
Confronting SARS-CoV-2 Infection: Patients’ Experience in the First Pandemic Wave—Cross-Sectional Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Assessment Variables
2.3. Statistical Methods
3. Results
4. Discussion
4.1. Main Findings
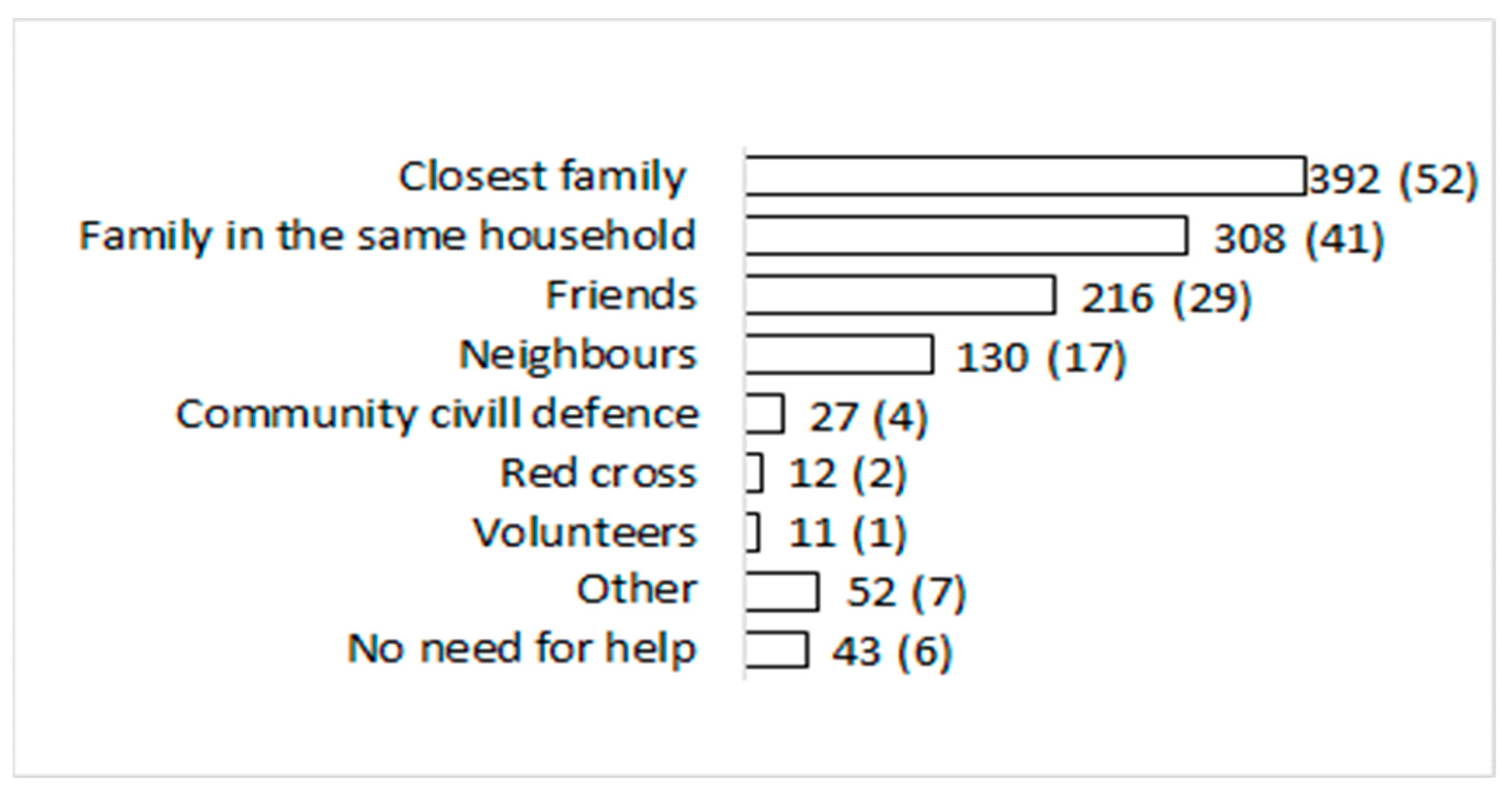
4.2. Social Support
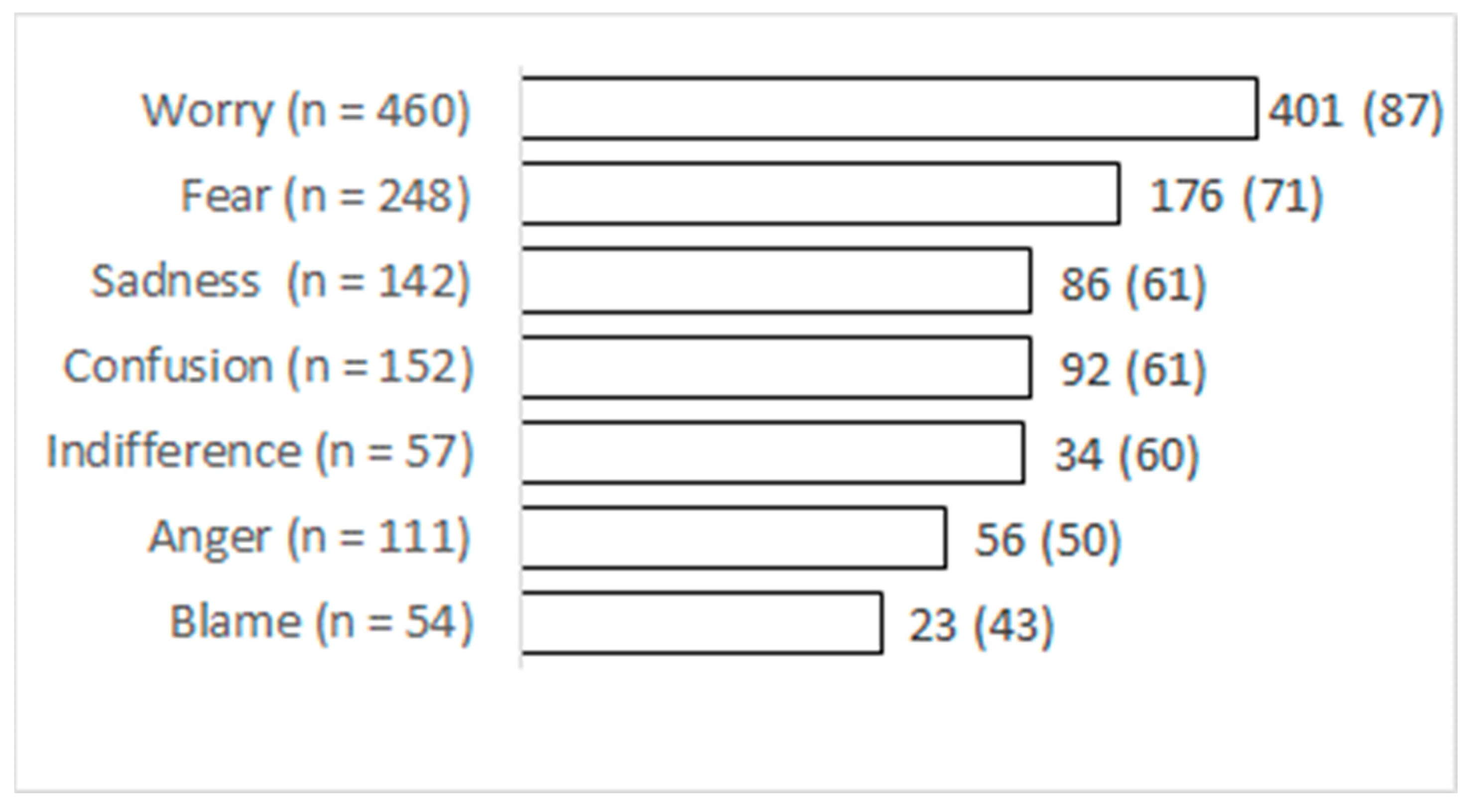
