacunación frente a la COVID-19 en nefrólogos: Resultados de una encuesta nacional sobre aceptación y efectos adversos. J. Helathcare Qual. Res. 2021, 36, 363–369. [Google Scholar] [CrossRef]
- FAO and WFP. Mitigating the Effects of the COVID-19 Pandemic on Food and Nutrition of Schoolchildren; Food and Agriculture Organization of the United Nations (FAO): Rome, Italy, 2020. [Google Scholar]
- Singh, S.; Roy, D.; Sinha, K.; Parveen, S.; Sharma, G.; Joshi, G. Impact of COVID-19 and lockdown on mental health of children and adolescents: A narrative review with recommendations. Psychiatry Res. 2020, 293, 113429. [Google Scholar] [CrossRef]
- Saurabh, K.; Ranjan, S. Compliance and Psychological Impact of Quarantine in Children and Adolescents due to Covid-19 Pandemic. Indian J. Pediatr. 2020, 87, 532–536. [Google Scholar] [CrossRef]
- Wang, G.; Zhang, Y.; Zhao, J.; Zhang, J.; Jiang, F. Mitigate the effects of home confinement on children during the COVID-19 outbreak. Lancet 2020, 395, 945–947. [Google Scholar] [CrossRef]
- Agarwal, A. Moving beyond DSM5 and ICD11: Acoustic analysis for psychological stress on daily-wage workers in India during COVID. Comput. Hum. Behav. Rep. 2021, 3, 100075. [Google Scholar] [CrossRef]
- Lee, J.; Jeong, H.J.; Kim, S. Stress, Anxiety, and Depression Among Undergraduate Students during the COVID-19 Pandemic and their Use of Mental Health Services. Innov. High. Educ. 2021, 46, 519–538. [Google Scholar] [CrossRef] [PubMed]
- Banna, M.H.A.; Sayeed, A.; Kundu, S.; Christopher, E.; Hasan, M.T.; Begum, M.R.; Kormoker, T.; Dola, S.T.I.; Hassan, M.; Chowdhury, S.; et al. The impact of the COVID-19 pandemic on the mental health of the adult population in Bangladesh: A nationwide cross-sectional study. Int. J. Environ. Health Res. 2022, 32, 850–861. [Google Scholar] [CrossRef] [PubMed]
- Manchia, M.; Gathier, A.W.; Yapici-Eser, H.; Schmidt, M.V.; de Quervain, D.; van Amelsvoort, T.; Bisson, J.I.; Cryan, J.F.; Howes, O.D.; Pinto, L.; et al. The impact of the prolonged COVID-19 pandemic on stress resilience and mental health: A critical review across waves. Eur. Neuropsychopharmacol. 2021, 55, 22–83. [Google Scholar] [CrossRef] [PubMed]
- Cénat, J.M.; Blais-Rochette, C.; Kokou-Kpolou, C.K.; Noorishad, P.-G.; Mukunzi, J.N.; McIntee, S.-E.; Dalexis, R.D.; Goulet, M.-A.; Labelle, P.R. Prevalence of symptoms of depression, anxiety, insomnia, posttraumatic stress disorder, and psychological distress among populations affected by the COVID-19 pandemic: A systematic review and meta-analysis. Psychiatry Res. 2021, 295, 113599. [Google Scholar] [CrossRef]
- Pandey, K.; Thurman, M.; Johnson, S.D.; Acharya, A.; Johnston, M.; Klug, E.A.; Olwenyi, O.A.; Rajaiah, R.; Byrareddy, S.N. Mental Health Issues During and After COVID-19 Vaccine Era. Brain Res. Bull. 2021, 176, 161–173. [Google Scholar] [CrossRef]
- Khan, W.; Hussain, A.; Khan, S.A.; Al-Jumailey, M.; Nawaz, R.; Liatsis, P. Analysing the impact of global demographic characteristics over the COVID-19 spread using class rule mining and pattern matching. R. Soc. Open Sci. 2021, 8, 201823. [Google Scholar] [CrossRef]
- Sobotka, T.; Brzozowska, Z.; Muttarak, R.; Zeman, K.; di Lego, V. Age, gender and COVID-19 infections. medRxiv 2020. [Google Scholar]
- Pradhan, A.; Olsson, P.-E. Sex differences in severity and mortality from COVID-19: Are males more vulnerable? Biol. Sex Differ. 2020, 11, 1–11. [Google Scholar] [CrossRef]
- Al-Maroof, R.; Alhumaid, K.; Akour, I.; Salloum, S. Factors That Affect E-Learning Platforms after the Spread of COVID-19: Post Acceptance Study. Data 2021, 6, 49. [Google Scholar] [CrossRef]
