
Characteristics and Treatment Outcomes among Migrants with Pulmonary Tuberculosis: A Retrospective Cohort Study in Japan, 2009–2018

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source—Japan TB Surveillance System
2.2. Study Design and Populations
2.3. Definitions and Data Management
2.3.1. Treatment Outcomes
2.3.2. Other Socio-Economic Variables
2.4. Statistical Analysis
3. Results
3.1. Characteristics of Overseas-Born Patients with PTB
3.2. Treatment Outcomes
3.3. Factors of Treatment Non-Success
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Tuberculosis Report 2021; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- World Health Organization. The END TB Strategy; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Karo, B.; Hauer, B.; Hollo, V.; van der Werf, M.J.; Fiebig, L.; Haas, W. Tuberculosis treatment outcome in the European Union and European Economic Area: An analysis of surveillance data from 2002–2011. Eurosurveillance 2015, 20, 30087. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ejeta, E.; Beyene, G.; Balay, G.; Bonsa, Z.; Abebe, G. Factors associated with unsuccessful treatment outcome in tuberculosis patients among refugees and their surrounding communities in Gambella Regional State, Ethiopia. PLoS ONE 2018, 13, e0205468. [Google Scholar] [CrossRef] [PubMed]
- Mor, Z.; Kolb, H.; Lidji, M.; Migliori, G.; Leventhal, A. Tuberculosis diagnostic delay and therapy outcomes of non-national migrants in Tel Aviv, 1998–2008. Eurosurveillance 2013, 18, 20433. [Google Scholar] [CrossRef]
- Tuberculosis Surveillance Center; The Research Institute of Tuberculosis, Japan. Annual Report of Tuberculosis-Preliminary Report, 2021; The Research Institute of Tuberculosis: Tokyo, Japan, 2022. [Google Scholar]
- Kawatsu, L. The first step in Japan in bridging care and support for foreign-born persons with TB who are returning to countries of origin. In Proceedings of the 51st Union World Conference on Lung Health, Virtual Event, 20–24 October 2020. [Google Scholar]
- Masuyama, H.; Shimada, H.; Kinoshita, T.; Tajiri, S.; Imamura, M.; Takase, A.; Ehara, N.; Sekura, T.; Miyashita, O.; Huh, H.; et al. A study of ambulatory treatment for pulmonary tuberculosis in foreigners residing in Japan. Kekkaku 1993, 68, 301–312. [Google Scholar] [PubMed]
- Yamagishi, F.; Suzuki, K.; Sasaki, Y.; Yagi, T.; Miyazawa, Y.; Sato, N.; Togo, N.; Shirai, M.; Iohara, S.; Hayashi, A.; et al. The background of foreign patients with pulmonary tuberculosis and investigation of treatment results. Kekkaku 1993, 68, 545–550. [Google Scholar] [PubMed]
- Uchimura, K.; Ngamvithayapong-Yanai, J.; Kawatsu, L.; Ohkado, A.; Yoshiyama, T.; Shimouchi, A.; Ito, K.; Ishikawaa, N. Characteristics and treatment outcomes of tuberculosis cases by risk groups, Japan, 2007–2010. West. Pac. Surveill. Response J. WPSAR 2013, 4, 11–18. [Google Scholar] [CrossRef]
- Tsuda, Y.; Matsumoto, K.; Komukai, J.; Kasai, S.; Warabino, Y.; Hirota, S.; Koda, S.; Shimouchi, A. Pulmonary tuberculosis treatment outcome among foreign nationals residing in Osaka city. Kekkaku 2015, 90, 387–393. [Google Scholar]
- Kawatsu, L.; Uchimura, K.; Izumi, K.; Ohkado, A.; Ishikawa, N. Profile of tuberculosis among the foreign-born population in Japan, 2007–2014. West. Pac. Surveill Response J. 2016, 7, 7–16. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Definitions and Reporting Framework for Tuberculosis—2013 Revision (Updated December 2014 and January 2020); World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Tuberculosis Surveillance Center. Tuberculosis in Japan—Annual Report 2021; Department of Epidemiology and Clinical Research, The Research Institute of Tuberculosis: Tokyo, Japan, 2021. [Google Scholar]
- Tuberculosis Surveillance Center. Explanation of Data Input Items; Department of Epidemiology and Clinical Research, The Research Institute of Tuberculosis: Tokyo, Japan, 2021. (In Japanese) [Google Scholar]
- The World Bank. World Bank Analytical Classifications. The World Bank. Available online: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519 (accessed on 22 January 2021).
- Organization for Technical Intern Training. Business Summary 2021; Organization for Technical Intern Training: Tokyo, Japan, 2021.