4.3. Feelings
4.4. Stigma
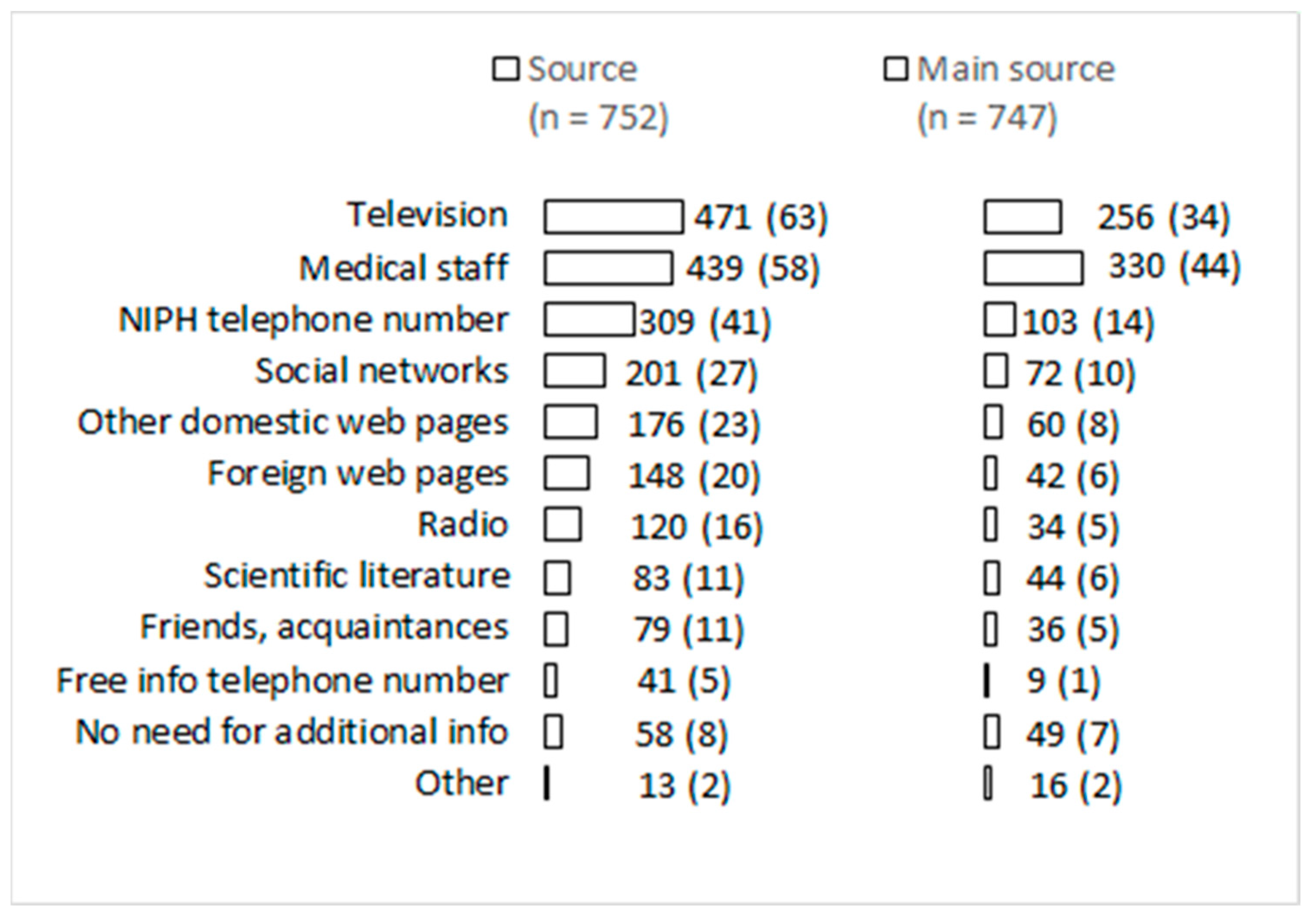
4.5. Information
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Holmes, E.C.; Goldstein, S.A.; Rasmussen, A.L.; Robertson, D.L.; Crits-Christoph, A.; Wertheim, J.O.; Anthony, S.J.; Barclay, W.S.; Boni, M.F.; Doherty, P.C.; et al. The origins of SARS-CoV-2: A critical review. Cell 2021, 184, 4848–4856. [Google Scholar] [CrossRef] [PubMed]
- WHO. Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19). Available online: https://www.who.int/docs/default-source/coronaviruse/who-china-joint-mission-on-covid-19-final-report.pdf (accessed on 15 September 2022).
