3.2. Journey to Integration
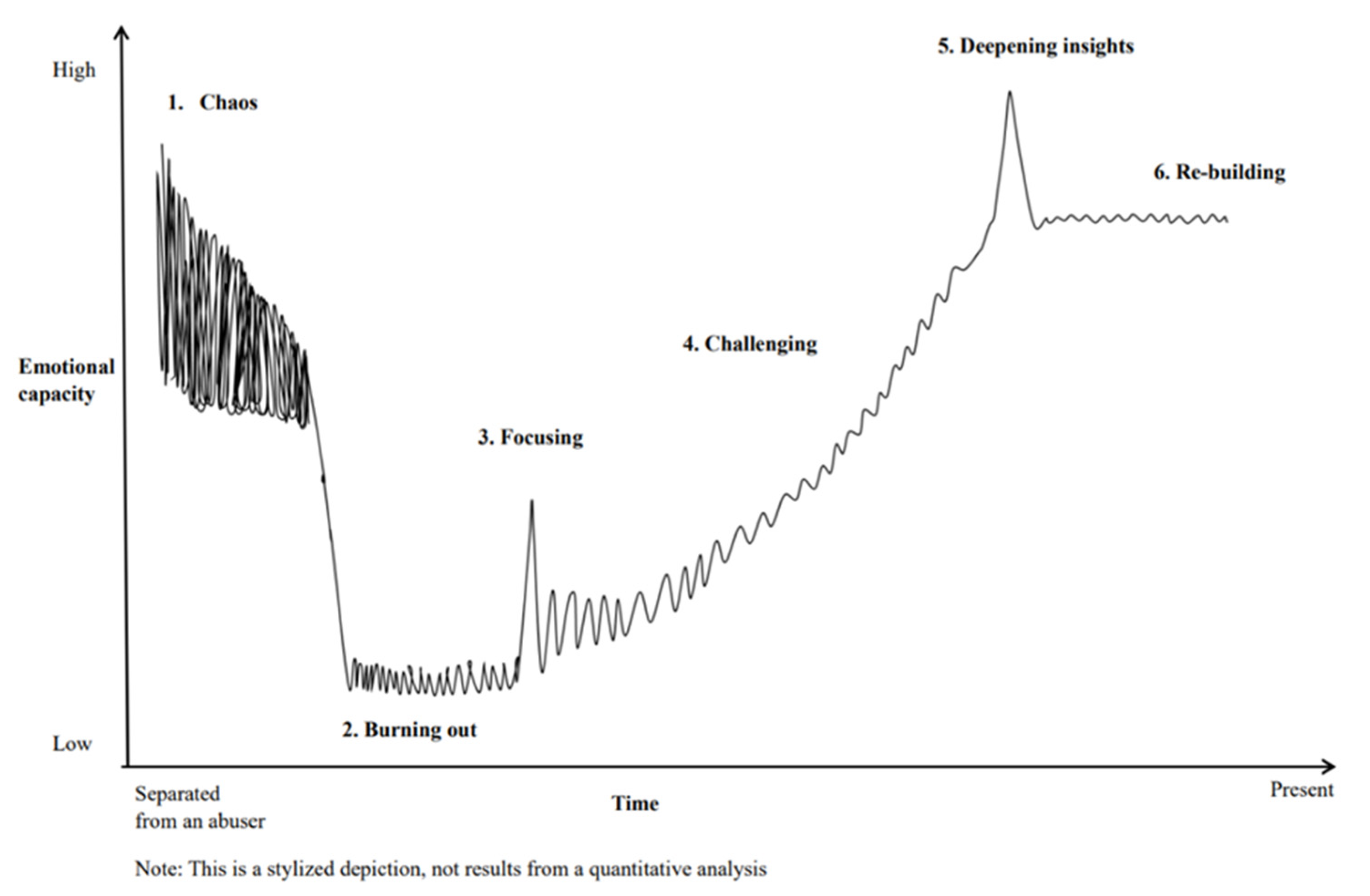
Six IPV recovery process categories were extracted: (1) Chaos, (2) Burning out, (3) Focusing, (4) Challenging, (5) Deepening insights, and (6) Re-building. The women described those six categories as stages or phases they passed through on their journey to their current recovery state (see
Figure 1). The x-axis was time, and the y-axis was emotional capacity. The time from the first to the last phase varied widely between the participants, ranging from 1.5 years to over 20 years. Therefore, the length of any given phase and the ratios of time of each phase were not the same; for instance, one survivor described that she stayed in the phase of Burning out for one year, and another said this phase lasted for over five years. These variations seemed to depend on numerous recovery conditions, such as their health status, the complexity of trauma and circumstance, and social support.
