
COVID-19 Vaccination Acceptance in the Context of the Health Belief Model: Comparative Cross-Sectional Study in Punjab, Pakistan

 , ,
, , 
Abstract
1. Introduction
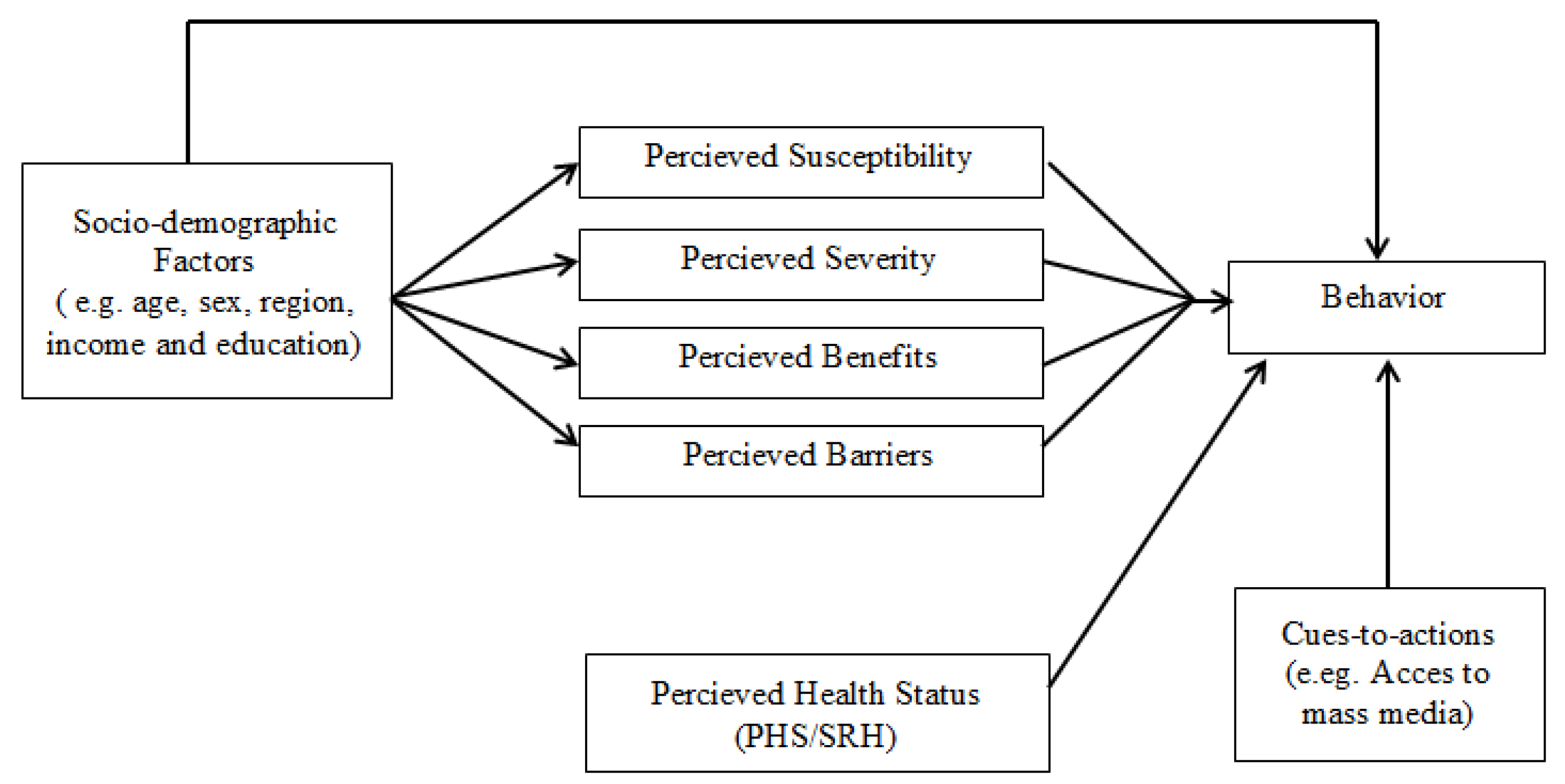
2. Health Belief Model
3. Materials and Methods
3.1. Study Design
3.2. Measures
3.3. Statistical Analysis
3.4. Ethical Considerations
4. Results
4.1. Characteristics of Study Participants
4.2. HBM and Vaccination Status
5. Discussion
6. Conclusions
6.1. Future Research
6.2. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- The Fastest Vaccine in History. Available online: https://connect.uclahealth.org/2020/12/10/the-fastest-vaccine-in-history/ (accessed on 14 December 2021).