- Perico, L.; Tomasoni, S.; Peracchi, T.; Perna, A.; Pezzotta, A.; Remuzzi, G.; Benigni, A. COVID-19 and lombardy: TESTing the impact of the first wave of the pandemic. EBioMedicine 2020, 61, 103069. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Chen, X.; Deng, X.; Chen, Z.; Gong, H.; Yan, H.; Wu, Q.; Shi, H.; Lai, S.; Ajelli, M.; et al. Disease burden and clinical severity of the first pandemic wave of COVID-19 in Wuhan; China. Nat. Commun. 2020, 11, 5411. [Google Scholar] [CrossRef] [PubMed]
- ECDC. Guidelines for the Implementation of Nonpharmaceutical Interventions against COVID-19. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/covid-19-guidelines-non-pharmaceutical-interventions-september-2020.pdf (accessed on 15 September 2022).
- Vatavali, F.; Gareiou, Z.; Kehagia, F.; Zervas, E. Impact of COVID-19 on Urban Everyday Life in Greece. Perceptions, Experiences and Practices of the Active Population. Sustainability 2020, 12, 9410. [Google Scholar] [CrossRef]
- Violant-Holz, V.; Gallego-Jiménez, M.G.; González-González, C.S.; Muñoz-Violant, S.; Rodríguez, M.J.; Sansano-Nadal, O.; Guerra-Balic, M. Psychological Health and Physical Activity Levels during the COVID-19 Pandemic: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 9419. [Google Scholar] [CrossRef]
- Panovska-Griffiths, J.; Szilassy, E.; Johnson, M.; Dixon, S.; De Simoni, A.; Wileman, V.; Dowrick, A.; Emsley, E.; Griffiths, C.; Barbosa, E.C.; et al. Impact of the first national COVID-19 lockdown on referral of women experiencing domestic violence and abuse in England and Wales. BMC Public Health 2022, 22, 504. [Google Scholar] [CrossRef]
- Lee, J.O.; Kapteyn, A.; Clomax, A.; Jin, H. Estimating influences of unemployment and underemployment on mental health during the COVID-19 pandemic: Who suffers the most? Public Health 2021, 201, 48–54. [Google Scholar] [CrossRef]
- Profeta, A.; Siddiqui, S.A.; Smetana, S.; Hossaini, S.M.; Heinz, V.; Kircher, C. The impact of Corona pandemic on consumer’s food consumption: Vulnerability of households with children and income losses and change in sustainable consumption behavior. J. Verbrauch. Lebensm. 2021, 16, 305–314. [Google Scholar] [CrossRef]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Horesh, D.; Kapel Lev-Ari, R.; Hasson-Ohayon, I. Risk factors for psychological distress during the COVID-19 pandemic in Israel: Loneliness; age; gender; and health status play an important role. Br. J. Health Psychol. 2020, 25, 925–933. [Google Scholar] [CrossRef]
- Oliveira, M.R.; Sudati, I.P.; Konzen, V.M.; de Campos, A.C.; Wibelinger, L.M.; Correa, C.; Miguel, F.M.; Silva, R.N.; Borghi-Silva, A. Covid-19 and the impact on the physical activity level of elderly people: A systematic review. Exp. Gerontol. 2022, 159, 111675. [Google Scholar] [CrossRef] [PubMed]
- Robinson, E.; Boyland, E.; Chisholm, A.; Harrold, J.; Maloney, N.G.; Marty, L.; Mead, B.R.; Noonan, R.; Hardman, C.A. Obesity; eating behavior and physical activity during COVID-19 lockdown: A study of UK adults. Appetite 2021, 156, 104853. [Google Scholar] [CrossRef] [PubMed]
- Rubio-Tomás, T.; Skouroliakou, M.; Ntountaniotis, D. Lockdown Due to COVID-19 and Its Consequences on Diet; Physical Activity; Lifestyle; and Other Aspects of Daily Life Worldwide: A Narrative Review. Int. J. Environ. Res. Public Health 2022, 19, 6832. [Google Scholar] [CrossRef] [PubMed]