- Loomba, S.; de Figueiredo, A.; Piatek, S.J.; de Graaf, K.; Larson, H.J. Measuring the impact of COVID-19 vaccine misinformation on vaccination intent in the UK and USA. Nat. Hum. Behav. 2021, 5, 337–348, Correction in 2021, 5, 960. [Google Scholar] [CrossRef]
- Russell, F.M.; Greenwood, B. Who should be prioritised for COVID-19 vaccination? Hum. Vaccines Immunother. 2020, 17, 1317–1321. [Google Scholar] [CrossRef] [PubMed]
- Bramer, C.A.; Kimmins, L.M.; Swanson, R.; Kuo, J.; Vranesich, P.; Jacques-Carroll, L.A.; Shen, A.K. Decline in child vaccination coverage during the COVID-19 pandemic. Am. J. Transplant. 2020, 20, 1930–1931. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, D.; Finlay, I.; Pollard, A.J.; Forsberg, L.; Skelton, A. Should we delay covid-19 vaccination in children? BMJ 2021, 374, n1687. [Google Scholar] [CrossRef] [PubMed]
- Karzan, R.S.; Dana, K.S.; Shakhawan, M.A.; Kodzius, R. Does Early Childhood Vaccination Protect Against COVID-19? Front. Mol. Biosci. 2020, 7. [Google Scholar]
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2021, 27, 225–228. [Google Scholar] [CrossRef]
- Paul, E.; Steptoe, A.; Fancourt, D. Attitudes towards vaccines and intention to vaccinate against COVID-19: Implications for public health communications. Lancet Reg. Health Eur. 2021, 1, 100012. [Google Scholar] [CrossRef]
- de Figueiredo, A. Sub-national forecasts of COVID-19 vaccine acceptance across the UK: A large-scale cross-sectional spatial modelling study. medRxiv 2020. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study/Method | Outcomes | Public Data | Comments |
|---|---|---|---|
| Ref. [15] Analysis of psychological stress associated with COVID-19 vaccination in China. Multi-linear regression (MLR) is used to identify the strength of the relationship | Higher stress level is noticed in participants with a low level of education, young age, history of chronic disease, mistrust of the vaccination | No | It would be better to ask participants about how they cope with mental stress. No multi-dimensional pattern analysis is performed |
| Ref. [12] 1024 parents were surveyed to analyse the parental stress and occurrence of adverse childhood experience (ACE) during the pandemic in Germany | Over 50% of the parents reported being stressed by social distancing and the closure of schools and childcare facilities. Up to 33% of the sample reported ACEs in the child’s lifetime | No | Simple frequency and correlation statistics are measured indicating the association between individual factors. No multi-dimensional pattern analysis is performed |
| Ref. [13] Gender differences in the mental health of university students during the COVID-19 pandemic is addressed using an online survey of 366 undergraduates | Female students are more affected by isolation in the pandemic as compared to males. Regardless of gender, the pandemic has a negative impact on social relationships | No | Study reported the use of social media as a coping strategy with the pandemic situation, however, it affected the students’ academic performance. No multi-dimensional pattern analysis is performed |
| Ref. [33] Stress, anxiety and depression among undergraduate students during the pandemic is addressed. Responses from 2059 students are considered for the analysis using MLR | Females, rural, low-income, and academically underperforming students are identified as being more vulnerable to mental stress, anxiety and depression | No | Study mainly focuses on pandemic-related issues. The authors could also include a survey question about coping strategies for these challenges. No multi-dimensional pattern analysis is performed |