- Reiter, P.L.; Pennell, M.L.; Katz, M.L. Acceptability of a COVID-19 vaccine among adults in the United States: How many people would get vaccinated? Vaccine 2020, 38, 6500–6507. [Google Scholar] [CrossRef]
- Dror, A.A.; Eisenbach, N.; Taiber, S.; Morozov, N.G.; Mizrachi, M.; Zigron, A.; Srouji, S.; Sela, E. Vaccine hesitancy: The next challenge in the fight against COVID-19. Eur. J. Epidemiol. 2020, 35, 775–779. [Google Scholar] [CrossRef] [PubMed]
- Machingaidze, S.; Wiysonge, C.S. Understanding COVID-19 vaccine hesitancy. Nat. Med. 2021, 27, 1338–1339. [Google Scholar] [CrossRef] [PubMed]
- Murphy, J.; Vallières, F.; Bentall, R.P.; Shevlin, M.; McBride, O.; Hartman, T.K.; McKay, R.; Bennett, K.; Mason, L.; Gibson-Miller, J.; et al. Psychological characteristics associated with COVID-19 vaccine hesitancy and resistance in Ireland and the United Kingdom. Nat. Commun. 2021, 12, 29. [Google Scholar] [CrossRef] [PubMed]
- Razai, M.S.; Osama, T.; McKechnie, D.G.; Majeed, A. COVID-19 vaccine hesitancy among ethnic minority groups. BMJ 2021, 372, n513. [Google Scholar] [CrossRef]
- Lucia, V.C.; Kelekar, A.; Afonso, N.M. COVID-19 vaccine hesitancy among medical students. J. Public Health 2021, 43, 445–449. [Google Scholar] [CrossRef] [PubMed]
- Chou, W.Y.; Budenz, A. Considering emotion in COVID-19 vaccine communication: Addressing vaccine hesitancy and fostering vaccine confidence. Health Commun. 2020, 35, 1718–1722. [Google Scholar] [CrossRef]
- Soares, P.; Rocha, J.V.; Moniz, M.; Gama, A.; Laires, P.A.; Pedro, A.R.; Dias, S.; Leite, A.; Nunes, C. Factors associated with COVID-19 vaccine hesitancy. Vaccines 2021, 9, 300. [Google Scholar] [CrossRef]
- Omer, S.B.; Salmon, D.A.; Orenstein, W.A.; DeHart, M.P.; Halsey, N. Vaccine refusal, mandatory immunization, and the risks of vaccine-preventable diseases. N. Engl. J. Med. 2009, 360, 1981–1988. [Google Scholar] [CrossRef]
- Okmi, E.A.; Almohammadi, E.; Alaamri, O.; Alfawaz, R.; Alomari, N.; Alnughaymishi, M.S.; Alsuwailem, S.; Moafa, N.J. Determinants of COVID-19 vaccine acceptance among the general adult population in Saudi Arabia based on the health belief model: A web-based cross-sectional study. Cureus 2022, 14, e28326. [Google Scholar] [CrossRef]
- Stein, J.; Bennett, D.; Coen, C.; Dunbar, R.; Goodwin, G.; Husain, M.; Mann, E.; Morris, J.; Rolls, E.; Taylor, J.S.; et al. The curated reference collection in neuroscience and biobehavioral psychology. Exp. Psychol. 2017, 1, 674. [Google Scholar]
- Kim, S.; Kim, S. Analysis of the impact of health beliefs and resource factors on preventive behaviors against the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 8666. [Google Scholar] [CrossRef] [PubMed]
- Janz, N.K.; Becker, M.H. The health belief model: A decade later. Health Educ. Q 1984, 11, 1–47. [Google Scholar] [CrossRef]
- Carpenter, C.J. A meta-analysis of the effectiveness of health belief model variables in predicting behavior. Health Commun. 2010, 25, 661–669. [Google Scholar] [CrossRef] [PubMed]
- Harrison, J.A.; Mullen, P.D.; Green, L.W. A meta-analysis of studies of the health belief model with adults. Health Educ. Res. 1992, 7, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Santos, A.J.; Kislaya, I.; Machado, A.; Nunes, B. Beliefs and attitudes towards the influenza vaccine in high-risk individuals. Epidemiol. Infect. 2017, 145, 1786–1796. [Google Scholar] [CrossRef] [PubMed]
