
Is Obesity a Risk Factor for Periodontal Disease in Adults? A Systematic Review



Abstract
:1. Introduction
2. Materials and Methods
- Is periodontitis measured by CAL more prevalent and severe in patients with a BMI of more than 30?
- Does BMI more than 30 affect tooth loss due to periodontitis and bleeding on probing?
2.1. Protocol and Registration
2.2. Eligibility Criteria
2.3. Information Sources and Search Strategies
2.4. Studies Selection
2.5. Data Extraction and Data Items
2.6. Diagnosis of Obesity
2.7. Diagnosis of Periodontitis
2.8. Risk of Bias in Individual Studies
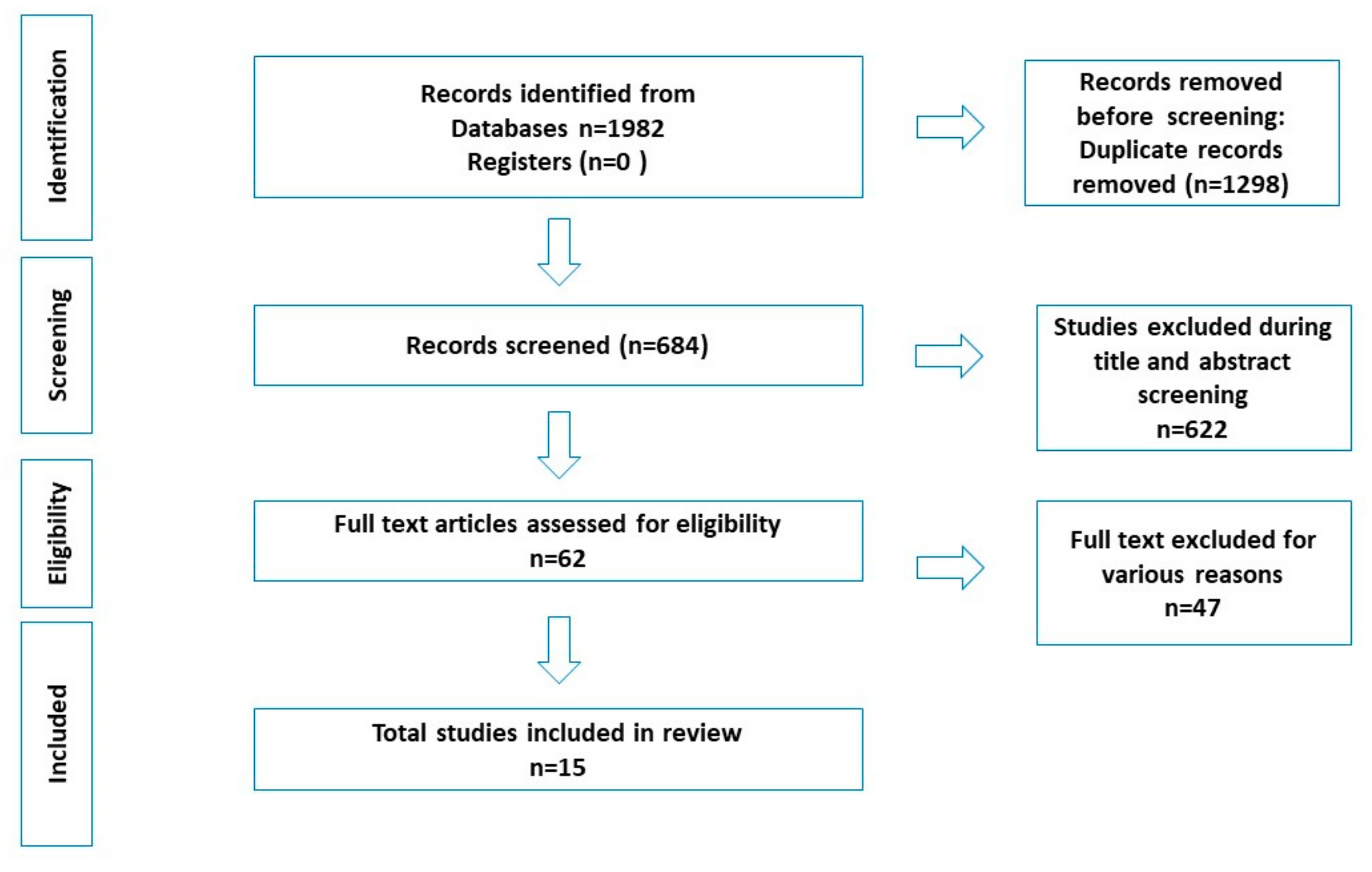
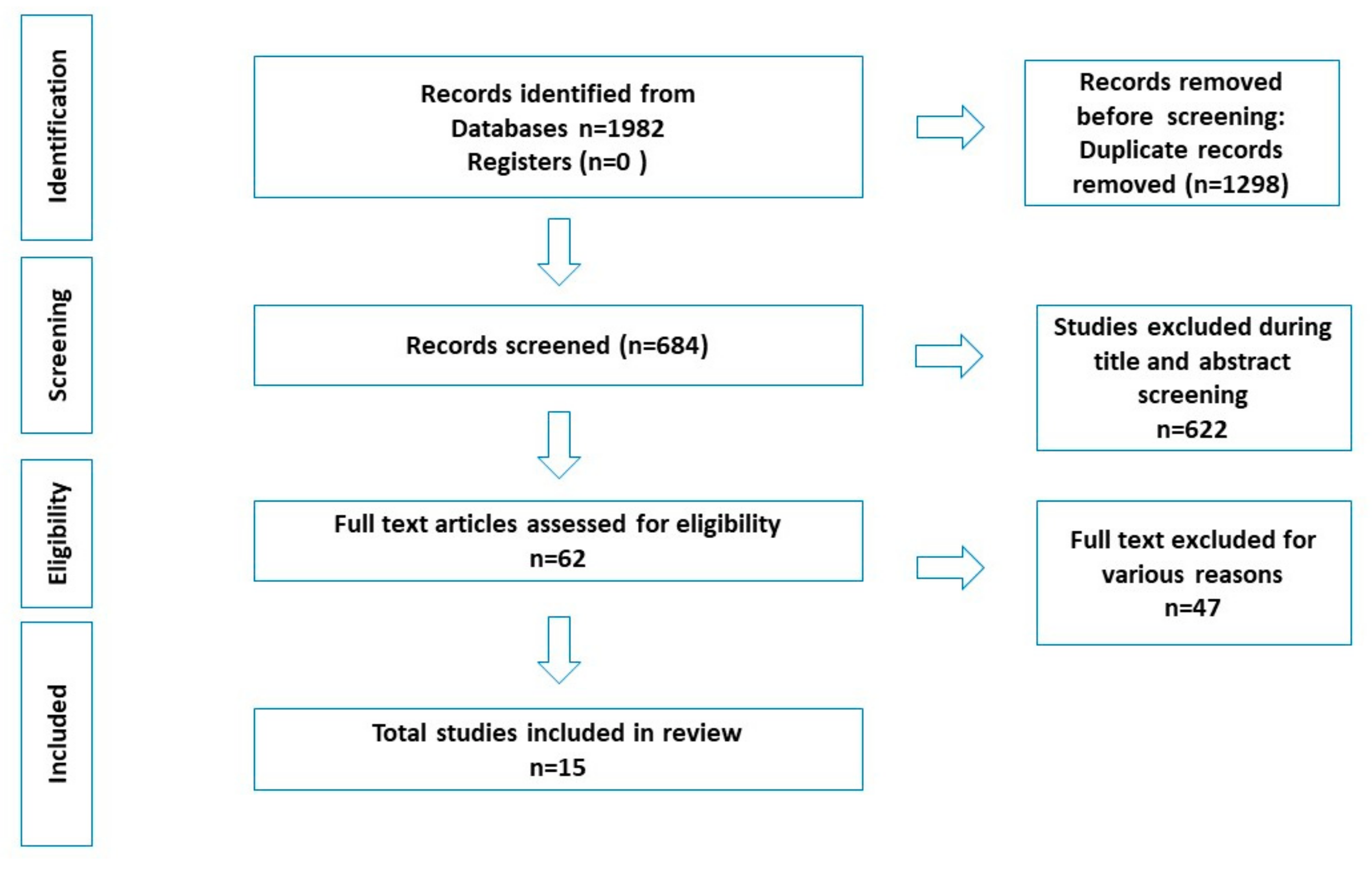
3. Results
3.1. Human Studies
3.2. Animal Studies and Systematic Review
3.3. Risk of Bias across Studies
4. Discussion
4.1. Mechanism Linking Obesity and Periodontal Disease
4.2. Association between Obesity and Periodontal Disease-Human Observational Studies
4.3. Evidence from Animal Studies
4.4. Evidence from Systematic Review
4.5. Implications for Clinical Practice
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, G.A.; Kim, K.K.; Wilding, J.P.H.; World Obesity Federation. Obesity: A chronic relapsing progressive disease process. A position statement of the World Obesity Federation. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2017, 18, 715–723. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hruby, A.; Hu, F.B. The Epidemiology of Obesity: A Big Picture. PharmacoEconomics 2015, 33, 673–689. [Google Scholar] [CrossRef] [PubMed]
- Field, A.E.; Coakley, E.H.; Must, A.; Spadano, J.L.; Laird, N.; Dietz, W.H.; Rimm, E.; Colditz, G.A. Impact of overweight on the risk of developing common chronic diseases during a 10-year period. Arch. Intern. Med. 2001, 161, 1581–1586. [Google Scholar] [CrossRef] [PubMed]
- Piche, M.E.; Tchernof, A.; Despres, J.P. Obesity Phenotypes, Diabetes, and Cardiovascular Diseases. Circ. Res. 2020, 126, 1477–1500. [Google Scholar] [CrossRef]
- Chaffee, B.W.; Weston, S.J. Association between chronic periodontal disease and obesity: A systematic review and meta-analysis. J. Periodontol. 2010, 81, 1708–1724. [Google Scholar] [CrossRef]
- Kononen, E.; Gursoy, M.; Gursoy, U.K. Periodontitis: A Multifaceted Disease of Tooth-Supporting Tissues. J. Clin. Med. 2019, 8, 1135. [Google Scholar] [CrossRef] [Green Version]
- Al-Zahrani, M.S.; Bissada, N.F.; Borawskit, E.A. Obesity and periodontal disease in young, middle-aged, and older adults. J. Periodontol. 2003, 74, 610–615. [Google Scholar] [CrossRef]
- Hegde, S.; Chatterjee, E.; Rajesh, K.S.; Kumar, M.S.A. Obesity and its association with chronic periodontitis: A cross-sectional study. J. Educ. Health Promot. 2019, 8, 222. [Google Scholar] [CrossRef]
- Martinez-Herrera, M.; Silvestre-Rangil, J.; Silvestre, F.J. Association between obesity and periodontal disease. A systematic review of epidemiological studies and controlled clinical trials. Med. Oral. Patol. Oral. Y Cir. Bucal. 2017, 22, e708–e715. [Google Scholar] [CrossRef]
- Suvan, J.; D’Aiuto, F.; Moles, D.R.; Petrie, A.; Donos, N. Association between overweight/obesity and periodontitis in adults. A systematic review. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2011, 12, e381–e404. [Google Scholar] [CrossRef]
- Genco, R.J.; Grossi, S.G.; Ho, A.; Nishimura, F.; Murayama, Y. A proposed model linking inflammation to obesity, diabetes, and periodontal infections. J. Periodontol. 2005, 76, 2075–2084. [Google Scholar] [CrossRef] [PubMed]
- Van Dyke, T.E. Pro-resolving mediators in the regulation of periodontal disease. Mol. Asp. Med. 2017, 58, 21–36. [Google Scholar] [CrossRef] [PubMed]
- Suvan, J.E.; Finer, N.; D’Aiuto, F. Periodontal complications with obesity. Periodontol. 2000 2018, 78, 98–128. [Google Scholar] [CrossRef] [PubMed]
- Jepsen, S.; Suvan, J.; Deschner, J. The association of periodontal diseases with metabolic syndrome and obesity. Periodontol. 2000 2020, 83, 125–153. [Google Scholar] [CrossRef] [PubMed]
- Wellen, K.E.; Hotamisligil, G.S. Obesity-induced inflammatory changes in adipose tissue. J. Clin. Investig. 2003, 112, 1785–1788. [Google Scholar] [CrossRef]
- Aronne, L.J.; Segal, K.R. Adiposity and fat distribution outcome measures: Assessment and clinical implications. Obes. Res. 2002, 10 (Suppl. 1), 14S–21S. [Google Scholar] [CrossRef]
- Ellulu, M.S.; Patimah, I.; Khaza’ai, H.; Rahmat, A.; Abed, Y. Obesity and inflammation: The linking mechanism and the complications. Arch. Med. Sci. AMS 2017, 13, 851–863. [Google Scholar] [CrossRef]
- Bistrian, B. Systemic response to inflammation. Nutr. Rev. 2007, 65, S170–S172. [Google Scholar] [CrossRef]
- Coelho, M.; Oliveira, T.; Fernandes, R. Biochemistry of adipose tissue: An endocrine organ. Arch. Med. Sci. AMS 2013, 9, 191–200. [Google Scholar] [CrossRef] [Green Version]
- Trayhurn, P.; Wood, I.S. Adipokines: Inflammation and the pleiotropic role of white adipose tissue. Br. J. Nutr. 2004, 92, 347–355. [Google Scholar] [CrossRef]
- Kwon, H.; Pessin, J.E. Adipokines mediate inflammation and insulin resistance. Front. Endocrinol. 2013, 4, 71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ritchie, C.S. Obesity and periodontal disease. Periodontol. 2000 2007, 44, 154–163. [Google Scholar] [CrossRef] [PubMed]
- Opatrilova, R.; Caprnda, M.; Kubatka, P.; Valentova, V.; Uramova, S.; Nosal, V.; Gaspar, L.; Zachar, L.; Mozos, I.; Petrovic, D.; et al. Adipokines in neurovascular diseases. Biomed. Pharmacother. Biomed. Pharmacother. 2018, 98, 424–432. [Google Scholar] [CrossRef] [PubMed]
- Nuttall, F.Q. Body Mass Index: Obesity, BMI, and Health: A Critical Review. Nutr. Today 2015, 50, 117–128. [Google Scholar] [CrossRef] [Green Version]