- Tuczyńska, M.; Matthews-Kozanecka, M.; Baum, E. Accessibility to Non-COVID Health Services in the World During the COVID-19 Pandemic: Review. Front. Public Health 2021, 9, 760795. [Google Scholar] [CrossRef] [PubMed]
- Xiong, J.; Lipsitz, O.; Nasri, F.; Lui, L.M.W.; Gill, H.; Phan, L.; Chen-Li, D.; Iacobucci, M.; Ho, R.; Majeed, A.; et al. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. J. Affect. Disord. 2020, 277, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Szkody, E.; Stearns, M.; Stanhope, L.; McKinney, C. Stress-Buffering Role of Social Support during COVID-19. Fam. Process. 2021, 60, 1002–1015. [Google Scholar] [CrossRef]
- Erčulj, V.I.; Žiberna, A. The Role of Online Social Support in Patients Undergoing Infertility Treatment—A Comparison of Pregnant and Non-pregnant Members. Health Commun. 2021, 36, 1–7. [Google Scholar] [CrossRef]
- Bowen, J.; Bulbena, A.; Fatjó, J. The Value of Companion Dogs as a Source of Social Support for Their Owners: Findings From a Pre-pandemic Representative Sample and a Convenience Sample Obtained During the COVID-19 Lockdown in Spain. Front. Psychiatry 2021, 12, 622060. [Google Scholar] [CrossRef]
- Orso, D.; Federici, N.; Copetti, R.; Vetrugno, L.; Bove, T. Infodemic and the spread of fake news in the COVID-19-era. Eur. J. Emerg. Med. 2020, 27, 327–328. [Google Scholar] [CrossRef]
- Tomaino, S.C.M.; Cipolletta, S.; Kostova, Z.; Todorova, I. Stories of Life during the First Wave of the COVID-19 Pandemic in Italy: A Qualitative Study. Int. J. Environ. Res. Public Health 2021, 18, 7630. [Google Scholar] [CrossRef]
- Wasim, A.; Truong, J.; Bakshi, S.; Majid, U. A systematic review of fear; stigma; and mental health outcomes of pandemics. J. Ment. Health 2022, 31, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Nasserie, T.; Hittle, M.; Goodman, S.N. Assessment of the Frequency and Variety of Persistent Symptoms Among Patients With COVID-19: A Systematic Review. JAMA Netw. Open 2021, 4, e2111417. [Google Scholar] [CrossRef] [PubMed]
- Sehgal, A.R.; Himmelstein, D.U.; Woolhandler, S. Feasibility of Separate Rooms for Home Isolation and Quarantine for COVID-19 in the United States. Ann. Intern. Med. 2021, 174, 127–129. [Google Scholar] [CrossRef]
- Smith, L.E.; Amlȏt, R.; Lambert, H.; Oliver, I.; Robin, C.; Yardley, L.; Rubin, G.J. Factors associated with adherence to self-isolation and lockdown measures in the UK: A cross-sectional survey. Public Health 2020, 187, 41–52. [Google Scholar] [CrossRef] [PubMed]
- Metin, A.; Erbiçer, E.S.; Şen, S.; Çetinkaya, A. Gender and COVID-19 related fear and anxiety: A meta-analysis. J. Affect. Disord. 2022, 310, 384–395. [Google Scholar] [CrossRef] [PubMed]
- Vindegaard, N.; Benros, M.E. COVID-19 pandemic and mental health consequences: Systematic review of the current evidence. Brain. Behav. Immun. 2020, 89, 531–542. [Google Scholar] [CrossRef]
- Zhang, H.; Xie, F.; Yang, B.; Zhao, F.; Wang, C.; Chen, X. Psychological experience of COVID-19 patients: A systematic review and qualitative meta-synthesis. Am. J. Infect. Control 2022, 50, 809–819. [Google Scholar] [CrossRef] [PubMed]