- Teitler-Regev, S.; Shahrabani, S.; Benzion, U. Factors affecting intention among students to be vaccinated against A/H1N1 influenza: A health belief model approach. Adv. Prev. Med. 2011, 2011, 353207. [Google Scholar] [CrossRef]
- Zampetakis, L.A.; Melas, C. The health belief model predicts vaccination intentions against COVID-19: A survey experiment approach. Appl. Psychol. Health Well-Being 2021, 13, 469–484. [Google Scholar] [CrossRef]
- Williams, G.; Di Nardo, F.; Verma, A. The relationship between self-reported health status and signs of psychological distress within European urban contexts. Eur. J. Public Health 2017, 27, 68–73. [Google Scholar] [CrossRef]
- Miilunpalo, S.; Vuori, I.; Oja, P.; Pasanen, M.; Urponen, H. Self-rated health status as a health measure: The predictive value of self-reported health status on the use of physician services and on mortality in the working-age population. J. Clin. Epidemiol. 1997, 50, 517–528. [Google Scholar] [CrossRef]
- Orji, R.; Vassileva, J.; Mandryk, R. Towards an effective health interventions design: An extension of the health belief model. Online J. Public Health Inform. 2012, 4, 3. [Google Scholar] [CrossRef] [PubMed]
- Glanz, K.; Rimer, B.K.; Viswanath, K. (Eds.) Health Behavior and Health Education: Theory, Research, and Practice; John Wiley & Sons: Hoboken, NJ, USA, 28 August 2008. [Google Scholar]
- Hossain, M.B.; Alam, M.Z.; Islam, M.S.; Sultan, S.; Faysal, M.M.; Rima, S.; Hossain, M.A.; Mamun, A.A. Health belief model, theory of planned behavior, or psychological antecedents: What predicts COVID-19 vaccine hesitancy better among the Bangladeshi adults? Front. Public Health 2021, 9, 711066. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Li, X.; Gao, J.; Liu, X.; Mao, Y.; Wang, R.; Zheng, P.; Xiao, Q.; Jia, Y.; Fu, H.; et al. Health belief model perspective on the control of COVID-19 vaccine hesitancy and the promotion of vaccination in china: Web-based cross-sectional study. J. Med. Internet Res. 2021, 23, e29329. [Google Scholar] [CrossRef] [PubMed]
- Marschalko, E.E.; Szabo, K.; Kotta, I.; Kalcza-Janosi, K. The role of positive and negative information processing in COVID-19 vaccine uptake in women of generation X, Y, and Z: The power of good is stronger than bad in youngsters? Front. Psychol. 2022, 13, 925675. [Google Scholar] [CrossRef] [PubMed]
- Wong, L.P.; Alias, H.; Wong, P.F.; Lee, H.Y.; AbuBakar, S. The use of the health belief model to assess predictors of intent to receive the COVID-19 vaccine and willingness to pay. Hum. Vaccines Immunother. 2020, 16, 2204–2214. [Google Scholar] [CrossRef] [PubMed]
- Patwary, M.M.; Bardhan, M.; Disha, A.S.; Hasan, M.; Haque, M.Z.; Sultana, R.; Hossain, M.R.; Browning, M.M.; Alam, M.A.; Sallam, M. Determinants of COVID-19 vaccine acceptance among the adult population of Bangladesh using the health belief model and the theory of planned behavior model. Vaccines 2021, 9, 1393. [Google Scholar] [CrossRef]
- Ahmed, T.F.; Ahmed, A.; Ahmed, S.; Ahmed, H.U. Understanding COVID-19 vaccine acceptance in Pakistan: An echo of previous immunizations or prospect of change? Expert Rev. Vaccines 2021, 20, 1185–1193. [Google Scholar] [CrossRef]
- Limbu, Y.B.; Gautam, R.K.; Pham, L. The Health Belief Model Applied to COVID-19 Vaccine Hesitancy: A Systematic Review. Vaccines 2022, 10, 973. [Google Scholar] [CrossRef]
- OECD Health Data. Statistics and Indicators for 30 Countries; OECD: Paris, France, 2007. [Google Scholar]