Additionally, the time frames of each phase were not necessarily demarcated. Phases frequently overlapped with others, moving back and forth. However, all the participants finally described the integration experience and the phases mentioned above. These phases represent the progression from initial escape toward their current state of trauma integration. In the following, we present the phases’ descriptions and highlight the subthemes that characterized these phases using italics.
Phase 1: Chaos. Chaos was the first phase women experienced as soon as they escaped from or were separated from their abusive partners. During the phase, they described feeling that they were in a chaotic situation, even though they seemed to be functioning. They also described feeling unsafe and disconnected from their body, mind, and social contexts. This phase was a highly tense period where they dealt with several problems following separation from their abuser, such as moving to a new place to live, managing their daily lives alone, and initiating legal divorce proceedings. The women reported that day-to-day troubles and feelings dominated their lives, leaving them no energy and time to pay attention to their internal feeling and problems. One woman said: “I didn’t know what to do, but I had to decide on an apartment and a school for my children quickly…I still don’t remember how I could deal with these things” (ID J0010).
In this phase, women experienced deep sorrow for losing their familiar environment, friends, and work. One woman reflected, “After leaving, I lost my house, friends, and job simultaneously. It was the most painful experience in my life” (ID J0028). They also described disappointment with responses from persons from whom they sought help. They were disappointed when they faced discrimination and rejection from parents, friends, and public officers when they sought help. Another woman said: “My parents told me, ‘…you embraced us because you got divorced and needed a place’ when I escaped to their house. I felt I was a troublemaker” (ID J0001). Women also described fears and panic of being chased by abusers and intense anxiety for the children, who were also affected by violence and separation. For example, one woman discussed their fears by saying: “A couple of days later, after escaping, my husband called me. At the time, I had no feeling except a strong fear of my husband, so I panicked” (ID J0005).
On the other hand, the women described a solid will to move forward from this chaotic situation. Additionally, ten women experienced gratitude for support from persons they sought help from and were surprised by positive changes in children soon after the separation. One woman said, “Before I left the house, I had a lot of feelings of anxiety, fear, and hesitation…but after leaving, I strongly felt I can’t come back anymore, and I have to move forward” (ID J0013). Another woman reflected, “I was so surprised that my child could sleep soundly the whole night since the day we left” (ID J0017).
Phase 2: Burning out. Women experienced the phase of Burning out after several of their day-to-day living and survival needs were met, and they started to live in a safe environment. This phase was referred to as the period that they faced and struggled with the severe and numerous impacts of violence, such as their physical, psychological, and social symptoms and emotional pain. Moreover, they suffered from feeling they had become different from others or had changed significantly, referring to it as “…falling from the bridge where everyone crosses” (ID J0013). They expressed that this phase was the hardest in their life after IPV. Nevertheless, they recognized this phase was a significant and necessary step toward becoming aware of and reconsidering their habitual ways of living and thinking.
Many women experienced unexplained physical symptoms in this phase, such as stomach pain, headache, nausea, palpitation, excessive weight loss, severe coldness, itchiness, or a long-lasting cough. One woman mentioned, “I was wondering what this palpitation is…and was very worried thinking that ‘I might die soon.’ I took medicine, but it didn’t work” (ID J0004). They also reported a lack of confidence and high pressure to proceed onward. For example, one woman noted, “My husband used to tell me, ‘you are useless and can’t do anything’ for a long time, so I didn’t think I could decide my future by myself” (ID J0013). They experienced loneliness and isolation for facing their feelings and experiences alone. Consequentially, they did not disclose or seek help from anybody. Four women reported explosive anger toward the abusers who had changed and ruined their lives. For example, one woman stated, “I repeatedly thought why he had done such terrible things to me…I wanted to pay (him) back. I was always irritated, and it made me so exhausted” (ID J0018).