- Shaban, R.Z.; Nahidi, S.; Sotomayor-Castillo, C.; Li, C.; Gilroy, N.; O’Sullivan, M.V.N.; Sorrell, T.C.; White, E.; Hackett, K.; Bag, S. SARS-CoV-2 infection and COVID-19: The lived experience and perceptions of patients in isolation and care in an Australian healthcare setting. Am. J. Infect. Control 2020, 48, 1445–1450. [Google Scholar] [CrossRef]
- Rewerska-Juśko, M.; Rejdak, K. Social Stigma of Patients Suffering from COVID-19: Challenges for Health Care System. Healthcare 2022, 10, 292. [Google Scholar] [CrossRef] [PubMed]
- Yuan, K.; Huang, X.L.; Yan, W.; Zhang, Y.X.; Gong, Y.M.; Su, S.Z.; Huang, Y.T.; Zhong, Y.; Wang, Y.J.; Yuan, Z.; et al. A systematic review and meta-analysis on the prevalence of stigma in infectious diseases; including COVID-19: A call to action. Mol. Psychiatry 2022, 27, 19–33. [Google Scholar] [CrossRef]
- Radhakrishnan, R.V.; Jain, M.; Mohanty, C.R.; Jacob, J.; Shetty, A.P.; Stephen, S.; Vijay, V.R.; Issac, A. The perceived social stigma; self-esteem; and its determinants among the health care professionals working in India during COVID 19 pandemic. Med. J. Armed Forces India 2021, 77 (Suppl. 2), S450–S458. [Google Scholar] [CrossRef]
- Bhatnagar, S.; Kumar, S.; Rathore, P.; Sarma, R.; Malhotra, R.K.; Choudhary, N.; Thankachan, A.; Haokip, N.; Singh, S.; Pandit, A.; et al. Surviving COVID-19 is Half the Battle; Living Life with Perceived Stigma is Other Half: A Cross-Sectional Study. Indian J. Psychol. Med. 2021, 43, 428–435. [Google Scholar] [CrossRef] [PubMed]
- Lin, B.; Zhong, G.; Liang, Z.; Huang, J.; Wang, X.; Lin, Y. Perceived-stigma level of COVID-19 patients in China in the early stage of the epidemic: A cross-sectional research. PLoS ONE 2021, 16, e0258042. [Google Scholar] [CrossRef] [PubMed]
- Haddad, C.; Bou, M.S.; Malaeb, D.; Sacre, H.; Saadeh, D.; Mourtada, V.; Salameh, P. Stigma toward people with COVID-19 among the Lebanese population: A cross-sectional study of correlates and mediating effects. BMC Psychol. 2021, 9, 164. [Google Scholar] [CrossRef] [PubMed]
- CIFRC; UNICEF. WHO Social Stigma Associated with COVID-19: A Guide to Preventing and Addressing Social Stigma. Available online: https://www.who.int/docs/default-source/coronaviruse/covid19-stigmaguide.pdf?sfvrsn=226180f4_29 (accessed on 15 September 2022).
- Ali, S.H.; Foreman, J.; Tozan, Y.; Capasso, A.; Jones, A.M.; DiClemente, R.J. Trends and Predictors of COVID-19 Information Sources and Their Relationship With Knowledge and Beliefs Related to the Pandemic: Nationwide Cross-Sectional Study. JMIR Public Health Surveill. 2020, 6, e21071. [Google Scholar] [CrossRef] [PubMed]
- Shen, Z.; Zhong, Z.; Xie, J.; Zhang, Q.; Li, S. The Effects of Information-Seeking Behaviors on Risk Perception During the COVID-19 Pandemic: A Cross-Sectional Correlational Survey. Psychol. Res. Behav. Manag. 2022, 15, 1707–1719. [Google Scholar] [CrossRef] [PubMed]
- Focosi, D.; Navarro, D.; Maggi, F.; Roilides, E.; Antonelli, G. COVID-19 infodemics: The role of mainstream and social media. Clin. Microbiol. Infect. 2021, 27, 1568–1569. [Google Scholar] [CrossRef] [PubMed]
- Anwar, A.; Malik, M.; Raees, V.; Anwar, A. Role of Mass Media and Public Health Communications in the COVID-19 Pandemic. Cureus 2020, 12, e10453. [Google Scholar] [CrossRef]
- Trnka, R.; Lorencova, R. Fear; anger; and media-induced trauma during the outbreak of COVID-19 in the Czech Republic. Psychol. Trauma 2020, 12, 546–549. [Google Scholar] [CrossRef] [PubMed]