- Coe, A.B.; Gatewood, S.B.; Moczygemba, L.R. The use of the health belief model to assess predictors of intent to receive the novel (2009) H1N1 influenza vaccine. Innov. Pharm. 2012, 3, 1. [Google Scholar] [CrossRef]
- Fall, E.; Izaute, M.; Chakroun-Baggioni, N. How can the health belief model and self-determination theory predict both influenza vaccination and vaccination intention? A longitudinal study among university students. Psychol. Health 2018, 33, 746–764. [Google Scholar] [CrossRef]
- Tong, K.K.; Chen, J.H.; Yu, E.W.; Wu, A.M. Adherence to COVID?19 precautionary measures: Applying the health belief model and generalised social beliefs to a probability community sample. Appl. Psychol. Health Well-Being 2020, 12, 1205–1223. [Google Scholar] [CrossRef] [PubMed]
- Fathian-Dastgerdi, Z.; Tavakoli, B.; Jaleh, M. Factors associated with preventive behaviors of COVID-19 among adolescents: Applying the health belief model. Res. Soc. Adm. Pharm. 2021, 18, 1786–1790. [Google Scholar] [CrossRef] [PubMed]
- Shmueli, L. Predicting intention to receive COVID-19 vaccine among the general population using the health belief model and the theory of planned behavior model. BMC Public Health 2021, 21, 804. [Google Scholar] [CrossRef] [PubMed]
- Wong, M.C.; Wong, E.L.; Huang, J.; Cheung, A.W.; Law, K.; Chong, M.K.; Ng, R.W.; Lai, C.K.; Boon, S.S.; Lau, J.T.; et al. Acceptance of the COVID-19 vaccine based on the health belief model: A population-based survey in Hong Kong. Vaccine 2021, 39, 1148–1156. [Google Scholar] [CrossRef] [PubMed]
- Mercadante, A.R.; Law, A.V. Will they, or Won’t they? Examining patients’ vaccine intention for flu and COVID-19 using the Health Belief Model. Res. Soc. Adm. Pharm. 2021, 17, 1596–1605. [Google Scholar] [CrossRef]
- Shah, G.H.; Faraz, A.A.; Khan, H.; Waterfield, K.C. Perceived benefits matter the most in COVID-19 preventive behaviors: Empirical evidence from Okara District, Pakistan. Int. J. Environ. Res. Public Health 2021, 18, 6772. [Google Scholar] [CrossRef] [PubMed]
- Yan, E.; Lai, D.W.; Lee, V.W. Predictors of intention to vaccinate against COVID-19 in the general public in Hong Kong: Findings from a population-based, cross-sectional survey. Vaccines 2021, 9, 696. [Google Scholar] [CrossRef]
- Sallam, M.; Dababseh, D.; Eid, H.; Al-Mahzoum, K.; Al-Haidar, A.; Taim, D.; Yaseen, A.; Ababneh, N.A.; Bakri, F.G.; Mahafzah, A. High rates of COVID-19 vaccine hesitancy and its association with conspiracy beliefs: A study in Jordan and Kuwait among other Arab countries. Vaccines 2021, 9, 42. [Google Scholar] [CrossRef]
- Detoc, M.; Bruel, S.; Frappe, P.; Tardy, B.; Botelho-Nevers, E.; Gagneux-Brunon, A. Intention to participate in a COVID-19 vaccine clinical trial and to get vaccinated against COVID-19 in France during the pandemic. Vaccine 2020, 38, 7002–7006. [Google Scholar] [CrossRef]
- Fisher, K.A.; Bloomstone, S.J.; Walder, J.; Crawford, S.; Fouayzi, H.; Mazor, K.M. Attitudes toward a potential SARS-CoV-2 vaccine: A survey of US adults. Ann. Intern. Med. 2020, 173, 964–973. [Google Scholar] [CrossRef]
- Kwok, K.O.; Li, K.K.; Wei, W.I.; Tang, A.; Wong, S.Y.; Lee, S.S. Influenza vaccine uptake, COVID-19 vaccination intention and vaccine hesitancy among nurses: A survey. Int. J. Nurs. Stud. 2021, 114, 103854. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2021, 27, 225–228. [Google Scholar] [CrossRef] [PubMed]