- Barlow, S.E.; Dietz, W.H. Obesity evaluation and treatment: Expert Committee recommendations. The Maternal and Child Health Bureau, Health Resources and Services Administration and the Department of Health and Human Services. Pediatrics 1998, 102, E29. [Google Scholar] [CrossRef] [Green Version]
- Ferrillo, M.; Migliario, M.; Roccuzzo, A.; Molinero-Mourelle, P.; Falcicchio, G.; Umano, G.R.; Pezzotti, F.; Bonda, P.L.F.; Calafiore, D.; de Sire, A. Periodontal Disease and Vitamin D Deficiency in Pregnant Women: Which Correlation with Preterm and Low-Weight Birth? J. Clin. Med. 2021, 10, 4578. [Google Scholar] [CrossRef]
- Sanz, M.; Del Castillo, A.M.; Jepsen, S.; Gonzalez-Juanatey, J.R.; D’Aiuto, F.; Bouchard, P.; Chapple, I.; Dietrich, T.; Gotsman, I.; Graziani, F.; et al. Periodontitis and cardiovascular diseases: Consensus report. J. Clin. Periodontol. 2020, 47, 268–288. [Google Scholar] [CrossRef]
- Nwizu, N.; Wactawski-Wende, J.; Genco, R.J. Periodontal disease and cancer: Epidemiologic studies and possible mechanisms. Periodontol. 2000 2020, 83, 213–233. [Google Scholar] [CrossRef]
- De Sire, A.; Invernizzi, M.; Ferrillo, M.; Gimigliano, F.; Baricich, A.; Cisari, C.; De Marchi, F.; Bonda, P.L.F.; Mazzini, L.; Migliario, M. Functional status and Oral health in patients with amyotrophic lateral sclerosis: A cross-sectional study. NeuroRehabilitation 2021, 48, 49–57. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Dubey, V.P.; Kievisiene, J.; Rauckiene-Michealsson, A.; Norkiene, S.; Razbadauskas, A.; Agostinis-Sobrinho, C. Bullying and Health Related Quality of Life among Adolescents-A Systematic Review. Children 2022, 9, 766. [Google Scholar] [CrossRef] [PubMed]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Carneiro, D.O.; Gomes-Filho, I.S.; da Cruz, S.S.; Trindade, S.C.; Santos, K.O.B.; Sarmento, V.A.; Freitas, T.O.B.; Dos Santos, H.L.R.; Hintz, A.M.; Santos, P.N.P.; et al. Obesity in young women is positively associated with periodontitis. Clin. Oral. Investig. 2022. [Google Scholar] [CrossRef]
- Vecchia, C.F.D.; Susin, C.; Rosing, C.K.; Oppermann, R.V.; Albandar, J.M. Overweight and obesity as risk indicators for periodontitis in adults. J. Periodontol. 2005, 76, 1721–1728. [Google Scholar] [CrossRef]
- Khader, Y.S.; Bawadi, H.A.; Haroun, T.F.; Alomari, M.; Tayyem, R.F. The association between periodontal disease and obesity among adults in Jordan. J. Clin. Periodontol. 2009, 36, 18–24. [Google Scholar] [CrossRef]
- Hel, S.A. Relationship between overall and abdominal obesity and periodontal disease among young adults. East. Mediterr. Health J. 2010, 16, 429–433. [Google Scholar]
- Deshpande, N.C.; Amrutiya, M.R. Obesity and oral health—Is there a link? An observational study. J. Indian Soc. Periodontol. 2017, 21, 229–233. [Google Scholar] [CrossRef]
- Gulati, N.N.; Masamatti, S.S.; Chopra, P. Association between obesity and its determinants with chronic periodontitis: A cross-sectional study. J. Indian Soc. Periodontol. 2020, 24, 167–172. [Google Scholar] [CrossRef]
- Santos, T.; Cury, P.R.; Santos, E.; Vasconcelos, R.; Santos, J.N.D.; Ramalho, L.M.P. Association Between Severe Periodontitis and Obesity Degree: A Preliminary Study. Oral. Health Prev. Dent. 2019, 17, 173–177. [Google Scholar] [CrossRef]
- Maulani, C.; Auerkari, E.I.; Masulili, S.L.C.; Kusdhany, L.S.; Prahasanti, C.; Soedarsono, N. Obesity correlated to a higher risk of acquiring periodontitis: A cross-sectional study. F1000 Res. 2021, 10, 643. [Google Scholar] [CrossRef]
- Pataro, A.L.; Costa, F.O.; Cortelli, S.C.; Cortelli, J.R.; Abreu, M.H.; Costa, J.E. Association between severity of body mass index and periodontal condition in women. Clin. Oral. Investig. 2012, 16, 727–734. [Google Scholar] [CrossRef] [PubMed]
- Sarlati, F.; Akhondi, N.; Ettehad, T.; Neyestani, T.; Kamali, Z. Relationship between obesity and periodontal status in a sample of young Iranian adults. Int. Dent. J. 2008, 58, 36–40. [Google Scholar] [PubMed]
- Buduneli, N.; Biyikoglu, B.; Ilgenli, T.; Buduneli, E.; Nalbantsoy, A.; Sarac, F.; Kinane, D.F. Is obesity a possible modifier of periodontal disease as a chronic inflammatory process? A case-control study. J. Periodontal Res. 2014, 49, 465–471. [Google Scholar] [CrossRef] [PubMed]
- Gaio, E.J.; Haas, A.N.; Rosing, C.K.; Oppermann, R.V.; Albandar, J.M.; Susin, C. Effect of obesity on periodontal attachment loss progression: A 5-year population-based prospective study. J. Clin. Periodontol. 2016, 43, 557–565. [Google Scholar] [CrossRef]
- Linden, G.; Patterson, C.; Evans, A.; Kee, F. Obesity and periodontitis in 60-70-year-old men. J. Clin. Periodontol. 2007, 34, 461–466. [Google Scholar] [CrossRef]
- Nascimento, G.G.; Peres, K.G.; Mittinty, M.N.; Mejia, G.C.; Silva, D.A.; Gonzalez-Chica, D.; Peres, M.A. Obesity and Periodontal Outcomes: A Population-Based Cohort Study in Brazil. J. Periodontol. 2017, 88, 50–58. [Google Scholar] [CrossRef]
- Cetin, M.B.; Sezgin, Y.; Onder, C.; Bakirarar, B. The relationship between body mass index and stage/grade of periodontitis: A retrospective study. Clin. Oral. Investig. 2022, 26, 1937–1945. [Google Scholar] [CrossRef]
- Caton, J.G.; Armitage, G.; Berglundh, T.; Chapple, I.L.C.; Jepsen, S.; Kornman, K.S.; Mealey, B.L.; Papapanou, P.N.; Sanz, M.; Tonetti, M.S. A new classification scheme for periodontal and peri-implant diseases and conditions—Introduction and key changes from the 1999 classification. J. Clin. Periodontol. 2018, 45 (Suppl. 20), S1–S8. [Google Scholar] [CrossRef]
- Amar, S.; Zhou, Q.; Shaik-Dasthagirisaheb, Y.; Leeman, S. Diet-induced obesity in mice causes changes in immune responses and bone loss manifested by bacterial challenge. Proc. Natl. Acad. Sci. USA 2007, 104, 20466–20471. [Google Scholar] [CrossRef] [Green Version]
- Cavagni, J.; de Macedo, I.C.; Gaio, E.J.; Souza, A.; de Molon, R.S.; Cirelli, J.A.; Hoefel, A.L.; Kucharski, L.C.; Torres, I.L.; Rosing, C.K. Obesity and Hyperlipidemia Modulate Alveolar Bone Loss in Wistar Rats. J. Periodontol. 2016, 87, e9–e17. [Google Scholar] [CrossRef] [PubMed]
