
Nutrition-Education-Based Interventions in Gestational Diabetes: A Scoping Review of Clinical Trials



Abstract
1. Introduction
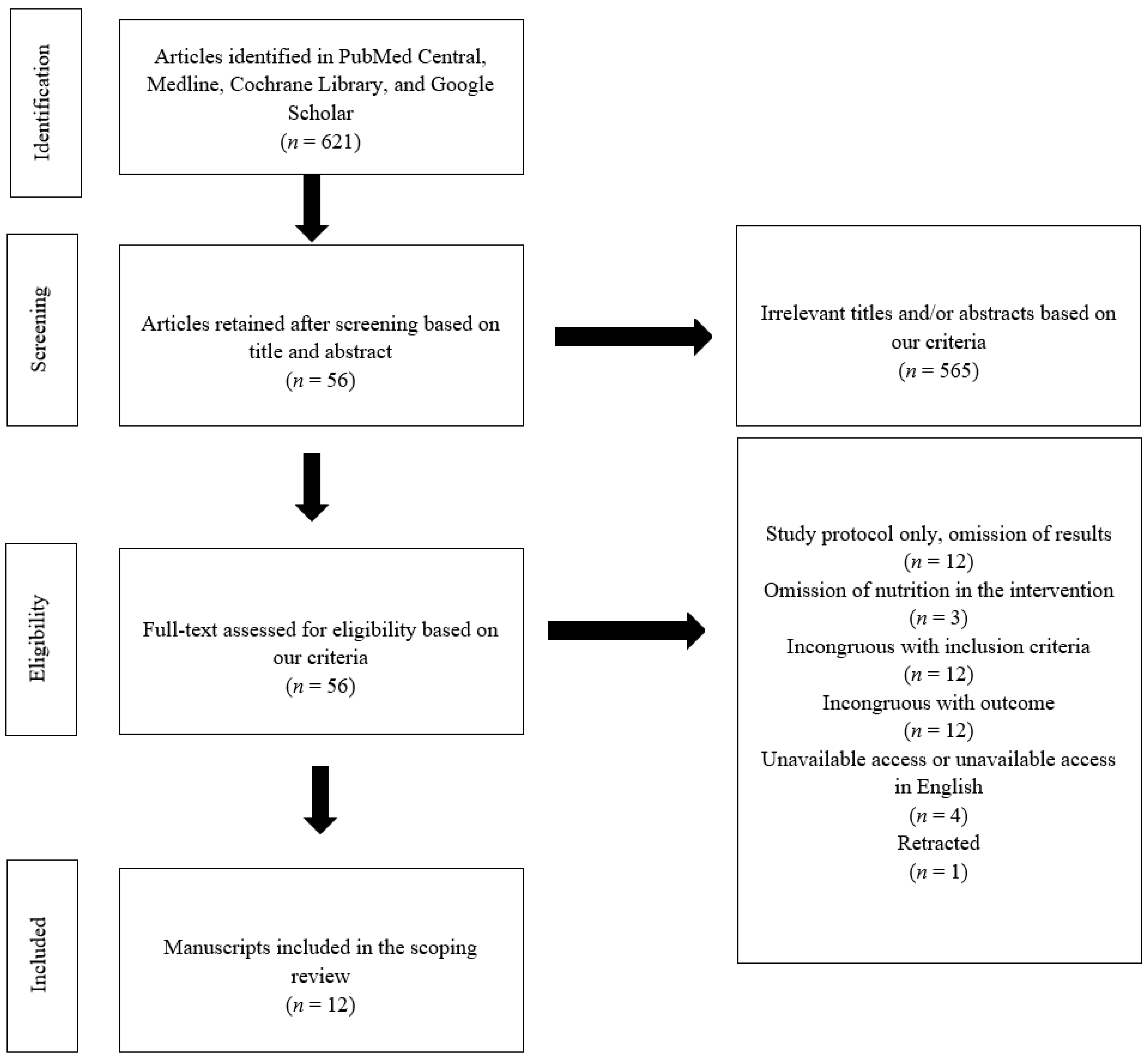
2. Materials and Methods
3. Results
3.1. Diabetes Self-Management Education
3.2. Medical Nutrition Therapy
4. Discussion and Conclusions
4.1. Discussion
4.2. Strengths and Limitations
4.3. Future Directions
4.4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K.; et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res. Clin. Pract. 2019, 157, 107843. [Google Scholar] [CrossRef] [PubMed]
- Yuen, L.; Saeedi, P.; Riaz, M.; Karuranga, S.; Divakar, H.; Levitt, N.; Yang, X.; Simmons, D. Projections of the prevalence of hyperglycaemia in pregnancy in 2019 and beyond: Results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res. Clin. Pract. 2019, 157, 107841. [Google Scholar] [CrossRef] [PubMed]
- Plows, J.F.; Stanley, J.L.; Baker, P.N.; Reynolds, C.M.; Vickers, M.H. The pathophysiology of gestational diabetes mellitus. Int. J. Mol. Sci. 2018, 19, 3342. [Google Scholar] [CrossRef]
- Sheiner, E. Gestational diabetes mellitus: Long-term consequences for the mother and child grand challenge: How to move on towards secondary prevention? Front. Clin. Diabetes Healthc. 2020, 1, 546256. [Google Scholar] [CrossRef]
- Mustafa, M.; Bogdanet, D.; Khattak, A.; Carmody, L.A.; Kirwan, B.; Gaffney, G.; O’Shea, P.M.; Dunne, F. Early gestational diabetes mellitus (GDM) is associated with worse pregnancy outcomes compared with GDM diagnosed at 24-28 weeks gestation despite early treatment. QJM 2021, 114, 17–24. [Google Scholar] [CrossRef]
- Franz, M.J.; Boucher, J.L.; Evert, A.B. Evidence-based diabetes nutrition therapy recommendations are effective: The key is individualization. Diabetes Metab. Syndr. Obes. Targets Ther. 2014, 7, 65–72. [Google Scholar] [CrossRef]