- Ministry of Education, Culture, Sports, Science and Technology, Japan. About the Formulation of the Outline of “300,000 International Students Plan”. Available online: https://www.mext.go.jp/a_menu/koutou/ryugaku/1420758.htm. (accessed on 1 March 2022). (In Japanese)
- Organization for Technical Intern Training. Heisei 29 nendo Heisei 30 nendo Gaikokujin Ginou Jissyukikou Gyoumu Toukei Gaiyou, “Business Statistics Summary, Organization for Technical Intern Training, FY2017-2018”; Organization for Technical Intern Training: Tokyo, Japan, 2019. (In Japanese)
- Organization for Technical Intern Training. Business Statistic 2018 (Heisei 30); Organization for Technical Intern Training: Tokyo, Japan, 2018. Available online: https://www.otit.go.jp/gyoumutoukei_2018/ (accessed on 14 June 2022). (In Japanese)
- Parikh, N.S. Migrant Health in Japan: Safety-Net Policies and Advocates’ Policy Solutions. Asia-Pac. J. 2010, 8, 3324. [Google Scholar]
- Maeda, K. Risk factors for mental health of technical intern trainees from the Philippines. J. Int. Health 2018, 33, 303–312. (In Japanese) [Google Scholar]
- Shinohara, A.; Kawasaki, R.; Kuwano, N.; Ohnishi, M. Interview survey of physical and mental changes and coping strategies among 13 Vietnamese female technical interns living in Japan. Health Care Women Int. 2021. [Google Scholar] [CrossRef] [PubMed]
- Takayanagi, K.; Nagata, Y.; Ota, M. Tuberculosis among foreign-born technical intern trainees in Japan: A questionnaire survey, 2018. Kekkaku 2022, 97, 155–161. [Google Scholar]
- Nagata, Y.; Takayanagi, K.; Yano, R.; Sawada, T.; Morita, N.; Murakami, K.; Takasaki, J. Utilization of medical interpreters for tuberculosis patients in Japan: A questionnaire survey, 2016. Kekkaku 2020, 95, 41–46. (In Japanese) [Google Scholar]
- Takayanagi, K. Current situation of foreign-born tuberculosis patients in Japan: How It Is and How It Should Be on Treating Especially Outpatients (in Japanese). Kekkaku 2019, 94, 541–546. [Google Scholar]
- Japan Student Services Organization. 2019 (Reiwa Gan) nendo Gaikokujin Ryugakusei Zaiseki Jyoukyou Chousa Kekka, “Survey on Affiliation of Foreign-Born Students Studying in Japan, FY2019”; Japan Student Services Organization: Tokyo, Japan, 2020. (In Japanese)
- Japan Student Services Organization. Heisei 29 nendo Shihi Gaikokujin Ryugakusei Seikatu Jittai Chousa, “Survey on Livelihood of Self-Funded Foreign-Born Students Studying in Japan, FY2017”; Japan Student Services Organization: Tokyo, Japan, 2019.
- Itaki, M.; Endo, M.; Ikedo, K.; Kayebeta, A.; Takahashi, I.; Ota, M.; Hirao, S.; Nagata, Y. A multidrug-resistant tuberculosis outbreak in a language school: Tokyo, Japan, 2019–2020. Int. J. Mycobacteriol. 2021, 10, 37–42. (In Japanese) [Google Scholar] [PubMed]
- Morita, M.; Kaguraoka, S. Responses for foreign-born tuberculosis patients: Response and lesson learnt for an outbreak in a Japanese language school. Hokenshi Kangoshi Kekkaku Tenbou 2016, 53, 7–15. (In Japanese) [Google Scholar]
- Morino, E.; Takasaki, J.; Sugiyama, H. Controlling tuberculosis in foreign-born persons in Japan. Kekkaku 2016, 91, 703–708. (In Japanese) [Google Scholar]
- Ohkado, A.; Querri, A.; Shimamura, T.; Ota, M.; Celina Garfin, A.M. Referral and treatment outcomes of tuberculosis patients who crossed the border from Japan to the philippines. Int. J. Mycobacteriol. 2019, 8, 180–184. [Google Scholar]
- Ohkado, A.; Kawatsu, L.; Lee, S.; Hamaguchi, Y.; Mitsuhashi, K.; Miyamoto, K.; Yamaguchi, A. Developing a cross-border referral program for tuberculosis patients: First report. In Proceedings of the 96th Annual Meeting of the Japanese Society for Tuberculosis and Nontuberculosis Mycobacteriosis. Kekkaku 2021, 96, 100. (In Japanese) [Google Scholar]
- Dara, M.; de Colombani, P.; Petrova-Benedict, R.; Centis, R.; Zellweger, J.-P.; Sandgren, A.; Heldal, E.; Sotgiu, G.; Jansen, N.; Bahtijarevic, R.; et al. Minimum package for cross-border TB control and care in the WHO European region: A Wolfheze consensus statement. Eur. Respir. J. 2012, 40, 1081–1090. [Google Scholar] [CrossRef]
- Dara, M.; Sulis, G.; Centis, R.; D’Ambrosio, L.; de Vries, G.; Douglas, P.; Garcia, D.; Jansen, N.; Zuroweste, E.; Migliori, G.B. Cross-border collaboration for improved tuberculosis prevention and care: Policies, tools and experiences. Int. J. Tuberc. Lung Dis. 2017, 21, 727–736. [Google Scholar] [CrossRef] [PubMed]
- Kawatsu, L.; Ohkado, A.; Uchimura, K.; Izumi, K. Evaluation of “international transfer-out” among foreign-born pulmonary tuberculosis patients in Japan—What are the implications for a cross-border patient referral system? BMC Public Health 2018, 18, 1355. [Google Scholar] [CrossRef] [PubMed]
- The Research Institute of Tuberculosis, Japan. Bridge TB Care: A Cross-Border Referral Program for Tuberculosis Patients; The Research Institute of Tuberculosis: Tokyo, Japan, 2021. Available online: https://jata.or.jp/bridge.php (accessed on 1 October 2021). (In Japanese).
