
Coping Strategies Furthering Post-Traumatic Growth in Multiple Sclerosis: A Longitudinal Study

Abstract
1. Introduction
2. Materials and Methods
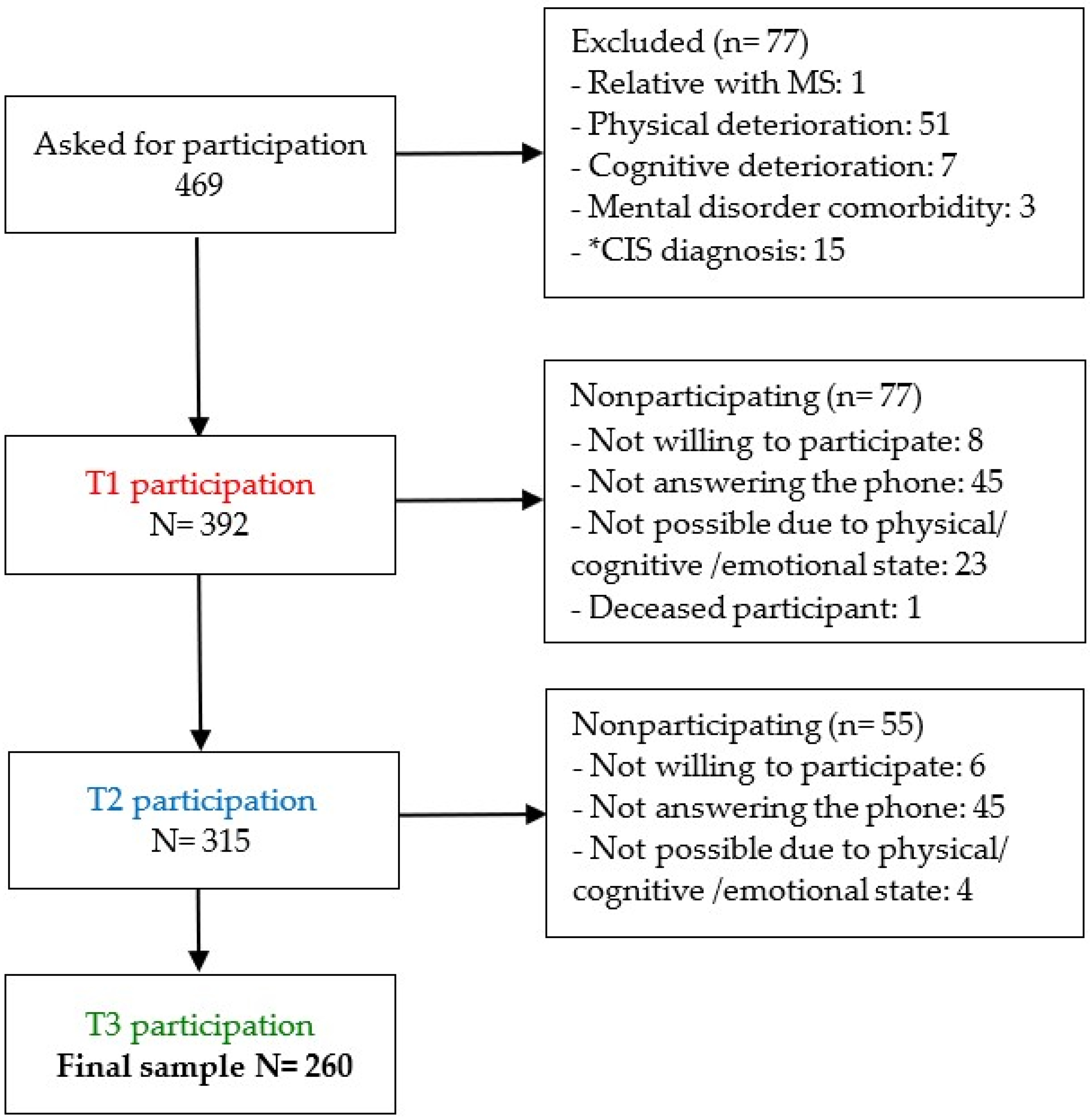
2.1. Participants and Procedure
2.2. Instruments
2.2.1. Post-Traumatic Growth
2.2.2. Coping Strategies
2.2.3. Expanded Disability Status Scale (EDSS)
2.3. Statistical Analysis
3. Results
3.1. Post-Traumatic Growth Levels and Assessment Time on Coping Strategies
3.1.1. Effects of Post-Traumatic Growth and Assessment Time on Coping Strategies
3.1.2. Main Effects: Post-Traumatic Growth Level Effect on Coping Strategies
3.1.3. Main Effects: Assessment Time on Coping Strategies
3.2. Predictors of Post-Traumatic Growth
4. Discussion
4.1. Post-Traumatic Growth Levels and Assessment Time on Coping Strategies
4.1.1. Interaction Effects
4.1.2. Main Effect of Post-Traumatic Growth Level on Coping Strategies
4.1.3. Effect of Assessment Time on Coping Strategies
4.2. Predictors of Post-Traumatic Growth
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hosseini, Z.; Homayuni, A.; Etemadifar, M. Barriers to quality of life in patients with multiple sclerosis: A qualitative study. BMC Neurol. 2022, 22, 174. [Google Scholar] [CrossRef] [PubMed]
- Faraclas, E.; Lynn, J.; Lau, J.D.; Merlo, A. Health-related quality of life in people with multiple sclerosis: How does this population compare to population-based norms in different health domains? J. Patient Rep. Outcomes 2022, 6, 12. [Google Scholar] [CrossRef] [PubMed]
- Gil-González, I.; Martín-Rodríguez, A.; Conrad, R.; Pérez-San-Gregorio, M.A. Quality of life in adults with multiple sclerosis: A systematic review. BMJ Open 2020, 10, e041249. [Google Scholar] [CrossRef] [PubMed]
- Kivi, M.S.; Jamei-Moghadam, M.; Khoshlahni, H.; Heidarzadeh, M.; Kamran, A.; Shahabi, H. Psychological changes in patients with multiple sclerosis. J. Holist. Nurs. Midwifery 2019, 29, 308–313. [Google Scholar] [CrossRef]
- Tedeschi, R.G.; Calhoun, L.G. Posttraumatic growth: Conceptual foundations and empirical evidence. Psychol. Inq. 2004, 15, 1–18. [Google Scholar] [CrossRef]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal, and Coping; Springer: New York, NY, USA, 1984. [Google Scholar]
- Henson, C.; Truchot, D.; Canevello, A. What promotes post traumatic growth? A systematic review. Eur. J. Trauma Dissoc. 2021, 5, 100195. [Google Scholar] [CrossRef]
- Prati, G.; Pietrantoni, L. Optimism, social support, and coping strategies as factors contributing to posttraumatic growth: A meta-analysis. J. Loss Trauma 2009, 14, 364–388. [Google Scholar] [CrossRef]
