
South Korean Early Cancer Patients’ Perceptions of Difficulties in Fighting Their Disease: A Q Methodological Approach


Abstract
:1. Introduction
2. Study Method
2.1. Study Procedure
2.2. Selection of the Q Population and Q Samples
2.3. P Sample Selection
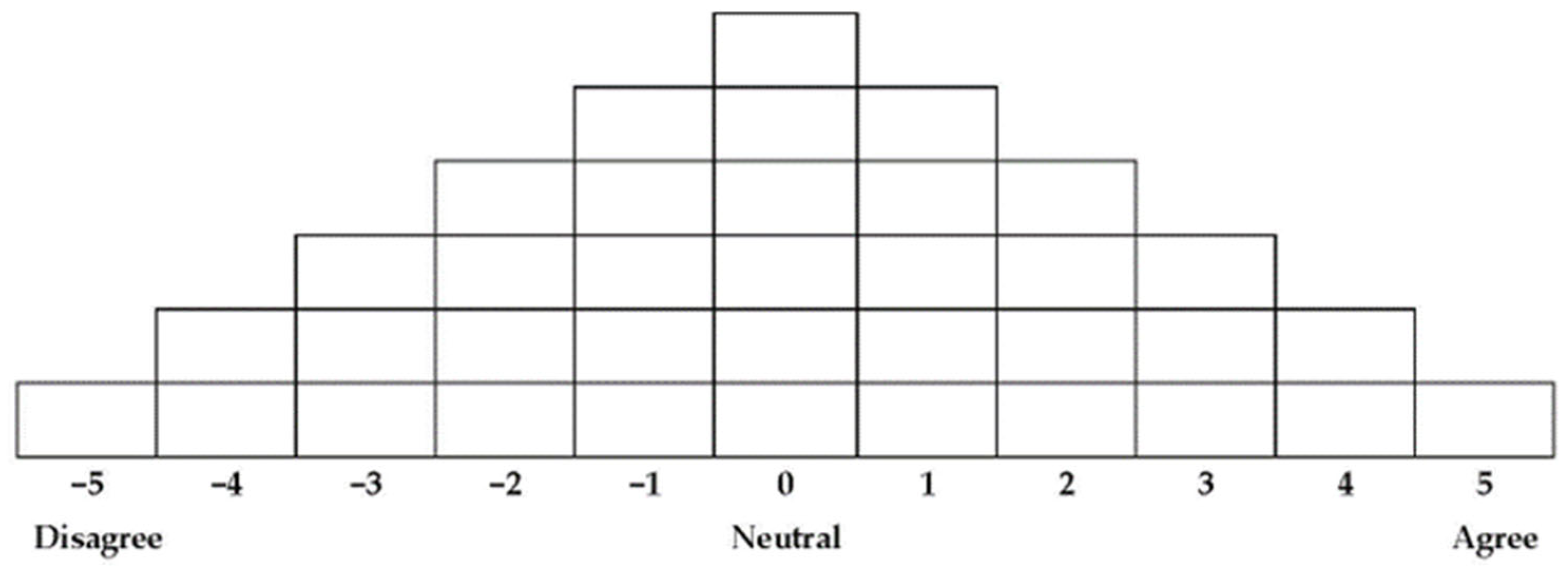
2.4. Q Sorting
2.5. Q Sorted Data Processing and Analysis
3. Study Results
3.1. Analysis of Results
3.2. Characteristics by Type
3.2.1. Type 1: Fear of the Future
3.2.2. Type 2: Helplessness against What Cannot Be Controlled
3.2.3. Type 3: Frustration Due to Difficulties in Role Performance
4. Discussion
5. Conclusions
6. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Madhan, E.S.; Neelakandan, S.; Annamalai, R. A novel approach for vehicle type classification and speed prediction using deep learning. J. Comput. Theor. Nanosci. 2020, 17, 2237–2242. [Google Scholar] [CrossRef]
- Korean Statisical Information Service. Available online: http://www.kosis.kr (accessed on 13 August 2022).
- National Breast Cancer Foundation, INC. Available online: https://www.nationalbreastcancer.org/breast-cancer-facts (accessed on 13 August 2022).