- Cavagni, J.; Wagner, T.P.; Gaio, E.J.; Rego, R.O.; Torres, I.L.; Rosing, C.K. Obesity may increase the occurrence of spontaneous periodontal disease in Wistar rats. Arch. Oral. Biol. 2013, 58, 1034–1039. [Google Scholar] [CrossRef] [PubMed]
- Muluke, M.; Gold, T.; Kiefhaber, K.; Al-Sahli, A.; Celenti, R.; Jiang, H.; Cremers, S.; Van Dyke, T.; Schulze-Spate, U. Diet-Induced Obesity and Its Differential Impact on Periodontal Bone Loss. J. Dent. Res. 2016, 95, 223–229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zuza, E.P.; Garcia, V.G.; Theodoro, L.H.; Ervolino, E.; Favero, L.F.V.; Longo, M.; Ribeiro, F.S.; Martins, A.T.; Spolidorio, L.C.; Zuanon, J.A.S.; et al. Influence of obesity on experimental periodontitis in rats: Histopathological, histometric and immunohistochemical study. Clin. Oral. Investig. 2018, 22, 1197–1208. [Google Scholar] [CrossRef] [PubMed]
- Damanaki, A.; Memmert, S.; Nokhbehsaim, M.; Sanyal, A.; Gnad, T.; Pfeifer, A.; Deschner, J. Impact of obesity and aging on crestal alveolar bone height in mice. Ann. Anat. Anat. Anz. Off. Organ Anat. Ges. 2018, 218, 227–235. [Google Scholar] [CrossRef] [PubMed]
- Damanaki, A.; Memmert, S.; Nokhbehsaim, M.; Abedi, A.; Rath-Deschner, B.; Nogueira, A.; Deschner, J. Effects of Obesity on Bone Healing in Rats. Int. J. Mol. Sci. 2021, 22, 13339. [Google Scholar] [CrossRef]
- Simch, R.P.; Gaio, E.J.; Rosing, C.K. Effect of body weight in the pathogenesis of ligature-induced periodontal disease in Wistar rats. Acta Odontol. Scand. 2008, 66, 130–134. [Google Scholar] [CrossRef]
- Verzeletti, G.N.; Gaio, E.J.; Linhares, D.S.; Rosing, C.K. Effect of obesity on alveolar bone loss in experimental periodontitis in Wistar rats. J. Appl. Oral. Sci. Rev. FOB 2012, 20, 218–221. [Google Scholar] [CrossRef]
- Tomofuji, T.; Yamamoto, T.; Tamaki, N.; Ekuni, D.; Azuma, T.; Sanbe, T.; Irie, K.; Kasuyama, K.; Umakoshi, M.; Murakami, J.; et al. Effects of obesity on gingival oxidative stress in a rat model. J. Periodontol. 2009, 80, 1324–1329. [Google Scholar] [CrossRef]
- Lopes, M.E.S.; Marcantonio, C.C.; de Molon, R.S.; Cerri, P.S.; Salmon, C.R.; Mofatto, L.S.; Nociti Junior, F.H.; Deschner, J.; Cirelli, J.A.; Nogueira, A.V.B. Obesity influences the proteome of periodontal ligament tissues following periodontitis induction in rats. J. Periodontal Res. 2022, 57, 545–557. [Google Scholar] [CrossRef]
- Brandelero, S., Jr.; Bonfleur, M.L.; Ribeiro, R.A.; Vanzela, E.C.; Nassar, C.A.; Nassar, P.O.; Balbo, S.L. Decreased TNF-alpha gene expression in periodontal ligature in MSG-obese rats: A possible protective effect of hypothalamic obesity against periodontal disease? Arch. Oral. Biol. 2012, 57, 300–306. [Google Scholar] [CrossRef] [PubMed]
- Moura-Grec, P.G.; Marsicano, J.A.; Carvalho, C.A.; Sales-Peres, S.H. Obesity and periodontitis: Systematic review and meta-analysis. Cienc. Saude Coletiva 2014, 19, 1763–1772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keller, A.; Rohde, J.F.; Raymond, K.; Heitmann, B.L. Association between periodontal disease and overweight and obesity: A systematic review. J. Periodontol. 2015, 86, 766–776. [Google Scholar] [CrossRef] [PubMed]
- Nascimento, G.G.; Leite, F.R.; Do, L.G.; Peres, K.G.; Correa, M.B.; Demarco, F.F.; Peres, M.A. Is weight gain associated with the incidence of periodontitis? A systematic review and meta-analysis. J. Clin. Periodontol. 2015, 42, 495–505. [Google Scholar] [CrossRef] [PubMed]
- Papageorgiou, S.N.; Reichert, C.; Jager, A.; Deschner, J. Effect of overweight/obesity on response to periodontal treatment: Systematic review and a meta-analysis. J. Clin. Periodontol. 2015, 42, 247–261. [Google Scholar] [CrossRef]
- Khan, S.; Barrington, G.; Bettiol, S.; Barnett, T.; Crocombe, L. Is overweight/obesity a risk factor for periodontitis in young adults and adolescents? A systematic review. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2018, 19, 852–883. [Google Scholar] [CrossRef]
- Da Silva, F.G.; Pola, N.M.; Casarin, M.; Silva, C.F.E.; Muniz, F. Association between clinical measures of gingival inflammation and obesity in adults: Systematic review and meta-analyses. Clin. Oral. Investig. 2021, 25, 4281–4298. [Google Scholar] [CrossRef]
- Foratori-Junior, G.A.; Pereira, P.R.; Gasparoto, I.A.; de Carvalho Sales-Peres, S.H.; Storniolo de Souza, J.M.; Khan, S. Is overweight associated with periodontitis in pregnant women? Systematic review and meta-analysis. Jpn. Dent. Sci. Rev. 2022, 58, 41–51. [Google Scholar] [CrossRef]
- Aronson, D.; Bartha, P.; Zinder, O.; Kerner, A.; Markiewicz, W.; Avizohar, O.; Brook, G.J.; Levy, Y. Obesity is the major determinant of elevated C-reactive protein in subjects with the metabolic syndrome. Int. J. Obes. Relat. Metab. Disord. J. Int. Assoc. Study Obes. 2004, 28, 674–679. [Google Scholar] [CrossRef] [Green Version]
- Zelkha, S.A.; Freilich, R.W.; Amar, S. Periodontal innate immune mechanisms relevant to atherosclerosis and obesity. Periodontol. 2000 2010, 54, 207–221. [Google Scholar] [CrossRef] [Green Version]
- Nishimura, F.; Murayama, Y. Periodontal inflammation and insulin resistance--lessons from obesity. J. Dent. Res. 2001, 80, 1690–1694. [Google Scholar] [CrossRef] [PubMed]
- Thomas, J.T.; Thomas, T.; Ahmed, M.; Kannan, S.K.; Abdullah, Z.; Alghamdi, S.A.; Joseph, B. Prevalence of Periodontal Disease among Obese Young Adult Population in Saudi Arabia-A Cross-Sectional Study. Medicina 2020, 56, 197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lundin, M.; Yucel-Lindberg, T.; Dahllof, G.; Marcus, C.; Modeer, T. Correlation between TNFalpha in gingival crevicular fluid and body mass index in obese subjects. Acta. Odontol. Scand. 2004, 62, 273–277. [Google Scholar] [CrossRef] [PubMed]
