


Healthcare Workers’ Resilience Toolkit for Disaster Management and Climate Change Adaptation



Abstract
1. Introduction
2. Methods
2.1. Design
2.2. Participant Recruitment
2.3. Data Collection and Analysis
2.4. Quality Assurance
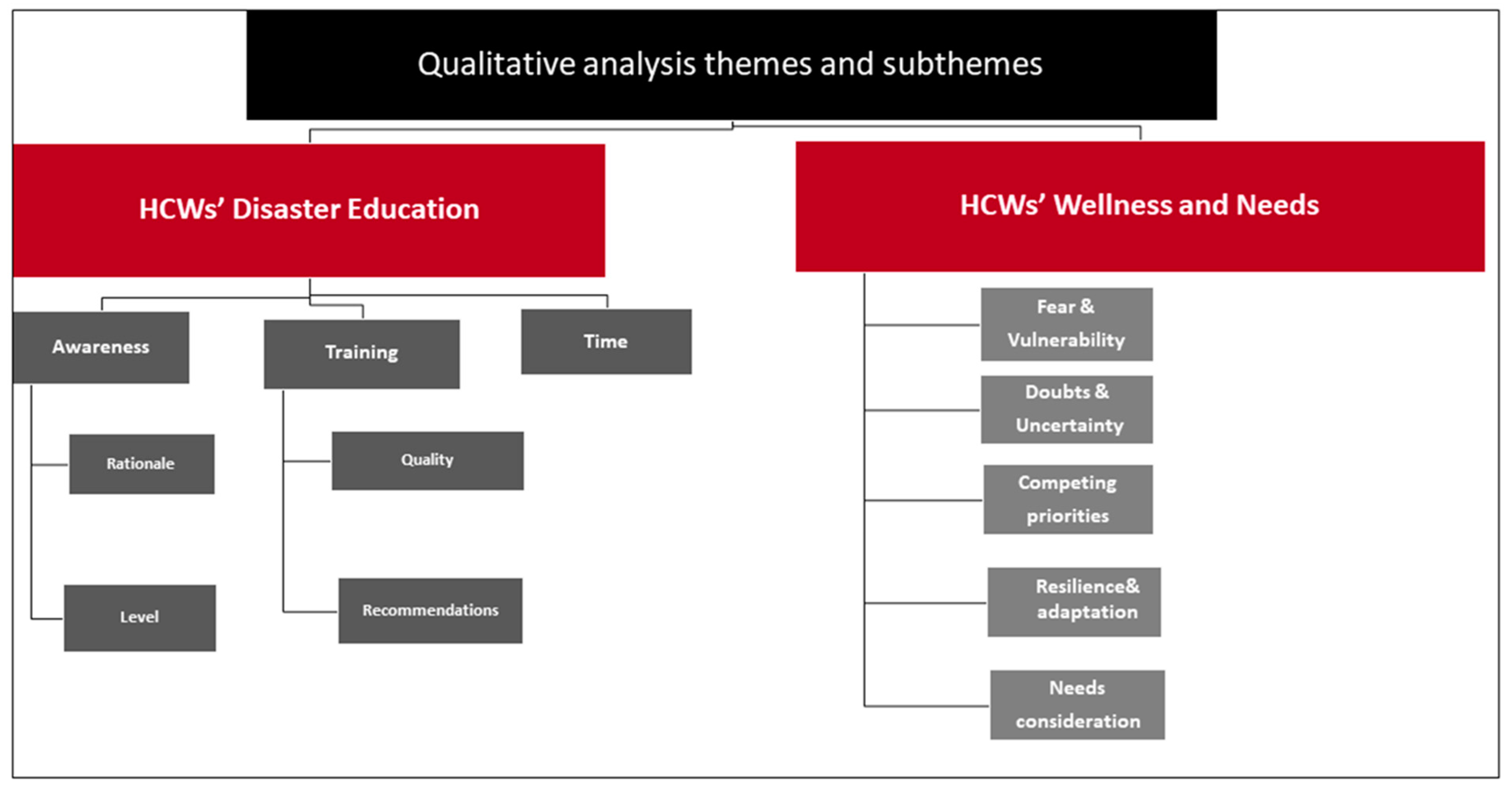
3. Results
3.1. HCWs’ Disaster Education Regarding Disaster Planning and Preparedness (DPP)
3.2. HCWs’ Wellness and Needs
4. Discussion
4.1. Enhancing Education and Training
4.2. Beyond Education and Training: The HCW’s Call for Action (SOS)
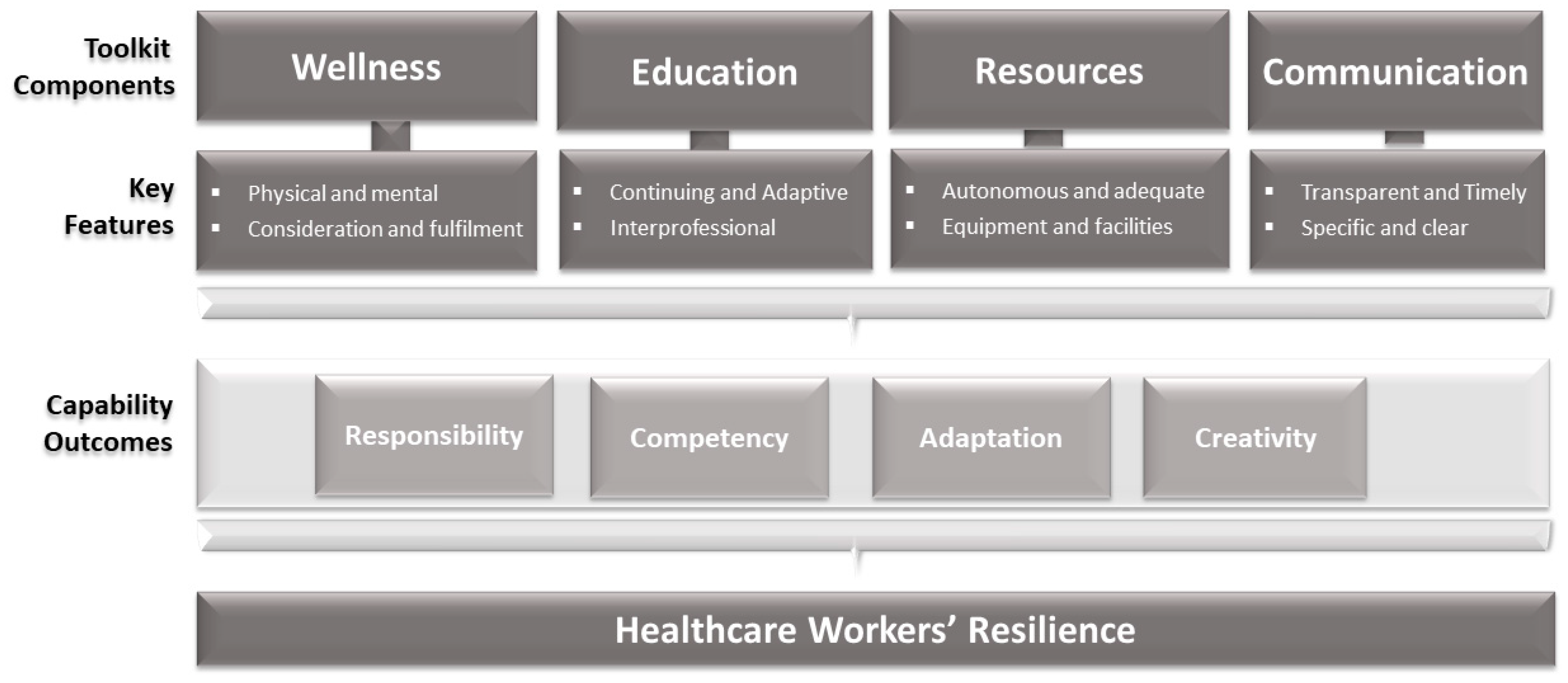
4.3. A Conceptual Framework for Action—A Healthcare Workers’ Resilience Toolkit for Their Disaster Management and Climate Change Adaptation
5. Limitations of the Study
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Benevolenza, M.A.; De Rigne, L. The impact of climate change and natural disasters on vulnerable populations: A systematic review of literature. J. Hum. Behav. Soc. Environ. 2019, 29, 266–281. [Google Scholar] [CrossRef]
- Kotcher, J.; Maibach, E.; Miller, J.; Campbell, E.; Alqodmani, L.; Maiero, M.; Wyns, A. Views of health professionals on climate change and health: A multinational survey study. Lancet Planet. Health 2021, 5, e316–e323. [Google Scholar] [CrossRef]
- Barouki, R.; Kogevinas, M.; Audouze, K.; Belesova, K.; Bergman, A.; Birnbaum, L.; Boekhold, S.; Denys, S.; Desseille, C.; Drakvik, E.; et al. The COVID-19 pandemic and global environmental change: Emerging research needs. Environ. Int. 2020, 146, 106272. [Google Scholar] [CrossRef]
- Gissing, A.; Timms, M.; Browning, S.; Crompton, R.; McAneney, J. Compound natural disasters in Australia: A historical analysis. Environ. Hazards 2021, 21, 1–15. [Google Scholar] [CrossRef]