- Barskova, T.; Oesterreich, R. Post-traumatic growth in people living with a serious medical condition and its relations to physical and mental health: A systematic review. Disabil. Rehabil. 2009, 31, 1709–1733. [Google Scholar] [CrossRef]
- Kim, J.; Han, A.; Piatt, J.A.; Kim, J. Investigating relationships among coping, personal growth, and life satisfaction among individuals with physical disabilities. Health Promot. Perspect. 2020, 10, 401–408. [Google Scholar] [CrossRef]
- O’Connor, S.; Hevey, D.; O’Keeffe, F. Illness perceptions, coping, health-related quality of life and psychological outcomes in cervical dystonia. J. Clin. Psychol. Med. Settings 2022. [Google Scholar] [CrossRef]
- Arjeini, Z.; Zeabadi, S.M.; Hefzabad, F.H.; Shahsavari, S. The relationship between posttraumatic growth and cognitive emotion regulation strategies in hemodialysis patients. Int. J. Health Promot. Educ. 2020, 9, 167. [Google Scholar] [CrossRef]
- Schwartz, J.R.; Thomas, E.B.K.; Juckett, M.B.; Costanzo, E.S. Predictors of posttraumatic growth among hematopoietic cell transplant recipients. Psycho-Oncology 2022, 31, 1013–1021. [Google Scholar] [CrossRef] [PubMed]
- Pérez-San-Gregorio, M.Á.; Martín-Rodríguez, A.; Borda-Mas, M.; Avargues-Navarro, M.L.; Pérez-Bernal, J.; Gómez-Bravo, M.A. Coping strategies in liver transplant recipients and caregivers according to patient posttraumatic growth. Front. Psychol. 2017, 8, 18. [Google Scholar] [CrossRef] [PubMed]
- Rogan, C.; Fortune, D.G.; Prentice, G. Post-traumatic growth, illness perceptions and coping in people with acquired brain injury. Neuropsychol. Rehabil. 2013, 23, 639–657. [Google Scholar] [CrossRef] [PubMed]
- Baka, C.; Chatira, K.; Karademas, E.C.; Kafetsios, K.G. Patients’ perspective on the psychological impact of multiple sclerosis on their life. Illn. Crisis Loss 2021, 30, 659–673. [Google Scholar] [CrossRef]
- Aflakseir, A.; Manafi, F. Posttraumatic growth and its relationship with cognitive emotion regulation strategies in patients with multiple sclerosis in shiraz. Iran. Pract. Clin. Psychol. 2018, 6, 57–62. [Google Scholar] [CrossRef]
- Pakenham, K.I. Benefit finding in multiple sclerosis and associations with positive and negative outcomes. Health Psychol. 2005, 24, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Gil-González, I.; Pérez-San-Gregorio, M.Á.; Conrad, R.; Martín-Rodríguez, A. Beyond the boundaries of disease-significant post-traumatic growth in multiple sclerosis patients and caregivers. Front. Psychol. 2022, 13, 903508. [Google Scholar] [CrossRef] [PubMed]