- Usui, M.; Onizuka, S.; Sato, T.; Kokabu, S.; Ariyoshi, W.; Nakashima, K. Mechanism of alveolar bone destruction in periodontitis—Periodontal bacteria and inflammation. Jpn. Dent. Sci. Rev. 2021, 57, 201–208. [Google Scholar] [CrossRef]
- Alabdulkarim, M.; Bissada, N.; Al-Zahrani, M.; Ficara, A.; Siegel, B. Alveolar bone loss in obese subjects. J. Int. Acad. Periodontol. 2005, 7, 34–38. [Google Scholar]
- Zhu, J.; Guo, B.; Gan, X.; Zhang, L.; He, Y.; Liu, B.; Chen, X.; Zhang, S.; Yu, H. Association of circulating leptin and adiponectin with periodontitis: A systematic review and meta-analysis. BMC Oral. Health 2017, 17, 104. [Google Scholar] [CrossRef] [Green Version]
- Falagas, M.E.; Kompoti, M. Obesity and infection. Lancet. Infect. Dis. 2006, 6, 438–446. [Google Scholar] [CrossRef]
- Suresh, S.; Mahendra, J. Multifactorial relationship of obesity and periodontal disease. J. Clin. Diagn. Res. JCDR 2014, 8, ZE01–ZE03. [Google Scholar] [CrossRef]
- Nishida, N.; Tanaka, M.; Hayashi, N.; Nagata, H.; Takeshita, T.; Nakayama, K.; Morimoto, K.; Shizukuishi, S. Determination of smoking and obesity as periodontitis risks using the classification and regression tree method. J. Periodontol. 2005, 76, 923–928. [Google Scholar] [CrossRef]
- Saito, T.; Shimazaki, Y.; Sakamoto, M. Obesity and periodontitis. N. Engl. J. Med. 1998, 339, 482–483. [Google Scholar] [CrossRef]
- Sangachin, M.G.; Cavuoto, L.A.; Wang, Y. Use of various obesity measurement and classification methods in occupational safety and health research: A systematic review of the literature. BMC Obes. 2018, 5, 28. [Google Scholar] [CrossRef]
- Saito, T.; Shimazaki, Y.; Koga, T.; Tsuzuki, M.; Ohshima, A. Relationship between upper body obesity and periodontitis. J. Dent. Res. 2001, 80, 1631–1636. [Google Scholar] [CrossRef] [PubMed]
- Brochu, M.; Starling, R.D.; Tchernof, A.; Matthews, D.E.; Garcia-Rubi, E.; Poehlman, E.T. Visceral adipose tissue is an independent correlate of glucose disposal in older obese postmenopausal women. J. Clin. Endocrinol. Metab. 2000, 85, 2378–2384. [Google Scholar] [CrossRef] [PubMed]
- Nascimento, G.G.; Peres, M.A.; Mittinty, M.N.; Peres, K.G.; Do, L.G.; Horta, B.L.; Gigante, D.P.; Correa, M.B.; Demarco, F.F. Diet-Induced Overweight and Obesity and Periodontitis Risk: An Application of the Parametric G-Formula in the 1982 Pelotas Birth Cohort. Am. J. Epidemiol. 2017, 185, 442–451. [Google Scholar] [CrossRef] [Green Version]
- Merchant, A.T.; Pitiphat, W.; Rimm, E.B.; Joshipura, K. Increased physical activity decreases periodontitis risk in men. Eur. J. Epidemiol. 2003, 18, 891–898. [Google Scholar] [CrossRef]
- Pischon, T.; Hankinson, S.E.; Hotamisligil, G.S.; Rifai, N.; Rimm, E.B. Leisure-time physical activity and reduced plasma levels of obesity-related inflammatory markers. Obes. Res. 2003, 11, 1055–1064. [Google Scholar] [CrossRef]
- Saxlin, T.; Ylostalo, P.; Suominen-Taipale, L.; Mannisto, S.; Knuuttila, M. Association between periodontal infection and obesity: Results of the Health 2000 Survey. J. Clin. Periodontol. 2011, 38, 236–242. [Google Scholar] [CrossRef]
- Bawadi, H.A.; Khader, Y.S.; Haroun, T.F.; Al-Omari, M.; Tayyem, R.F. The association between periodontal disease, physical activity and healthy diet among adults in Jordan. J. Periodontal Res. 2011, 46, 74–81. [Google Scholar] [CrossRef]
- Khan, S.; Bettiol, S.; Kent, K.; Barnett, T.; Peres, M.; Crocombe, L.A. Obesity and periodontitis in Australian adults: A population-based cross-sectional study. Int. Dent. J. 2020, 70, 53–61. [Google Scholar] [CrossRef]
- Natto, Z.S.; Ahmad, R.H.A.; Alsharif, L.T.; Alrowithi, H.F.; Alsini, D.A.; Salih, H.A.; Bissada, N.F. Chronic Periodontitis Case Definitions and Confounders in Periodontal Research: A Systematic Assessment. Biomed Res. Int. 2018, 2018, 4578782. [Google Scholar] [CrossRef] [Green Version]
- Owens, D.K.; Lohr, K.N.; Atkins, D.; Treadwell, J.R.; Reston, J.T.; Bass, E.B.; Chang, S.; Helfand, M. AHRQ series paper 5: Grading the strength of a body of evidence when comparing medical interventions—Agency for healthcare research and quality and the effective health-care program. J. Clin. Epidemiol. 2010, 63, 513–523. [Google Scholar] [CrossRef] [PubMed]
- Suresh, K.; Thomas, S.V.; Suresh, G. Design, data analysis and sampling techniques for clinical research. Ann. Indian Acad. Neurol. 2011, 14, 287–290. [Google Scholar] [CrossRef] [PubMed]
- Perlstein, M.I.; Bissada, N.F. Influence of obesity and hypertension on the severity of periodontitis in rats. Oral. Surg. Oral. Med. Oral. Pathol. 1977, 43, 707–719. [Google Scholar] [CrossRef]
- Azuma, T.; Tomofuji, T.; Endo, Y.; Tamaki, N.; Ekuni, D.; Irie, K.; Kasuyama, K.; Kato, T.; Morita, M. Effects of exercise training on gingival oxidative stress in obese rats. Arch. Oral. Biol. 2011, 56, 768–774. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Sl no | Author/Year Country/Study Design | Study Subjects | Age Range (Mean) Male/Female | Body Composition Criteria (BMI) | Definition of Periodontitis Used | Secondary Parameters (Tooth Loss, BOP) | Sampling Method | Inclusion of Smokers/Diabetics | Main Observations |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Dalla et al. 2005 [35] Brazil Cross-sectional study | 706 individuals (131 normal/ 134 overweight/ 64 obese | 30–65 years 329 males 377 females | * Four BMI categories (WHO criteria) | Individuals with ≥30% teeth with attachment loss ≥5 mm | Not mentioned | Multistage probability sampling method | Smokers and Diabetes (self-reported) | Higher risk of periodontitis among obese females than normal females (OR = 2.1). There is no significant association between overweight and periodontitis among females and the age group above 35 years—more pronounced association of BMI and periodontitis in non-smokers. |