- Vardoulakis, S. Reflections on climate change and the Australian health system. Aust. Health Rev. 2021, 45, 2–3. [Google Scholar] [CrossRef]
- Quitmann, C.; Sauerborn, R.; Danquah, I.; Herrmann, A. ‘Climate change mitigation is a hot topic, but not when it comes to hospitals’: A qualitative study on hospital stakeholders’ perception and sense of responsibility for greenhouse gas emissions. J. Med. Ethics 2022, 1–7. [Google Scholar] [CrossRef]
- Ali, H.M.; Desha, C.; Ranse, J.; Roiko, A. Planning and assessment approaches towards disaster resilient hospitals: A systematic literature review. Int. J. Disaster Risk Reduct. 2021, 61, 102319. [Google Scholar]
- Hathaway, J.; Maibach, E.W. Health Implications of Climate Change: A Review of the Literature About the Perception of the Public and Health Professionals. Curr. Environ. Health Rep. 2018, 5, 197–204. [Google Scholar] [CrossRef]
- Joseph, B.; Joseph, M. The health of the healthcare workers. Indian J. Occup. Environ. Med. 2016, 20, 71. [Google Scholar] [CrossRef]
- Ghanaatpisheh, E.; Khankeh, H.; Masoumi, G. Challenges for Hospital Resilience in Emergencies and Disasters: A Qualitative Study in Iran. J. Clin. Diagn. Res. 2019, 13, LC1–LC8. [Google Scholar] [CrossRef]
- Zhu, B.; Fan, H.; Xie, B.; Su, R.; Zhou, C.; He, J. Mapping the Scientific Research on Healthcare Workers’ Occupational Health: A Bibliometric and Social Network Analysis. Int. J. Environ. Res. Public Health 2020, 17, 2625. [Google Scholar] [CrossRef]
- Penwell-Waines, L.; Ward, W.; Kirkpatrick, H.; Smith, P.; Abouljoud, M. Perspectives on Healthcare Provider Well-Being: Looking Back, Moving Forward. J. Clin. Psychol. Med. Settings 2018, 25, 295–304. [Google Scholar] [CrossRef]