- World Health Organization. Regional Office for the Western Pacific. In Consultation on TB and Migration in the Western Pacific Region; Report; World Health Organization Regional Office for the Western Pacific: Manila, Philippines, 2013. [Google Scholar]
- Hayashi, H.; Matsukura, S.; Taguchi, M.; Yatagai, Y.; Funayama, Y. Clinical characteristics of tuberculosis patients among illegal overstayers. Kekkaku 2021, 96, 11–17. (In Japanese) [Google Scholar]
- Huffman, S.A.; Veen, J.; Hennink, M.M.; McFarland, D.A. Exploitation, vulnerability to tuberculosis and access to treatment among Uzbek labor migrants in Kazakhstan. Soc. Sci. Med. 2012, 74, 864–872. [Google Scholar] [CrossRef] [PubMed]
- Muñoz-Sellart, M.; Cuevas, L.E.; Tumato, M.; Merid, Y.; Yassin, M.A. Factors associated with poor tuberculosis treatment outcome in the Southern Region of Ethiopia. Int. J. Tuberc. Lung Dis. 2010, 14, 973–979. [Google Scholar]
- Kulkarni, P.; Akarte, S.; Mankeshwar, R.; Bhawalkar, J.; Banerjee, A.; Kulkarni, A. Non-adherence of new pulmonary tuberculosis patients to anti-tuberculosis treatment. Ann. Med. Health Sci. Res. 2013, 3, 67–74. [Google Scholar] [CrossRef] [Green Version]
- Hongguang, C.; Min, L.; Shiwen, J.; Fanghui, G.; Shaoping, H.; Tiejie, G.; Na, L.; Zhiguo, Z. Impact of diabetes on clinical presentation and treatment outcome of pulmonary tuberculosis in Beijing. Epidemiol. Infect. 2015, 143, 150–156. [Google Scholar] [CrossRef]
- Chenciner, L.; Annerstedt, K.S.; Pescarini, J.M.; Wingfield, T. Social and health factors associated with unfavourable treatment outcome in adolescents and young adults with tuberculosis in Brazil: A national retrospective cohort study. Lancet Glob. Health 2021, 9, e1380–e1390. [Google Scholar] [CrossRef]
- Tuberculosis Surveillance Center. Tuberculosis in Japan—Annual Report 2019; Department of Epidemiology and Clinical Research, The Research Institute of Tuberculosis: Tokyo, Japan, 2019. [Google Scholar]
- Liew, S.M.; Khoo, E.M.; Ho, B.K.; Lee, Y.K.; Mimi, O.; Fazlina, M.Y.; Asmah, R.; Lee, W.K.; Harmy, M.Y.; Chinna, K.; et al. Tuberculosis in Malaysia: Predictors of treatment outcomes in a national registry. Int. J. Tuberc. Lung Dis. 2015, 19, 764–771. [Google Scholar] [CrossRef]
- Przybylski, G.; Dąbrowska, A.; Trzcińska, H. Alcoholism and other socio-demographic risk factors for adverse TB-drug reactions and unsuccessful tuberculosis treatment-data from ten years’ observation at the Regional Centre of Pulmonology, Bydgoszcz, Poland. Med. Sci. Monit. 2014, 20, 444–453. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Category | Sub-Category | Treatment Success n = 6143 (67.1%) | Non-Success n = 3008 (32.9%) | Total n = 9151 | |||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Sex | Female | 3203 | 70.0 | 1371 | 30.0 | 4574 | 50.0 |