- Malik, A.A.; McFadden, S.M.; Elharake, J.; Omer, S.B. Determinants of COVID-19 vaccine acceptance in the US. EClinicalMedicine 2020, 26, 100495. [Google Scholar] [CrossRef] [PubMed]
- Taylor, S.; Landry, C.A.; Paluszek, M.M.; Groenewoud, R.; Rachor, G.S.; Asmundson, G.J. A proactive approach for managing COVID-19: The importance of understanding the motivational roots of vaccination hesitancy for SARS-CoV2. Front. Psychol. 2020, 11, 2890. [Google Scholar] [CrossRef]
- Freeman, D.; Loe, B.S.; Chadwick, A.; Vaccari, C.; Waite, F.; Rosebrock, L.; Jenner, L.; Petit, A.; Lewandowsky, S.; Vanderslott, S.; et al. COVID-19 vaccine hesitancy in the UK: The Oxford coronavirus explanations, attitudes, and narratives survey (Oceans) II. Psychol. Med. 2020, 1–15. [Google Scholar] [CrossRef]
- Rhodes, A.; Hoq, M.; Measey, M.A.; Danchin, M. Intention to vaccinate against COVID-19 in Australia. Lancet Infect. Dis. 2021, 21, e110. [Google Scholar] [CrossRef]
- Chaudhary, F.A.; Ahmad, B.; Khalid, M.D.; Fazal, A.; Javaid, M.M.; Butt, D.Q. Factors influencing COVID-19 vaccine hesitancy and acceptance among the Pakistani population. Hum. Vaccines Immunother. 2021, 17, 3365–3370. [Google Scholar] [CrossRef]
- Lin, Y.; Hu, Z.; Zhao, Q.; Alias, H.; Danaee, M.; Wong, L.P. Understanding COVID-19 vaccine demand and hesitancy: A nationwide online survey in China. PLoS Negl. Trop. Dis. 2020, 14, e0008961. [Google Scholar] [CrossRef]
- Wang, K.; Wong, E.L.; Ho, K.F.; Cheung, A.W.; Chan, E.Y.; Yeoh, E.K.; Wong, S.Y. Intention of nurses to accept coronavirus disease 2019 vaccination and change of intention to accept seasonal influenza vaccination during the coronavirus disease 2019 pandemic: A cross-sectional survey. Vaccine 2020, 38, 7049–7056. [Google Scholar] [CrossRef]
- Magadmi, R.M.; Kamel, F.O. Beliefs and barriers associated with COVID-19 vaccination among the general population in Saudi Arabia. BMC Public Health 2021, 21, 1438. [Google Scholar] [CrossRef]
- Sarasty, O.; Carpio, C.E.; Hudson, D.; Guerrero-Ochoa, P.A.; Borja, I. The demand for a COVID-19 vaccine in Ecuador. Vaccine 2020, 38, 8090–8098. [Google Scholar] [CrossRef] [PubMed]
- Reno, C.; Maietti, E.; Fantini, M.P.; Savoia, E.; Manzoli, L.; Montalti, M.; Gori, D. Enhancing COVID-19 Vaccines Acceptance: Results from a Survey on Vaccine Hesitancy in Northern Italy. Vaccines 2021, 9, 378. [Google Scholar] [CrossRef] [PubMed]
- Sherman, S.M.; Smith, L.E.; Sim, J.; Amlôt, R.; Cutts, M.; Dasch, H.; Rubin, G.J.; Sevdalis, N. COVID-19 vaccination intention in the UK: Results from the COVID-19 vaccination acceptability study (CoVAccS), a nationally representative cross-sectional survey. Hum. Vaccines Immunother. 2021, 17, 1612–1621. [Google Scholar] [CrossRef] [PubMed]
- Gagneux-Brunon, A.; Detoc, M.; Bruel, S.; Tardy, B.; Rozaire, O.; Frappe, P.; Botelho-Nevers, E. Intention to get vaccinations against COVID-19 in French healthcare workers during the first pandemic wave: A cross-sectional survey. J. Hosp. Infect. 2021, 108, 168–173. [Google Scholar] [CrossRef] [PubMed]
- Qunaibi, E.; Basheti, I.; Soudy, M.; Sultan, I. Hesitancy of Arab healthcare workers towards COVID-19 vaccination: A Large-Scale multinational study. Vaccines 2021, 9, 446. [Google Scholar] [CrossRef]
- Zakar, R.; Zakar, M.Z.; Qureshi, S.; Fischer, F. Harnessing information technology to improve women’s health information: Evidence from Pakistan. BMC Women’s Health 2014, 14, 105. [Google Scholar] [CrossRef]