- Beiter, K.J.; Wiedemann, R.P.; Thomas, C.L.; Conrad, E.J. Alcohol Consumption and COVID-19–Related Stress Among Health Care Workers: The Need for Continued Stress-Management Interventions. Public Health Rep. 2022, 137, 326–335. [Google Scholar] [CrossRef]
- Achour, N.; Munokaran, S.; Barker, F.; Soetanto, R. Staff Stress: The Sleeping Cell of Healthcare Failure. Procedia Eng. 2018, 212, 459–466. [Google Scholar] [CrossRef]
- McCann, C.M.; Beddoe, E.; McCormick, K.; Huggard, P.; Kedge, S.; Adamson, C.; Huggard, J. Resilience in the health professions: A review of recent literature. Int. J. Wellbeing 2013, 3, 60–81. [Google Scholar] [CrossRef]
- Samsuddin, N.M.; Takim, R.; Nawawi, A.H. Human Behaviour and Resilience Hospital. Asian J. Behav. Stud. 2017, 2, 21–32. [Google Scholar] [CrossRef][Green Version]
- Baskin, R.G.; Bartlett, R. Healthcare worker resilience during the COVID-19 pandemic: An integrative review. J. Nurs. Manag. 2021, 29, 2329–2342. [Google Scholar] [CrossRef]
- Erdem, H.; Lucey, D.R. Healthcare worker infections and deaths due to COVID-19: A survey from 37 nations and a call for WHO to post national data on their website. Int. J. Infect. Dis. 2021, 102, 239–241. [Google Scholar] [CrossRef]
- Tovaranonte, P.; Cawood, T.J. Impact of the Christchurch Earthquakes on Hospital Staff. Prehospital Disaster Med. 2013, 28, 245–250. [Google Scholar] [CrossRef]
- Tseng, H.-M.; Shih, W.-M.; Shen, Y.-C.; Ho, L.-H.; Wu, C.-F. Work Stress, Resilience, and Professional Quality of Life Among Nurses Caring for Mass Burn Casualty Patients After Formosa Color Dust Explosion. J. Burn Care Res. 2017, 39, 798–804. [Google Scholar] [CrossRef]
- Park, Y.S.; Behrouz-Ghayebi, L.; Sury, J.J. Do Shared Barriers When Reporting to Work During an Influenza Pandemic Influence Hospital Workers’ Willingness to Work? A Multilevel Framework. Disaster Med. Public Health Prep. 2015, 9, 175–185. [Google Scholar] [CrossRef][Green Version]