| Male | 2940 | 64.2 | 1637 | 35.8 | 4577 | 50.0 | |
| Age group | Under 24 | 2130 | 67.8 | 1011 | 32.2 | 3141 | 34.3 |
| 25–34 | 2281 | 69.2 | 1017 | 30.8 | 3298 | 36.0 | |
| 35–44 | 865 | 69.1 | 387 | 30.9 | 1252 | 13.7 | |
| 45–54 | 476 | 68.2 | 222 | 31.8 | 698 | 7.6 | |
| 55–64 | 196 | 59.2 | 135 | 40.8 | 331 | 3.6 | |
| 65+ | 195 | 45.2 | 236 | 54.8 | 431 | 4.7 | |
| Country of birth by income classification | Low income country | 531 | 74.3 | 184 | 25.7 | 715 | 7.8 |
| Lower-middle income country | 3024 | 68.7 | 1376 | 31.3 | 4400 | 48.1 | |
| Upper-middle income country | 1892 | 65.1 | 1014 | 34.9 | 2906 | 31.8 | |
| High-income country | 411 | 61.3 | 260 | 38.8 | 671 | 7.3 | |
| Unknown country of birth | 285 | 62.1 | 174 | 37.9 | 459 | 5.0 | |
| Time between entry to Japan and TB diagnosis | 10+ year | 536 | 74.8 | 181 | 25.2 | 717 | 16.0 |
| Less than 1 year | 751 | 66.5 | 378 | 33.5 | 1129 | 25.2 | |
| 1–5 year | 1523 | 70.4 | 641 | 29.6 | 2164 | 48.3 | |
| 5–10 year | 368 | 78.5 | 101 | 21.5 | 469 | 10.5 | |
| Occupation or social status | Students of high school and higher | 1852 | 70.7 | 768 | 29.3 | 2620 | 28.6 |
| Workers in service industries, and health and educational sectors * | 415 | 70.6 | 173 | 29.4 | 588 | 6.4 | |
| Regular workers other than service industries, and health and educational sectors | 1825 | 70.0 | 782 | 30.0 | 2607 | 28.5 | |
| Temporary and day workers | 590 | 67.2 | 288 | 32.8 | 878 | 9.6 | |
| Others, including unknown ** | 784 | 62.4 | 473 | 37.6 | 1257 | 13.7 | |
| Unemployed | 677 | 56.4 | 524 | 43.6 | 1201 | 13.1 | |
| Health insurance type | Employees’ health insurance | 2293 | 72.0 | 890 | 28.0 | 3183 | 34.8 |
| National health insurance | 3271 | 70.3 | 1382 | 29.7 | 4653 | 50.8 | |
| Medical care system for the elderly aged 75 and over | 66 | 38.4 | 106 | 61.6 | 172 | 1.9 | |
| Social welfare assistance *** | 163 | 57.8 | 119 | 42.2 | 282 | 3.1 | |
| Others and unknown | 350 | 40.7 | 511 | 59.4 | 861 | 9.4 | |
| HIV comorbidity | Not-positive **** | 4749 | 69.0 | 2136 | 31.0 | 6885 | 99.3 |
| Positive | 21 | 42.9 | 28 | 57.1 | 49 | 0.7 | |
| Sputum smear | Negative, not tested, and unknown | 3910 | 68.6 | 1794 | 31.5 | 5704 | 62.3 |
| Positive | 2233 | 64.8 | 1214 | 35.2 | 3447 | 37.7 | |
| Culture | Negative | 2098 | 71.6 | 833 | 28.4 | 2931 | 32.0 |
| Positive | 3636 | 68.0 | 1715 | 32.1 | 5351 | 58.5 | |
| Others | 409 | 47.1 | 460 | 52.9 | 869 | 9.5 | |
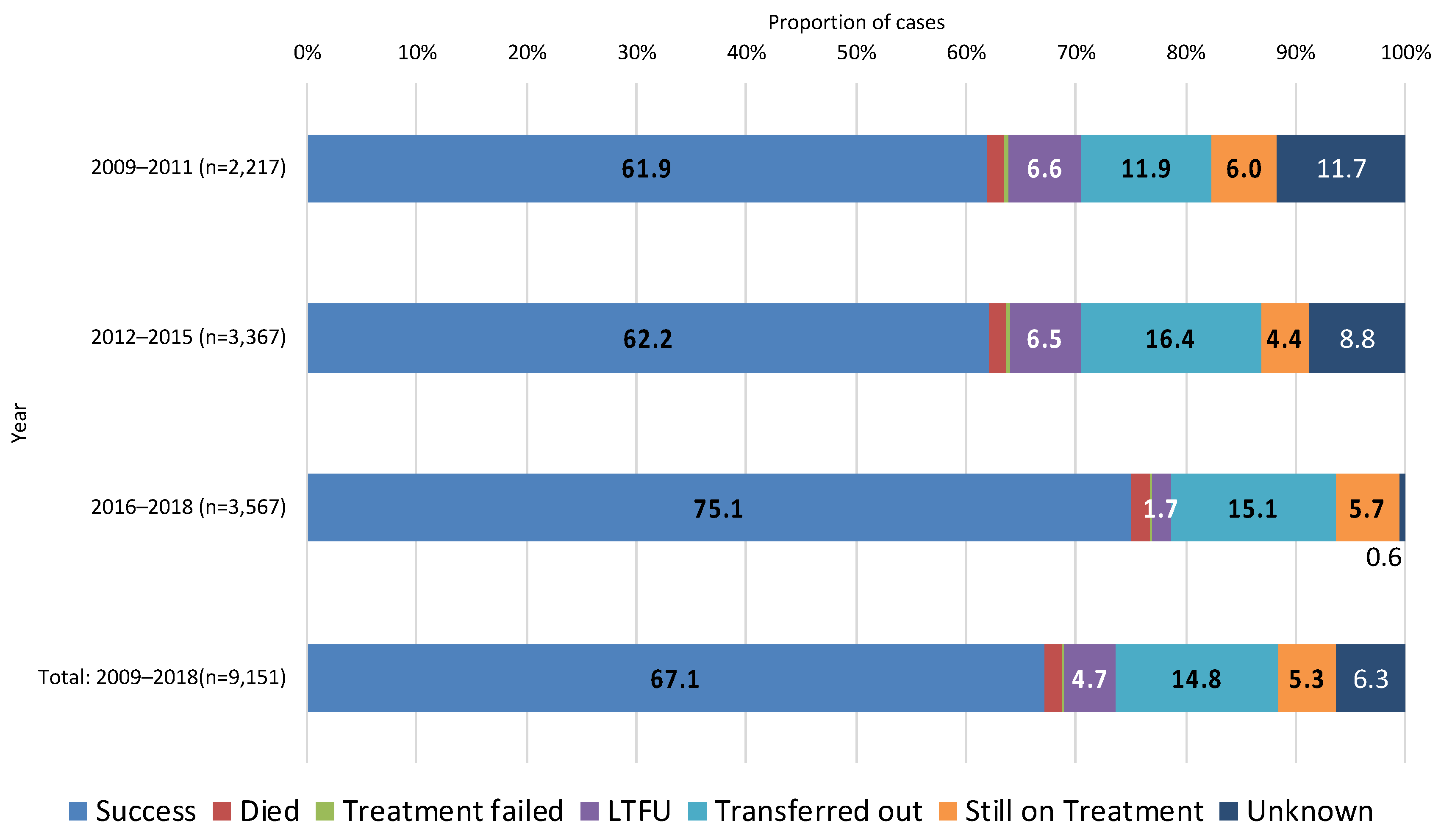
| 2009–2011 | 1373 | 61.9 | 844 | 38.1 | 2217 | 24.2 | |
| 2012–2015 | 2093 | 62.2 | 1274 | 37.8 | 3367 | 36.8 | |