- Khalafzai, A.K.; Nirupama, N. Building resilient communities through empowering women with information and communication technologies: A Pakistan case study. Sustainability 2011, 3, 82–96. [Google Scholar] [CrossRef]
- Chib, A.; Chen, V.H. Midwives with mobiles: A dialectical perspective on gender arising from technology introduction in rural Indonesia. New Media Soc. 2011, 13, 486–501. [Google Scholar] [CrossRef]
- World Bank. Rural Population—Pakistan. Available online: https://data.worldbank.org/indicator/SP.RUR.TOTL.ZS?locations=PK (accessed on 14 December 2021).


{kind=link}
| Characteristics | n 1 | % |
|---|---|---|
| Vaccination status | ||
| Vaccinated | 795 | 60.0 |
| Not Vaccinated | 530 | 40.0 |
| Sex | ||
| Male | 972 | 73.4 |
| Female | 353 | 26.6 |
| Age (in years) | ||
| 40–49 | 646 | 48.8 |
| 50–59 | 421 | 31.8 |
| 60–69 | 192 | 14.5 |
| 70–79 | 52 | 3.9 |
| 80+ | 14 | 1.1 |
| Mean age (in years) ± SD | 51.2 ± 9.34 | |
| Area of residence | ||
| Rural | 266 | 20.2 |
| Urban | 1024 | 77.7 |
| Semi-urban | 28 | 2.1 |
| Religion | ||
| Islam | 1270 | 96.1 |
| Christianity | 51 | 3.9 |
| Others | 1 | 0.1 |
| Monthly household income | ||
| ≤PKR 20,000 | 355 | 30.3 |
| PKR 20,001–50,000 | 525 | 44.7 |
| PKR 50,001–100,000 | 201 | 17.1 |
| >PKR 100,000 | 92 | 7.8 |
| Marital status | ||
| Currently married | 1234 | 94.1 |
| Not currently married 2 | 78 | 5.9 |
| Number of children | ||
| 0 | 40 | 3.2 |
| 1–2 | 289 | 23.0 |
| 3–4 | 603 | 48.0 |
| 5 and above | 325 | 25.9 |
| Highest level of education | ||
| No formal education | 223 | 16.9 |
| Primary (1–5 years) | 109 | 8.3 |
| Middle (6–10 years) | 474 | 36.0 |
| Secondary (11–12 years) | 168 | 12.8 |
| Higher (13 years and above) | 343 | 26.0 |
| Employment status | ||
| Employed | 853 | 65.1 |
| Not employed 3 | 458 | 34.9 |
| Access to mass media | ||
| No access | 42 | 3.2 |
| Low access 4 | 235 | 17.8 |
| Moderate access 5 | 478 | 36.3 |
| High access 6 | 562 | 42.7 |
| Characteristics | COVID-19-Related Knowledge | OR (95% CI) | p-Value | AOR (95% CI) | p-Value | |||
|---|---|---|---|---|---|---|---|---|
| Poor | Good | |||||||
| n | % | n | % | |||||
| Sex | ||||||||
| Male | 403 | 42.2 | 553 | 57.8 | 1 | 1 | ||
| Female | 165 | 57.8 | 187 | 42.2 | 0.82 (0.64–1.05) | 0.12 | 0.68 (0.46–1.01) | 0.05 |
| Age (in years) | ||||||||
| 40–49 | 277 | 43.6 | 359 | 56.4 | 1 | 1 | ||
| 50–59 | 172 | 41.3 | 244 | 58.7 | 1.09 (0.85–1.40) | 0.47 | 1.10 (0.82–1.46) | 0.51 |
| 60–69 | 85 | 44.5 | 106 | 55.5 | 0.96 (0.69–1.33) | 0.81 | 1.07 (0.72–1.59) | 0.71 |
| 70–79 | 25 | 49.0 | 26 | 51.0 | 0.80 (0.45–1.42) | 0.45 | 1.41 (0.67–2.96) | 0.35 |
| 80+ | 9 | 64.3 | 5 | 35.7 | 0.42 (0.14–1.29) | 0.13 | 0.70 (0.19–2.57) | 0.59 |
| Area of residence | ||||||||
| Rural | 146 | 55.5 | 117 | 44.5 | 1 | 1 | ||
| Urban | 409 | 40.4 | 603 | 59.6 | 1.84 (1.39–2.41) | <0.01 * | 1.40 (1.02–1.92) | 0.03 * |
| Semi-urban | 11 | 39.3 | 17 | 60.7 | 1.92 (0.87–4.27) | 0.10 | 1.88 (0.74–4.74) | 0.17 |
| Monthly household income | ||||||||
| ≤PKR 20,000 | 186 | 53.0 | 165 | 47.0 | 1 | 1 | ||
| PKR 20,001–50,000 | 217 | 41.7 | 303 | 58.3 | 1.57 (1.19–2.06) | <0.01 * | 1.32 (0.97–1.77) | 0.06 |
| PKR 50,001–100,000 | 78 | 39.0 | 122 | 61.0 | 1.76 (1.23–2.51) | <0.01 * | 1.08 (0.71–1.64) | 0.70 |
| >PKR 100,000 | 37 | 40.7 | 54 | 59.3 | 1.64 (1.03–2.62) | 0.03 * | 0.97 (0.56–1.67) | 0.92 |
| Marital status | ||||||||