- Traboulssi, M.; Pidgeon, M.; Weathers, E. My wife has breast cancer: The lived experience of Arab men. Semin. Oncol. Nurs. 2022, 38, 151307. [Google Scholar] [CrossRef] [PubMed]
- Dafni Rose, J.; VijayaKumar, K.; Singh, L.; Sharma, S.K. Computer-aided diagnosis for breast cancer detection and classification using optimal region growing segmentation with MobileNet model. Concurr. Eng. 2022, 30, 1063293X221080518. [Google Scholar] [CrossRef]
- Golden-Kreutz, D.M.; Andersen, B.L. Depressive symptoms after breast cancer surgery: Relationships with global, cancer-related, and life event stress. Psycho-Oncology 2004, 13, 211–220. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.R. Endometrial Adverse Events in Breast Cancer Patients Treated with Anti-Hormonal Therapy: A National Health Insurance Claim Database Analysis. Ph.D. Thesis, University of Ulsan, Ulsan, Korea, 2017. [Google Scholar]
- Iddrisu, M.; Aziato, L.; Dedey, F. Psychological and physical effects of breast cancer diagnosis and treatment on young Ghanaian women: A qualitative study. BMC Psychiatry 2020, 20, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Runowicz, C.D.; Leach, C.R.; Henry, N.L.; Henry, K.S.; Mackey, H.T.; Cowens-Alvarado, R.L.; Ganz, P.A. American cancer society/American society of clinical oncology breast cancer survivorship care guideline. CA A Cancer J. Clin. 2016, 66, 43–73. [Google Scholar] [CrossRef]
- Oberst, M.T.; Hughes, S.H.; Chang, A.S.; McCubbin, M.A. Self-care burden, stress appraisal, and mood among persons receiving radiotherapy. Cancer Nurs. 1991, 14, 71–78. [Google Scholar] [CrossRef]
- Maglia, M.; Tortorici, J.; Lenzo, V.; Aiello, D.; Alì, M.; Aiello, R.; Caponnetto, P. The network that unites a qualitative study on clinical psychological intervention for women with a history of breast cancer and chronic pain. Eur. J. Investig. Health Psychol. Educ. 2022, 12, 619–630. [Google Scholar] [CrossRef]
- Cappiello, M.; Cunningham, R.S.; Tish Knobf, M.; Erdos, D. Breast cancer survivors: Information and support after treatment. Clin. Nurs. Res. 2007, 16, 278–293. [Google Scholar] [CrossRef]
- Kim, K.H.; Kwon, H.J.; Choi, M.H.; Kim, J.; Kim, K.S. The relationship of sexual satisfaction and daily stress in the breast cancer patients. Korean J. Adult Nurs. 2009, 21, 529–537. [Google Scholar]
- Martino, M.L.; Lemmo, D.; Testoni, I.; Iacona, E.; Pizzolato, L.; Freda, M.F.; Neimeyer, R.A. Anticipatory mourning and narrative meaning-making in the younger breast cancer experience: An application of the meaning of loss codebook. Behav. Sci. 2022, 12, 93. [Google Scholar] [CrossRef] [PubMed]
- Dewji, S. The Impact of Emotional Support on Identity in Breast Cancer Survivors. Bachelor’s Thesis, The University of Central Florida, Orlando, FL, USA, 2022. [Google Scholar]
- Smedsland, S.K.; Vandraas, K.F.; Bøhn, S.K.; Dahl, A.A.; Kiserud, C.E.; Brekke, M.; Reinertsen, K.V. Sexual activity and functioning in long-term breast cancer survivors; exploring associated factors in a nationwide survey. Breast Cancer Res. Treat. 2022, 193, 139–149. [Google Scholar] [CrossRef] [PubMed]
- Pereira, M.; Ribeiro, C.; Ferreira, G.; Machado, J.C.; Leite, Â. The indirect effect of body image on distress in women with breast cancer undergoing chemotherapy. Health Psychol. Rep. 2022, 10, 47–57. [Google Scholar] [CrossRef]
- Rajagopal, S. Kerala needs a women’s movement for breast cancer: An exploratory study on breast cancer awareness in Kerala. J. Int. Women’s Stud. 2022, 24, 6. [Google Scholar]
- Lee, J.W.; Kum, H.S. Working women’s life satisfaction, couples’ gender role attitude and the division of housework. Fam. Cult. 2020, 32, 34–69. [Google Scholar]
- Schenker, R.A.; Ciurea, M.E.; Stovicek, P.O.; Ciubara, A.; Schenker, M.; Marinescu, I. Depression and anxiety-risk factors in the evolution of breast cancer in women. Broad Res. Artif. Intell. Neurosci. 2022, 13 (Supp. S1), 135–158. [Google Scholar] [CrossRef] [PubMed]