- Jaimes, A.; Hassan, G.; Rousseau, C. Hurtful Gifts? Trauma and Growth Transmission Among Local Clinicians in Postearthquake Haiti. J. Trauma. Stress 2019, 32, 186–195. [Google Scholar] [CrossRef]
- Turner, S.B. Resilience of Nurses in the Face of Disaster. Disaster Med. Public Health Prep. 2015, 9, 601–604. [Google Scholar] [CrossRef]
- Casiraghi, A.; Domenicucci, M.; Cattaneo, S.; Maggini, E.; Albertini, F.; Avanzini, S.; Marini, M.P.; Galante, C.; Guizzi, P.; Milano, G. Operational strategies of a trauma hub in early coronavirus disease 2019 pandemic. Int. Orthop. 2020, 44, 1511–1518. [Google Scholar] [CrossRef]
- Raphael, T. Why Surgeons Don’t Want to Operate Right Now. Available online: https://www.bloomberg.com/opinion/articles/2020-03-24/the-coronavirus-crisis-is-putting-surgeons-at-risk-too (accessed on 24 September 2022).
- Wang, N.; Li, Y.; Wang, Q.; Lei, C.; Liu, Y.; Zhu, S. Psychological impact of COVID-19 pandemic on healthcare workers in China Xi’an central hospital. Brain Behav. 2021, 11, e02028. [Google Scholar] [CrossRef]
- Zahos, H.; Crilly, J.; Ranse, J. Psychosocial problems and support for disaster medical assistance team members in the preparedness, response and recovery phases of natural hazards resulting in disasters: A scoping review. Australas. Emerg. Care 2022, 25, 259–266. [Google Scholar] [CrossRef]
- World Health Organization. WHO Guidance on Research Methods for Health Emergency and Disaster Risk Management; World Health Organization: Geneva, Switzerland, 2021.
- Pan American Health Organization. Emergency Preparedness; Disaster Relief Coordination Program. Principles of Disaster Mitigation in Health Facilities; Pan American Health Organization: Washington, DC, USA, 2000.