| 2016–2018 | 2677 | 75.1 | 890 | 25.0 | 3567 | 39.0 | |
| Total (2009–2018) | 6143 | 67.1 | 3008 | 32.9 | 9151 | 100.0 | |
| Category | Sub-Category | 2009–2011 (n = 2217) | 2012–2015 (n = 3367) | 2016–2018 (n = 3567) | |||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Sex | Female | 1202 | 54.2 | 1701 | 50.5 | 1671 | 46.9 |
| Male | 1015 | 45.8 | 1666 | 49.5 | 1896 | 53.2 | |
| Age group | Under 24 | 681 | 30.7 | 1102 | 32.7 | 1358 | 38.1 |
| 25–34 | 833 | 37.6 | 1171 | 34.8 | 1294 | 36.3 | |
| 35–44 | 334 | 15.1 | 502 | 14.9 | 416 | 11.7 | |
| 45–54 | 168 | 7.6 | 289 | 8.6 | 241 | 6.8 | |
| 55–64 | 75 | 3.4 | 127 | 3.8 | 129 | 3.6 | |
| 65+ | 126 | 5.7 | 176 | 5.2 | 129 | 3.6 | |
| Country of birth by income classification | Low income country | 114 | 5.1 | 248 | 7.4 | 353 | 9.9 |
| Lower-middle income country | 828 | 37.4 | 1512 | 44.9 | 2060 | 57.8 | |
| Upper-middle income country | 902 | 40.7 | 1145 | 34.0 | 859 | 24.1 | |
| High-income country | 263 | 11.9 | 257 | 7.6 | 151 | 4.2 | |
| Unknown country of birth | 110 | 5.0 | 205 | 6.1 | 144 | 4.0 | |
| Time between entry to Japan and TB diagnosis | 10+ year | - | - | 393 | 18.7 | 324 | 13.6 |
| Less than 1 year | - | - | 497 | 23.7 | 632 | 26.6 | |
| 1–5 year | - | - | 949 | 45.2 | 1215 | 51.1 | |
| 5–10 year | - | - | 260 | 12.4 | 209 | 8.8 | |
| Occupation or social status | Students of high school and higher | 526 | 23.7 | 918 | 27.3 | 1176 | 33.0 |
| Workers in service industries, and health and educational sectors * | 174 | 7.9 | 209 | 6.2 | 205 | 5.8 | |
| Regular workers other than service industries, and health and educational sectors | 547 | 24.7 | 941 | 28.0 | 1119 | 31.4 | |
| Temporary and day workers | 261 | 11.8 | 349 | 10.4 | 268 | 7.5 | |
| Others, including unknown ** | 497 | 22.4 | 396 | 11.8 | 364 | 10.2 | |
| Unemployed | 212 | 9.6 | 554 | 16.5 | 435 | 12.2 | |
| Health insurance type | Employees’ health insurance | 680 | 30.7 | 1169 | 34.7 | 1334 | 37.4 |
| National health insurance | 1096 | 49.4 | 1703 | 50.6 | 1854 | 52.0 | |
| Medical care system for the elderly aged 75 and over | 56 | 2.5 | 72 | 2.1 | 44 | 1.2 | |
| Social welfare assistance *** | 93 | 4.2 | 116 | 3.5 | 73 | 2.1 | |
| Others and unknown | 292 | 13.2 | 307 | 9.1 | 262 | 7.4 | |
| HIV comorbidity | Not positive **** | - | - | 3340 | 99.2 | 3545 | 99.4 |
| Positive | - | - | 27 | 0.8 | 22 | 0.6 | |
| Sputum smear | Negative, not tested, and unknown | 1328 | 59.9 | 2066 | 61.4 | 2310 | 64.8 |
| Positive | 889 | 40.1 | 1301 | 38.6 | 1257 | 35.2 | |
| Culture | Negative | 670 | 30.2 | 1077 | 32.0 | 1184 | 33.2 |
| Positive | 1230 | 55.5 | 1945 | 57.8 | 2176 | 61.0 | |
| Others | 317 | 14.3 | 345 | 10.3 | 207 | 5.8 | |