- Kassie, S.A.; Alia, J.; Hyland, L. Biopsychosocial implications of living with multiple sclerosis: A qualitative study using interpretative phenomenological analysis. BMJ Open 2021, 11, e049041. [Google Scholar] [CrossRef]
- Tedeschi, R.G.; Calhoun, L.G. The posttraumatic growth inventory: Measuring the positive legacy of trauma. J. Trauma Stress 1996, 9, 455–471. [Google Scholar] [CrossRef]
- Weiss, T.; Berger, R. Reliability and validity of a Spanish version of the posttraumatic growth inventory. Res. Soc. Work Pract. 2006, 16, 191–199. [Google Scholar] [CrossRef]
- Carver, C.S. You want to measure coping but your protocol’s too long: Consider the brief COPE. Int. J. Behav. Med. 1997, 4, 92–100. [Google Scholar] [CrossRef] [PubMed]
- Morán, C.; Landero, R.; González, M.T. COPE-28: A psychometric analysis of the spanish version of the brief COPE. Univ. Psychol. 2010, 9, 543–552. [Google Scholar] [CrossRef]
- Haber, A.; LaRocca, N.G. Minimal Record of Disability for Multiple Sclerosis; National Multiple Sclerosis Society: New York, NY, USA, 1985. [Google Scholar]
- Kurtzke, J.F. Rating neurologic impairment in multiple sclerosis: An expanded disability status scale (EDSS). Neurology 1983, 33, 1444–1452. [Google Scholar] [CrossRef]
- Şen, S. Neurostatus and EDSS calculation with cases. Noro Psikiyatr Ars. 2018, 55 (Suppl. S1), 80–83. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Hillside, N.J., Ed.; Lawrence Erlbaum Associates: New York, NY, USA, 1988; ISBN 0-8058-0283-5. [Google Scholar]
- Neate, S.L.; Taylor, K.L.; Jelinek, G.A.; de Livera, A.M.; Simpson, S.; Bevens, W.; Weiland, T.J. On the path together: Experiences of partners of people with multiple sclerosis of the impact of lifestyle modification on their relationship. Health Soc. Care Community 2019, 27, 1515–1524. [Google Scholar] [CrossRef]
- Treder-Rochna, N. Adaptation to the disease—The psychological resources of families struggling with multiple sclerosis. Health Psychol. Rep. 2020, 8, 136–144. [Google Scholar] [CrossRef]
- Kunz, S.; Joseph, S.; Geyh, S.; Peter, C. Coping and posttraumatic growth: A longitudinal comparison of two alternative views. Rehab. Psychol. 2018, 63, 240–249. [Google Scholar] [CrossRef]
- Panichelli, C.; Albert, A.; Donneau, A.; D’Amore, S.; Triffaux, J.; Ansseau, M. Humor associated with positive outcomes in individual psychotherapy. Am. J. Psychother. 2018, 71, 95–103. [Google Scholar] [CrossRef]