| Not currently married | 46 | 59.0 | 32 | 41.0 | 1 | 1 | ||
| Currently married | 519 | 42.5 | 702 | 57.5 | 1.94 (1.22–3.09) | <0.01 * | 2.03 (1.02–4.03) | 0.04 * |
| Number of children | ||||||||
| 0 | 21 | 52.5 | 19 | 47.5 | 1 | 1 | ||
| 1–2 | 113 | 39.5 | 173 | 60.5 | 1.69 (0.87–3.28) | 0.12 | 2.30 (1.04–5.08) | 0.03 * |
| 3–4 | 248 | 41.5 | 350 | 58.5 | 1.56 (0.82–2.96) | 0.17 | 3.03 (0.94–4.39) | 0.06 |
| 5 and above | 159 | 49.7 | 161 | 50.3 | 1.11 (0.58–2.16) | 0.73 | 1.62 (0.73–3.57) | 0.23 |
| Highest level of education | ||||||||
| No formal education | 136 | 61.8 | 84 | 38.2 | 1 | 1 | ||
| Primary | 56 | 51.4 | 53 | 48.6 | 1.53 (0.96–2.43) | 0.07 | 1.46 (0.88–2.42) | 0.14 |
| Middle | 190 | 40.7 | 277 | 59.3 | 2.36 (1.69–3.27) | <0.01 * | 1.82 (1.24–2.68) | <0.01 * |
| Secondary | 75 | 44.9 | 92 | 55.1 | 1.98 (1.32–2.99) | <0.01 * | 1.44 (0.87–2.38) | 0.15 |
| Higher | 107 | 31.7 | 231 | 68.3 | 3.49 (2.44–4.98) | <0.01 * | 2.36 (1.45–3.83) | <0.01 * |
| Employment status | ||||||||
| Not employed | 209 | 45.7 | 248 | 54.3 | 1 | 1 | ||
| Employed | 357 | 42.6 | 482 | 57.4 | 1.13 (0.90–1.43) | 0.27 | 0.79 (0.54–1.13) | 0.20 |
| Access to mass media | ||||||||
| No access | 26 | 61.9 | 16 | 38.1 | 1 | 1 | ||
| Low access | 119 | 51.1 | 114 | 48.9 | 1.55 (0.79–3.05) | 0.19 | 1.27 (0.61–2.64) | 0.51 |
| Moderate access | 222 | 47.2 | 248 | 52.8 | 1.81 (0.94–3.47) | 0.07 | 1.22 (0.60–2.49) | 0.58 |
| High access | 199 | 35.8 | 357 | 64.2 | 2.91 (1.52–5.56) | <0.01 * | 1.59 (0.76–3.32) | 0.21 |
| Dimensions of Health Belief Model | Total | Vaccinated | Not Vaccinated | OR (95% CI) | p-Value | |||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |||
| P-SUS | ||||||||
| Yes | 874 | 66.1 | 575 | 72.6 | 299 | 56.4 | 2.05 (1.62–2.58) | <0.01 * |
| No | 448 | 33.9 | 217 | 27.4 | 231 | 43.6 | 1 | |
| P-SEV | ||||||||
| Yes | 930 | 70.8 | 586 | 74.6 | 344 | 65.0 | 1.58 (1.25–2.01) | <0.01 * |
| No | 384 | 29.2 | 199 | 25.4 | 185 | 35.0 | 1 | |
| P-BEN | ||||||||
| Yes | 896 | 67.8 | 649 | 81.9 | 247 | 46.7 | 5.18 (4.04–6.65) | <0.01 * |
| No | 425 | 32.2 | 143 | 18.1 | 282 | 53.3 | 1 | |
| P-BAR | ||||||||
| Yes | 678 | 51.4 | 300 | 38.0 | 378 | 71.3 | 1 | |
| No | 641 | 48.6 | 489 | 62.0 | 152 | 28.7 | 4.05 (3.20–5.14) | <0.01 * |
| PHS | ||||||||
| Poor | 81 | 6.1 | 30 | 3.8 | 51 | 9.6 | 1 | |
| Fair | 361 | 27.3 | 217 | 27.3 | 144 | 27.2 | 2.56 (1.56–4.21) | <0.01 * |
| Good | 882 | 66.6 | 547 | 68.9 | 335 | 63.2 | 2.78 (1.73–4.45) | <0.01 * |
| Access to mass media (cue-to-action) | ||||||||
| No access | 42 | 3.2 | 21 | 2.7 | 21 | 4.0 | 1 | |
| Low access | 235 | 17.8 | 106 | 13.5 | 129 | 24.4 | 0.82 (0.43–1.59) | 0.56 |
| Moderate access | 478 | 36.3 | 281 | 35.7 | 197 | 37.2 | 1.43 (0.76–2.68) | 0.27 |
| High access | 562 | 42.7 | 380 | 48.2 | 182 | 34.4 | 2.09 (1.11–3.92) | 0.02 * |
| Model 1 | Model 2 | Model 3 | Model 4 | Model 5 | Model 6 | Model 7 | Model 8 | ||
|---|---|---|---|---|---|---|---|---|---|
| AOR | AOR | AOR | AOR | AOR | AOR | AOR | AOR | ||
| (95% CI) | (95% CI) | (95% CI) | (95% CI) | (95% CI) | (95% CI) | (95% CI) | (95% CI) | ||
| P-SUS | No | (1) | |||||||
| Yes | 2.07 * (1.64–2.62) | 1.97 * (1.56–2.50) | 2.20 * (1.70–2.83) | 1.47 * (1.11–1.94) | 1.49 * (1.13–1.98) | 1.68 * (1.23–2.30) | 1.63 * (1.19–2.23) | 1.54 * (1.11–2.13) | |
| P-SEV | No | (1) | |||||||
| Yes | 1.43 * (1.12–1.83) | 1.50 * (1.15–1.95) | 1.29 (0.97–1.70) | 1.27 (0.96–1.68) | 1.23 (0.90–1.66) | 1.26 (0.93–1.72) | 1.27 (0.92–1.74) | ||