- Rasmussen, L.; Poulsen, C.W.; Kampmann, U.; Smedegaard, S.B.; Ovesen, P.G.; Fuglsang, J. Diet and healthy lifestyle in the management of gestational diabetes mellitus. Nutrients 2020, 12, 3050. [Google Scholar] [CrossRef]
- U.S. Department of Health and Human Services; National Institutes of Health. Managing Gestational Diabetes: A Patient’s Guide to a Healthy Pregnancy. Eunice Kennedy Shriver National Institute Child Health. 2004; pp. 2–49. Available online: https://www.nichd.nih.gov/sites/default/files/publications/pubs/Documents/managing_gestational_diabetes.pdf (accessed on 28 May 2022).
- Kapur, K.; Kapur, A.; Hod, M. Nutrition management of gestational diabetes mellitus. Ann. Nutr. Metab. 2020, 76, 17–29. [Google Scholar] [CrossRef] [PubMed]
- Vivanti, A.; Lewis, J.; O’Sullivan, T.A. The nutrition care process terminology: Changes in perceptions, attitudes, knowledge and implementation amongst Australian dietitians after three years. Nutr. Diet. 2018, 75, 87–97. [Google Scholar] [CrossRef] [PubMed]
- Griffith, R.J.; Alsweiler, J.; Moore, A.E.; Brown, S.; Middleton, P.; Shepherd, E.; Crowther, C.A. Diabetes mellitus: An overview of Cochrane Reviews (Review). Cochrane Database Syst. Rev. 2020, CD012394. [Google Scholar] [CrossRef]
- Chatterjee, S.; Davies, M.J.; Heller, S.; Speight, J.; Snoek, F.J.; Khunti, K. Diabetes structured self-management education programmes: A narrative review and current innovations. Lancet Diabetes Endocrinol. 2018, 6, 130–142. [Google Scholar] [CrossRef]
- National Institute of Health. NIH’s Definition of a Clinical Trial. NIH Grants & Funding. Available online: https://grants.nih.gov/policy/clinical-trials/definition.htm (accessed on 1 October 2022).