| Category | Sub-Category | Univariate (Unadjusted) | Multivariable AOR | ||||||
|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | ||||
| Sex | Female | 1.0 | 1.0 | ||||||
| Male | 1.30 | 1.19 | 1.42 | <0.001 | 1.34 | 1.16 | 1.54 | <0.001 | |
| Age group | Under 24 | 1.0 | 1.0 | ||||||
| 25–34 | 0.94 | 0.85 | 1.04 | 0.24 | 0.98 | 0.83 | 1.16 | 0.82 | |
| 35–44 | 0.94 | 0.82 | 1.09 | 0.41 | 1.17 | 0.91 | 1.51 | 0.23 | |
| 45–54 | 0.98 | 0.82 | 1.17 | 0.85 | 1.35 | 0.96 | 1.90 | 0.09 | |
| 55–64 | 1.45 | 1.15 | 1.83 | 0.002 | 1.53 | 0.98 | 2.38 | 0.06 | |
| 65+ | 2.55 | 2.08 | 3.13 | <0.001 | 1.59 | 0.94 | 2.68 | 0.08 | |
| Country of birth by income classification | Low income country | 1.0 | 1.0 | ||||||
| Lower-middle income country | 1.31 | 1.10 | 1.57 | 0.003 | 1.50 | 1.16 | 1.95 | 0.002 | |
| Upper-middle income country | 1.55 | 1.29 | 1.86 | <0.001 | 1.63 | 1.25 | 2.14 | <0.001 | |
| High-income country | 1.83 | 1.45 | 2.29 | <0.001 | 1.53 | 1.01 | 2.32 | 0.04 | |
| Unknown country of birth | 1.76 | 1.37 | 2.27 | <0.001 | 1.47 | 0.87 | 2.49 | 0.15 | |
| Time between entry to Japan and TB diagnosis | 10+ year | 1.0 | 1.0 | ||||||
| Less than 1 year | 1.49 | 1.21 | 1.84 | <0.001 | 2.61 | 1.97 | 3.46 | <0.001 | |
| 1–5 year | 1.25 | 1.03 | 1.51 | 0.03 | 2.44 | 1.88 | 3.17 | <0.001 | |
| 5–10 year | 0.81 | 0.62 | 1.07 | 0.14 | 1.24 | 0.91 | 1.70 | 0.17 | |
| Occupation or social status | Students of high school and higher | 1.0 | 1.0 | ||||||
| Workers in service industries, and health and educational sectors * | 1.01 | 0.83 | 1.22 | 0.96 | 1.49 | 1.05 | 2.11 | 0.03 | |
| Regular workers other than service industries, and health and educational sectors | 1.03 | 0.92 | 1.16 | 0.59 | 1.37 | 1.09 | 1.74 | 0.01 | |
| Temporary and day workers | 1.18 | 1.00 | 1.39 | 0.051 | 1.53 | 1.15 | 2.04 | 0.003 | |
| Others, including unknown ** | 1.45 | 1.26 | 1.68 | <0.001 | 1.66 | 1.26 | 2.19 | <0.001 | |
| Unemployed | 1.87 | 1.62 | 2.15 | <0.001 | 2.06 | 1.55 | 2.74 | <0.001 | |
| Health insurance type | Employees’ health insurance | 1.0 | 1.0 | ||||||
| National health insurance | 1.09 | 0.99 | 1.20 | 0.10 | 1.32 | 1.09 | 1.60 | 0.004 | |
| Medical care system for the elderly aged 75 and over | 4.14 | 3.01 | 5.68 | <0.001 | 2.90 | 1.38 | 6.07 | 0.01 | |
| Social welfare assistance *** | 1.88 | 1.47 | 2.41 | <0.001 | 1.56 | 0.92 | 2.66 | 0.100 | |
| Others and unknown | 3.76 | 3.22 | 4.40 | <0.001 | 3.43 | 2.57 | 4.58 | <0.001 | |
| HIV comorbidity | Not positive **** | 1.0 | 1.0 | ||||||
| Positive | 2.96 | 1.68 | 5.23 | <0.001 | 2.21 | 1.00 | 4.87 | 0.05 | |
| Sputum smear | Negative, not tested, and unknown | 1.0 | 1.0 | ||||||
| Positive | 1.18 | 1.08 | 1.30 | <0.001 | 1.19 | 1.02 | 1.39 | 0.03 | |