| Ref. [14] Anxiety, stress, depression, and fear during the pandemic in healthcare workers (365 survey participants) are analysed in Jordan | Psychological distress is associated with multiple factors including being male, married, aged 40 years and older, and having more clinical experience. Study also reported that social support during the pandemic is primarily dependent on support from their families, followed by support from friends | Yes | Authors may use appropriate data transformation (e.g., one-hot encoding). Study also addressed some strategies to mental health issues (e.g., social support during pandemic). Sample is comparatively small. No multi-dimensional pattern analysis is performed |
| Ref. [34] Pandemic impact on the mental health of adults in Bangladesh is addressed. A total of 1427 participants were surveyed and analysed using MLR. | Study reported a high level of: -Anxiety within the older age group (40 plus), females, low education level, and housewives -Depressive symptoms in youth (23 years and younger), females, and unemployed people -Stress in females and unemployed people. | No | Study addresses the sociodemographic factors, including gender, age, educational level, religion, etc., however, with limited diversity (e.g., one ethnic background and 75% male participants). No multi-dimensional pattern analysis is performed |
| Refs. [35,36,37] Review studies on mental health issues associated with COVID-19, vaccination, and the pandemic | [37] COVID-19 has direct and indirect impacts on mental health. [35] Healthcare workers, children, students, people with existing psychiatric disorder, and adolescents have been particularly affected by the pandemic. [36] Depression, anxiety, and psychological distress are highly associated with the pandemic. There is no significant difference in gender and geographic locations | NA | Recommended non-psychiatrist coping mechanisms to help prevent mental health issues. Large subjective variations exists in relation to mental health issues, indicating the need to provide personalised help and interventions (for post-pandemic and future epidemics) mainly to the vulnerable groups. |
| Attribute | n(%) | Attribute | n(%) | Attribute | n(%) |
|---|---|---|---|---|---|
| Ethnicity | |||||
| - Asian/Arabic | 146(24) | Profession | age-Group | ||
| - White British | 386(64) | - Education | 284(47) | - Under 20 | 12(2) |
| - White EU | 51(8) | - Medical | 107(18) | - 21–30 | 68(11) |
| - Other | 17(3) | - Other | 209(35) | - 31–40 | 113(19) |
| Stress reduced | - 41–50 | 156(26) | |||
| Safe vaccine | - yes | 283(47) | - 51–60 | 137(23) | |
| - yes | 507(84) | - no | 198(33) | - 61–70 | 81(14) |
| - no | 93(16) | - do not know | 119(20) | - Over 70 | 33(6) |
| Stress-causes | |||||
| □ Work | 203(48) | ||||
| Sex | Stress COVID | □ Pandemic | 183(43) | ||
| - male | 252(42) | - yes | 402(67) | □ COVID-19 (infection) | 152(36) |
| - female | 348(58) | - no | 198(33) | □ Childcare/School | 105(25) |
| Type of vaccine | □ Relationships | 92(22) | |||
| - None | 123(20) | □ Other | 54(12) | ||
| - pFizer-BioNtech | 180(30) | □ Finance | 46(11) | ||
| - Oxford-AstraZeneca | 290(48) | □ Studies/perf | 42(10) | ||
| - Other | 7(1) | □ Vaccine | 39(9) | ||
| Side effects of vaccine | |||||
| □ Tired | 228(47) | Shopping online | |||
| □ Muscle-Pain/Swell | 184(38) | Stress management | - yes | 396(66) | |
| □ Headache | 175(36) | □ Speak to family | 242(40) | - no | 204(24) |