Additionally, eight women experienced bewilderment to their child’s emotional explosion, such as aggressive behaviors, withdrawal, anger, shame, resistance to changing lifestyles, and regression due to the high stress of leaving a familiar environment and their father. One woman said, “My adolescent son started to be violent towards me because he didn’t like the situation of using a welfare service to live” (ID J0004). Another woman mentioned, “My (4-year-old) daughter … always chased me around and became insecure for 24 h. I think she exploded her suppressed trauma” (ID J0027).
Although they experienced these intense feelings, survivors also reported feeling suddenly powerless and sluggish. One woman described it as if “…an inflated balloon was popped” (ID J0009). They felt guilty and impatient for being lethargic. They felt too lonely and exhausted to think about their problems and future. They forgot their values, blamed themselves for being unable to live their lives properly, and felt impatient with themselves for their inability to work despite wanting to. Survivors summarized these feelings, saying: “I felt I was lazy and useless for myself being unable to do anything” (ID J0017); “I didn’t have power left to think about myself” (ID J0009); and “I felt very lonely compared to my children who seemed to adapt to this situation smoothly” (ID J0027).
Phase 3:Focusing. This phase occurred when the survivors focused on internal and external causes of their distress experienced in the Burning out phase, such as their habitual ways of thinking and becoming aware of their strong desire to stay true to themselves and to change their lives. In this phase, they described living “someone else’s life” as one of the leading causes of their distress, low self-confidence, and sense of inferiority. They also noticed the persistence of gender roles in their environment, as well as in their self-expectations. For example, one woman said: “I noticed I was exhausted because I had clung to the ideal characteristics of a ‘woman,’ ‘wife,’ and ‘mother,’ such that a wife has to make three meals every day and a mother has to smile and be cheerful all the time” (ID J0027). Seven women noticed that they always cared about others’ perceptions, resulting in physical and psychological distress, such as shame, regret, and fear. For instance, another woman mentioned, “When I looked back, I always thought that ‘I have to be a good woman’ from the perspective of my parents, my husband, and the world in general. I felt like I was living according to other people’s wishes” (ID J0018).
Survivors experienced an awareness that suppressing physical symptoms and psychological emotions is abnormal. To survive in a violent and unsafe environment, they tried not to feel any physical symptoms and distressing emotions, such as body pain, anger, unpleasantness, sadness, and loneliness. However, in this phase, they noticed this was abnormal and unhealthy. One woman described, “I had held tons of black stones (Kuroi-ishi) in myself, and I had tried to ignore all of them to keep a ‘normal life’ with my husband. However, I noticed that holding the black stones is not healthy for me and (that they) have to be released to the outside” (ID J0010).
Once the survivors became aware of these internal causes of distress, they felt an awakening desire to stay true to themselves. They desired to regain their senses and to do so, and they attempted to change their circumstances. One woman said: “I became so calm after I noticed I have freedom (nobody controls me), and I naturally started to think about what I want to do, and what makes me happier and calmer” (ID J0009).
Phase 4:Challenging. After becoming aware of the causes of their burning out and discovering their desire to change, survivors moved to the Challenging phase. The Challenging phase was described as the period in which they explored and tried to protect, re-discover, and regain sensibility, living life by healing physical and psychological distress, reconnecting with trusted others, and acquiring knowledge and skill to cope with trauma. However, survivors also simultaneously experienced new challenges, resulting in further distress. In this phase, all the women experimented with new actions to heal themselves and expand their possibilities, such as connecting with or joining a peer support group for IPV, finding or starting a job, and receiving several formal and informal (e.g., traditional) therapies. While forming connections with trusted others, such as peers, a new partner, and family, they experienced regaining a sense of security and peace with others and increasing confidence in their decision-making capacity. One woman noted, “I feel that peers are very important for me. We don’t deny our feelings and opinions with each other. I feel so easy and secure in the relationships” (ID J0025). Another mentioned, “My ex-husband used to repeatedly say, ‘You are not useful in the society,’ so I had to quit my job. In contrast, I noticed, ‘Oh, I’m very useful in society!’ when I came back to the job” (ID J0013).