- Beck, J.; Greenwood, D.A.; Bollinger, S.T.; Condon, J.E.; Faulkner, P.; Francis, T.; Lavin-Tompkins, J.M.; Maryniuk, M.; Orzeck, E.A.; Reed, A.A.; et al. 2017 National standards for diabetes self-management education and support. Diabetes Care 2017, 40, 1409–1419. [Google Scholar] [CrossRef] [PubMed]
- He, R.; Lei, Q.; Hu, H.; Li, H.; Tian, D.; Lai, Z. The effect of health education combined with personalized psychological nursing intervention on pregnancy outcome of pregnant women with gestational diabetes mellitus. BioMed Res. Int. 2022, 2022, 3157986. [Google Scholar] [CrossRef]
- Tian, Y.; Zhang, S.; Huang, F.; Ma, L. Comparing the efficacies of telemedicine and standard prenatal care on blood glucose control in women with gestational diabetes mellitus: Randomized controlled trial. JMIR mHealth uHealth 2021, 9, 1–13. [Google Scholar] [CrossRef]
- Guo, Y.; Zhou, L.; Sun, B.; Wang, C.; Zhang, J. Application of online-offline integrated medical care management in patients with gestational diabetes. Ginekol. Pol. 2021, 92, 720–725. [Google Scholar] [CrossRef] [PubMed]
- Yew, T.W.; Chi, C.; Chan, S.-Y.; van Dam, R.M.; Whitton, C.; Lim, C.S.; Foong, P.S.; Fransisca, W.; Teoh, C.L.; Chen, J.; et al. A randomized controlled trial to evaluate the effects of a smartphone application–based lifestyle coaching program on gestational weight gain, glycemic control, and maternal and neonatal outcomes in women with gestational diabetes mellitus: The smart-gdm. Diabetes Care 2021, 44, 456–463. [Google Scholar] [CrossRef]
- Borgen, I.; Smastuen, M.C.; Jacobsen, A.F.; Garnweidner-Holme, L.M.; Fayyad, S.; Noll, J.; Lukasse, M. Effect of the pregnant+ smartphone application in women with gestational diabetes mellitus: A randomised controlled trial in Norway. BMJ Open 2019, 9, e030884. [Google Scholar] [CrossRef] [PubMed]
- Mohebbi, B.; Tol, A.; Sadeghi, R.; Mohtarami, S.F.; Shamshiri, A. Self-management intervention program based on the health belief model (Hbm) among women with gestational diabetes mellitus: A quazi-experimental study. Arch. Iran. Med. 2019, 22, 168–173. [Google Scholar] [PubMed]
- Kolivand, M.; Rahimi, M.A.; Keramat, A.; Shariati, M.; Emamian, M.H. Effect of a new self-care guide package on maternal and neonatal outcomes in gestational diabetes: A randomized control trial. J. Diabetes 2019, 11, 139–147. [Google Scholar] [CrossRef]
- Carolan-Olah, M.; Sayakhot, P. A randomized controlled trial of a web-based education intervention for women with gestational diabetes mellitus. Midwifery 2019, 68, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Durnwald, C.P.; Kallan, M.J.; Allison, K.C.; Sammel, M.D.; Wisch, S.; Elovitz, M.; Parry, S. A randomized clinical trial of an intensive behavior education program in gestational diabetes mellitus women designed to improve glucose levels on the 2-hour oral glucose tolerance test. Am. J. Perinatol. 2016, 33, 1145–1151. [Google Scholar] [CrossRef] [PubMed]
- Yuan, K.; Wang, H.; Chen, Y.; Li, S.; Wang, Q.; Cao, Y.; Gao, S.; Xu, X.; Xie, Q. A 12-hour comprehensive nutrition care benefits blood glucose level and weight gain and improves outcomes in pregnant women with gestational diabetes mellitus. Ann. Cardiothorac. Surg. 2020, 9, 661–670. [Google Scholar] [CrossRef] [PubMed]
- Lv, S.; Yu, S.; Chi, R.; Wang, D. Effects of nutritional nursing intervention based on glycemic load in patients with gestational diabetes mellitus. Ginekol. Pol. 2019, 90, 46–49. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Castilla, C.; Hernandez, M.; Bergua, M.; Alvarez, M.C.; Arce, M.A.; Rodriguez, K.; Martinez-Alonso, M.; Iglesias, M.; Mateu, M.; Santos, M.D.; et al. Low-carbohydrate diet for the treatment of gestational diabetes mellitus: A randomized controlled trial. Diabetes Care 2013, 36, 2233–2238. [Google Scholar] [CrossRef] [PubMed]