| 2 | Sarlati et al. 2008 [43] Iran Case-control study | 80 young volunteers (40 normal/40 overweight/obese) | 18–34 years; obese individuals (29.1 + 4.7 years) and normal individuals (24 + 5 years) 10 males 70 females | * Four BMI categories (WHO criteria) | PPD and CAL | Not mentioned | Not mentioned | Smokers and Diabetes (self-reported) | Positive correlations between BMI and PPD (R = 0.33) BMI and CAL (R = 0.39). Not adjusted for confounding. |
| 3 | Khader et al. 2009 [36] Jordan Cross-sectional study | 340 persons (13 underweight/108 normal/115 overweight/104 obese) | 18–70 years 168 males 172 females | * Two BMI categories (WHO criteria) obese and overweight | Four or more teeth with one or more sites with PPD ≥4 mm, CAL ≥ 3 mm. | Obese patients had a significantly higher average of GI. | Systematic random sampling | Smokers and Diabetes (self-reported) | Higher risk of periodontitis in obese patients (OR = 2.9; CI 1.3, 6.1). Insignificant association between smoking and the prevalence of periodontal disease. |
| 4 | Amin 2010 [37] Egypt Cross-sectional study | 380 adults (92 normal/161 overweight/127 obese) | 20–26 years 170 males 210 females | * 3 BMI categories (WHO criteria) normal weight, overweight, obese | CAL, GI, and CPI | Significant correlation between BMI and G.I. | Not mentioned | No | High correlation between CAL and BMI (r = 0.9, p < 0.01) in young females than in males. |
| 5 | Pataro et al. 2012 [42] Brazil Cross-sectional study | 594 females (352 normal/54 overweight/48 obesity level I/56 obesity level II/74 obesity level III) | 18–65 years; 39.7 ± 17.35 years 594 females | Normal weight (BMI 20–24.99 kg/m2) overweight (BMI 25–29.99 kg/m2), ** obesity level I, obesity level II and obesity level III (WHO 1997) | Proximal CAL ≥ 4 mmin two or more teeth, or proximal PD ≥ 5 mm in two or more teeth (Page et al. 2007) | BOP was more prevalent in the obese group III (34.8%, p < 0.001) | Convenience sampling | Both were included but unclear how it was evaluated. | Statistically significant differences in BOP, PPD, CAL ≥ 4 mm (p < 0.05) among obese and overweight women as compared to women with normal BMI. BMI > 30 kg/m2 interacted with diabetes (4.03), and smoking (15.79) (p < 0.03). The association was more evident as obesity increased. |
| 6 | Budduneli et al. 2014 [44] Turkey Case-control study | 91 females (31 normal and 60 obese) | 43.10 ± 10.87 years 91 females only | Obesity is diagnosed based on the WHO criteria (not specified) | Not clearly defined. PPD, CAL, and dichotomous BOP (present or absent within 10 s after probing) recorded | Not mentioned | Not mentioned | Smokers (self-reported). Diabetes excluded. | BMI did not correlate to clinical periodontal parameters in the obese group (but correlated with serum levels of inflammatory molecules (p < 0.05). Smokers (obese and non-obese) did not show significant differences in P.D., BOP, and PI (p > 0.05). Obese non-smokers had higher periodontitis CAL, BOP and PI (p < 0.05). PD was the same in obese and control groups of non-smokers. |
| 7 | Gaio et al. 2016 [45] Brazil Cohort study | 583 individuals (297 normal/177 overweight/108 obese) | 36.02 ± 14.97 years 333 males 249 females | * Four BMI categories (WHO criteria) | Proximal PAL ≥ 3 mm in ≥ 4 teeth over the 5 years of follow-up. | Not mentioned | Multistage probability sampling strategy | Smokers (self-reported) Diabetes excluded. | Higher risk of PAL in obese females than normal weight females (R.R. = 1.64, 95% CI = 1.11–2.43) and males. No statistically significant associations were observed between obesity and PAL progression for never or ever smokers. |
| 8 | Deshpande and Amrutiya 2017 [38] India Cross-sectional study | 100 patients with chronic generalized periodontitis/gingivitis (50 normal/50 obese) | 18–63 years Mean age 34.14 ± 11.70 (non-obese) and 34.02 ± 9.03 (obese) 63 males 37 females | Obese (BMI > 30) Non-obese (BMI < 30) | PPD and CAL | Not mentioned | Convenience sampling | Unclear | Higher prevalence of periodontitis in obese patients than in the control group (p < 0.05 for PPD, and p < 0.031 for CAL). |
| 9 | Nascimento et al. 2017 [47] Brazil Cohort study | 1076 individuals | 20–59 years 463 males 603 females | Obese (BMI ≥ 25 Kg/m2) | Combination of CAL and BOP | Tooth loss was mentioned but not mentioned if due to periodontal disease | Not mentioned | Smokers and diabetes (self-reported) | A higher risk of attachment loss and BOP in obese patients presented (RR 1.45 for AL and BOP in different teeth; RR 1.84 for AL and BOP in the same tooth). |
| 10 | Santos et al. 2019 [40] Brazil Cross-sectional study | 236 individuals (156 normal/ 69 overweight 80 obese | 18–34; 35 and above 52 males 184 females | * Two BMI categories (WHO criteria) overweight, obese. | Based on CDC-AAP case classification | Not mentioned | Not mentioned | Smokers (self-reported) Diabetes excluded. | Positive association between severe periodontitis and obesity (OR = 3.25, 95% CI = 1.27–8.31, p = 0.01) but not with overweight (p = 0.59). |
| 11 | Gulati et al. 2020 [39] India Cross-sectional study | 317 individuals (52 overweight/ 251 obesity I/ 9 obesity II 5 obesity III) | 25–70 years 203 males 114 females | ** Obese Class I, Class II, Class III | Four or more teeth with one site or more with PPD ≥ 4 mm and CAL ≥ 3 mm was present. | Not mentioned | Not mentioned | Unclear | Deeper PD was significantly associated with obesity determinants, especially among Class 2 and Class 3 obese individuals with chronic periodontitis. |
| 12 | Maulani et al. 2021 [41] Indonesia Cross-sectional study | 262 individuals (135 normal/ 127 overweight or obese) | 18–66 years 105 males 157 females | * Four BMI categories (WHO criteria by the Asia-Pacific perspective) | CAL 5 mm and PD 6 mm were cut-off measurements between mild and severe periodontitis | Yes; not associated with increased BMI | Consecutive sampling | Yes, but unclear how it was recorded | Increased BMI showed a positive correlation with periodontitis of all severity. (aOR = 1.88, 95%CI 1.05-3.37; p < 0.05). Lower BMI is found in smokers than in non-smokers. |