- de Almeida, C.V.; Nunes, C. Humor Is Important in Healthcare Relationship? Open Access Libr. J. 2020, 7, e6372. [Google Scholar] [CrossRef]
- Malone, J.; Dadswell, A. The role of religion, spirituality and/or belief in positive ageing for older adults. Geriatrics 2018, 3, 28. [Google Scholar] [CrossRef] [PubMed]
- Santangelo, G.; Corte, M.D.; Sparaco, M.; Miele, G.; Garramone, F.; Cropano, M.; Esposito, S.; Lavorgna, L.; Gallo, A.; Tedeschi, G.; et al. Coping strategies in relapsing–remitting multiple sclerosis non-depressed patients and their associations with disease activity. Acta Neurol. Belg. 2021, 121, 465–471. [Google Scholar] [CrossRef] [PubMed]
- Kar, M.K.; Whitehead, L.; Smith, C.M. Characteristics and correlates of coping with multiple sclerosis: A systematic review. Disabil. Rehabil. 2019, 41, 250–264. [Google Scholar] [CrossRef]
- Gil-González, I.; Martín-Rodríguez, A.; Conrad, R.; Pérez-San-Gregorio, M.Á. Coping with multiple sclerosis: Reconciling significant aspects of health-related quality of life. Psychol. Health Med. 2022, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Furmańska, J.; Rzepa, T.N.; Koziarska, D.; Rutkowska, E.; Bulsa, M. Stereotypes vs. reality: Shame and coping strategies applied by healthy subjects and multiple sclerosis patients—Preliminary research. Postępy Psychiatr. I Neurol. 2020, 29, 11–24. [Google Scholar] [CrossRef]
- Calhoun, L.G.; Tedeschi, R.G. The foundations of posttraumatic growth: An expanded framework. In Handbook of Posttraumatic Growth: Research & Practice; Calhoun, L.G., Tedeschi, R.G., Eds.; Lawrence Erlbaum Associates Publishers: Mahwah, NJ, USA, 2006; pp. 3–23. [Google Scholar]
- Wawrziczny, E.; Corrairie, A.; Antoine, P. Relapsing-remitting multiple sclerosis: An interpretative phenomenological analysis of dyadic dynamics. Disabil. Rehabil. 2021, 43, 76–84. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Post-Traumatic Growth Level | Intergroup Comparisons | Effect Size | ||||
|---|---|---|---|---|---|---|
| Low (n = 85) | Medium (n = 84) | High (n = 91) | χ2 | p | Cohen´s w | |
| Gender n (%) | 0.222 | 0.895 | 0.029 (N) | |||
| Male | 28 (32.9) | 26 (31) | 27 (29.7) | |||
| Female | 57 (67.1) | 58 (69) | 64 (70.3) | |||
| Partnership n (%) | 1.871 | 0.392 | 0.084 (N) | |||
| No partner | 59 (69.4) | 66 (78.6) | 68 (74.7) | |||
| Partner | 26 (30.6) | 18 (21.4) | 23 (25.3) | |||
| Occupation n (%) | 1.247 | 0.536 | 0.068 (N) | |||
| Employed/In education | 34 (40) | 27 (32.1) | 31 (34.1) | |||