- McKeown, B.; Thomas, D. Q Methodology; Sage: Beverly Hills, CA, USA, 2013. [Google Scholar]
- Dennis, K.A. Goldberg. Weight control self-efficiency types and transitions affect weight loss outcomes in obese women. Addict. Behav. 1996, 21, 103–116. [Google Scholar] [CrossRef]
- Kerlinger, F.N. Chapter 32: Q methodology. In Foundations of Behavioral Research; Wadsworth Publishing: Belmont, CA, USA, 1986; Volume 3. [Google Scholar]
- Kil, B.O.; Lee, S.H.; Lee, S.Y.; Jeong, H.J. Understanding and Application of Q Methodology; Chungnam National University Publishing & Cultural Center: Daejeon, Korea, 2020. [Google Scholar]
- Kim, B.J. Understanding the Q methodology and its application to consumer research. Asia Mark. J. 1999, 1, 120–140. [Google Scholar]
- Lee, J.Y. A Study on the Teacher’s Perception of Child Play Leadership in Free Play-Focusing on the Q-Methodology Approach. Ph.D. Thesis, Namseoul University, Cheonan, Korea, 2020. [Google Scholar]
- Seo, S.J.; Nho, J.H.; Lee, M.H.; Park, Y.S. Influence of lifestyle, depression, and marital intimacy on quality of life in breast cancer survivors. Korean J. Women Health Nurs. 2020, 26, 28–36. [Google Scholar] [CrossRef]
- Park, S.Y.; Noh, E.J.; Koo, H.N.; Baek, J.Y.; Park, H.K. Living after diagnosis of middle-aged and elderly breast cancer survivors at early stages. Health Soc. Welf. Rev. 2020, 40, 90–123. [Google Scholar]
- Kim, H.K. Q Methodology: Philosophy, Theories, Analysis, and Application; Communication Books: Seoul, Korea, 2008. [Google Scholar]
- Brown, S.R. Political Subjectivity: Applications of Q Methodology in Political Science; Yale University Press: New Haven, CT, USA, 1980. [Google Scholar]
- Paik, Y.D.; Kim, S.S. An observation on Q-methodology studies. J. Educ. Cult. Soc. 1998, 4, 47–71. [Google Scholar]
- Schapira, L.; Zheng, Y.; Gelber, S.I.; Poorvu, P.; Ruddy, K.J.; Tamimi, R.M.; Peppercorn, J.; Come, S.E.; Borges, V.F.; Partridge, A.H.; et al. Trajectories of fear of cancer recurrence in young breast cancer survivors. Cancer 2022, 128, 335–343. [Google Scholar] [CrossRef] [PubMed]
- Thewes, B.; Bell, M.L.; Butow, P.; Beith, J.; Boyle, F.; Friedlander, M.; McLachlan, S.A.; the Members of the FCR Study Advisory Committee. Psychological morbidity and stress but not social factors influence level of fear of cancer recurrence in young women with early breast cancer: Results of a cross-sectional study. Psycho-Oncology 2013, 22, 2797–2806. [Google Scholar] [CrossRef] [PubMed]
- Waroquier, P.; Delevallez, F.; Razavi, D.; Merckaert, I. Psychological factors associated with clinical fear of cancer recurrence in breast cancer patients in the early survivorship period. Psycho-Oncology, 2022; Early View. [Google Scholar]
- Gutiérrez-Leal, G.; Mendoza-Madero, D.L.; Gómez-Zarco, A.; Lima-Quezada, A.; Escudero-Castelán, A.Y. Positive psychology interventions in patients with breast cancer. J. Basic Appl. Psych. Res. 2022, 3, 22–28. [Google Scholar] [CrossRef]
- Arnedo, C.O.; Balado, C.P.; Travier, N.; Feixa, L.M.; Valle, A.F.; de Frutos, M.L.; Blasco, M.S. Stressful life events and distress in breast cancer: A 5-years follow-up. Int. J. Clin. Health Psychol. 2022, 22, 51–60. [Google Scholar]
- Hernandez, A.; Reyes, C.L.; Garcia, I.; Palacios, R.L. “I felt defeated. I felt helpless”: Social determinants of health influencing the cancer survivorship of a young Latina mother. J. Cancer Ther. 2022, 13, 440–449. [Google Scholar] [CrossRef]
- Rottmann, N.; Dalton, S.O.; Christensen, J.; Frederiksen, K.; Johansen, C. Self-efficacy, adjustment style and well-being in breast cancer patients: A longitudinal study. Qual. Life Res. 2010, 19, 827–836. [Google Scholar] [CrossRef]
- Owen, S.V.; Froman, R.D. Development of a college academic self-efficacy. In Proceedings of the Annual Meeting of the National Council on Measurement in Education, New Orleans, LA, USA, 6–8 April 1988; pp. 143–150. [Google Scholar]
- Khalid, M.; Majeed, S. Optimism, spousal support and quality of life in women with breast cancer. Pak. J. Med. Health Sci. 2022, 16, 769. [Google Scholar] [CrossRef]