Moreover, the connections they noticed between trauma, body, and mind were described after acquiring knowledge and skills through books, classes, and peer-support groups, yielding a greater understanding of their experience and symptoms. For example, one woman said, “I didn’t know why, but sometimes I felt pain and discomfort around my uterus, and when I felt it, my tears suddenly came out. But after I recognized that I was raped, I understood that the pain in my uterus came from my trauma and emotions” (ID J0025).
While embracing the positive changes, survivors also confronted new types of internal conflicts and distress during this phase, and their emotions were “shaken.” For example, they described helplessness for impulsive and intense anger and fear concerning their ex-husbands and other people (e.g., their parents and co-workers) who were indifferent towards, ignored, prejudiced, and discriminated against their trauma. One woman said: “I was used to thinking and living like ‘it is all my fault.’ But after I learned and recognized, ‘My trauma is not my fault,’ intense anger and hatred against the abuser and other people around me who didn’t help me suddenly came up. I couldn’t handle these painful feelings.” (ID J0025). In addition, women felt hopeless and vulnerable to unfairness, prejudice, and discrimination surrounding them by incessantly facing prejudice and victimization. One survivor mentioned, “When I started to work in a female counseling office for victims of violence, I saw my senior workers who labeled victims as ‘weak and troublesome women’ saying, ‘Victims have some faults (that cause them to be)…abused.’ I felt very sad, vulnerable, and hopeless” (ID J0005). Two survivors also described facing a core source of distress they had ignored, such as painful childhood experiences that deepened their understanding of their suffering. One woman expressed it as “…opening a locked box left alone for a long time” (ID J0017). They felt anger, helplessness, regret, chaos, and self-blame when they remembered their experience during childhood. Another woman mentioned, “I noticed my senses of shame, inferiority, isolation, and loneliness came from my childhood experience. My mother used to frequently slap and pinch me when I didn’t do what she wanted me to do. My friends said it was child abuse, but defining the experience is (still) too painful for me because I loved my mother” (ID J0018).
Phase 5: Deepening insights. After skills, knowledge, and thoughts were accumulated during the previous phase, survivors experienced the phase of Deepening insights. This phase was described as the period when they deepened their insights about themselves and their trauma, deciphered the meaning of their trauma and its impact on their lives, and interpreted why it happened. Such profound insights and philosophies developed gradually among some women but came up suddenly for others. By deepening their insights, survivors discovered connections between their trauma and emotions, their past and current experiences, and their body, mind, and social contexts. One woman described this phase as “…knitting together the lines that had broken apart” (ID J0025).
First, women began to view their lives, including trauma episodes, from multiple angles, noticing that life can’t be explained by trauma alone. Women not only focused on their misery but also remembered and appreciated the meaning and impact of pleasant times in their lives, affirming that trauma was only one part of their lives. One woman stated, “I don’t want to recognize myself as a victim because this is only one part of my life. I have experienced many happy times in my life, such as spending time with my children and doing my work” (ID J0004). Another survivor said, “I recognized that the saddest and the happiest moments were represented by one event in my life, such as the marriage with my ex-husband. So, I can’t judge my life using only one standard” (ID J0017). Additionally, the survivors expanded their perspectives toward people who had hurt them in the past, such as their abusive ex-husband and parents. They discovered different aspects of the person who hurt them by viewing these people from more distant and different angles. They recognized that the people who hurt them were not merely “bad people.” One woman said, “Looking back, I find that my dominant mother just didn’t know how to do it. I now know she raised me sternly” (ID J0009). Another said, “After I heard my father used to be abused by his mother, I feel that my father who abused me was also suffering” (ID J0017).
Survivors recognized that their trauma had been healed by trusted others, such as peers, friends, children, new partners, and co-workers. Throughout rebuilding secure and stable relationships with others, survivors felt they had been protected, healed, encouraged, and helped to confront and overcome their challenging period after GBV. One woman said: “My children, my new partner, and I discussed anything freely and equally. Those secure relationships healed my trauma” (ID J0013). Based on their newfound trust in and acceptance by others, women regained the confidence to stay true to themselves. Survivors examined their selfhood, discovering their strengths, weaknesses, and habitual thought and action patterns while trying to understand their aggressors. One woman mentioned: “It is better to think about what I want to be and not what other people expect of me. I want to focus on what kind of human being I am and how I want to live” (ID J0027). Six survivors described trying to interpret or discover why GBV happened to them. One woman stated, “I think my loneliness since childhood attracted my ex-husband (abuser) who had had similar experiences” (ID J0027). Another woman said, “I used to be controlled by my mother. Now I feel the controlling relationship just moved from my mother to my ex-husband.” (ID J0009).