| 13 | Carneiro et al. 2022 [34] Brazil Cross-sectional study | 345 individuals (133 normal/ 106 obese) | 49.08 years (±) 14.26 92 males 253 females | * Six BMI categories (WHO criteria) low weight, normal weight, overweight, ** obese I, obese II, obese III | CDC/AAP criteria | Not mentioned | Not mentioned | Smokers (self-reported) Unclear how diabetes was recorded. | Females and younger participants showed a positive association between obesity and periodontitis. |
| 14 | Cetin et al. 2022 [48] Turkey Retrospective study | 142 with periodontitis (59 normal/62 overweight/21 obese) | above 18; 57.24 ± 8.78 82 males 60 females | * Three BMI categories (WHO criteria) normal weight, overweight, obese | interdental CAL at the site of greatest loss (staging and grading) | number of remaining teeth | not mentioned | Smokers (self-reported) Diabetic status obtained from the ‘patient’s hospital records. | CAL (p < 0.001), PPD (p < 0.05), PI (p < 0.05)), stage and grade of periodontitis (p < 0.05) were higher overweight and obese patients. BMI and smoking status showed no significant association (p = 0.142). Overweight and obese patients were at higher risk of developing stage III–IV periodontitis |
| 15 | Linden et al. 2007 [46] UK. Retrospective cohort study | 1362 males (336 normal/ 728 overweight/ 298 obese) | 60–70 years; 64 ± 2.9 1362 males | Four BMI categories (WHO criteria) | High-threshold periodontitis was identified when ≥ 15% of all sites measured had a loss of attachment ≥6 mm, and there was at least one site with deep pocketing (≥6 mm). | Tooth loss mentioned | the multistage probability sampling method. | Smokers and Diabetes (self-reported) | Strong association between BMI and high-threshold periodontitis for heavy smokers (OR 4.21, 95% CI% 2.04–8.72, p 0.0001) and light smokers (OR 3.22, 95% CI% 1.76–5.88, p 0.0001) among older men. High BMI levels in early life did not predict periodontitis in later life in the men studied. |
| Sl No | Author and Year Country | Study Subjects | Parameters Studies | Major Observations |
|---|---|---|---|---|
| 1 | Amar et al. 2007 [50] USA | DIO mice and lean control C57BL/6 mice were infected orally | Oral microbial sampling, inflammatory response, (TNF-alpha, IL-6, and serum amyloid A (SAA). | Obesity causes immune dysregulation. It also interferes with the ability of the immune system to respond to P. gingivalis infection. Increased alveolar bone loss after bacterial infection was observed in mice with DIO. |
| 2 | Simch et al. 2008 [57] Brazil | 30 female Wistar rat. Test group (n = 14 rats on cafeteria diet) control group (n = 16 on regular). | Morphometric analysis of alveolar bone loss by standardized digital photographs (software Image Tool 3.0). | No statistically significant differences between alveolar bone loss of test animals and controls. Progression of alveolar bone loss in rats not influenced by obesity. |
| 3 | Tomofuji et al. 2009 [59] Japan | 28 rats. The obese Zucker rats (n = 14) lean littermates (n = 14) | 8-hydroxydeoxyguanosine, ratio of reduced/oxidized glutathione, serum level of reactive oxygen metabolites, gingival gene-expression pattern. | Obese rats had higher levels of gingival 8-hydroxydeoxyguanosine. There was also a decreased ratio of reduced/oxidized glutathione with increasing serum reactive oxygen metabolites. No significant differences in the degree of alveolar bone loss between lean and obese rats Gene expressions related to a capacity for xenobiotic detoxification were downregulated in obese rats. |
| 4 | Verzeletti et al. 2012 [58] Brazil | 24 female Wistar rats cafeteria diet (n = 13) regular diet (n = 11) | Body weight, Morphometric registration of alveolar bone loss. | Alveolar bone loss was not statistically different between obese and non-obese group |
| 5 | Brandelero et al. 2012 [61] Brazil | 20 newborn male Wistar rats MSG group (n = 10) Control group (n-10) | Radiographic analyses of alveolar bone resorption, Tumor Necrosis Factor α (TNFα), Gene expression in gingival tissue. | The alveolar bone resorption was 44% lower in MSG-obese rats compared with control rats. Hypothalamic obesity may produce a protective effect against periodontal disease |
| 6 | Cavagni et al. 2013 [52] Brazil | 28 Wistar rats. Control group (n = 10) Test group (cafeteria diet: n = 10) | Morphometric analysis of standard digital photographs, Mean alveolar bone loss. | Animals in the test group showed 20 sites with spontaneous periodontal disease, whereas in control animals, only 8 sites exhibited periodontal breakdown. Obesity increases the occurrence of spontaneous periodontal disease in Wistar rats. |
| 7 | Cavagni et al. 2016 [51] Brazil | 60 male Wistar rats. Control group (n = 15) periodontitis (n = 15) obesity/hyperlipidemia (n = 15) obesity/hyperlipidemia plus periodontitis (n = 15). | Body weight and Lee index, Serum glucose and cholesterol/ triglycerides, alveolar bone loss (micro CT), Serum tumor necrosis factor (TNF)-α, Interleukin (IL)-1β. | Groups exposed to CAF exhibited higher ABL in the sides without ligature. No differences were observed among groups for IL-1β and TNF-α. Obesity and hyperlipidemia modulate the host response to challenges in the periodontium, increasing the expression of periodontal breakdown. |
| 8 | Muluke et al. 2016 [53] USA | Four-week-old male C57BL/6 mice (n = 10 per group) high-fat diet (HFD) normal caloric diet | percentage fat, serum inflammation (TNF-α, OC, CTX, P1NP markers | Alveolar bone loss was significantly greater in obese animals. Osteoclasts also showed an augmented inflammatory response to P. gingivalis in obese animals. High-fat diet was more important than obesity in affecting alveolar bone loss. |