- Fortin, J.; Rivest-Beauregard, M.; Defer, C.; Leblanc, M.; Thamar Louis, L.A.; Roy, C.A.; Lapierre, I.; Brunet, A.; Montreuil, M.; Marin, M.-F.; et al. The impact of Canadian medical delays and preventive measures on breast cancer experience: A silent battle masked by the COVID-19 pandemic. Can. J. Nurs. Res. 2022, 1–13. [Google Scholar] [CrossRef]
- Chin, J.-C.; Chen, Y.-Y. Mother–child dyad support needs to be expressed by mothers diagnosed with breast cancer. J. Clin. Nurs. 2022; Early View. [Google Scholar]
- Falk, R.S.; Bøhn, S.; Kiserud, C.; Lie, H.; Smedsland, S.; Ewertz, M.; Reinertsen, K. Work Ability Among Long-term Breast Cancer Survivors–Exploring the Role of Social Support in a Nation-wide Study. Res. Sq. 2022, 1–14. Available online: https://www.researchsquare.com/article/rs-1224688/v1 (accessed on 13 August 2022).
- Harianja, R.; Wahidi, K.R.; Mutiara, R. The effect of education on quality of life of breast cancer patients with family assistance and treatment compliance as a mediation variable. J. Health Sains 2022, 3, 748–756. [Google Scholar] [CrossRef]
- Zhang, X.; Gong, N.; Li, N.; Zhang, Y.; Du, Q.; Zou, W.; Zhang, M. Why breast cancer patients avoid communicating disease-related information to their dependent children: A qualitative study. J. Clin. Nurs. 2022; Early View. [Google Scholar] [CrossRef]
- Gotay, C. The experience of cancer during early and advanced stages: The views of patients and their mates. Soc. Sci. Med. 1984, 18, 605–613. [Google Scholar] [CrossRef]
- Kirsner, R.S.; Ma, F.; Fleming, L.E.; Federman, D.D.; Rapido, E.; Duncan, R.; Rouhani, P.; Wilkinson, J.D. Earlier stage at diagnosis and improved survival among Medicare HMO patients with breast cancer. J. Women’s Health 2010, 19, 1619–1624. [Google Scholar] [CrossRef] [PubMed]
- Vos, P.J.; Garssen, B.; Visser, A.P.; Duivenvoorden, H.J.; de Haes, H.C. Early stage breast cancer: Explaining level of psychosocial adjustment using structural equation modeling. J. Behav. Med. 2004, 27, 557–580. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| No. | Statement |
|---|---|
| 1 | I feel helpless because cancer is a disease that is beyond my control. |
| 2 | I feel flustered when I cannot control my emotions, leading me to have sudden feelings of depression and anxiety. |
| 3 | I always feel exhausted from lack of sleep due to continual worry about having breast cancer. |
| 4 | I feel lonely and isolated. |
| 5 | I am angry because I feel it is unfair that I got breast cancer. |
| 6 | Not knowing when I will die fills me with fear. |
| 7 | I feel pathetic when I see myself trying so hard not to feel anxious. |
| 8 | I feel helpless because I cannot plan for my future. |
| 9 | I feel like I am suffering from severe pain due to chemotherapy. |
| 10 | I feel doubtful about whether I will ever be cancer-free. |
| 11 | I feel a sense of loss about losing my breasts after undergoing mastectomy surgery. |
| 12 | I am afraid my partner will treat me differently regarding our sex life. |
| 13 | It is uncomfortable for me to go to public places like saunas. |
| 14 | I find it difficult to accept how I look due to hair loss. |
| 15 | I feel that I have lost my feminine identity. |
| 16 | I fear my nails falling off and my skin discolouring during treatment. |
| 17 | My family cannot understand my suffering. |
| 18 | I am worried that I will burden my family. |
| 19 | I am worried about not being able to fulfil my role and responsibilities at home during treatment. |
| 20 | I feel easily hurt when people around me try to console me with superficial greetings. |
| 21 | I am afraid that my breast cancer might be genetic. |
| 22 | I feel drained when people who had the same experience overwhelm me with excessive emotional expression and information. |
| 23 | I feel that my family and colleagues do not care when they still expect me to fulfil my roles and responsibilities. |