| Unemployed | 51 (60) | 57 (67.9) | 60 (65.9) | |||
| Educational level n (%) | 8.039 | 0.090 | 0.175 (S) | |||
| Primary education | 8 (9.4) | 10 (11.9) | 17 (18.7) | |||
| Secondary education | 26 (30.6) | 34 (40.5) | 22 (24.2) | |||
| University or higher | 51 (60) | 40 (47.6) | 52 (57.1) | |||
| MS subtype n (%) | 0.541 | 0.763 | 0.046 (N) | |||
| Remittent | 76 (89.4) | 72 (85.7) | 80 (87.9) | |||
| Progressive | 9 (10.6) | 12 (14.3) | 11 (12.1) | |||
| F (2,257) | p | Cohen´s d | ||||
| Age (M ± SD) | 45.7 ± 11.1 | 45.4 ± 10.9 | 44.1 ± 9.9 | 0.581 | 0.560 | 0.015 (N) |
| EDSS (M ± SD) | 3.1 ± 1.8 | 3.1 ± 1.9 | 3.4 ± 2.1 | 0.704 | 0.495 | 0.040 (N) |
| Months since diagnosis (M ± SD) | 140.3 ± 98.4 | 147.6 ± 92.3 | 146.2 ± 77.8 | 0.159 | 0.853 | 0.021 (N) |
| Months since outbreak (M ± SD) | 181.4 ± 112.9 | 190.8 ± 112.4 | 184.4 ± 108.4 | 0.084 | 0.919 | 0.020 (N) |
| Main Effects (Cohen´s f) | |||
|---|---|---|---|
| Phase | Post-Traumatic Growth | Interaction Effects (Cohen´s f) | |
| F (2,514) | F (2,257) | F (4,514) | |
| Acceptance | 26.463 ** 0.320 M | 2.869 0.149 S | 0.378 0.054 N |
| Emotional support | 82.898 ** 0.568 L | 7.050 ** 0.234 S | 4.252 ** 0.181 S |
| Humor | 82.970 ** 0.568 L | 4.623 0.190 S | 1.383 0.105 S |
| Positive reframing | 75.263 ** 0.541 L | 5381 ** 0.204 S | 4.395 ** 0.184 S |
| Religion | 9.566 ** 0.193 S | 1.019 0.089 N | 1.239 0.1 S |
| Active coping | 102.369 ** 0.631 L | 11.2 ** 0.29 M | 6.612 ** 0.226 S |
| Instrumental support | 15.780 ** 0.250 M |
5.107 ** 0.198 S |
0.923 0.083 N |
| Planning | 86.358 ** 0.580 L | 3.239 * 0.206 S | 5.107 ** 0.198 S |
| Behavioral disengagement | 0.015 0 N | 1.091 0.008 N | 1.393 0.011 N |
| Denial | 0.325 0.031 N | 1.298 0.100 S | 3.035 0.153 S |
| Self-distraction | 49.652 ** 0.439 L | 3.319 * 0.160 S | 0.780 0.077 N |
| Self-blaming | 109.678 ** 0.653 L | 0.767 0.077 N | 0.364 0.054 N |
| Substance use | 1.008 0.063 N | 0.792 0.044 N | 1.012 0.089 N |
| Venting | 24.560 ** 0.308 M | 0.736 0.077 N |
1.246 0.101 S |
| Post-Traumatic Growth Level M (SD) | Phases | Comparisons p (Cohen’s d) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Low (a) n = 85 | Medium (b) n = 84 | High (c) n = 91 | 1 | 2 | 3 | Group Levels | Phases | |||||
| a–b | a–c | b–c | 1–2 | 1–3 | 2–3 | |||||||
| Acceptance | 2.40 (0.81) | 2.44 (0.72) | 2.56 (0.57) | 2.28 (0.73) | 2.58 (0.56) | 2.56 (0.60) | 1 0.05 N | 0.072 0.23 S | 0.237 0.18 N | <0.001 0.58 M | <0.001 0.42 S | 1 0.03 N |
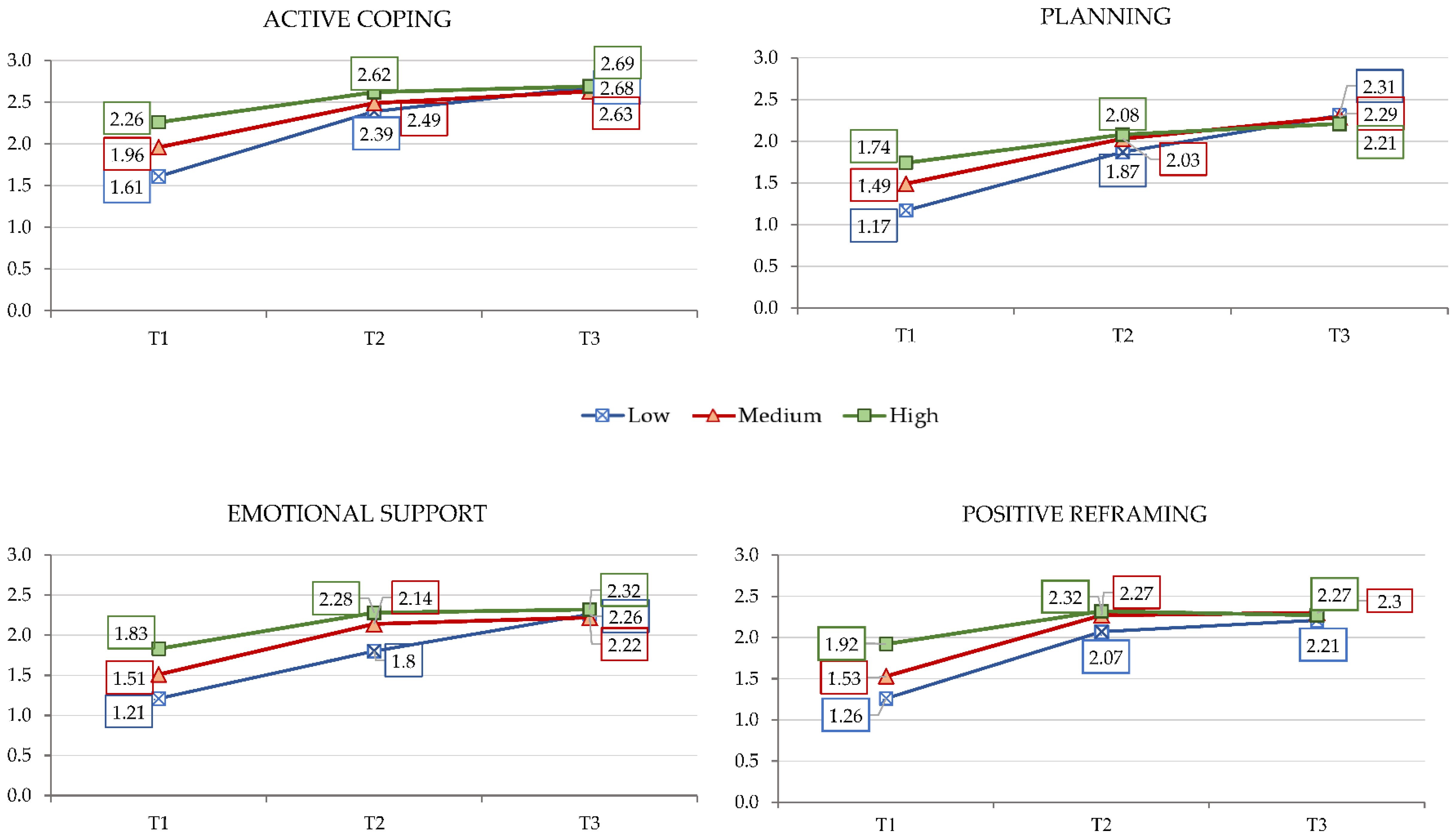