- Nenkovic-Riznic, M.; Brankov, B.D.; Peirović, S.M.; Puca, M. Safe healthcare facilities Their Place and Role in Resilient Cities. Therm. Sci. 2018, 22, S1001–S1010. [Google Scholar] [CrossRef]
- Murshid, M.E.; Riaz, B.K.; Islam, Z.; Haque, M. Assessment of Safety Status and Response Capacity of Selected Primary Health Care Hospitals in Bangladesh. Eurasian J. Emerg. Med. 2019, 18, 137–141. [Google Scholar] [CrossRef]
- Sunindijo, R.Y.; Lestari, F.; Wijaya, O. Hospital safety index: Assessing the readiness and resiliency of hospitals in Indonesia. Facilities 2019, 38, 39–51. [Google Scholar] [CrossRef]
- Takim, R.; Samsuddin, N.M.; Nawawi, A.H. Assessing the content validity of hospital disaster resilience assessment instrument. J. Teknol. 2016, 78, 35–42. [Google Scholar] [CrossRef][Green Version]
- Zazali, A.K. Healthcare workers resilience from managing COVID-19 pandemic: A review. ITTPCOVID19 2021, 1, 1. [Google Scholar]
- Charney, R.; Rebmann, T.; Flood, R.G. Working After a Tornado: A Survey of Hospital Personnel in Joplin, Missouri. Biosecurity Bioterrorism Biodefense Strat. Pract. Sci. 2014, 12, 190–200. [Google Scholar] [CrossRef]
- Almukhlifi, Y.; Crowfoot, G.; Wilson, A.; Hutton, A. Emergency healthcare workers’ preparedness for disaster management: An integrative review. J. Clin. Nurs. 2021, 1–16. [Google Scholar] [CrossRef]
- Pariès, J.; Hollnagel, E.; Woods, D.D.; Wreathall, J. Resilience Engineering in Practice: A Guidebook; CRC Press LLC: Farnham, UK, 2010. [Google Scholar]
- Ali, H.M.; Ranse, J.; Roiko, A.; Desha, C. Investigating Organizational Learning and Adaptations for Improved Disaster Response Towards “Resilient Hospitals:” An Integrative Literature Review. Prehospital Disaster Med. 2022, 37, 1–9. [Google Scholar]
- Hegde, S.; Hettinger, A.Z.; Fairbanks, R.J.; Wreathall, J.; Wears, R.L.; Bisantz, A.M. Knowledge elicitation for resilience engineering in health care. In Proceedings of the Human Factors and Ergonomics Society Annual Meeting, Los Angeles, CA, USA, 26–30 October 2015; SAGE Publications: Los Angeles, CA, USA, 2015. [Google Scholar]
- Hollnagel, E.; Woods, D.D.; Leveson, N. Resilience Engineering: Concepts and Precepts; Ashgate Publishing, Ltd.: Farnham, UK, 2006. [Google Scholar]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Lincoln, Y.S.; Guba, E.G. Naturalistic Inquiry; SAGE Publication: Los Angeles, CA, USA, 1985. [Google Scholar]
- Roostaie, S.; Nawari, N.; Kibert, C. Sustainability and resilience: A review of definitions, relationships, and their integration into a combined building assessment framework. Build. Environ. 2019, 154, 132–144. [Google Scholar] [CrossRef]
- Mistretta, E.G.; Davis, M.C.; Temkit, M.; Lorenz, C.; Darby, B.; Stonnington, C. Resilience Training for Work-Related Stress Among Health Care Workers: Results of a Randomized Clinical Trial Comparing In-Person and Smartphone-Delivered Interventions. J. Occup. Environ. Med. 2018, 60, 559–568. [Google Scholar] [CrossRef]
- Al Thobaity, A.; Plummer, V.; Innes, K.; Copnell, B. Perceptions of knowledge of disaster management among military and civilian nurses in Saudi Arabia. Australas. Emerg. Nurs. J. 2015, 18, 156–164. [Google Scholar] [CrossRef]
- Iryanidar, I.; Kadar, K.S.; Irwan, A.M. Readiness of nurses working in COVID-19 pandemic. Int. J. Health Sci. 2022, 1639–1649. [Google Scholar] [CrossRef]
- Aliyu, S.; Norful, A.A.; Schroeder, K.; Odlum, M.; Glica, B.; Travers, J.L. The powder keg: Lessons learned about clinical staff preparedness during the early phase of the COVID-19 pandemic. Am. J. Infect. Control 2020, 49, 478–483. [Google Scholar] [CrossRef]