| P-BAR | Yes | (1) | |||||||
| No | 4.31 * (3.37–5.51) | 3.66 * (2.83–4.75) | 3.698 * (2.85–4.78) | 3.35 * (2.53–4.43) | 3.43 * (2.58–4.56) | 3.53 * (2.63–4.74) | |||
| P-BEN | No | (1) | |||||||
| Yes | 3.99 * (3.02–5.26) | 3.90 * (2.95–5.16) | 3.93 * (2.88–5.34) | 3.82 * (2.80–5.21) | 3.67 * (2.66–5.06) | ||||
| PHS | Poor | (1) | |||||||
| Average | 2.82 * (1.57–5.05) | 2.88 * (1.48–5.59) | 2.95 * (1.50–5.81) | 3.05 * (1.51–6.13) | |||||
| Good | 2.80 *(1.61–4.87) | 2.41 *(1.27–4.54) | 2.53 *(1.32–4.84) | 2.66 *(1.36–5.19) | |||||
| Age (in years) | 40–49 | (1) | |||||||
| 50–59 | 1.12 (0.82–1.53) | 1.20 (0.88–1.65) | 1.37 (0.99–1.90) | ||||||
| 60–69 | 1.73 * (1.13–2.65) | 1.84 * (1.19–2.84) | 2.13 * (1.36–3.35) | ||||||
| 70–79 | 0.96 (0.44–2.08) | 1.01 (0.46–2.23) | 1.06 (0.45–2.48) | ||||||
| 80+ | 0.79 (0.23–2.75) | 0.91 (0.25–3.26) | 1.38 (0.37–5.05) | ||||||
| Sex | Male | (1) | |||||||
| Female | 0.53 * (0.38–0.72) | 0.53 * (0.38–0.73) | 0.61 * (0.43–0.85) | ||||||
| Region | Rural | (1) | |||||||
| Urban | 2.34 * (1.66–3.30) | 2.17 * (1.53–3.08) | 1.74 * (1.20–2.51) | ||||||
| Semi-urban | 0.61 (0.21–1.75) | 0.60 (0.21–1.73) | 0.45 (0.15–1.34) | ||||||
| Income (in PKR) | ≤20,000 | (1) | |||||||
| 20,001–50,000 | 1.12 (0.80–1.55) | 1.02 (0.73–1.43) | 0.86 (0.60–1.23) | ||||||
| 50,001–100,000 | 0.99 (0.65–1.52) | 0.81 (0.52–1.26) | 0.56 * (0.35–0.91) | ||||||
| >100,000 | 0.65 (0.38–1.12) | 0.50 * (0.28–0.89) | 0.34 * (0.18–0.62) | ||||||
| Access to mass media | No access | (1) | |||||||
| Low access | 0.57 (0.25–1.28) | 0.45 (0.19–1.01) | |||||||
| Moderate access | 1.13 (0.52–2.45) | 0.69 (0.31–1.53) | |||||||
| High access | 1.40 (0.64–3.07) | 0.71 (0.31–1.60) | |||||||
| Educational level | No formal education | (1) | |||||||
| Primary | 1.22 (0.67–2.23) | ||||||||
| Middle | 3.92 * (2.50–6.16) | ||||||||
| Secondary | 4.38 * (2.44–7.84) | ||||||||
| Higher | 4.53 * (2.60–7.90) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zakar, R.; Momina, A.u.; Shahzad, R.; Shahzad, S.; Hayee, M.; Zakar, M.Z.; Fischer, F. COVID-19 Vaccination Acceptance in the Context of the Health Belief Model: Comparative Cross-Sectional Study in Punjab, Pakistan. Int. J. Environ. Res. Public Health 2022, 19, 12892. https://doi.org/10.3390/ijerph191912892
Zakar R, Momina Au, Shahzad R, Shahzad S, Hayee M, Zakar MZ, Fischer F. COVID-19 Vaccination Acceptance in the Context of the Health Belief Model: Comparative Cross-Sectional Study in Punjab, Pakistan. International Journal of Environmental Research and Public Health. 2022; 19(19):12892. https://doi.org/10.3390/ijerph191912892
Chicago/Turabian StyleZakar, Rubeena, Ain ul Momina, Ruhma Shahzad, Sara Shahzad, Mahwish Hayee, Muhammad Zakria Zakar, and Florian Fischer. 2022. "COVID-19 Vaccination Acceptance in the Context of the Health Belief Model: Comparative Cross-Sectional Study in Punjab, Pakistan" International Journal of Environmental Research and Public Health 19, no. 19: 12892. https://doi.org/10.3390/ijerph191912892
APA StyleZakar, R., Momina, A. u., Shahzad, R., Shahzad, S., Hayee, M., Zakar, M. Z., & Fischer, F. (2022). COVID-19 Vaccination Acceptance in the Context of the Health Belief Model: Comparative Cross-Sectional Study in Punjab, Pakistan. International Journal of Environmental Research and Public Health, 19(19), 12892. https://doi.org/10.3390/ijerph191912892