- Evert, A.B.; Dennison, M.; Gardner, C.D.; Garvey, W.T.; Lau, K.H.K.; MacLeod, J.; Mitri, J.; Pereira, R.F.; Rawlings, K.; Robinson, S.; et al. Nutrition therapy for adults with diabetes or prediabetes: A consensus report. Diabetes Care 2019, 42, 731–754. [Google Scholar] [CrossRef]
- Alvarado, F.L.; O’tierney-Ginn, P.; Catalano, P. Contribution of gestational weight gain on maternal glucose metabolism in women with GDM and normal glucose tolerance. J. Endocr. Soc. 2021, 5, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Wu, Y.; Miao, L. Study on the effects of individualized nutritional intervention on pregnancy outcome and neonatal immune function in patients with gestational diabetes mellitus. BioMed Res. Int. 2022, 2022, 3246784. [Google Scholar] [CrossRef]
- Shi, M.; Liu, Z.-L.; Steinmann, P.; Chen, J.; Chen, C.; Ma, X.-T.; Han, S.-H. Medical nutrition therapy for pregnant women with gestational diabetes mellitus—A retrospective cohort study. Taiwan. J. Obstet. Gynecol. 2016, 55, 666–671. [Google Scholar] [CrossRef]
- Ho, T.C.; Yan, Y.H.; Lu, M.C.; Yu, C.W.; Wang, P. Influence of medical nutrition therapy on borderline glucose intolerance in pregnant Taiwanese women. J. Matern. Neonatal Med. 2016, 29, 1181–1186. [Google Scholar] [CrossRef] [PubMed]
- Schnell, O.; Alawi, H.; Battelino, T.; Ceriello, A.; Diem, P.; Felton, A.-M.; Grzeszczak, W.; Harno, K.; Kempler, P.; Satman, I. Self-monitoring of blood glucose in type 2 diabetes: Recent studies. J. Diabetes Sci. Technol. 2013, 7, 478–488. [Google Scholar] [CrossRef]
- Sankar, U.; Fisher, L.; Schillinger, D. Is self-efficacy associated with diabetes self-management across race/ethnicity and health literacy? Diabetes Care 2006, 29, 823–829. [Google Scholar] [CrossRef] [PubMed]
- Al-Hashmi, I.; Hodge, F.; Nandy, K.; Thomas, E.; Brecht, M. The effect of a self-efficacy-enhancing intervention on perceived self-efficacy and actual adhereance to healthy behaviours among women with gestational diabetes mellitus. Sultan Qaboos Univ. Med. J. 2018, 18, e513–e519. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.N.; Kalsoom, S.; Khan, A.A. Food exchange list and dietary management of non-communicable diseases in cultural perspective. Pak. J. Med. Sci. 2017, 33, 1273–1278. [Google Scholar] [CrossRef] [PubMed]
- Yuen, L.; Wong, V.W. Gestational diabetes mellitus: Challenges for different ethnic groups. World J. Diabetes 2015, 6, 1024–1032. [Google Scholar] [CrossRef]
- Franzago, M.; Fraticelli, F.; Stuppia, L.; Vitacolonna, E. Nutrigenetics, epigenetics and gestational diabetes: Consequences in mother and child. Epigenetics 2019, 14, 215–235. [Google Scholar] [CrossRef]
- Dabelea, D.; Mayer-Davis, E.J.; Lamichhane, A.P.; D’Agostino, R.B., Jr.; Liese, A.D.; Vehik, K.S.; Narayan, K.M.V.; Zeitler, P.; Hamman, R.F. Association of intrauterine exposure to maternal diabetes and obesity with type 2 diabetes in youth: The SEARCH case-control study. Diabetes Care 2008, 31, 1422–1426. [Google Scholar] [CrossRef]
- Jiang, Y.; Yu, Y.C.; Ding, G.L.; Gao, Q.; Chen, F.; Luo, Q. Intrauterine hyperglycemia induces intergenerational Dlk1-Gtl2 methylation changes in mouse placenta. Oncotarget 2018, 9, 22398–22405. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Author, Year (Country) | Study Design | Gestational Age at Intervention | DSME Intervention | Nutrition Education Content of DSME | Assessment of Clinical Endpoints |
|---|---|---|---|---|---|
| He et al., 2022 (China) [15] | RCT (n = 170) | 28.3 ± 4 wks | Structured HE; exercise; BG self-monitoring; personalized psychological nursing; PA | Low-fat, high-fiber, low-glycemic diet | ↓ 2hPPG, FPG |
| Tian et al., 2021 (China) [16] | RCT (n = 269) | 23–30 wks | Weekly management/HE messages through WeChat; BG self-monitoring; PA | Increasing food diversity, high-fiber cereals; recipes; photos of meals; PA | ↑ BG control |