- Balay-Odao, E.M.; Alquwez, N.; Inocian, E.P.; Alotaibi, R.S. Hospital Preparedness, Resilience, and Psychological Burden Among Clinical Nurses in Addressing the COVID-19 Crisis in Riyadh, Saudi Arabia. Front. Public Health 2021, 8, 573932. [Google Scholar] [CrossRef] [PubMed]
- Brandrud, A.S.; Bretthauer, M.; Brattebø, G.; Pedersen, M.J.; Håpnes, K.; Møller, K.; Bjorge, T.; Nyen, B.; Strauman, L.; Schreiner, A.; et al. Local emergency medical response after a terrorist attack in Norway: A qualitative study. BMJ Qual. Saf. 2017, 26, 806–816. [Google Scholar] [CrossRef] [PubMed]
- Meyer, D.; Bishai, D.; Ravi, S.J.; Rashid, H.; Mahmood, S.S.; Toner, E.; Nuzzo, J.B. A checklist to improve health system resilience to infectious disease outbreaks and natural hazards. BMJ Glob. Health 2020, 5, e002429. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.R.; Coker, R.; Vrijhoef, H.J.-M.; Leo, Y.S.; Chow, A.; Lim, P.L.; Tan, Q.; Chen, M.I.-C.; Hildon, Z.J.-L. Mapping infectious disease hospital surge threats to lessons learnt in Singapore: A systems analysis and development of a framework to inform how to DECIDE on planning and response strategies. BMC Health Serv. Res. 2017, 17, 622. [Google Scholar] [CrossRef] [PubMed]
- Cariaso-Sugay, J.; Hultgren, M.; Browder, B.A.; Chen, J.-L. Nurse Leaders’ Knowledge and Confidence Managing Disasters in the Acute Care Setting. Nurs. Adm. Q. 2021, 45, 142–151. [Google Scholar] [CrossRef] [PubMed]
- Drevin, G.; Alvesson, H.M.; Van Duinen, A.; Bolkan, H.A.; Koroma, A.P.; Von Schreeb, J. “For this one, let me take the risk”: Why surgical staff continued to perform caesarean sections during the 2014–2016 Ebola epidemic in Sierra Leone. BMJ Glob. Health 2019, 4, 10. [Google Scholar] [CrossRef] [PubMed]
- Bikomeye, J.C.; Rublee, C.S.; Beyer, K.M.M. Positive Externalities of Climate Change Mitigation and Adaptation for Human Health: A Review and Conceptual Framework for Public Health Research. Int. J. Environ. Res. Public Health 2021, 18, 2481. [Google Scholar] [CrossRef]
- Besley, J.C.; Dudo, A.; Yuan, S.; Lawrence, F. Understanding Scientists’ Willingness to Engage. Sci. Commun. 2018, 40, 559–590. [Google Scholar] [CrossRef]
- Ebi, K.L.; Vanos, J.; Baldwin, J.W.; Bell, J.E.; Hondula, D.M.; Errett, N.A.; Hayes, K.; Reid, C.E.; Saha, S.; Spector, J.; et al. Extreme Weather and Climate Change: Population Health and Health System Implications. Annu. Rev. Public Health 2021, 42, 293. [Google Scholar] [CrossRef]
- Hayes, K.; Poland, B. Addressing Mental Health in a Changing Climate: Incorporating Mental Health Indicators into Climate Change and Health Vulnerability and Adaptation Assessments. Int. J. Environ. Res. Public Health 2018, 15, 1806. [Google Scholar] [CrossRef]
- Azzollini, S.C.; DePaula, P.D.; Cosentino, A.C.; Pupko, V.B. Applications of Psychological First Aid in Disaster and Emergency Situations: Its Relationship with Decision-Making. Athens J. Soc. Sci. 2018, 5, 201–214. [Google Scholar] [CrossRef]
- Ćosić, K.; Popović, S.; Šarlija, M.; Kesedžić, M. Impact of human disasters and COVID-19 pandemic on mental health: Potential of digital psychiatry. Psychiatr. Danub. 2020, 32, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Huggard, P. Caring for the Carers: The emotional effects of disasters on health care professionals. Australas. J. Disaster Trauma Stud. 2011, 2, 60–62. [Google Scholar]