| 9 | Zuza et al. 2018 [54] Brazil | 48 adult Wistar rats High fat diet group (n = 24) Normal diet group (n = 24) | Histopathological, histometric, and immunohistochemical analyses. TRAP, RANKL, OPG via immunolabeling. | Histology shows that inflammation lasted longer in obese rats. Obesity induced by a high-fat diet caused more severe local inflammatory response and alveolar bone loss. |
| 10 | Damanaki et al. 2018 [55] Germany | 12 C57BL/6 mice Younger lean mice (n = 4) Older lean mice (n = 4) Younger obese mice (n = 4) | IL-6, COX-2, visfatin and adiponectin in gingival samples (real-time PCR) | Alveolar bone loss was significantly lower in the older mice as compared to the younger animals. Gingival COX-2 and visfatin expressions were higher in the obese versus lean mice and in the older versus younger mice |
| 11 | Damanaki et al. 2021 [56] Germany | 15 Wistar rats High-fat diet (n = 15) Normal diet (n = 15) | Histomorphometry to assess healing, TRAP staining and immuno-histochemistry for RUNX2 and osteopontin. | Spontaneous bone healing in periodontal defects is affected by obesity even in the presence of regeneration-promoting molecules like EMD. |
| 12 | Lopes et al. 2022 [60] Brazil | 16 Holtzman rats were ligature-induced periodontitis (n = 8). Obesity plus ligature-induced periodontitis (O.P.) (n = 8) | Body weight, adipose tissue weight, and blood test, Bone loss (micro-CT and histologic analyses), Proteome analysis from the periodontal ligament tissues (PDL), Immunohistochemistry for spondin1, vinculin, and TRAP. | Histologically, it was found that obesity did not significantly affect bone loss resulting from periodontitis. Obesity affects the proteome of PDL submitted to experimental periodontitis. |
| Sl. No | Author/Year/Country | Number of Studies | Study Period | Major Observations |
|---|---|---|---|---|
| 1 | Chaffee and Weston 2010 [5] USA | 57 | Up to 2010 | In total, 41 studies suggested a positive association consistent with a biologically plausible role for obesity in the development of periodontal disease. The fixed-effects summary odds ratio was 1.35, with some evidence of a stronger association among younger adults, women, and non-smokers. Also, a greater mean CAL among obese individuals, a higher mean BMI among periodontal patients, and a trend of increasing odds of prevalent periodontal disease with increasing BMI. |
| 2 | Suvan et al. 2011 [10] U.K. | 33 | Up to 2009 | There were 19 studies included in the meta-analyses. Statistically significant associations between periodontitis and BMI category obese OR 1.81(1.42, 2.30), overweight OR 1.27(1.06, 1.51), and obese and overweight combined OR 2.13(1.40, 3.26). Support an association between BMI overweight and obesity and periodontitis, although the magnitude is unclear. |
| 3 | Moura-Grec et al. 2014 [62] Brazil | 31 | Up to 2010 | A positive association in 25 studies (not associated in 6 studies). The meta-analysis showed a significant association with obesity and periodontitis (OR = 1.30 [95% Confidence Interval (CI), 1.25–1.35]) and with mean BMI and periodontal disease (mean difference = 2.75). Obesity was associated with periodontitis, however, the risk factors that aggravate these diseases should be better clarified to elucidate the direction of this association. |
| 4 | Keller et al. 2015 [63] Denmark | 13 | Up to June 2014 | Two longitudinal studies found a direct association between being overweight and the subsequent risk of developing periodontitis. Three studies found a direct association between obesity and the development of periodontitis among adults. Two intervention studies on the influence of obesity on periodontal treatment effects found that the response to non-surgical periodontal treatment was better among lean than obese patients. The remaining three studies did not report treatment differences between obese and lean participants. Among the eight longitudinal studies, one study adjusted for C-reactive protein (CRP), and biologic markers of inflammation such as CRP, interleukin-6, and tumor necrosis factor-α, and inflammation markers were analyzed separately in three of the five intervention studies. This systematic review suggests that overweight, obesity, weight gain, and increased waist circumference may be risk factors for the development of periodontitis or worsening of periodontal measures. |
| 5 | Nascimento et al. 2015 [64] Brazil | 5 | Up to Feb 2015 | Subjects who became overweight and obese presented a higher risk of developing new cases of periodontitis (RR 1.13; 95%CI 1.06–1.20 and RR 1.33 95%CI 1.21–1.47 respectively) compared with counterparts who stayed at a normal weight. A clear positive association between weight gain and new cases of periodontitis was found. However, these results originated from limited evidence. Thus, more studies with prospective longitudinal designs are needed. |
| 6 | Papageorgiou et al. 2015 [65] Germany | 15 | Up to July 2013 | No difference was found in clinical periodontal parameters, but significant differences in inflammatory or metabolic parameters were found between overweight/obese and normal-weight patients. Existing evidence is weak. |
| 7 | Martinez-Herrera et al. 2017 [9] Spain | 28 | 2000-2017 | A total of 26 studies described an association between obesity and periodontal disease (no association n = 2). The development of insulin resistance as a consequence of a chronic inflammatory state and oxidative stress could be implicated in the association between obesity and periodontitis. |