| Emotional support | 1.75 (0.95) | 1.96 (0.77) | 2.15 (0.91) | 1.52 (0.92) | 2.07 (0.96) | 2.26 (0.83) | 0.178 0.24 S | 0.001 0.43 S | 0.211 0.23 S | <0.0001 0.58 M | <0.0001 0.88 L | 0.005 0.21 S |
| Humor | 1.81 (1.05) | 1.83 (1.04) | 2.13 (1.10) | 1.42 (1.10) | 2.24 (0.98) | 2.11 (1.02) | 1 0.02 N | 0.023 0.30 S | 0.035 0.28 S | <0.0001 0.79 M | <0.0001 0.65 M | 0.103 0.13 N |
| Positive reframing | 1.84 (0.95) | 2.03 (0.81) | 2.17 (0.93) | 1.57 (0.94) | 2.21 (0.88) | 2.26 (0.87) | 0.196 0.22 S | 0.004 0.30 S | 0.504 0.16 N | <0.0001 0.70 M | <0.0001 0.76 M | 1 0.06 N |
| Religion means | 0.90 (0.88) | 1.06 (0.73) | 1.07 (0.94) | 0.86 (0.98) | 1.06 (1.07) | 1.09 (1.08) | 0.701 0.19 N | 0.605 0.19 N | 1 0.01 N | 0.001 0.20 S | <0.0001 0.22 S | 1 0.03 N |
| Active coping | 2.25 (0.85) | 2.36 (0.65) | 2.52 (0.67) | 1.94 (0.79) | 2.50 (0.62) | 2.67 (0.58) | 0.121 0.15 N | <0.0001 0.35 S | 0.029 0.24 S | <0.0001 0.78 M | <0.0001 1.03 L | 0.004 0.28 S |
| Instrumental support | 1.42 (0.78) | 1.55 (0.84) | 1.76 (0.90) | 1.38 (0.86) | 1.64 (0.98) | 1.73 (0.96) | 0.713 0.16 N | 0.005 0.40 S | 0.158 0.24 S | <0.0001 0.28 S | <0.0001 0.38 S | 0.555 0.09 N |
| Planning | 1.78 (0.78) | 1.94 (0.76) | 2.01 (0.82) | 1.47 (0.83) | 1.99 (0.90) | 2.27 (0.81) | 0.293 0.20 S | 0.039 0.29 S | 1 0.09 N | <0.0001 0.60 M | <0.0001 0.98 L | <0.001 0.33 S |
| Behavioral disengagement | 0.39 (0.57) | 0.37 (0.52) | 0.40 (0.66) | 0.39 (0.59) | 0.39 (0.61) | 0.38 (0.54) | 1 0.04 N | 1 0.02 N | 0.427 0.05 N | 1 0 N | 1 0.02 N | 1 0.02 N |
| Denial | 0.46 (0.62) | 0.45 (0.73) | 0.36 (0.57) | 0.41 (0.64) | 0.42 (0.61) | 0.45 (0.63) | 1 0.02 N | 0.469 0.17 N | 0.535 0.14 N | 1 0.02 N | 1 0.06 N | 1 0.05 N |
| Self-distraction | 1.40 (1.05) | 1.51 (0.92) | 1.77 (1.07) | 1.57 (1.02) | 2.05 (0.94) | 2.28 (0.78) | 0.552 0.11 N | 0.032 0.35 S | 0.678 0.26 S | <0.0001 0.50 M | <0.0001 0.78 M | 0.003 0.26 S |
| Self-blaming | 1.61 (0.99) | 1.74 (0.88) | 1.71 (1.02) | 1.15 (0.97) | 1.83 (0.90) | 2.07 (0.81) | 0.703 0.14 N | 1 0.09 N | 1 0.03 N | <0.0001 0.77 M | <0.0001 1.02 L | <0.0001 0.28 S |
| Substance use | 0.10 (0.35) | 0.113 (0.23) | 0.13 (0.47) | 0.11 (0.37) | 0.14 (0.51) | 0.10 (0.35) | 1 0.04 N | 0.742 0.07 N | 1 0.05 N | <0.0001 0.07 N | <0.0001 0.02 N | 0.705 0.09 N |
| Venting | 0.97 (0.83) | 0.89 (0.68) | 1.15 (0.81) | 1.01 (0.78) | 1.26 (0.80) | 1.37 (0.64) | 1 0.11 N | 1 0.12 N | 0.766 0.35 S | <0.0001 0.32 S | <0.0001 0.50 M | 0.138 0.15 N |
| Comparison between Phases, p (Cohen´s d) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Low CP | Medium CP | High CP | |||||||