| 24 | I have resentment because I feel I got breast cancer due to continual stress from my family and work. |
| 25 | I do not want people to gossip about me being a breast cancer patient. |
| 26 | I am worried about chemotherapy treatment because of its possible side effects that can lead to other illnesses. |
| 27 | I feel that the immense amount of examinations I undergo at the hospital is burdensome and a hassle. |
| 28 | I am afraid that my breast cancer might spread or that I might have complications. |
| 29 | I am afraid that my breast cancer might return. |
| 30 | I feel that it is difficult to find a reliable surgeon. |
| 31 | It makes me sad when I think about the possibility of a day when I will have to accept that I will die because my breast cancer returned and I ran out of treatment options. |
| 32 | I feel degraded when medical professionals treat me without empathy, as if our relationship is strictly business. |
| 33 | I am frustrated because it is difficult to understand what the medical professionals say regarding my treatment process and the resultant symptoms. |
| 34 | It is difficult to accept that I no longer have a normal life. |
| 35 | I am worried that my coworkers will judge me and lower their expectations concerning my work ability because of my cancer. |
| 36 | I am worried that I might no longer be able to work. |
| 37 | I feel like everything I have built throughout my life has become meaningless. |
| 38 | I feel burdened about having to care more about my health. |
| 39 | I feel that treatment is too expensive. |
| 40 | I think that I will eventually have to end my career. |
| Raw Score | −5 | −4 | −3 | −2 | −1 | 0 | +1 | +2 | +3 | +4 | +5 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Converted score | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 |
| Content/Type | I | II | III |
|---|---|---|---|
| Chosen eigenvalue | 3.4018 | 1.3569 | 1.1593 |
| Total variance | 0.2617 | 0.1044 | 0.0892 |
| Cumulative variance | 0.2617 | 0.3661 | 0.4552 |
| Type 1 | Type 2 | Type 3 | |
|---|---|---|---|
| Type 1 | 1.0000 | ||
| Type 2 | 0.291 | 1.000 | |
| Type 3 | 0.249 | 0.128 | 1.000 |
| Type | P | Gender | Age | Treatment Period (Months) | Marital Status | Occupational Status | Factor Weight |
|---|---|---|---|---|---|---|---|
| Type 1 (n = 7) | 1 | Female | 50 | 7 | Married | Housewife | 0.4254 |
| 4 | Female | 51 | 1 | Married | Housewife | 0.7596 | |
| 5 | Female | 43 | 2 | Married | Housewife | 0.7764 | |
| 6 | Female | 39 | 3 | Married | Unemployed | 0.8815 | |
| 9 | Female | 45 | 7 | Married | Employed | 0.5381 | |
| 10 | Female | 53 | 7 | Married | Housewife | 0.6871 | |
| 12 | Female | 54 | 3 | Married | Employed | 1.3366 | |
| Type 2 (n = 3) | 3 | Female | 58 | 1 | Married | Employed | 1.0520 |
| 11 | Female | 65 | 8 | Married | Housewife | 0.7990 | |
| 13 | Female | 53 | 11 | Married | Housewife | 1.6403 | |
| Type 3 (n= 3) | 2 | Female | 41 | 8 | Married | Unemployed | 1.0198 |
| 7 | Female | 52 | 11 | Married | Housewife | 0.1803 | |
| 8 | Female | 43 | 4 | Divorced | Leave of absence | 0.8183 |
| No. | Statement | Standard Score |
|---|---|---|
| 28 | I am afraid that my breast cancer might spread or that I might experience complications. | 2.28 |
| 29 | I am afraid that my breast cancer might return. | 1.89 |
| 1 | I feel helpless because cancer is a disease that is beyond my control. | 1.84 |
| 36 | I am worried that I might not be able to work anymore. | 1.14 |
| 21 | I am afraid that my breast cancer might be genetic. | 1.10 |
| 37 | I feel like everything I have built throughout my life has become meaningless. | 1.02 |
| 11 | I feel a sense of loss about losing my breasts after going through mastectomy surgery. | −1.94 |
| 16 | I fear my nails falling off and my skin discolouring during treatment. | −1.58 |
| 3 | I always feel exhausted from lack of sleep due to continual worries about having breast cancer. | −1.39 |
| 2 | I feel flustered when I cannot control my emotions, leading me to have sudden feelings of depression and anxiety. | −1.26 |