| 8 | Khan et al. 2018 [66] Australia | 25 | 2003 and 2016 | There were 25 eligible studies from 12 countries. 17 showed an association between obesity and periodontitis (odds ratios ranged from 1.1 to 4.5). The obesity indicators of BMI, waist circumference, waist-hip ratio, and body fat percentage were significantly associated with measures of periodontitis of bleeding on probing, plaque index, probing depths, clinical attachment loss, calculus, oral hygiene index, and community periodontal index. Two prospective cohort studies in the review showed no significant association between obesity and periodontitis, but these studies had limitations in study design and used inappropriate epidemiological diagnostic measures of periodontitis. Evidence suggests that obesity is associated with periodontitis in adolescents and young adults. |
| 9 | da Silva et al. 2021 [67] Brazil | 92 | upto Jan 2021 | Ninety studies were included (cross-sectional/clinical trials [n = 82], case-control [n = 3], cohorts [n = 5]). Most of the studies demonstrated no significant difference in the measures of gingival inflammation regardless of the comparison performed. Meta-analysis showed that among individuals with periodontitis, significantly higher levels of gingival inflammation are observed in those with obesity (n of individuals = 240) when compared to those who were not obese (n of individuals = 574) (SMD:0.26; 95%CI:0.07–0.44). When considering population-based/those studies that did not provide periodontal diagnosis, significantly higher measures of gingival inflammation were observed in the groups with higher BMI. |
| 10 | Foratori-Junior et al. 2022 [68] Brazil | 11 | 2000–2021 | 11 studies were included. Most studies had a low risk of bias. A positive association between overweight/obesity and periodontitis was found, with an average of 61.04% of women with overweight/obesity and periodontitis, showing the overall random-effects relative risk and 95% CI of 2.21 (1.53–3.17) (p < 0.001). A positive association was found between overweight/obesity and periodontitis during pregnancy. |
| (a) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Cross-Sectional Studies | ||||||||||
| Sl. No | Author; Year | Selection | Comparability | Outcome | Total (Out of 10) | |||||
| Representativeness of the sample | Sample size | Non-respondents | Ascertainment of the exposure (risk factor): | Comparability of different outcome groups based on the design or analysis | Ascertainment of outcome | The same method of ascertainment for cases and controls | ||||
| 1 | Dalla et al. 2005 [35] | 1 | 1 | 1 | 2 | 2 | 1 | 1 | 9 (low bias) | |
| 2 | Khader et al. 2009 [36] | 1 | 1 | 1 | 2 | 2 | 1 | 1 | 9 (low bias) | |
| 3 | Amin 2010 [37] | 1 | 1 | 0 | 2 | 0 | 1 | 0 | 5 (high bias) | |
| 4 | Pataro et 2012 [42] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 7 (moderate bias) | |
| 5 | Deshpande and Amrutiya 2017 [38] | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 6 (high bias) | |
| 6 | Santos et al. 2019 [40] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 7 (moderate bias) | |
| 7 | Gulati et al. 2020 [39] | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 5 (high bias) | |
| 8 | Maulani et al. 2021 [41] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 7 (moderate bias) | |
| 9 | Carneiro et al. 2022 [34] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 7 (moderate bias) | |
| (b) | ||||||||||
| Case Control Studies | ||||||||||
| Sl. No | Author; Year | Selection | Comparability | Exposure | Total (out of 9) | |||||
| Adequate definition | Representativeness of case | Selection of Control | Definition of control | Comparability of cases and controls based on the design or analysis | Ascertainment of exposure | The same method of ascertainment for cases and controls | Non-response rate | |||
| 1 | Sarlati et al. 2008 [43] | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 0 | 6 (moderate bias) |
| 2 | Budduneli et al. 2014 [44] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 8 (low bias) |
| Cohort Studies | ||||||||||
| Sl. No | Author; Year | Selection | Comparability | Outcome | Total (out of 9) | |||||
| Representativeness of the exposed cohort | Selection of the non-exposed cohort | Ascertainment of exposure | Shows that outcome of interest was not present at the start of the study | Comparability of cohorts based on the design or analysis | Assessment of outcome | Was follow-up long enough for outcomes to occur | Adequacy of follow-up of cohorts | |||
| 1 | Liden et al. 2007 [46] | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 1 | 9 (low bias) |
| 2 | Gaio et al. 2016 [45] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 8 (low bias) |
| 3 | Nascimento et al. 2017 [47] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 8 (low bias) |
| 4 | Cetin et al. 2022 [48] | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 7 (low bias) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abu-Shawish, G.; Betsy, J.; Anil, S. Is Obesity a Risk Factor for Periodontal Disease in Adults? A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 12684. https://doi.org/10.3390/ijerph191912684
Abu-Shawish G, Betsy J, Anil S. Is Obesity a Risk Factor for Periodontal Disease in Adults? A Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(19):12684. https://doi.org/10.3390/ijerph191912684
Chicago/Turabian StyleAbu-Shawish, Ghadah, Joseph Betsy, and Sukumaran Anil. 2022. "Is Obesity a Risk Factor for Periodontal Disease in Adults? A Systematic Review" International Journal of Environmental Research and Public Health 19, no. 19: 12684. https://doi.org/10.3390/ijerph191912684
APA StyleAbu-Shawish, G., Betsy, J., & Anil, S. (2022). Is Obesity a Risk Factor for Periodontal Disease in Adults? A Systematic Review. International Journal of Environmental Research and Public Health, 19(19), 12684. https://doi.org/10.3390/ijerph191912684