- Melki, J.; Tamim, H.; Hadid, D.; Makki, M.; El Amine, J.; Hitti, E. Mitigating infodemics: The relationship between news exposure and trust and belief in COVID-19 fake news and social media spreading. PLoS ONE 2021, 16, e0252830. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Patients’ Data | No. (%) |
|---|---|
| Gender | |
| Female | 418 (55.5) |
| Male | 335 (44.5) |
| Median (IQR) age (n = 727) | 49 (33–59) |
| Education | |
| Elementary | 89 (11.9) |
| Secondary | 327 (43.8) |
| University | 331 (44.3) |
| Concomitant disease (n = 767) | 381 (49.7) |
| Course of SARS-CoV-2 Infection | No. (%) |
|---|---|
| Need for medical advice (n = 756) | 503 (66.5) |
| Hospitalization (n = 767) | 177 (23.1) |
| Median (IQR) duration of hospitalization (n = 175) | 9 (5–16) |
| Symptoms on the 15th day (n = 760) | 484 (63.7) |
| Everyday activities on the 15th day, the same as pre-COVID-19 (n = 746) | 325 (43.6) |
| Support | No. (%) |
|---|---|
| Support from family members and friends | |
| No | 4 (0.5) |
| Partly | 27 (3.6) |
| Yes | 716 (95.9) |
| Support from acquaintances and co-workers | |
| No | 54 (7.4) |
| Partly | 106 (14.5) |
| Yes | 572 (78.1) |
| Support from medical staff | |
| No | 47 (6.4) |
| Partly | 70 (9.6) |
| Yes | 615 (84) |
| Feelings and Stigmatization | No. (%) |
|---|---|
| Feelings at diagnosis (n = 681) | |
| Sadness | 145 (21.3) |
| Fear | 256 (37.6) |
| Worry | 479 (70.3) |
| Indifference | 58 (8.5) |
| Anger | 114 (16.7) |
| Blame | 57 (8.4) |
| Confusion | 165 (24.2) |
| Feelings during illness (n = 655) | |
| Sadness | 120 (18.3) |
| Fear | 215 (32.8) |
| Worry | 452 (69) |
| Indifference | 65 (9.9) |
| Anger | 83 (12.7) |
| Blame | 37 (5.6) |
| Confusion | 121 (18.5) |
| Stigmatization | |
| No | 391 (52.6) |
| Partly | 186 (25) |
| Yes | 167 (22.4) |
| Worry | Fear | Sadness | ||||
|---|---|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | |
| Male gender | 0.65 (0.44–0.95) | 0.024 | 0.47 (0.32–0.69) | <0.001 | 0.74 (0.48–1.16) | 0.188 |
| Age | 1.04 (1.03–1.05) | <0.001 | 1.02 (1.01–1.03) | <0.001 | 1.01 (1–1.02) | 0.204 |
| Having pet | 1.09 (0.75–1.58) | 0.669 | 0.81 (0.57–1.17) | 0.264 | 0.81 (0.53–1.25) | 0.349 |
| SSS * | 0.93 (0.51–1.69) | 0.819 | 0.6 (0.34–1.04) | 0.067 | 0.48 (0.27–0.88) | 0.017 |
| No isolation | 0.92 (0.63–1.35) | 0.676 | 0.87 (0.6–1.25) | 0.446 | 0.59 (0.37–0.93) | 0.022 |
| NIS ** | 1.26 (1.12–1.43) | <0.001 | 1.05 (0.94–1.17) | 0.401 | 1.03 (0.9–1.17) | 0.693 |
| NCS # | 1.12 (0.82–1.52) | 0.472 | 1.65 (1.22–2.21) | 0.001 | 1.24 (0.88–1.76) | 0.217 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Socan, M.; Erčulj, V.I. Confronting SARS-CoV-2 Infection: Patients’ Experience in the First Pandemic Wave—Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 12743. https://doi.org/10.3390/ijerph191912743
Socan M, Erčulj VI. Confronting SARS-CoV-2 Infection: Patients’ Experience in the First Pandemic Wave—Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2022; 19(19):12743. https://doi.org/10.3390/ijerph191912743
Chicago/Turabian StyleSocan, Maja, and Vanja Ida Erčulj. 2022. "Confronting SARS-CoV-2 Infection: Patients’ Experience in the First Pandemic Wave—Cross-Sectional Study" International Journal of Environmental Research and Public Health 19, no. 19: 12743. https://doi.org/10.3390/ijerph191912743