| 14 | I find it difficult to accept how I look due to hair loss. | −1.22 |
| No. | Statement | Standard Score |
|---|---|---|
| 1 | I feel helpless because cancer is a disease that is beyond my control | 2.32 |
| 28 | I am afraid that my breast cancer might spread or that I might have complications. | 1.76 |
| 26 | I am worried about chemotherapy treatment because of its possible side effects that can lead to other illnesses. | 1.54 |
| 25 | I do not want people to gossip about me being a breast cancer patient. | 1.39 |
| 38 | I feel burdened about having to care more about my health. | 1.37 |
| 29 | I am afraid that my breast cancer might return. | 1.24 |
| 27 | I feel that the immense amount of examinations at the hospital is burdensome and a hassle. | 1.18 |
| 21 | I am afraid that my breast cancer might be genetic. | 1.05 |
| 37 | I feel like everything I have built throughout my life has become meaningless. | −1.94 |
| 31 | It makes me sad when I think about the possibility of a day when I have to accept that I will die because my breast cancer returned and I ran out of treatment options. | −1.78 |
| 35 | I am worried that my coworkers will judge me and have lower expectations from me regarding my work ability because of my cancer. | −1.48 |
| 36 | I am worried that I might not be able to work anymore. | −1.29 |
| 32 | I feel degraded when medical professionals treat me without empathy, as if our relationship is strictly business. | −1.10 |
| No. | Statement | Standard Score |
|---|---|---|
| 1 | I feel helpless because cancer is a disease that is beyond my control. | 2.10 |
| 36 | I am worried that I might not be able to work anymore. | 1.55 |
| 19 | I am worried about not being able to fulfil my role and responsibilities at home during treatment. | 1.54 |
| 40 | I think that I will eventually have to end my career. | 1.35 |
| 13 | I find it uncomfortable to go to public places such as saunas. | 1.24 |
| 18 | I am worried that I will burden my family. | 1.06 |
| 24 | I have some resentment because I feel I got breast cancer due to the continual stress from my family and work life. | −2.02 |
| 6 | Not knowing when I will die fills me with fear. | −2.01 |
| 21 | I am afraid that my breast cancer might be genetic. | −1.99 |
| 3 | I always feel exhausted from lack of sleep due to continual worries about having breast cancer. | −1.56 |
| 4 | I feel lonely and isolated. | −1.54 |
| 23 | I feel that my family and colleagues do not care when they still expect me to fulfil my roles and responsibilities. | −1.37 |
| No. | Statement | Standard Score |
|---|---|---|
| 1 | I feel helpless because cancer is a disease that is beyond my control. | 2.09 |
| 19 | I am worried about not being able to fulfil my role and responsibilities at home during treatment. | 1.16 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shim, M.-J.; Lee, S.-Y. South Korean Early Cancer Patients’ Perceptions of Difficulties in Fighting Their Disease: A Q Methodological Approach. Int. J. Environ. Res. Public Health 2022, 19, 12510. https://doi.org/10.3390/ijerph191912510
Shim M-J, Lee S-Y. South Korean Early Cancer Patients’ Perceptions of Difficulties in Fighting Their Disease: A Q Methodological Approach. International Journal of Environmental Research and Public Health. 2022; 19(19):12510. https://doi.org/10.3390/ijerph191912510
Chicago/Turabian StyleShim, Min-Jeung, and Song-Yi Lee. 2022. "South Korean Early Cancer Patients’ Perceptions of Difficulties in Fighting Their Disease: A Q Methodological Approach" International Journal of Environmental Research and Public Health 19, no. 19: 12510. https://doi.org/10.3390/ijerph191912510
APA StyleShim, M.-J., & Lee, S.-Y. (2022). South Korean Early Cancer Patients’ Perceptions of Difficulties in Fighting Their Disease: A Q Methodological Approach. International Journal of Environmental Research and Public Health, 19(19), 12510. https://doi.org/10.3390/ijerph191912510