| 1–2 | 1–3 | 2–3 | 1–2 | 1–3 | 2–3 | 1–2 | 1–3 | 2–3 | |
| Emotional support | <0.0001 0.61 M | <0.0001 1.06 L | <0.0001 0.50 M | <0.0001 0.72 M | <0.0001 0.86 L | 1 0.09 N | <0.0001 0.49 S | <0.0001 0.57 M | 1 0.05 N |
| Positive reframing | <0.0001 0.85 L | <0.0001 1.05 L | 0.529 0.15 N | <0.0001 0.87 L | <0.0001 0.90 L | 1 0.02 N | 0.002 0.46 S | 0.003 0.39 S | 1 0.05 N |
| Active coping | <0.0001 0.85 L | <0.0001 1.24 L | <0.0001 0.45 S | <0.0001 0.78 M | <0.0001 1.06 L | 0.318 0.23 S | <0.0001 0.60 M | <0.0001 0.65 M | 1 0.08 N |
| Planning | <0.0001 0.79 M | <0.0001 1.18 L | <0.0001 0.50 M | <0.0001 0.61 M | <0.0001 1.01 L | 0.048 0.29 S | 0.003 0.42 S | <0.0001 0.67 M | 0.642 0.22 S |
| F | R2 | B | SE.B | β | 1-β | f2 | |
|---|---|---|---|---|---|---|---|
| Model 1 | 54.523 (1.405) | 0.119 ** | 34.292 | 2.159 | 0.99 | 0.135 (S) | |
| Positive reframing | 8.798 | 1.192 | 0.344 ** | ||||
| Model 2 | 37.997 (2.404) | 0.158 ** | 28.824 | 2.456 | 0.99 | 0.187 (M) | |
| Positive reframing | 7.001 | 1.236 | 0.274 ** | ||||
| Emotional support | 5.402 | 1.238 | 0.211 ** | ||||
| Model 3 | 29.391 (3.403) | 0.180 ** | 25.331 | 2.659 | 0.99 | 0.222 (M) | |
| Positive reframing | 5.869 | 1.272 | 0.230 ** | ||||
| Emotional support | 4.604 | 1.248 | 0.180 ** | ||||
| Planning | 4.471 | 1.386 | 0.158 ** | ||||
| Model 4 | 24.082 (4.402) | 0.193 * | 24.812 | 2.647 | 0.99 | 0.239 (M) | |
| Positive reframing | 5.306 | 1.281 | 0.208 ** | ||||
| Emotional support | 3.791 | 1.277 | 0.148 ** | ||||
| Planning | 4.457 | 1.376 | 0.158 ** | ||||
| Religion means | 3.054 | 1.165 | 0.126 ** | ||||
| Model 5 | 20.227 (5.401) | 0.201 * | 22.896 | 2.802 | 0.99 | 0.251 (M) | |
| Positive reframing | 4.806 | 1.300 | 0.188 ** | ||||
| Emotional support | 3.883 | 1.273 | 0.152 ** | ||||
| Planning | 3.784 | 1.410 | 0.134 ** | ||||
| Religion means | 2.789 | 1.168 | 0.115 * | ||||
| Self-distraction | 2.361 | 1.170 | 0.098 * |
| F | R2 | B | SE.B | β | 1-β | f2 | |
|---|---|---|---|---|---|---|---|
| Model 1 | 43.189 (1.322) | 0.118 ** | 52.846 | 1.614 | 0.99 | 0.134 (S) | |
| Religion means | 7.356 | 1.119 | 0.344 ** | ||||
| Model 2 | 47.097 (2.323) | 0.227 ** | 36.552 | 2.860 | 1 | 0.294 (M) | |
| Religion means | 7.094 | 1.050 | 0.332 ** | ||||
| Emotional support | 7.876 | 1.173 | 0.330 ** | ||||
| Model 3 | 38.739 (3.321) | 0.266 ** | 21.330 | 4.606 | 1 | 0.362 (L) | |
| Religion means | 6.955 | 1.025 | 0.325 ** | ||||
| Emotional support | 6.985 | 1.164 | 0.292 ** | ||||