- Raven, J.; Wurie, H.; Witter, S. Health workers’ experiences of coping with the Ebola epidemic in Sierra Leone’s health system: A qualitative study. BMC Health Serv. Res. 2018, 18, 9. [Google Scholar] [CrossRef]
- Hoque, M.E. Three domains of learning: Cognitive, affective and psychomotor. J. EFL Educ. Res. 2016, 2, 45–52. [Google Scholar]
- Yphantides, N.; Escoboza, S.; Macchione, N. Leadership in Public Health: New Competencies for the Future. Front. Public Health 2015, 3, 24. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Constructed Reflections Based on a Synthesis of Participants’ Voices | Excerpts from Participants’ Transcripts |
|---|---|
| I became aware of disaster planning and preparedness because … * | The rationale for DPP awareness, including the reasons and methods that led the participants to be aware of their hospitals’ DPP documents and processes |
| |
| My knowledge/competencies about DPP are…. | The DPP awareness level, including the participants’ perception and evaluation of their or others’ knowledge and competencies a result of this awareness. |
|
| Constructed Reflections Based on a Synthesis of Participants’ Voices | Excerpts from Participants’ Transcripts |
|---|---|
| I figured out that my training is … * | Quality of DPP training: including the participants’ perceptions, expectations and thoughts regarding their DPP training and practice. |
| |
| What I need regarding training is … | Recommendations: including the participants’ recommendations and suggestions on their DPP training and in particular the simulations. |
| |
| What I need regarding simulation is … | The significance of time: including the effect of time on the quality and application of DPP training, |
|
| Constructed Reflections Based on a Synthesis of Participants’ Voices | Excerpts from Participants’ Transcripts |
| The time factor affected me by … * | The significance of time: including the effect of time on the quality and application of DPP training |
|
| Constructed Reflections Based on a Synthesis of Participants’ Voices | Subtheme: Fear and Vulnerability |
|---|---|
| My feelings and concerns are/were … |
|
| Sub-Theme: Doubts and Uncertainty | |
| |
| My resilience and adaptation levels are … | Sub-Theme: Competing priorities |
| |
| My resilience and adaptation levels are … | Sub-Theme: Resilience, and Adaptation |
| |
| My needs to be considered are … | Sub-Theme: Needs Considerations |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mohtady Ali, H.; Ranse, J.; Roiko, A.; Desha, C. Healthcare Workers’ Resilience Toolkit for Disaster Management and Climate Change Adaptation. Int. J. Environ. Res. Public Health 2022, 19, 12440. https://doi.org/10.3390/ijerph191912440
Mohtady Ali H, Ranse J, Roiko A, Desha C. Healthcare Workers’ Resilience Toolkit for Disaster Management and Climate Change Adaptation. International Journal of Environmental Research and Public Health. 2022; 19(19):12440. https://doi.org/10.3390/ijerph191912440
Chicago/Turabian StyleMohtady Ali, Heba, Jamie Ranse, Anne Roiko, and Cheryl Desha. 2022. "Healthcare Workers’ Resilience Toolkit for Disaster Management and Climate Change Adaptation" International Journal of Environmental Research and Public Health 19, no. 19: 12440. https://doi.org/10.3390/ijerph191912440
APA StyleMohtady Ali, H., Ranse, J., Roiko, A., & Desha, C. (2022). Healthcare Workers’ Resilience Toolkit for Disaster Management and Climate Change Adaptation. International Journal of Environmental Research and Public Health, 19(19), 12440. https://doi.org/10.3390/ijerph191912440