| Culture | Negative | 1.0 | 1.0 | ||||||
| Positive | 1.19 | 1.08 | 1.31 | 0.001 | 1.14 | 0.97 | 1.36 | 0.12 | |
| Others | 2.83 | 2.42 | 3.31 | <0.001 | 2.38 | 1.83 | 3.10 | <0.001 | |
| Category | Sub-Category | Year 2009–2011 | Year 2012–2015 | Year 2016–2018 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| AOR | 95% CI | p-Value | AOR | 95% CI | p-Value | AOR | 95% CI | p-Value | |||||
| Sex | Female | 1.0 | 1.0 | 1.0 | |||||||||
| Male | 1.24 | 1.02 | 1.50 | 0.03 | 1.25 | 1.03 | 1.52 | 0.03 | 1.51 | 1.22 | 1.85 | <0.001 | |
| Age group | Under 24 | 1.0 | 1.0 | 1.0 | |||||||||
| 25–34 | 0.83 | 0.66 | 1.05 | 0.12 | 0.82 | 0.65 | 1.04 | 0.10 | 1.22 | 0.96 | 1.54 | 0.11 | |
| 35–44 | 0.87 | 0.64 | 1.20 | 0.40 | 1.04 | 0.73 | 1.47 | 0.83 | 1.34 | 0.91 | 1.99 | 0.14 | |
| 45–54 | 0.62 | 0.42 | 0.94 | 0.02 | 1.57 | 0.99 | 2.51 | 0.06 | 1.06 | 0.61 | 1.85 | 0.84 | |
| 55–64 | 1.32 | 0.77 | 2.25 | 0.31 | 1.76 | 0.95 | 3.25 | 0.07 | 1.67 | 0.84 | 3.32 | 0.15 | |
| 65+ | 1.18 | 0.66 | 2.12 | 0.58 | 2.55 | 1.23 | 5.30 | 0.01 | 1.04 | 0.46 | 2.34 | 0.93 | |
| Country of birth by income classification | Low income country | 1.0 | 1.0 | 1.0 | |||||||||
| Lower-middle income country | 0.96 | 0.63 | 1.47 | 0.85 | 1.17 | 0.80 | 1.70 | 0.41 | 2.00 | 1.37 | 2.93 | <0.001 | |
| Upper-middle income country | 0.93 | 0.61 | 1.41 | 0.72 | 1.30 | 0.89 | 1.89 | 0.17 | 1.73 | 1.14 | 2.61 | 0.01 | |
| High-income country | 0.88 | 0.55 | 1.43 | 0.61 | 1.08 | 0.62 | 1.88 | 0.80 | 2.01 | 1.05 | 3.82 | 0.03 | |
| Unknown country of birth | 1.32 | 0.76 | 2.31 | 0.33 | 1.45 | 0.75 | 2.80 | 0.27 | 1.01 | 0.38 | 2.69 | 0.99 | |
| Time between entry to Japan and TB diagnosis | 10+ year | — | — | — | — | 1.0 | 1.0 | ||||||
| Less than 1 year | — | — | — | — | 2.88 | 1.96 | 4.22 | <0.001 | 3.17 | 2.01 | 4.99 | <0.001 | |
| 1–5 year | — | — | — | — | 2.38 | 1.68 | 3.37 | <0.001 | 3.26 | 2.11 | 5.05 | <0.001 | |
| 5–10 year | — | — | — | — | 1.31 | 0.88 | 1.94 | 0.178 | 1.25 | 0.72 | 2.18 | 0.43 | |
| Occupation or social status | Students of high school and higher | 1.0 | 1.0 | 1.0 | |||||||||
| Workers in service industries, and health and educational sectors * | 0.84 | 0.55 | 1.28 | 0.41 | 1.91 | 1.18 | 3.09 | 0.01 | 1.19 | 0.69 | 2.05 | 0.53 | |
| Regular workers other than service industries, and health and educational sectors | 1.05 | 0.76 | 1.44 | 0.78 | 1.52 | 1.09 | 2.10 | 0.01 | 1.32 | 0.93 | 1.87 | 0.12 | |
| Temporary and day workers | 1.00 | 0.70 | 1.44 | 0.98 | 1.83 | 1.25 | 2.66 | 0.002 | 0.98 | 0.61 | 1.58 | 0.93 | |
| Others, including unknown ** | 1.09 | 0.79 | 1.53 | 0.59 | 1.94 | 1.32 | 2.86 | 0.001 | 1.48 | 0.98 | 2.25 | 0.07 | |