| Active coping | 6.927 | 1.668 | 0.202 ** | ||||
| Model 4 | 31.681 (4.320) | 0.284 ** | 18.040 | 4.703 | 1 | 0.396 (L) | |
| Religion means | 6.388 | 1.034 | 0.299 ** | ||||
| Emotional support | 6.414 | 1.169 | 0.269 ** | ||||
| Active coping | 5.793 | 1.698 | 0.169 ** | ||||
| Positive reframing | 3.586 | 1.270 | 0.144 ** | ||||
| Model 5 | 26.496 (5.319) | 0.294 * | 15.609 | 4.820 | 1 | 0.416 (L) | |
| Religion means | 6.011 | 1.044 | 0.281 ** | ||||
| Emotional support | 6.084 | 1.174 | 0.255 ** | ||||
| Active coping | 5.616 | 1.691 | 0.164 ** | ||||
| Positive reframing | 2.956 | 1.298 | 0.119 * | ||||
| Self-distraction | 2.608 | 1.242 | 0.107 * |
| F | R2 | B | SE.B | β | 1-β | f2 | |
|---|---|---|---|---|---|---|---|
| Model 1 | 104.556 (1.312) | 0.093 ** | 60.810 | 3.252 | 0.98 | 0.103 (S) | |
| Positive reframing | 7.037 | 1.344 | 0.306 | ||||
| Model 2 | 56.012 (2.311) | 0.148 ** | 53.024 | 3.679 | 0.99 | 0.173 (M) | |
| Positive reframing | 6.801 | 1.306 | 0.295 | ||||
| Instrumental support | 4.831 | 1.172 | 0.234 | ||||
| Model 3 | 39.010 (3.310) | 0.172 ** | 51.892 | 3.657 | 1 | 0.207 (M) | |
| Positive reframing | 6.198 | 1.309 | 0.269 | ||||
| Instrumental support | 4.434 | 1.166 | 0.215 | ||||
| Religion | 2.866 | 1.038 | 0.158 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gil-González, I.; Martín-Rodríguez, A.; Conrad, R.; Pérez-San-Gregorio, M.Á. Coping Strategies Furthering Post-Traumatic Growth in Multiple Sclerosis: A Longitudinal Study. Int. J. Environ. Res. Public Health 2022, 19, 12679. https://doi.org/10.3390/ijerph191912679
Gil-González I, Martín-Rodríguez A, Conrad R, Pérez-San-Gregorio MÁ. Coping Strategies Furthering Post-Traumatic Growth in Multiple Sclerosis: A Longitudinal Study. International Journal of Environmental Research and Public Health. 2022; 19(19):12679. https://doi.org/10.3390/ijerph191912679
Chicago/Turabian StyleGil-González, Irene, Agustín Martín-Rodríguez, Rupert Conrad, and María Ángeles Pérez-San-Gregorio. 2022. "Coping Strategies Furthering Post-Traumatic Growth in Multiple Sclerosis: A Longitudinal Study" International Journal of Environmental Research and Public Health 19, no. 19: 12679. https://doi.org/10.3390/ijerph191912679
APA StyleGil-González, I., Martín-Rodríguez, A., Conrad, R., & Pérez-San-Gregorio, M. Á. (2022). Coping Strategies Furthering Post-Traumatic Growth in Multiple Sclerosis: A Longitudinal Study. International Journal of Environmental Research and Public Health, 19(19), 12679. https://doi.org/10.3390/ijerph191912679