| Guo et al., 2021 (China) [17] | RCT (n = 140) | 26.7 ± 3 wks | Integrated doctor and nurse communication; WeChat HE communication for families and patients; PA | Five to six meals/day; avoid high sugar, oil and fat; avoid a spicy diet; prioritize F/V | ↓ 2hPPG, FPG ↑ self-management ability |
| Yew et al., 2021 (Singapore) [18] | RCT (n = 333) | 27 ± 3.2 wks | Structured HE based on HBM; smartphone app with more detailed dietary/PA guidance | CHO and kcal amounts of culturally relevant foods | ↓ proportion of BG above targets |
| Borgen et al., 2019 (Norway) [19] | RCT (n = 233) | <33 wks | Structured HE; exercise; BG self-monitoring; smartphone app with more detailed diet/PA recommendations, feedback on BG | Culturally adapted diet suggestions; limited sugar; increased WG, F/V; small meals | ∅ |
| Mohebbi et al., 2019 (Iran) [20] | RCT, quazi-experimental (n = 110) | Not provided | Structured HE based on HBM; BG self-monitoring; phone call reminders; motivational interviewing | Healthy diet | ↓ HbA1c |
| Kolivand et al., 2019 (Iran) [21] | RCT (n = 151) | 26.7 ± 5 wks | Structured HE up to 34 wks GA; self-care guidebook, log book; educational DVDs; stress reduction; PA; BG self-monitoring | Nutrition assessment and control | ↓ 2hPPG |
| Carolan-Olah et al., 2019 (Australia) [22] | RCT (n = 110) | 28–32 wks | Structured HE; web-access to HE with quizzes; healthy habits, lifestyle; emotions; BG self-monitoring | Healthy food choices; healthy shopping; increase V; identify sugar | ↓ BMI, SBP, glycemic level |
| Durnwald et al., 2016 (United States) [23] | RCT (n = 101) | 30.8 ± 2 wks | Structured behavioral modification HE; motivational messaging; weekly phone call review; pedometer for PA; BG self-monitoring | ADA dietary guidelines; nutritional facts | ∅ |
| Author, Year (Country) | Study Design | Gestational Age at Intervention | MNT Intervention | Assessment of Clinical Endpoints |
|---|---|---|---|---|
| Yuan et al., 2020 (China) [24] | RCT (n = 312) | 24–28 wks | 12 h comprehensive nutrition care process; five meals individualized to personal needs over 12 h; education on food exchange method and calorie counting | ↓ 2hPPG, FPG, GWG, incidence of complications |
| Lv et al., 2019 (China) [25] | RCT (n = 134) | 35 wks | Personalized diet based on ideal weight, actual weight gain, eating habits; education based on blood glycemic load | ↓ 2hPPG, FPG; ∅ incidence of complications |
| Moreno-Castilla et al., 2013 (Spain) [26] | RCT (n = 130) | 30.4 ± 3 wks | Caloric intake calculated based on pre-pregnancy body weight; 20% PRO, 40% CHO, 40% fat; design of three meals and three snacks per day divided by CHO distribution | ∅ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Helm, M.M.; Izuora, K.; Basu, A. Nutrition-Education-Based Interventions in Gestational Diabetes: A Scoping Review of Clinical Trials. Int. J. Environ. Res. Public Health 2022, 19, 12926. https://doi.org/10.3390/ijerph191912926
Helm MM, Izuora K, Basu A. Nutrition-Education-Based Interventions in Gestational Diabetes: A Scoping Review of Clinical Trials. International Journal of Environmental Research and Public Health. 2022; 19(19):12926. https://doi.org/10.3390/ijerph191912926
Chicago/Turabian StyleHelm, Macy M., Kenneth Izuora, and Arpita Basu. 2022. "Nutrition-Education-Based Interventions in Gestational Diabetes: A Scoping Review of Clinical Trials" International Journal of Environmental Research and Public Health 19, no. 19: 12926. https://doi.org/10.3390/ijerph191912926
APA StyleHelm, M. M., Izuora, K., & Basu, A. (2022). Nutrition-Education-Based Interventions in Gestational Diabetes: A Scoping Review of Clinical Trials. International Journal of Environmental Research and Public Health, 19(19), 12926. https://doi.org/10.3390/ijerph191912926