| □ Chill/Aches | 166(34) | □ Watch TV, etc. | 203(34) | Social media time | |
| □ Fever | 106(22) | □ Engage in hobbies | 178(30) | - yes | 577(96) |
| □ None | 95(20) | □ No stress | 123(20) | - no | 23(4) |
| □ Strange feeling | 52(11) | □ Sports/games | 111(18) | Stress-shopping | |
| □ Nausea | 48(10) | □ Other | 83(14) | - yes | 350(58) |
| □ Dizziness | 36(8) | □ Social media use | 79(13) | - no | 250(42) |
| Accept vaccine | Concerns vaccine | 93 (15) | Future SOP | ||
| □ Yourself | 451(75) | □ Side effects | 70(67) | □ Mask wear | 328(55) |
| □ Children | 283(47) | □ Other | 33(32) | □ Social distance | 291(48) |
| □ Family | 483(80) | □ Personal beliefs | 15(14) | □ Tier response | 197(33) |
| □ None | 32(5) | □ Allergic | 9(8) | □ No restriction | 167(28) |
| □ Do not know | 37(6) | □ Needle-phobia | 4(4) | □ Lockdown | 81(13) |
| Childcare and School Closure | Work | Vaccine | Pandemic | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| X2 | Df | p-Value | X2 | df | p-Value | X2 | Df | p-Value | X2 | df | p-Value | |
| Ethnicity | 4.9 | 3 | 0.11 | 5.8 | 3 | 0.12 | 19 | 3 | 0.0002 | 4.5 | 3 | 0.21 |
| Age group | 88 | 6 | 2.2 × 10−16 | 38 | 6 | 9.4 × 10−7 | 11 | 6 | 0.08 | 12 | 6 | 0.06 |
| Sex | 5.3 | 1 | 0.02 | 1.8 | 1 | 0.17 | 0 | 1 | 1 | 5.7 | 1 | 0.01 |
| Profession | 3.6 | 2 | 0.12 | 15.6 | 2 | 0.0003 | 2.3 | 2 | 0.3 | 1.9 | 2 | 0.3 |
| Relationships | Stress_COVID | Finance | Studies/Performance | |||||||||
| Ethnicity | 6.9 | 3 | 0.07 | 6.9 | 3 | 0.07 | 18.4 | 3 | 0.0003 | 21 | 3 | 0.00001 |
| Age group | 10.4 | 6 | 0.1 | 16 | 6 | 0.01 | 11.7 | 6 | 0.06 | 45 | 6 | 4.2 × 10−8 |
| Gender | 1.9 | 1 | 0.15 | 21.4 | 1 | 3.5 × 10−6 | 0 | 1 | 1 | 0.8 | 1 | 0.3 |
| Profession | 0.6 | 2 | 0.7 | 17.6 | 2 | 0.0001 | 7.5 | 2 | 0.02 | 2.6 | 2 | 0.2 |
| Safe Vaccine | Vaccine Acceptance | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Yourself | Children | Family | None | |||||||
| X2 | p | X2 | p | X2 | P | X2 | p | X2 | p | |
| Age group | 22 | 0.0009 | 10 | 0.1 | 23 | 0.0005 | 7 | 0.34 | 9 | 0.16 |
| Sex | 0.01 | 0.91 | 13 | 0.7 | 0.8 | 0.35 | 3.8 | 0.05 | 0.1 | 0.7 |
| Profession | 12 | 0.002 | 20 | 4 × 10−5 | 20 | 3.7 × 10−5 | 19 | 6.3 × 10−5 | 9 | 0.01 |
| Ethnicity | 38 | 1 × 10−8 | 48 | 2 × 10−10 | 35 | 1.1 × 10−7 | 31 | 7.8 × 10−7 | 17 | 0.0007 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khan, W.; Khan, B.M.; Yasen, S.; Al-Dahiri, A.; Al-Jumeily, D.; Dajani, K.; Hussain, A. COVID-19 Vaccination and Mental Stress within Diverse Sociodemographic Groups. Int. J. Environ. Res. Public Health 2022, 19, 12932. https://doi.org/10.3390/ijerph191912932
Khan W, Khan BM, Yasen S, Al-Dahiri A, Al-Jumeily D, Dajani K, Hussain A. COVID-19 Vaccination and Mental Stress within Diverse Sociodemographic Groups. International Journal of Environmental Research and Public Health. 2022; 19(19):12932. https://doi.org/10.3390/ijerph191912932
Chicago/Turabian StyleKhan, Wasiq, Bilal M. Khan, Salwa Yasen, Ahmed Al-Dahiri, Dhiya Al-Jumeily, Khalil Dajani, and Abir Hussain. 2022. "COVID-19 Vaccination and Mental Stress within Diverse Sociodemographic Groups" International Journal of Environmental Research and Public Health 19, no. 19: 12932. https://doi.org/10.3390/ijerph191912932
APA StyleKhan, W., Khan, B. M., Yasen, S., Al-Dahiri, A., Al-Jumeily, D., Dajani, K., & Hussain, A. (2022). COVID-19 Vaccination and Mental Stress within Diverse Sociodemographic Groups. International Journal of Environmental Research and Public Health, 19(19), 12932. https://doi.org/10.3390/ijerph191912932