When survivors reviewed and interpreted their entire life, all the survivors described reconnecting with their experiences, body, minds, and social contexts. They were convinced that their physical and psychological distresses, such as persistent headaches, breathlessness, or a loss of desire to live, were associated with trauma. One woman expressed this by saying, “…my body and mind remember the trauma” (ID J0013). For example, one woman mentioned, “I feel my emotions and memories relating to the past trauma that can’t be released and handled sometimes appear as various physical symptoms” (ID J0013). Another said: “…vague difficulties, such as persistent loneliness and a lack of self-confidence, have been lasting since my childhood. These feelings were related to my experience being with my parents” (ID J0009).
Furthermore, women recognized that their bodies and minds were always interconnected and that they influenced each other. One woman said, “…when I have a headache, I interpret I’m emotionally exhausted, so I try to rest or avoid the stressors” (ID J0005). Another said, “…my shoulder and back pains came from the pressure and stress of work” (ID J0028). While pondering on their entire lives and health, the survivors regained and increased the manageability and predictability of their physical and psychological distresses. They also acquired skills to cope with their distress, such as providing self-compassion with words such as “I can’t get frustrated, so don’t worry. You are doing best” (ID J0018), taking purposeful breaks, sharing feelings with trusted others, or seeking helping professionals (e.g., healer and acupuncture therapist).
Phase 6:Re-building. All the women experienced the final phase of Re-building. This phase was described as the period wherein women felt they had integrated the trauma into their lives, embraced their selfhood, and gained confidence in their ability to deal with the trauma impact. During this phase, they could see an overall picture of their selfhood, believe in their strength, and look toward the future. All the women described peace of mind and appreciating life as, “My mind is now calm like the sea” (ID J0009) and “I’m very glad to be alive” (ID J0027).
First, women believed that trauma is also an important aspect of their lives. They appreciated meeting or reconnecting with trusted others. Survivors now viewed the trauma as one event in the course of life and recognized that their current life was re-constructed by trauma. One woman mentioned, “It is my life, even if it gets painful” (ID J0010). Another woman stated, “I used to want to erase the hard period of my life, but now I feel that the period is also my life” (ID J0027).
Furthermore, survivors believed that “the trauma strengthened me.” Survivors felt they learned essential things from their experiences and became more mature. They understood the feelings of people with similar experiences, devoid of prejudice and discrimination, and they felt they became more compassionate than before the trauma. One woman said: “I have learned a lot from the struggling period. I became a person who understands people’s feelings” (ID J0017).
Furthermore, survivors strongly believed in their competence and decisions. They were proud of themselves that they could overcome such a challenging period and rebuild their lives. One woman stated: “When looking back to my past, I finally overcame so many challenging things in my life. I am proud of myself and believe I can overcome anything the future holds” (ID J0010). Moreover, they firmly believed that their decisions were not all ‘wrong.’ These decisions included not only the divorce from their ex-husband but also the smaller decisions in daily life. Women reported that although they did sometimes make mistakes in life, they could always learn something from these mistakes. One woman mentioned, “I made various mistakes and sometimes regretted it, but I think my key decisions, including separating from my husband, were not wrong” (ID J0001).
After regaining confidence in their competence and decisions, women finally embraced their lives and the fact that they had experienced trauma. They decided to live with the trauma, respect their feelings and hopes, avoid being manipulated by others, and recognize that “…it was fine to be me even if I am not perfect” (ID J0027). Survivors affirmed and embraced their way of living and were rarely influenced or shaken by other people anymore. One woman said: “I don’t mind how other people perceive me. I like myself now, even if it may seem weird to other people” (ID J0028). Another woman, who had experienced sexual violence, reported decreased shame and began to enjoy being a woman. Consequentially, these survivors started to look at the future and not the past, focusing on enriching their lives more. One woman said: “I don’t know what will happen in the future. However, I always want to look forward to making my life better” (ID J0009).




{kind=link}