| Unemployed | 1.35 | 0.90 | 2.02 | 0.14 | 2.10 | 1.42 | 3.12 | <0.001 | 2.15 | 1.40 | 3.31 | <0.001 | |
| Health insurance type | Employees’ health insurance | 1.0 | 1.0 | 1.0 | |||||||||
| National health insurance | 1.0 | 0.75 | 1.22 | 0.73 | 1.1 | 0.84 | 1.39 | 0.55 | 1.7 | 1.3 | 2.3 | 0.001 | |
| Medical care system for the elderly aged 75 and over | 2.0 | 0.91 | 4.32 | 0.09 | 1.9 | 0.65 | 5.63 | 0.24 | 5.9 | 2.0 | 17.5 | 0.001 | |
| Social welfare assistance *** | 1.5 | 0.89 | 2.40 | 0.13 | 1.1 | 0.54 | 2.22 | 0.81 | 2.8 | 1.2 | 6.4 | 0.02 | |
| Others and unknown | 2.1 | 1.58 | 2.88 | <0.001 | 2.5 | 1.70 | 3.74 | <0.001 | 4.7 | 3.0 | 7.4 | <0.001 | |
| HIV comorbidity | Not-positive **** | — | — | — | — | 1.0 | 1.0 | ||||||
| Positive | — | — | — | — | 3.67 | 1.17 | 11.52 | 0.03 | 1.12 | 0.32 | 3.93 | 0.86 | |
| Sputum smear | Negative, not tested and unknown | 1.0 | 1.0 | 1.0 | |||||||||
| Positive | 0.91 | 0.74 | 1.12 | 0.37 | 1.08 | 0.87 | 1.34 | 0.51 | 1.26 | 1.00 | 1.60 | 0.054 | |
| Culture | Negative | 1.0 | 1.0 | 1.0 | |||||||||
| Positive | 1.11 | 0.88 | 1.39 | 0.40 | 1.18 | 0.94 | 1.50 | 0.16 | 1.18 | 0.92 | 1.52 | 0.20 | |
| Others | 2.61 | 1.96 | 3.48 | <0.001 | 2.32 | 1.65 | 3.25 | <0.001 | 2.15 | 1.39 | 3.33 | 0.001 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.; Aung, M.N.; Kawatsu, L.; Uchimura, K.; Miyahara, R.; Takasaki, J.; Ohkado, A.; Yuasa, M. Characteristics and Treatment Outcomes among Migrants with Pulmonary Tuberculosis: A Retrospective Cohort Study in Japan, 2009–2018. Int. J. Environ. Res. Public Health 2022, 19, 12598. https://doi.org/10.3390/ijerph191912598
Lee S, Aung MN, Kawatsu L, Uchimura K, Miyahara R, Takasaki J, Ohkado A, Yuasa M. Characteristics and Treatment Outcomes among Migrants with Pulmonary Tuberculosis: A Retrospective Cohort Study in Japan, 2009–2018. International Journal of Environmental Research and Public Health. 2022; 19(19):12598. https://doi.org/10.3390/ijerph191912598
Chicago/Turabian StyleLee, Sangnim, Myo Nyein Aung, Lisa Kawatsu, Kazuhiro Uchimura, Reiko Miyahara, Jin Takasaki, Akihiro Ohkado, and Motoyuki Yuasa. 2022. "Characteristics and Treatment Outcomes among Migrants with Pulmonary Tuberculosis: A Retrospective Cohort Study in Japan, 2009–2018" International Journal of Environmental Research and Public Health 19, no. 19: 12598. https://doi.org/10.3390/ijerph191912598
APA StyleLee, S., Aung, M. N., Kawatsu, L., Uchimura, K., Miyahara, R., Takasaki, J., Ohkado, A., & Yuasa, M. (2022). Characteristics and Treatment Outcomes among Migrants with Pulmonary Tuberculosis: A Retrospective Cohort Study in Japan, 2009–2018. International Journal of Environmental Research and Public Health, 19(19), 12598. https://doi.org/10.3390/ijerph191912598